
Abstract
The purpose of this mixed-methods study was to measure perceived social standing within an assisted living (PSS-AL), and to identify individual determinants and empirical correlates of this construct. The sample consisted of 200 residents of 21 assisted livings (ALs). A self-anchoring ladder measured PSS-AL (M = 6.95, SD = 2.04) and an open-ended follow-up question assessed individual determinants of PSS-AL ratings. In a multiple regression, mental health (β = .27, p = .001), intimate staff-resident relationships (β = .22, p = .024), and extraversion (β = .27, p < .001) were significant predictors of PSS-AL. Qualitative findings revealed that inter-personal factors, prosocial behaviors, and health were key determinants of PSS-AL. Results highlight the social demands of AL and associated implications for residents with varying social abilities, skills, and interests. Findings also suggest that staff-resident relationships may shape and-or reinforce resident social hierarchies. The authors discuss implications for research and practice.
Keywords
Introduction
Assisted living (AL) is an umbrella term used to describe residential care settings that provide supportive services, while prioritizing independence and control for adults with significant health needs (Kane et al., 2007). Recent estimates suggest that ALs are home to over 700,000 Americans with diverse physical, cognitive, and functional profiles (Khatutsky et al., 2016). As the AL industry continues to grow and more adults with varying backgrounds make this setting their permanent residence, research on social dynamics can provide valuable information regarding the resident experience after relocation.
Previous studies reported that AL residents often form social groups based on similar abilities and interests, which can contribute to unequal levels of social standing or social status within the community (Hrybyk et al., 2012; Kemp et al., 2012; Sandhu et al., 2013). Social standing or status refers to the level of regard, respect, and admiration for an individual by others in the same social context (Fragale et al., 2011). Subjective ratings of social standing or status capture an individual’s perceived placement within a defined social hierarchy (Singh-Manoux et al., 2003). This rating procedure involves a complex subjective process of weighting and averaging salient personal and community characteristics to derive a self-report of individual social standing or status within the referent social context (Garbarski, 2010). Previous scholars suggest that subjective measurements of social standing and status can provide valuable insight into the social dynamics of a community (Koski et al., 2015).
In AL, a resident’s perceived placement within their community’s social hierarchy may influence social experiences and quality of life. For example, in residential care settings, previous studies found that residents with higher social standing or status reported greater co-resident relationships and activity involvement (Iecovich & Lev-Ran, 2006; Sandhu et al., 2013). By investigating perceived social standing, this study comments on social hierarchies within AL communities.
Numerous terms appear in the literature to describe an individual’s placement within a social hierarchy, including social status, social standing, social position, social rank, and sociometric status. In the current study, we use the term “perceived social standing” over other commonly used terms (e.g., “subjective social status”) to describe residents’ self-reported placement within the social hierarchy in their AL community. Consistent with rationale provided by Garbarski (2010), we favor the term “perceived” over “subjective” because participants in the current study respond to an external question, rather than describe an existing internal phenomenon. In addition, researchers commonly use the term “social status” to describe socioeconomic status (Adler & Stewart, 2007). Therefore, to avoid confusion, we use “social standing” because our study does not specifically focus on economic aspects of social hierarchies. Further, “social rank” and “social position” imply that individuals are the units of measurement (e.g., higher than Person A, but lower than Person B); however, participants in our study will only report their own placement within a social hierarchy. Similarly, “sociometric status” requires peer ratings or nominations (Jiang & Cillessen, 2005), which lack validity in AL and is beyond the scope of this study. Thus, the term “perceived social standing” best fits the objectives of the current study.
To the knowledge of the authors, the literature has yet to operationalize and measure perceived social standing within an assisted living (PSS-AL), nor are the determinants or correlates of this construct well-defined among AL residents. This mixed-methods study addresses this limitation by measuring PSS-AL and assessing its individual determinates and empirical correlates in a sample of AL residents from multiple communities.
Literature Review
Festinger’s (1954) Social Comparison Theory suggests that individuals evaluate their own resources and abilities by comparisons to others. This natural process of social comparison can lead to the formation of groups with others believed to possess similar resources. Ultimately, these groups result in social hierarchies (i.e., groups of individuals with greater resources experiencing higher social standing; Anderson et al., 2012).
Consistent with Social Comparison Theory, multiple qualitative studies reported that AL residents formed relationships with others perceived as having similar resources like physical, cognitive, and-or sensory abilities (Kemp et al., 2012; Perkins et al., 2012; Sandhu et al., 2013). Other factors that may inform the formation of resident social groups in AL include: demographics (e.g., age, gender, race, and ethnicity), personality, family visitation patterns, physical appearance, occupation, socioeconomic status, education, and personal skills or interests (Cruz, 2006; Dobbs et al., 2008; Kemp et al., 2012; Perkins et al., 2012; Sandhu et al., 2013). Therefore, it is no surprise that social hierarchies exist among residents in AL communities. Further, previous studies reported that AL residents with lower social standing within their community experienced heightened risk for negative interactions and poor social integration (Dobbs et al., 2008; Doyle et al., 2012; Iecovich & Lev-Ran, 2006; Kemp et al., 2012). Taken together, social standing may represent a major component of the resident experience and psychosocial well-being after relocation to an AL community.
Previous studies used various strategies to assess perceived social standing and related constructs (e.g., social status, social rank, or sociometric status). Some studies measured these constructs using peer ratings or nominations within a defined social context (Jiang & Cillessen, 2005). This method is often used in social contexts where group members have regular encounters with peers, like in a classroom. Peer ratings are quite time intensive and represent a challenge in AL, where residents may not interact with or recall the names of all other members of their community. Other studies utilized social comparison scales of desirable traits to indirectly assess social standing (Allan & Gilbert, 1995). This measurement strategy requires that scales are tailored to the environment and population of interest (MacMahon & Jahoda, 2008), and traits associated with PSS-AL are not yet captured in the literature. Thus, there are unique challenges to measuring perceived social standing within ALs.
Although commonly used to assess socioeconomic status (Adler & Stewart, 2007), a self-anchoring ladder is a promising method for measuring perceived standing within a defined social hierarchy (Kilpatrick & Cantril, 1960). Previous studies used self-anchoring ladders to measure perceived social standing across neighborhoods, friend groups, and even in residential care communities (Ayalon, 2019; Geiger et al., 2019). This method has also demonstrated acceptable reliability for measuring constructs that accept inter-individual variability, like quality of life or community engagement (Di Napoli & Arcidiacono, 2013; Kilpatrick & Cantril, 1960). For these reasons, a self-anchoring ladder was a good fit to measure PSS-AL in the current study.
Perceived social standing is often applied to societal social hierarchies, such as global socioeconomic status (Singh-Manoux et al., 2003). However, community social hierarchies (e.g., neighborhoods, religious groups, workplaces, or friend groups) are gaining more attention in the literature (Zell et al., 2018). Multiple studies found that, when compared to societal hierarchies, social standing within a community yielded stronger positive relationships with physical and mental health outcomes (Anderson et al., 2012; Zell et al., 2018). Similarly, previous studies with older adults found that higher perceived community social standing related with greater self-rated health, mental well-being, and social satisfaction (Cundiff et al., 2011, 2013). Further, Ayalon (2019) reported that higher social standing predicted lower perceived loneliness and greater social relationships in a continuing care retirement community. Overall, previous findings suggest that perceived standing within a community social hierarchy may be a significant component of psychosocial and overall quality of life.
Previous scholars suggest that individuals may interpret and rate perceived community social standing differently than societal social standing (Andersson, 2018). However, only a few studies offer insight into determinants of perceived social standing, particularly within community contexts. One study found that volunteering, citizenship, respect, and social acceptance were indicators of perceived social standing within a community, whereas wealth, occupation, and education were indicators of societal social standing (Snibbe et al., 2007). Although, it should be noted that these authors did not specify a referent community (e.g., a neighborhood or workplace). Another study reported that correlates of perceived social standing varied based on cultural and socioenvironmental factors salient to the referent community (Brown et al., 2008). Taken together, it is particularly important to explore determinants and correlates of PSS-AL in order to provide insight into the unique social context of this residential care setting.
Purpose
The purpose of this study was to measure PSS-AL, and to investigate its individual determinants and empirical correlates in a sample of AL residents from multiple communities. To accomplish this, we used both quantitative and qualitative methods. First, we measured PSS-AL using a self-anchoring ladder and assessed the relationships between PSS-AL and demographic, health, social, psychological, and community variables. Next, using an open-ended question, we identified individual determinants of PSS-AL ratings. Lastly, we interpreted quantitative and qualitative data concurrently to comment on resident social hierarchies within AL communities.
Research Design
Study Design
This study utilized a cross-sectional concurrent triangulation design to analyze quantitative and qualitative data, with a quantitative priority (O’Cathain et al., 2010). See Figure 1 for a visual representation of data collection, analysis, and interpretation procedures.

Process of collecting and analyzing mixed-methods data.
Setting & Participants
The current sample consisted of 200 participants from 21 ALs located in the western United States. Communities ranged in size from 16 to 104 residents (M = 54.19, SD = 25.07). The majority of ALs were chain operated (n = 11), cost more than $3,000 per month (n = 16), and housed mostly private-pay residents (n = 14; i.e. 75% or more of the residents were private-pay).
The 200 participants ranged in age from 51 to 100 (M = 83.05, SD = 10.32). Most were female (n = 143, 72%), white (n = 180, 90%), widowed (n = 118, 59%), had higher than a high school education (n = 133, 67%), and used private payment (n = 139, 69%). The majority of participants (n = 103, 52%) moved to their AL from a private residence; length of stay ranged from less than 1 month to 160 months (M = 21.17 months, SD = 20.44).
Procedures
The affiliated Institutional Review Board approved all study procedures. Prior to data collection, pilot analyses with 11 residents in a single AL guided modifications to measures and procedures, including the measurement of PSS-AL. Specifically, the study team slightly modified the verbal prompt and added “best thought of residents” and “worst thought of residents” to the ladder. This addition helped ensure participants were oriented to the targeted construct of perceived social standing.
The researchers identified ALs to serve as data collection sites by emailing or calling allied staff (i.e., executive directors, administrators, or activity directors) or through referrals from other ALs, professional organizations, or operating company administrators. Multiple strategies helped recruit a convenience sample of residents at the targeted ALs, including staff nominations, in-person announcements, and snowball sampling.
The current study used the following inclusion criteria: (a) age 50 or older; (b) able to speak and understand English; (c) own decision-maker; and (d) score of five or above on the Memory Impairment Scale (Buschke et al., 1999). These criteria are consistent with ethical standards for research with populations at-risk for cognitive impairment (Alzheimer’s Association, 2004); the impact of inclusion criteria is discussed further in the limitations section. Two hundred thirty-five residents volunteered for the current study; 30 were excluded for not meeting criterion d, 3 were excluded for not meeting criterion a, and 2 additional participants were excluded for missing PSS-AL data. Overall, 200 residents were included in analyses.
The primary author met with each participant individually to determine eligibility, obtain written informed consent, and administer select survey questions, including PSS-AL and the open-ended follow-up question. The primary author administered all open-ended questions using a standardized prompt and took detailed handwritten notes on participant answers, transcribing responses verbatim when possible. Additional quantitative measures were administered either during in-person interviews facilitated by the primary author or a trained research assistant (i.e., verbal administration; n = 184), or by using alternative methods like a group interview or a take-home copy to be returned within 24 hours (n = 16). Independent samples t-tests revealed no differences in PSS-AL (p = .430) or social desirability (p = .574), as measured by the 5-item Socially Desirable Response Set (Hays et al., 1989), based on survey administration method (i.e., in-person or alternative).
Measures
PSS-AL
The current study measured PSS-AL using a 10-rung self-anchoring ladder (Kilpatrick & Cantril, 1960). Participants were prompted to indicate their social standing on the ladder relative to other residents in their AL community. The prompt used in this study was adopted from the MacArthur Study (Adler & Stewart, 2007) and modified based on pilot analyses with AL residents, see Online Appendix for measure and prompt. In previous studies targeting social standing in unspecified community contexts, self-anchoring ladders evidenced acceptable test-retest reliability and construct validity with psychosocial measures (Cundiff et al., 2013; Giatti et al., 2012). Scores ranged from 1 to 10, with 10 = highest standing and 1 = lowest standing. Consistent with previous studies (Hoebel et al., 2017), PSS-AL ratings were classified based on quintiles: low (quintile 1; PSS-AL = 1–5), medium (quintiles 2–4; PSS-AL = 6–8), and high (quintile 5; PSS-AL = 9–10).
Directly after administrating the PSS-AL measure, the interviewer asked participants a standardized prompt: “Tell me about why you placed yourself there?” This question was designed to provide insight into participants’ determinants of PSS-AL ratings. Follow-up questions were only used for clarification of participant responses.
Demographics
Staff at each community reported ownership type, size, costs, and resident financing strategies (e.g., percent of Medicaid beds). Resident participants self-reported gender, ethnicity, age, education, marital status, length of stay, and Medicaid status.
Health
Subscales from the Patient Reported Outcome Measurement Information System (PROMIS) Short-Form Global Health Scale (Hays et al., 2009) assessed physical and mental health. For each subscale, scores range from 4 to 20 with higher scores indicating greater health. Internal consistency for the sample was acceptable for both the physical health (Cronbach’s α = .71) and mental health (Cronbach’s α = .73) subscale.
Participants responded to two single-item questions assessing vision and hearing on five-point scales, 1 = poor, 5 = excellent. Items were summed to assess overall sensory ability; scores range from 2 to 10, higher scores indicate greater sensory ability.
Cognitive ability was assessed using the Clock Drawing Test (CDT) with a three-factor scoring method (Cahn et al., 1996; Rouleau et al., 1992): integrity of the clock face (0–2); presence and sequencing of numbers (0–4); and presence and placement of the hands (0–4). Inter-rater reliability between two independent raters using a subsample of 28 drawings was acceptable in the current study (ICC = .71, p < .001). Scores range from 0 to 10, higher scores indicate greater cognitive ability.
Relationships
Single items from a modified version of the 6-item Lubben Social Network Scale (Lubben et al., 2006) measured relationships with other residents, staff, and outside visitors (i.e., family and friends). For each targeted source of support (e.g., staff or residents), participants indicated number of friendships (e.g., “How many other residents [at your assisted living] do you consider friends?”) and intimate relationships (e.g., “How many staff members [at your assisted living] do you feel at ease with that you can talk about private matters that you would not openly share with others?”) on a 6-point scale, 0 = none, 5 = 9+.
Activity Attendance
Participants self-reported activity attendance in the seven days prior to data collection by indicating each programmed activity (1 = yes, 0 = no) they attended on an index created from each AL’s unique activity calendar. To control for variability in activity offerings, the authors used the percentage of offered activities attended in analyses.
Extraversion
Two items from the Big Five Inventory-10 item version measured extraversion (Rammstedt & John, 2007). Scores range from 2 to 10, higher scores indicate greater extraversion. Internal consistency with the sample was acceptable (Cronbach’s α = .73).
Data Analysis Plan
The authors used SPSS v.25 for quantitative analyses and Atlas.ti 8 for qualitative analyses. Prior to quantitative analysis, statistical assumptions were tested and no transformations to the data were required. PSS-AL did not significantly correlate with social desirability (r = .05, p = .480). Only the CDT evidenced missing data (n = 15) and, to avoid bias, no imputations were made.
Twenty-four (12%) participants did not respond to the open-ended question. Missing qualitative data was observed for 6 (14%) participants with low, 17 (15%) participants with medium, and 1 (2%) participant with high PSS-AL. There were no significant group differences based on missing data (i.e., missing qualitative data or not) in PSS-AL scores when measured as a categorical (χ2(2) = 4.91, p = .086) or continuous (t(198) = .72, p = .470) variable. There were no significant group differences related to missing data for most study variables, including demographic, health, and relationship factors (p > .157). However, participants that did not respond to open-ended questions evidenced slightly higher cognitive ability than those who provided qualitative answers (t(183) = −2.01, p = .046); no changes were made to the data as this finding was determined to not significantly bias results or interpretations from the current study.
To offer insight into empirical correlates of PSS-AL, we used Pearson’s correlation coefficients for relationships with continuous study variables and independent samples t-tests for dichotomous study variables. In addition, we performed a multiple linear regression with PSS-AL as the dependent variable and health, social, and psychological factors as independent variables. To offer insight into the profile of residents across PSS-AL ratings, we performed a series of one-way ANOVAs with PSS-AL categorized into low, medium, and high ratings as the independent variable, and demographic, health, social, psychological, and community factors as dependent variables.
Qualitative responses to the open-ended question typically consisted of one to two sentences or phrases. These responses were uploaded into Atlas.ti 8 for analysis. The authors served as two independent raters and coded responses using an iterative process consistent with conventional content analysis (Hsieh & Shannon, 2005). In conventional content analysis, codes and categories emerge directly from the data, rather than using preconceived categories to guide qualitative analysis. This method allowed the authors to code and categorize qualitative data without influence from quantitative analyses and, then, compare independent qualitative and quantitative findings in the discussion section.
For quantitative analysis, first, the primary author read all responses word-for-word to create an initial codebook that defined each code to ensure consistency across raters. Next, both authors reviewed all responses and met to refine the codebook, keeping an audit trail of all changes. The authors then independently coded the entire dataset and met again to discuss discrepancies and modify the codebook accordingly. Finally, both authors conducted an independent final coding of the entire dataset, inter-rater agreement was 98%. Some responses generated multiple codes; the authors reported the total number of codes reported across participants (i.e., more than one code per participant in certain cases).
Results
Quantitative Analyses
Descriptive statistics are presented in Table 1. Physical and mental health in the current sample were lower than previously reported among healthy adult and community-living older adult samples (Hays et al., 2009; Rosenberg et al., 2015). Despite using a cognitive screen for inclusion criteria, the current sample ranged from 1 to 10 on the CDT (n = 185; M = 7.69, SD = 1.93). Based on cutoffs identified in previous research (Conner et al., 2005), 38% (n = 71 of 185) of participants that completed the CDT reported scores consistent with a neurocognitive disorder (i.e., 7 or below). It should be noted that CDT data were missing for 8% (n = 15) of the current sample.
Descriptive Statistics of Study Variables and Correlations.

Note. * p < .05. ** p < .01. *** p < .001.
PSS-AL ratings ranged from 1 to 10 (M = 6.95, SD = 2.04, Median = 7), see Figure 2. Based on the identified cutoffs, 44 (22%) participants rated PSS-AL as low, 113 (57%) participants rated PSS-AL as medium, and 43 (21%) participants rated PSS-AL as high.
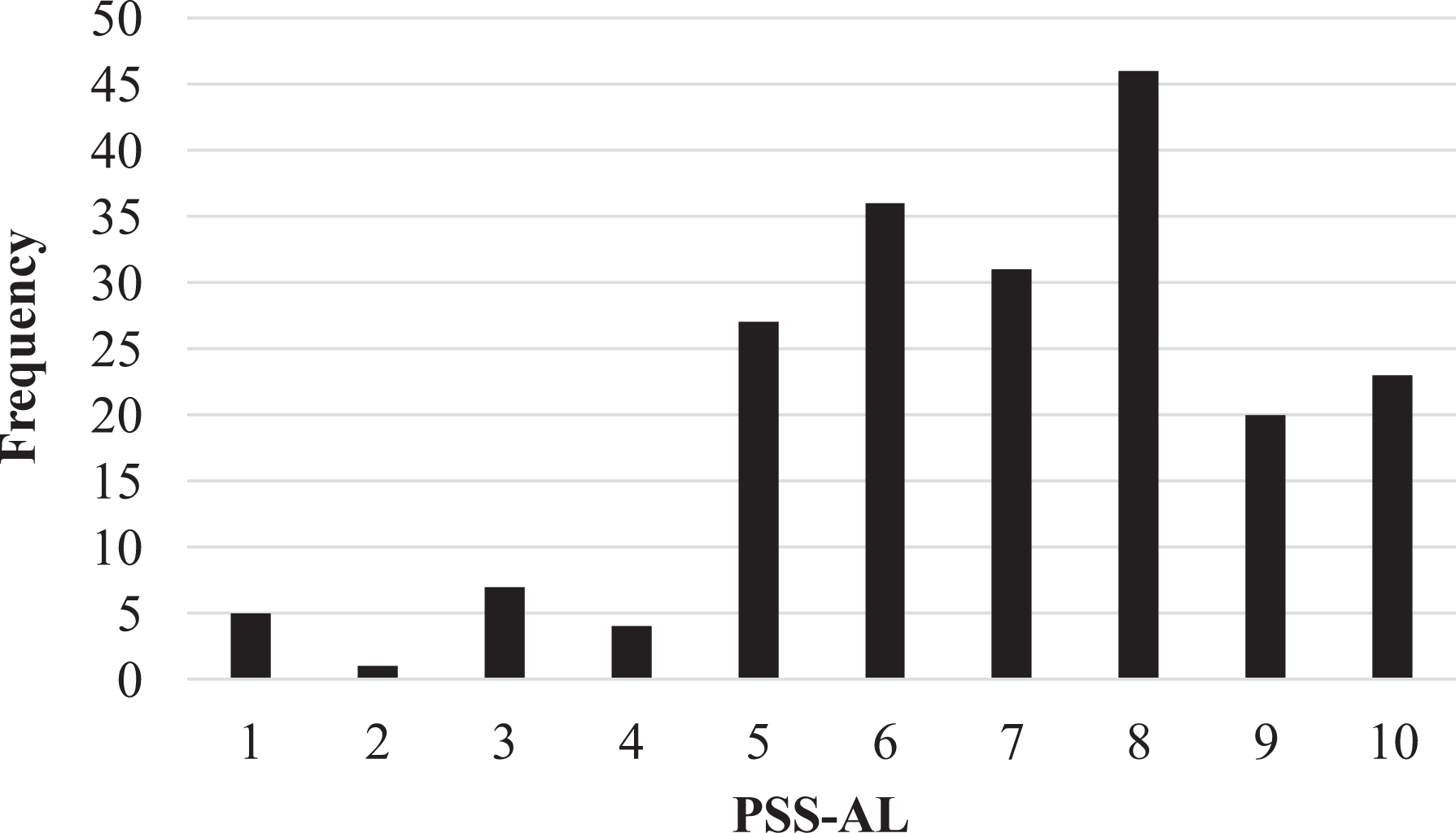
Distribution of PSS-AL ratings.
Relationships between PSS-AL and study variables are presented in Table 1. Correlations revealed no significant relationships between PSS-AL and age, length of stay, or size of the AL community. Independent samples t-tests revealed no significant differences in PSS-AL across gender, marital status (i.e., widowed), socioeconomic status (i.e., financing AL with Medicaid), living in a chain operated community, or AL cost (i.e., more than $3,000 per month).
Study variables were regressed on PSS-AL. There were no violation to assumptions, including multicollinearity (VIF < 2.29). The regression model explained 28% of the variance in PSS-AL (F(12, 172) = 5.66, p < .001). Mental health (β = .27, p = .001), intimate staff-resident relationships (β = .22, p = .024), and extraversion (β = .27, p < .001) yielded significant relationships with PSS-AL in the multivariate model.
One-way ANOVAs revealed that participants with high PSS-AL reported significantly greater physical health, F(2, 197) = 4.57, p = .011, η2 = .04; mental health, F(2, 197) = 13.24, p < .001, η2 = .12; co-resident intimacy, F(2, 197) = 4.87, p = .009, η2 = .05; staff-resident intimacy, F(2, 197) = 5.60, p = .004, η2 = .05; and extraversion, F(2, 197) = 12.45, p < .001, η2 = .11, compared to residents with low PSS-AL; see Table 2.
Group Differences Between Low, Medium, and High Ranked Residents.

Note. * p < .05. ** p < .01. *** p < .001.
a = significant compared to low PSS-AL.
Qualitative Analyses
Participants who responded to open-ended questions ranged in PSS-AL from 1 to 10 (n = 176, M = 6.99, SD = 2.10); 38 (22%) rated PSS-AL as low, 95 (54%) rated PSS-AL as medium, and 43 (24%) rated PSS-AL as high. Participant responses contained 311 codes, representing 58 (19%) codes for participants with low, 156 (50%) codes for participants with medium, and 97 (31%) codes for participants with high PSS-AL ratings.
Three main categories emerged from the coded data: inter-personal factors, prosocial behaviors, and health and ability. Primary categories were determined based on frequency and substantial reflection in the data (Hsieh & Shannon, 2005). All categories, including those that were less frequent and reflected in the data, are presented in Table 3.
Qualitative Open-Ended Responses: Reasons for PSS-AL Ratings.

Note. Some participant responses contained multiple themes. Percentages were calculated with the number of themes for each category.
In the inter-personal category of codes, participants discussed the sources, processes, and depth of inter-personal relationships, mostly with co-residents and staff within their AL, as reasons for PSS-AL ratings. For example, one participant stated, “I’m well-liked by staff and other residents (PSS-AL = 8).” Depth of relationships also emerged in open-ended responses, with participants differentiating between knowing names and intimate details about others in their community. For example, participants stated, “I don’t know anything about anyone, and I’m embarrassed by that (PSS-AL = 3),” and “I only know a few people and those I do, it’s not an intimate relationship (PSS-AL = 6).” Participants also discussed the importance of skills that contributed to social abilities and personality characteristics that made it easier to build relationships with others. For example, participants stated, “I listen to really get to know people (PSS-AL = 10),” and, “I don’t like to socialize (PSS-AL = 3).”
Another category of codes related to prosocial behaviors. This category included acting in accordance with perceived social expectations, as well as behaviors consistent with being a “good” person or resident. Some participants discussed not meeting perceived expectations (e.g., “I’m not very into this place, I got no spirit [PSS-AL = 7]”). However, many participants mentioned meeting or exceeding perceived social expectations within their AL, often related to helping behaviors (e.g., “I help others…staff come to me for help [PSS-AL = 10]”). A few participants referenced deference or not causing trouble in the community. For example, one participant stated, “I’m nice…I don’t cause problems by asking too much of staff (PSS-AL = 6).” In addition, some participants discussed involvement in service roles within their AL; for example, “I’m the chairman of resident council and am vocal in the community (PSS-AL = 9),” and “I was asked to be a greeter to new residents, I help others feel welcome (PSS-AL = 8).”
Another category that emerged from the coded data related to health and ability. This category included physical, cognitive, sensory, and emotional health, as well as the ability to communicate. Many participants reported that high physical and cognitive ability was their reason for a high PSS-AL rating; for example, “[My] mental ability is higher than most (PSS-AL = 10),” and “I’m still able to communicate, think, and walk (PSS-AL = 10).” A few participants described their health as either facilitating or hindering social relationships, exemplifying the inter-related nature of categories. For example, a participant noted, “I can’t hear anyone, I just hear ‘blah, blah, blah’ (PSS-AL = 1).”
Additional codes related to individual characteristics, such as: life accomplishments, skills or talents, intelligence or knowledge, physical appearance, socioeconomic status, or education as reasons for PSS-AL ratings. However, these codes were less common and often enveloped in larger categories. For example, participants mentioned individual characteristics in tandem with health attributes, like cognitive ability (e.g., “I have skills and talents like trivia…I know more than the others [PSS-AL = 9]”). In another example, participants discussed individual characteristics in the context of relationship building: “I have a lot of experience with work to share with others (PSS-AL = 9).”
Discussion
By triangulating quantitative and qualitative data, this study offers an in-depth description of PSS-AL. In quantitative analyses, health and social factors yielded significant relationships with PSS-AL. In qualitative analyses, inter-personal factors, prosocial behaviors, and health and ability emerged as key determinants of PSS-AL ratings. Similarities across quantitative and qualitative findings highlight the relationships between PSS-AL, social, and health factors. Differing results revealed additional relevant constructs that were not captured in quantitative analyses, like prosocial behaviors. Overall, findings suggest that health abilities and social factors, particularly intimate relationships within the AL community and an outgoing personality, strongly relate to PSS-AL.
Inter-personal factors, like relationships, extraversion, and prosocial behaviors, strongly related with PSS-AL in the current sample. AL is a socially demanding communal-living environment in which residents with diverse attributes regularly interact with co-residents and staff. In this environment, residents with advanced social skills, outgoing personalities, and health factors that support sociability may be more likely to build high social standing within the community. Conversely, residents with limited capacity or desire for sociability may experience negative psychosocial consequences related to low social standing. Further, in AL, services that aim to promote quality of life often involve a high amount of social engagement (e.g., programmed activities; Plys, 2019). Therefore, additional attention is needed to investigate quality of life promoting services for residents with limited social abilities (e.g., cognitive or sensory limitations affecting community abilities) or interests in socializing (e.g., introverted residents).
Staff-resident relationships emerged as a key correlate of PSS-AL in the current study. In fact, staff-resident intimacy, mental health, and extraversion were the only factors yielding significant relationships with PSS-AL in a multivariate model. Therefore, it is possible that staff-resident relationships may have an important role in maintaining or disrupting social hierarchies in AL. For example, staff may knowingly or unknowingly demonstrate preference for residents with high levels of functional ability, socially engagement, and cooperation, thus, reinforcing hierarchical social structures in the community. This example is similar to previous research in classrooms which suggests that teachers may contribute to the formation and-or reinforcement of hierarchies through demonstrating preferences for academically-talented students (Mikami et al., 2012). However, to the knowledge of the authors, the role of staff in forming, maintaining, and-or disrupting resident social hierarchies has yet to be investigated in the AL setting. Additional research is needed to address the potential psychosocial implications of staff-resident interactions.
Clinical Implications
Interventions designed to address potentially damaging social hierarchies often target the social context of classrooms. These interventions typically incorporate social skills training, teacher education, or cooperative learning (Farmer et al., 2018). Applied to AL, this literature suggests that interventions at the resident-, staff-, and community-level may help address potentially damaging social dynamics and resident hierarchies. Specifically, AL residents may benefit from education on communication skills for engaging with individuals of various levels of cognitive and sensory abilities. In addition, staff may benefit from skills training to increase positive interactions with all residents. This may include building awareness of explicit and implicit actions that can influence whether residents of varying health or social abilities feel valued and influential within the community. Lastly, cooperative or shared goals within an AL may help disrupt social hierarchies. This may involve initiatives that define appropriate roles for each community member, such as a service project. Future research is needed to investigate the feasibility and impact of the aforementioned interventions in AL, particularly in communities that offer services to residents with a range of physical, cognitive, sensory, and social abilities.
Research Implications
Additional research is needed to investigate factors that relate to the development, maintenance, and-or disruption of social hierarchies in AL. By reporting cross-sectional correlates of PSS-AL, the current study is a first step in this area of research. Yet, the literature on this topic is still in its nascency. Our results suggest that social skills and prosocial behaviors, as well as health abilities that support these factors, may be important to consider in future studies. One potential direction for this body of research may involve investigating the impact of resident variability or staff and resident turnover on social hierarchies in AL.
Another interesting area of future research is to compare ratings and correlates of perceived social standing across different social contexts throughout the lifespan. For example, our findings are consistent with previous research that found social skills, prosocial behaviors, and health positively related with social standing among children and adolescents in classrooms as well as young adults in the workplace (Koski et al., 2015; Scott & Judge, 2009). On the other hand, previous studies found that social standing in childhood and adolescence also related to antisocial behaviors, visibility, and body composition (Koski et al., 2015). These findings differ from the current sample of older adults in AL, which found that PSS-AL related to prosocial behaviors, deference, and health factors that aided sociability like hearing and cognition. Therefore, the current findings may offer guidance for future works investigating similarities and differences in factors related to social standing across various contexts and life stages. Specifically, given that our findings highlight the salience of social gratification, generativity, and function for PSS-AL, it is possible that lifespan developmental theories like Gerotranscendence (Tornstam, 1997) or Socioemotional Selectivity Theory (Carstensen et al., 1999) may provide relevant frameworks for future studies.
Limitations
The current study has limitations that should be addressed in future research. First, a non-representative sample likely influenced our results. Most importantly, we excluded residents with significant cognitive impairment. The cognitive ability of the current sample varied, with at least 36% of the total sample evidencing a level of cognitive impairment consistent with neurocognitive disorder; however, national estimates suggest that 42% of AL residents have a neurocognitive disorder (Khatusky et al., 2016). Therefore, the current sample was not representative of the full range of cognitive abilities in AL. This, coupled with recruitment strategies that may have targeted residents who are more outgoing (e.g., staff nominations and in-person announcements at common activities), suggests that the current study may not have fully captured the voice of residents with the lowest social standing in their AL community. Therefore, the strength of relationships and factors emerging from this study may not be generalizable to all AL residents. In addition, the current sample may have evidenced a restricted range on certain measures (e.g., CDT), which could have impacted statistical analyses. Taken together, future research is needed to investigate PSS-AL with a more representative sample of AL residents. One method to address this limitation in future research may be to employ a mixture of peer- and staff-informant ratings of social standing, consistent with literature on sociometric status (Jiang & Cillessen, 2005). However, additional research is needed to investigate the feasibility and validity of these types of ratings in AL.
Another limitation is that this study sampled ALs from a similar geographic region. Future research may choose to investigate social dynamics in different regions of the United States and internationally to explore the impact of cultural influences on PSS-AL. Further, the self-anchoring ladder used in the current study was not previously validated for perceived social standing in AL communities. Additional research is needed to establish validity of a self-anchoring ladder in AL. In addition, we did not audio record responses to open-ended questions, limiting our ability to crosscheck transcriptions of open-ended responses. Lastly, the current study is cross-sectional and, therefore, we cannot infer causal relationships.
Conclusion
This study contributes to the AL literature by providing an in-depth investigation of PSS-AL and, in doing so, offers insights into social hierarchies among residents. A growing body of literature suggests that perceived community social standing has implications for health and well-being in older adulthood (Demakakos et al., 2018), including in residential care settings (Ayalon, 2019). This study fills a gap in the literature by addressing the determinants and correlates of perceived social standing in a sample of AL residents. In summary, social relationships, extraversion, prosocial behaviors, and health factors related to PSS-AL in the current sample. Findings also suggest that staff-resident relationships may be an important area to target in future psychosocial research. Results from the current study provide various avenues for future research to advance developmental perspectives on social standing and social hierarchies, as well as to contribute to the understanding of social dynamics in the AL setting. Findings may also have clinical implications in AL by informing future studies investigating individual-, staff-, or community-level interventions to address potentially harmful social hierarchies among residents.
Supplemental Material
Supplemental Material, APPENDIX - Perceived Social Standing in Assisted Living Communities: A Mixed-Methods Study of Social Hierarchies Among Residents
Supplemental Material, APPENDIX for Perceived Social Standing in Assisted Living Communities: A Mixed-Methods Study of Social Hierarchies Among Residents by Evan Plys and Rachel Johnson-Koenke in Research on Aging
Footnotes
Acknowledgments
We are grateful to Dr. Sara Qualls for feedback that greatly improved this manuscript and for her ongoing mentorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part [EP] by a training grant from the National Institute on Aging, award number T32AG044296.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.