
Abstract
Older LGBTQ adults face elevated risk for subjective cognitive decline (SCD), yet variation by sexual orientation and gender identity (SOGI) remains underexplored. Guided by minority stress theory, we analyzed Wave 1 data from the LGBTQ Social Networks, Aging, and Policy Study (QSNAPS), a nonprobability panel of 1,255 LGBTQ adults aged 50–76 years in four Southern states. SCD was assessed using a 15-item index capturing any, mild, and severe cognitive difficulties. Logistic regression estimated adjusted predicted probabilities of SCD by SOGI, controlling for sociodemographic characteristics, HIV status, and state. Overall, 40% reported any SCD, 11% mild SCD, and 4% severe SCD. Bisexual and transgender/gender diverse participants had significantly higher probabilities of any SCD than gay/lesbian and cisgender peers. Findings reveal substantial heterogeneity in cognitive health within older LGBTQ populations, highlighting the need for targeted, SOGI informed dementia prevention and mental health interventions in the US South.
Keywords
Introduction
As global populations age, the prevalence of memory issues, subjective cognitive decline, and dementias such as Alzheimer’s disease is becoming a major public health concern. Within this broader trend, lesbian, gay, bisexual, transgender, and queer (LGBTQ+) older adults represent a rapidly growing and notably diverse segment of the senior population, with emerging research revealing that they may be at heightened risk for cognitive impairment and memory-related conditions compared to their heterosexual and cisgender peers (Dragon et al., 2017; Flatt et al., 2021; Sage and Alzheimer’s Association, 2018). Studies using both population-based surveys and clinical cohorts suggest that sexual and gender minority (SGM) adults not only show a higher prevalence of subjective cognitive complaints and functional limitations due to cognitive difficulties but also carry a disproportionate burden of risk factors for dementia including elevated rates of depression, social isolation, cardiovascular diseases, diabetes, and minority stress (Fredriksen-Goldsen et al., 2018; Hsieh et al., 2021; Romanelli et al., 2024). While findings across the literature remain complex, with some studies reporting higher rates of objective cognitive impairment and dementia among LGBTQ + individuals (particularly transgender adults) (Dragon et al., 2017; Guo et al., 2022), and others finding no significant differences after adjustment for confounders (Perales-Puchalt et al., 2019), there is a broad consensus that the intersection of social disadvantage, health disparities, and lifetime exposure to stigma plays a critical role in shaping cognitive health trajectories in this population.
It is estimated that by 2030 there will be 6 million older adults in the United States that identify as being LGBTQ+ and nearly 1 million of them will be diagnosed with ADRD (Fredriksen-Goldsen et al., 2018). Older LGBTQ adults are vulnerable to sociocultural factors that put them at higher risk for subjective cognitive decline. They are more likely to experience lifetime victimization of violence discrimination, and stigmatization, to be exposed to minority stress, to have higher rates of financial instability and to encounter social barriers to healthcare compared to their straight and cisgender counterparts (Casey et al., 2019; Fredriksen-Goldsen et al., 2013, 2015). Overall cognitive impairments within older LGBTQ + groups and has been partially attributed chronic depressive symptoms that older LGBTQ + adults may have experienced over their lifetime (Hsieh et al., 2021). These studies describe how the presence of chronic mental illnesses such as depression is a major risk factor for developing dementia and other cognitive impairments (Byers & Yaffe, 2011; Richard et al., 2013). While many studies provide evidence of higher rates of SCD and cognitive impairment for older LGBTQ + adults individuals (Akre et al., 2024; Fredriksen-Goldsen et al., 2022), these studies merged groups that assume homogeneity and elide differences across sexual orientation and gender identity. While this practice increases the statistical power of the analysis, it prevents the identification of potential variations in rates of SCD within LGBTQ + subgroups.
Minority stress theory provides a useful framework for understanding elevated dementia risk among LGBTQ + older adults by situating cognitive aging within a lifelong context of chronic, stigma related stress exposure. Minority stress refers to the additive burden of distal stressors such as discrimination, victimization, and structural exclusion, and proximal stressors such as internalized stigma and concealment, that accrue due to a marginalized sexual or gender identity and can dysregulate neuroendocrine and cardiovascular systems implicated in cognitive decline. (Meyer, 2003; Zhong et al., 2026). These processes are salient for LGBTQ + older adults, who experience higher rates of depression, loneliness, and social isolation, as well as disproportionate burdens of cardiovascular disease, diabetes, and disability, which are established risk factors for ADRD (Fredriksen-Goldsen et al., 2013, 2015; Meyer, 2003). Chronic minority stress in later life has been linked to poorer self-rated health, more chronic conditions, and elevated subjective cognitive difficulties among LGBTQ + elders, suggesting that sustained exposure to stigma related stress may accelerate brain aging and heighten vulnerability to ADRD (Fredriksen-Goldsen et al., 2018; Meyer, 2003; Zhong et al., 2026). At the same time, minority stress theory emphasizes the importance of resilience, coping resources, and affirming social networks, which may buffer the cognitive consequences of chronic stress and represent modifiable targets for intervention to promote cognitive health equity in LGBTQ + aging populations.
Despite the evident heterogeneity within LGBTQ + communities, there is one study that explores differences in cognitive health within LGBTQ + communities, but this study only focuses on sexual minority women and does not include gender diverse individuals (Seelman, 2018). Furthermore, studies have not focused on this difference in the South Census region on the United States, an area with the highest rate of LGBTQ + identified individuals (Hasenbush et al., 2014; Jones, 2022, 2025; Pew Research Center, 2019; Thornton, 2023). Intersectional identities must also be taken into consideration when addressing memory issues within this population. Therefore, this study aims to systematically investigate variations in self-reported memory issues across distinct sexual orientation and gender identity groups, leveraging a novel dataset with robust identification of older LGBTQ + adults. Guided by minority stress theory, we hypothesize that individuals whose sexual orientations and gender identities are subject to greater societal stigmatization, discrimination, and lack of legal and policy protections will exhibit disproportionately higher rates of subjective memory problems, reflecting the compounded impact of minority stress and structural inequities on cognitive health (Dragon et al., 2017; Flatt et al., 2021; Sage and Alzheimer’s Association, 2018).
Methods
Data and Sample
We use the LGBTQ + Social Networks, Aging, and Policy Study (QSNAPS), a panel study of midlife and older LGBTQ adults (Q SNAPS). QSNAPS began collecting data in 2020 from 1,256 respondents between the ages of 50-76 who reside in Alabama, North Carolina, Georgia, and Tennessee to understand health, aging, and the social relationships that older LGBTQ, nonbinary, and gender non-conforming adults draw on for support. QSNAPS uses purposeful online and venue-based sampling, linked referrals and community outreach to LGBTQ + serving organizations to recruit participants. Wave 1 was fielded from April 1, 2020, to September 30, 2021. We dropped one observation because the respondent did not reside in the South Census region yielding an analytic sample including respondents who provided responses for the items that measure cognitive impairment (n = 1,255). This study was approved by the Vanderbilt University Institutional Review Board.
Outcome Measure
We measured cognitive health using a modified version of the Short Form of the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE), a widely used, validated instrument that is correlated with a range of objective cognitive tests and with cognitive decline over time (Jorm, 1994, 2004; Jorm et al., 2000; Li et al., 2012). The original Short Form IQCODE is a 16-item index in which informants rate changes in the respondent’s memory and day-to-day decision-making over the past two years on a 5-point scale (better, the same, or worse). In the QSNAPS survey, items from the Short Form IQCODE were adapted so that participants self-reported whether they experienced each difficulty using dichotomous response options (“Yes” = 1, “No” = 0); we then averaged responses across 15 items to create a continuous index of subjective cognitive difficulties. Respondents were asked to self-report “Yes” or “No” to survey items that explored difficulties like “understanding what’s going on and reasoning things through,” “remembering recent events,” and “learning new things in general.” This instrument was validated in previous study on older LGBTQ + adults (Barbee et al., 2024).
Prior validation studies of the IQCODE indicate that scores of approximately 3.19 or higher on the original 5-point scale are suggestive of mild cognitive impairment in community, non-hospital populations using the English-language questionnaire (Li et al., 2012). Because our items were dichotomized, we operationalized thresholds by approximating comparable levels of difficulty on the 0–1 scale and by emphasizing increasing burden across multiple domains of functioning. Specifically, any subjective cognitive difficulty was defined as endorsing at least one item. Mild cognitive impairment was defined as endorsing three or more difficulties, which represents a conservative threshold corresponding to multiple, recurrent problems rather than a single isolated complaint. Severe impairment was defined as endorsing five or more difficulties, capturing respondents with a more extensive pattern of daily cognitive challenges. These cut points therefore align our binary-item index with established IQCODE guidance while distinguishing gradations in the severity and breadth of subjective cognitive problems among older LGBTQ + adults. See Appendix A provides a comprehensive list of measures.
Key Explanatory Variables
We examine two key explanatory variables. First, we examine self-reported sexual orientation, defined as lesbian/gay, bisexual, or something else/do not know. To ascertain what respondents meant by “something else” they were asked the following: By something else do you mean that, (1) You are not straight, but identify with another label such as queer, trisexual, omnisexual, or pansexual; (2) You are transgender or transexual; (3) You have not or are in the process of figuring our your sexuality; (4) You do not think of yourself of having a sexuality; (5) You personally reject all labels of yourself; (6) You made a mistake and did not mean to pick this answer; and (7) You mean something else. No respondents selected option 6 and 5 respondents provided additional information about their sexual orientation.
Second, we examine self-reported gender identity which we define as cisgender (gender identity is the same as sex assigned at birth) and transgender/gender diverse. We define transgender/gender diverse as individuals who self-report identifying as transgender or gender non-conforming (neither man nor women, nonbinary, no gender).
Additional Explanatory Variables
We examine the following demographic characteristics: age (50-54, 55-59, 60-64, 65-69, and 70-76), race and ethnicity (Non-Hispanic White, Non-Hispanic Black, Latino/Hispanic – any race, Non-Hispanic Asian, and Other/Multiracial), highest level of education (Less than Bachelors, Bachelors, more than Bachelors), sex at birth (male/female/intersex). We also examine whether a respondent has access to LGBTQ + affirming care and current HIV status (HIV positive/not HIV positive).
Empirical Approach
First, we describe the sociodemographic characteristics, sexual orientation, gender identity, and memory issues in the overall sample. Then we describe the sociodemographic characteristics of the sample by sexual orientation and gender identity. We test for differences in characteristics using Chi Square tests for all categorical variables and ANOVA for continuous variables compared across three groups.
Descriptive Statistics
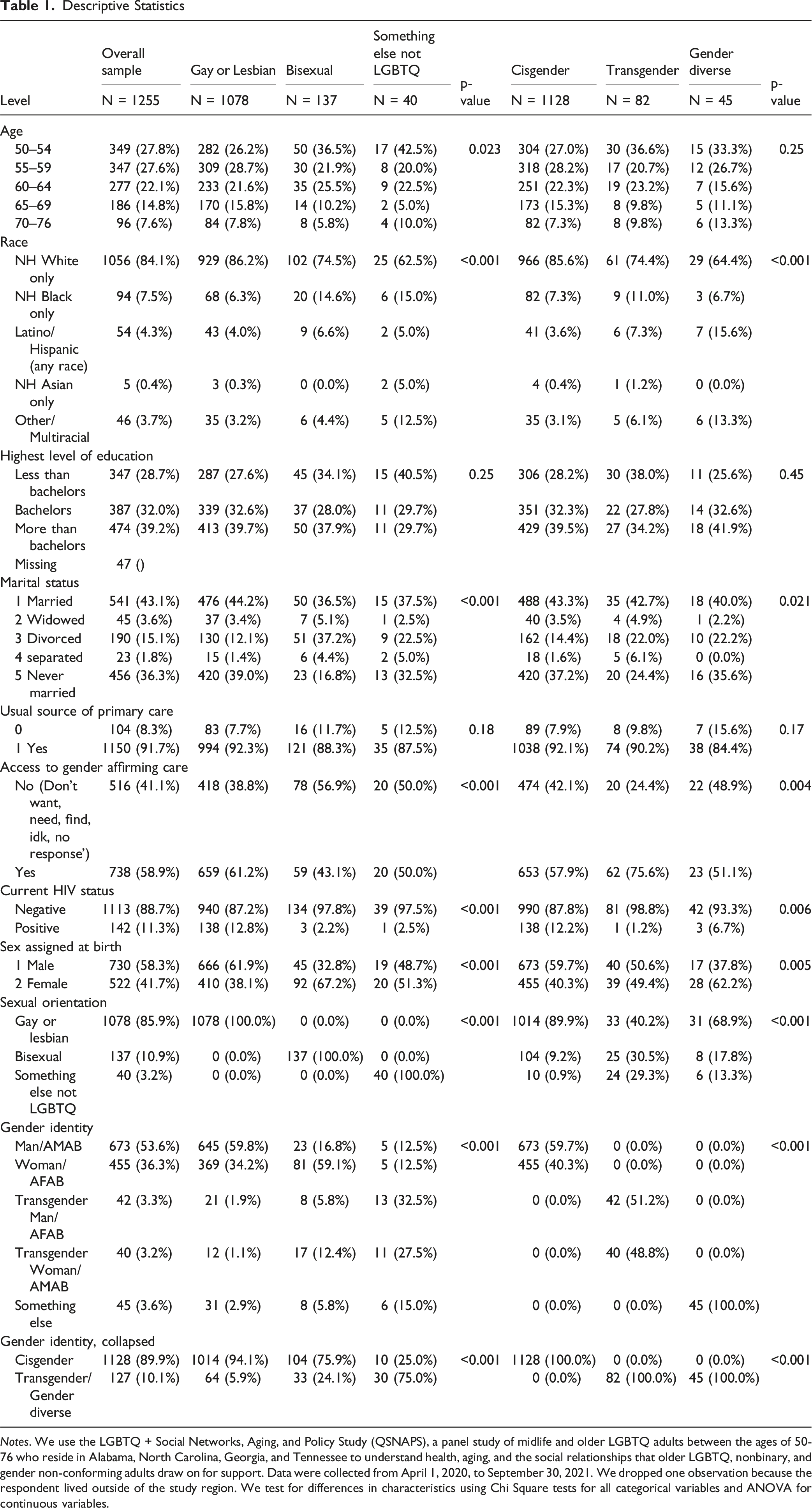
Notes. We use the LGBTQ + Social Networks, Aging, and Policy Study (QSNAPS), a panel study of midlife and older LGBTQ adults between the ages of 50-76 who reside in Alabama, North Carolina, Georgia, and Tennessee to understand health, aging, and the social relationships that older LGBTQ, nonbinary, and gender non-conforming adults draw on for support. Data were collected from April 1, 2020, to September 30, 2021. We dropped one observation because the respondent lived outside of the study region. We test for differences in characteristics using Chi Square tests for all categorical variables and ANOVA for continuous variables.
Results
Descriptive Statistics
Among the overall sample, we find respondents are more likely to be aged 50-60 (55.4%), non-Hispanic white (84%), not married (57%), have a usual source of care (92%), have full-time employment (50%), and are not HIV positive (89%), see Table 1. We observe 86% of the sample self-identifies as lesbian/gay, 11% as bisexual, and 3% as “something/don’t know/not LGBTQ”. We observe 54% of the sample reports being male/assigned male at birth, 36% as female/assigned female at birth, 2.3% as transgender man, 4% as transgender woman, and 3.7% as gender non-conforming. Approximately 40% of the total sample screened positive for any subjective cognitive decline while 11% meet the threshold for mild cognitive decline.
When examining the sample characteristics by sexual orientation, we see that compared to individuals who are bisexual or something/don’t know/not LGBTQ individuals who are lesbian/gay are slightly younger and more likely to be non-Hispanic white, married, have a usual source of care, and report being HIV positive, identify as male/assigned male at birth, to have subjective cognitive decline and mild cognitive impairment (Table 1).
When examining the sample characteristics by gender identity, we observe transgender men are the youngest group while male/assigned male at birth and female/assigned female at birth are the oldest groups. Individuals who are male/assigned male at birth or female/assigned female at birth are disproportionately non-Hispanic white compared to individuals identifying as transgender men, transgender women, or gender non-conforming (Table 1).
Percent of Respondents With Cognitive Problems/Impairment Across Sexual Orientation and Gender Identity
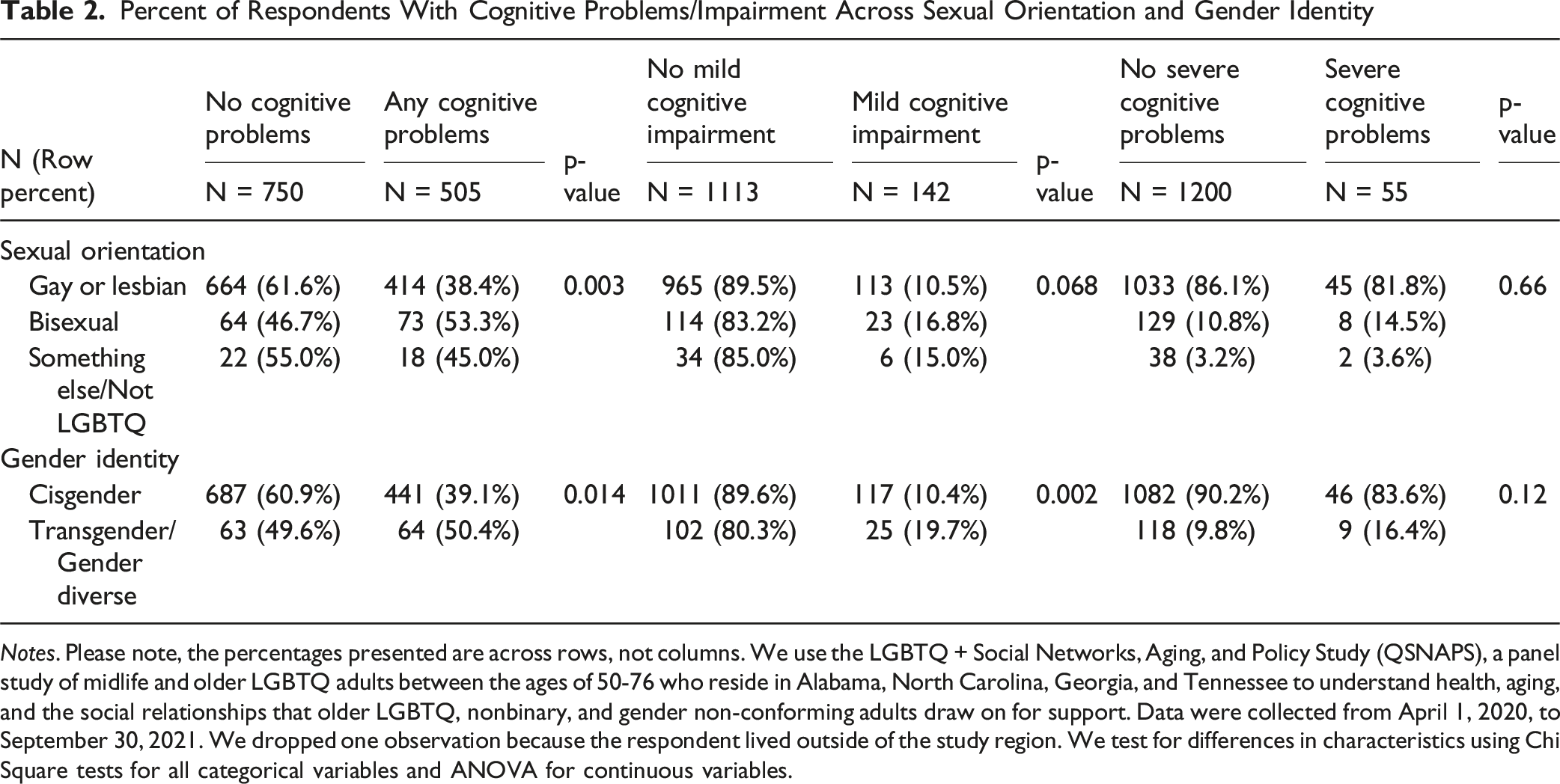
Notes. Please note, the percentages presented are across rows, not columns. We use the LGBTQ + Social Networks, Aging, and Policy Study (QSNAPS), a panel study of midlife and older LGBTQ adults between the ages of 50-76 who reside in Alabama, North Carolina, Georgia, and Tennessee to understand health, aging, and the social relationships that older LGBTQ, nonbinary, and gender non-conforming adults draw on for support. Data were collected from April 1, 2020, to September 30, 2021. We dropped one observation because the respondent lived outside of the study region. We test for differences in characteristics using Chi Square tests for all categorical variables and ANOVA for continuous variables.
Regression Results: Any Cognitive Problems
After adjusting for sociodemographic characteristics and state fixed effects, we find that individuals who are bisexual have an average predicted probability of 0.510 (95% CI: 0.421, 0.598), individuals who are gay or lesbian have an average predicted probability of 0.388 (95% CI: 0.358, 0.417), and individuals who are something else/not LGBTQ have an average predicted probability of 0.412 (95% CI: 0.0.249, 0.575) of having any cognitive impairment (Figure 1), Compared to people who are gay or lesbian, individuals who are bisexual have a 12.2 percentage point increase in the predicted probability of having any cognitive problems (p = 0.012). When comparing people who are gay or lesbian to those who report their sexual orientation as “something else/do not know”, we find no evidence of a significant difference in the predicted probability of having any cognitive impairment. Predicted probability of any cognitive impairment by sexual orientation and gender identity.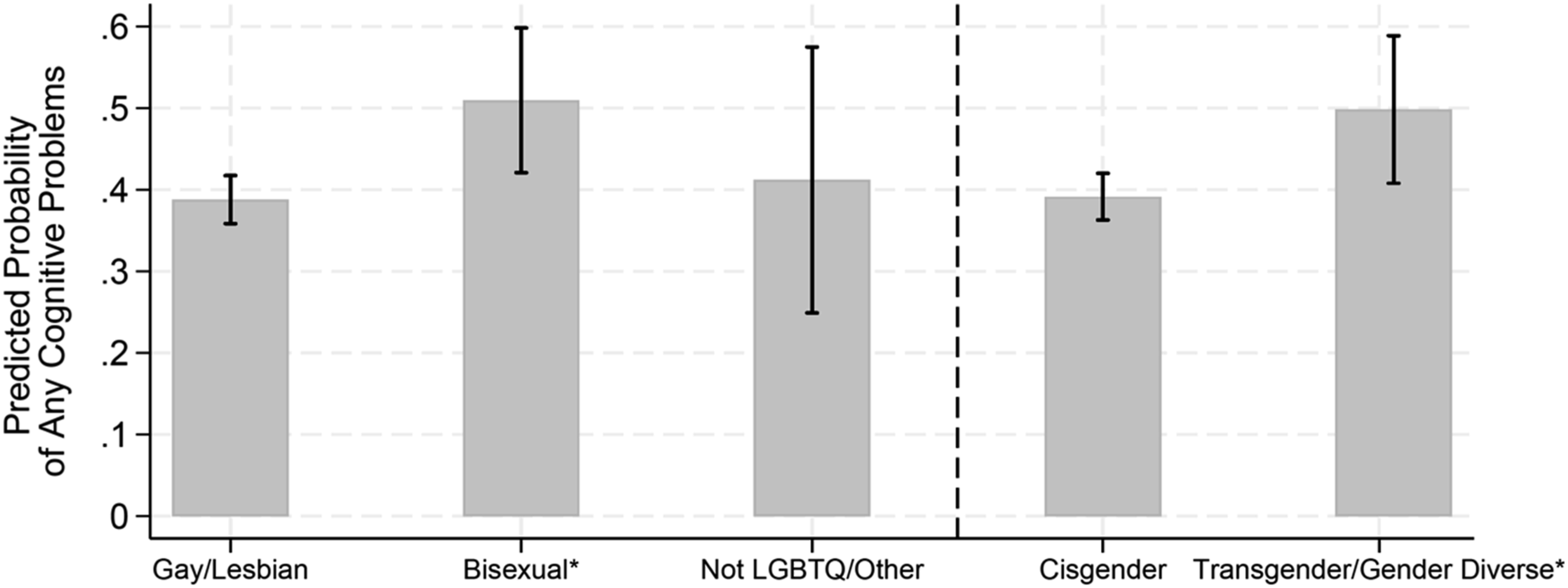
After adjusting for sociodemographic characteristics and state fixed effects, we find that individuals who are cisgender have an average predicted probability of 0.391 (95% CI: 0.363, 0.420) and individuals who are transgender/gender diverse have an average predicted probability of 0.498 (95% CI: 0.408, 0.589) of having any cognitive impairment (Figure 1). Compared to people who are cisgender, individuals who are transgender/gender diverse have a 10.7 percentage point increase in the predicted probability of having any cognitive problems (p = 0.028) Figures 2 and 3. Predicted probability of mild cognitive impairment by sexual orientation and gender identity. Predicted probability of severe cognitive impairment by sexual orientation and gender identity.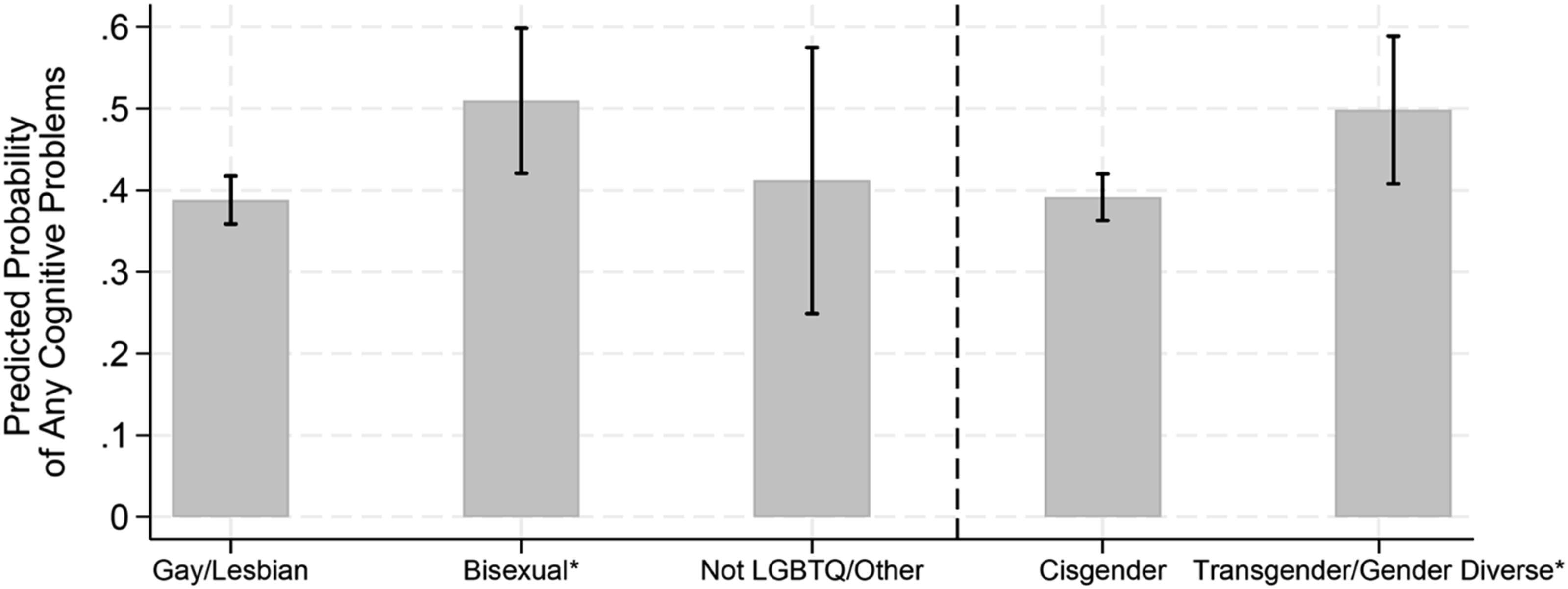
Regression Results: Mild Cognitive Impairment
After adjusting for sociodemographic characteristics and state fixed effects, we find that individuals who are bisexual have an average predicted probability of 0.160 (95% CI: 0.096, 0.225), individuals who are gay or lesbian have an average predicted probability of 0.109 (95% CI: 0.090, 0.128), and individuals who are something else/not LGBTQ have an average predicted probability of 0.126 (95% CI: 0.022, 0.230) of reporting mild cognitive impairment. Compared to people who are gay or lesbian, we find no evidence of a significant association of bisexuality with a difference in the predicted probability of having mild cognitive decline.
After adjusting for sociodemographic characteristics and state fixed effects, we find that individuals who are cisgender have an average predicted probability of 0.107 (95% CI: 0.089, 0.125) and individuals who are transgender/gender diverse have an average predicted probability of 0.190 (95% CI: 0.120, 0.261) of reporting mild cognitive impairment. Compared to people who are cisgender, individuals who are transgender/gender diverse are 8.3 percentage point increase in the predicted probability of having any cognitive problems (p = 0.026).
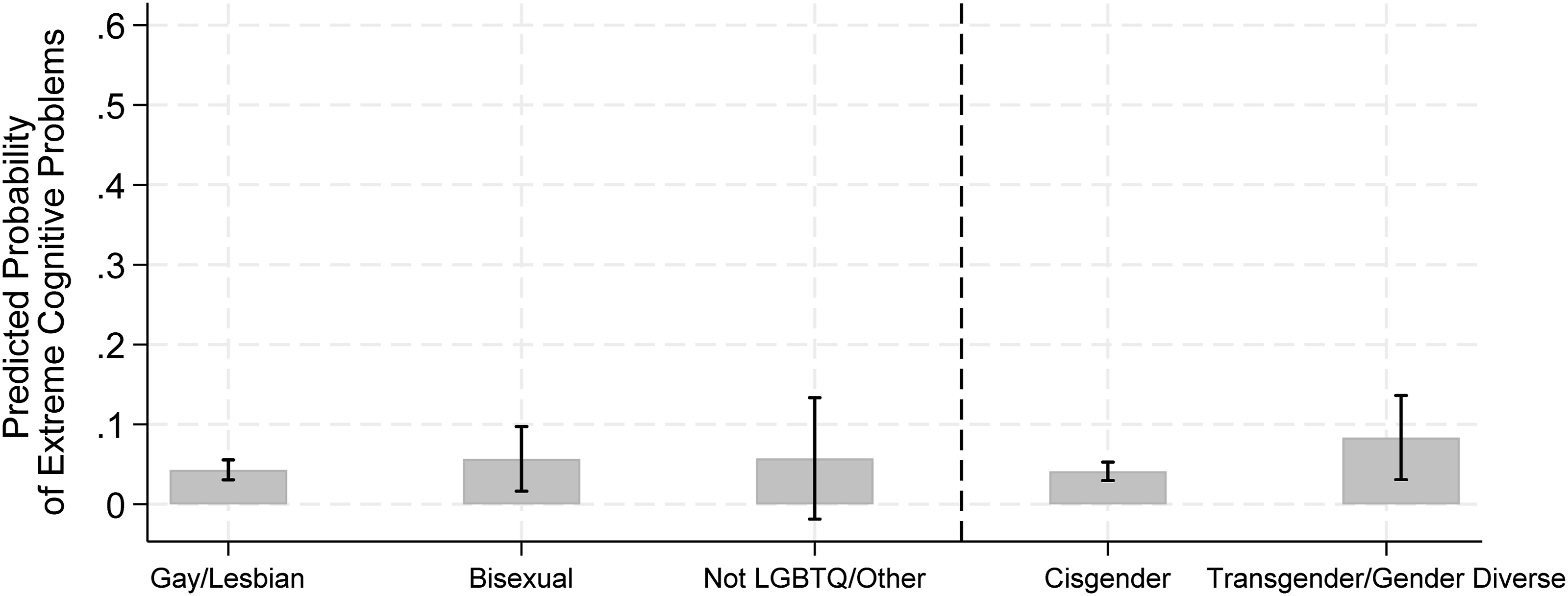
Regression Results: Extreme Cognitive Impairment
After adjusting for sociodemographic characteristics and state fixed effects, regression models dropped 5 observations due to race perfectly predicting the outcome. We find that individuals who are bisexual have an average predicted probability of 0.057 (95% CI: 0.016, 0.097), individuals who are gay or lesbian have an average predicted probability of 0.043 (95% CI: 0.031, 0.055), and individuals who are something else/not LGBTQ have an average predicted probability of 0.057 (95% CI: −0.019, 0.133) in the probability of having extreme cognitive impairment. Compared to people who are gay or lesbian, we find no evidence of an association that individuals who are bisexual have a significant difference in the predicted probability of having extreme cognitive decline.
Individuals who are cisgender have an average predicted probability of 0.041 (95% CI: 0.030, 0.053) and individuals who are transgender/gender diverse have an average predicted probability of 0.083 (95% CI: 0.031, 0.136) of extreme cognitive impairment. Compared to people who are cisgender, we find no evidence of an association that individuals who are transgender/gender diverse have significant differences in the predicted probability of having extreme cognitive decline. Predicted probabilities of outcomes variables across sexual orientations and gender identities was included in Appendix B.
Discussion
The purpose of this study was to identify variation in levels of cognitive issues in older LGBTQ + adults across sexual orientation and gender identity. Using a novel data set, QSNAPS, which used multistage question to ascertain sexual orientation and gender identity (Cahill et al., 2016) our study demonstrates that there are significant differences in experiences of cognitive impairment across sexual orientation and gender identity. The findings of this study underscore persistent disparities in cognitive health among SGM populations, particularly bisexual and transgender/gender diverse individuals, compared to their gay/lesbian and cisgender peers. These results resonate with and extend the existing literature documenting higher rates of subjective cognitive decline and cognitive impairment among older LGBTQ + adults (Correro & Nielson, 2020; Flatt et al., 2021; Frost & Meyer, 2023; Manca et al., 2024; Meyer, 2003). Several broad patterns emerge, warranting both sociocultural interpretation and targeted policy interventions.
The elevated risk of cognitive problems among bisexual and transgender/gender diverse individuals may be attributed to several interrelated factors. One study demonstrated that sexual minority older adults had slightly better episodic memory than heterosexual peers and minority stress uniquely predicted lower fluid intelligence only among sexual minority participants (Manca & Venneri, 2023). Minority stress theory provides a compelling framework, positing that chronic exposure to stigma, discrimination, and social exclusion imposes both physiological and psychological tolls. These stressors are linked to neurobiological mechanisms such as elevated cortisol and other stress hormones, which can negatively affect cognitive aging through their neurotoxic impact on the brain’s hippocampus and prefrontal cortex, regions vital for memory and executive function (Correro & Nielson, 2020). Empirical research supports that SGM individuals report not only more SCD but also an accelerated trajectory of cognitive decline, plausibly mediated by stress (Cicero et al., 2023).
Furthermore, mental health factors may be particularly salient in illuminating these disparities. Studies show that SGM populations, and especially bisexual individuals, consistently display higher rates of depression and anxiety, conditions well-known to be associated with poorer cognitive outcomes in later life (Hsieh et al., 2021; Liu et al., 2021; Robertson et al., 2021). For example, recent research indicates that depressive symptoms are among the strongest predictors of cognitive disadvantage in lesbian, gay, and bisexual people, hinting that the excess burden of cognitive impairment is at least in part psychological in origin (Hsieh et al., 2021).
Social determinants of health, such as reduced access to culturally competent healthcare, greater social isolation, and experiences of discrimination, further exacerbate these disparities. Older LGBTQ + adults are more likely to rate their health as poor, to suffer from chronic conditions, and to experience disability, which may compound risk for cognitive decline (Dawson et al., 2023; Lampe et al., 2024). For transgender and gender diverse people, exposure to prejudice can make it difficult to access necessary care, and many face higher prevalence of known dementia risk factors such as cardiovascular disease, diabetes, and substance use disorders. Barriers to health care, including poverty, lack of insurance, and discrimination by providers, further reduce opportunities for early detection and management of cognitive problems (Dawson et al., 2023, 2024; Serchen et al., 2024).
At the policy level, it is crucial to enact antidiscrimination laws that strengthen protections for LGBTQ + people across settings, ensuring equal access to care, employment, housing, and social support (Serchen et al., 2024; Tran & Gonzales, 2025). Robust data collection on sexual and gender identity within health surveys and clinical care is needed to identify and track disparities over time, which can inform targeted interventions (Cicero et al., 2023; Tran & Gonzales, 2025). Health systems should prioritize cultural competence training for all providers, ensuring affirming, inclusive, and stigma-free environments for LGBTQ + people (Cicero et al., 2023; Serchen et al., 2024). Expanding access to mental health support and developing tailored interventions to address the psychological burdens facing bisexual and transgender/gender diverse individuals are warranted, given the strong links between mood disorder and cognitive outcomes (Correro & Nielson, 2020; Hsieh et al., 2021). Furthermore, increasing research aimed at disentangling the contributions of psychosocial risk, minority stress, and clinical risk factors will help refine prevention and intervention strategies.
This study makes several unique contributions to the literature on cognitive aging among LGBTQ adults. Using QSNAPS, a large regional panel of midlife and older LGBTQ adults in the US South, the analysis provides rare, subgroup specific estimates of subjective cognitive decline that distinguish both sexual orientation and gender identity. By examining multiple levels of self-reported cognitive difficulties and linking them to minority stress theory, the study offers a more nuanced understanding of how stigma related exposures may produce heterogeneous cognitive risks across bisexual, transgender and gender diverse, and gay and lesbian older adults. These findings highlight both the necessity and the opportunity to reduce cognitive health disparities in sexual and gender minority populations. Solutions require a coordinated, multisectoral response—including legal, health system, and community-level actions—to foster environments where all older adults can achieve optimal cognitive and overall well-being. Continued efforts in research, inclusive data collection, and culturally responsive care will be essential to address and ultimately eliminate these deeply rooted inequities.
Limitation
As with any research, our study is not without its limitations. First, in our analytic sample, the oldest participant was 76 years of age; therefore, these findings may not be generalizable to adults in the oldest-old age groups, who may have different patterns of subjective cognitive decline and related risk factors. In addition, because our sample does not include individuals older than 76 and may underrepresent certain segments of the older adult population. Second, QSNAPS is a nonprobability, community-based panel of LGBTQ + adults aged 50–76 in Alabama, Georgia, North Carolina, and Tennessee, recruited through LGBTQ+ and aging organizations, community events, social networks, and targeted online advertisements. As such, the sample reflects older LGBTQ + adults who are connected to community networks and have access to online recruitment channels, rather than a probability sample of all LGBTQ + people in the U.S. South. Available comparisons with U.S. Census Household Pulse Survey data indicate that QSNAPS participants are broadly similar in age and gender composition but are more likely to have a college degree, and less likely to identify as bisexual or Latino/Hispanic, than LGBTQ + adults of the same ages in the region (Bureau, 2021). Consequently, our findings should be interpreted as describing this community-engaged cohort and may underestimate the burden of cognitive difficulties among more socioeconomically disadvantaged and racially and ethnically minoritized older LGBTQ + adults. In our sample, 8.2% of respondents aged 65 and older met criteria for mild subjective cognitive decline (82 per 1,000 adults 65+), a prevalence somewhat lower than population-based estimates for older adults (approximately 11–24%) (Salari et al., 2025). Third, the use of the modified IQCoDE instruction precludes this study from being able to capture more nuance for difficulties that are present as with the original IQCoDE instrument. The cross-sectional nature of the study prevents us from understanding causal relationships for variation in subjective cognitive impairment experiences with other individual, community, and health system factors that may influence cognitive health. Fourth, our outcome measures are based solely on self-reported cognitive difficulties without clinician confirmed diagnoses; while subjective cognitive decline is a recognized risk factor for later cognitive impairment, these data cannot determine whether participants have objectively verifiable cognitive deficits. Lastly, the sample consisted of primary gay, White, and AMAB respondents. Additional, efforts to oversample for gender non-conforming, bisexual and respondents of color is needed to make the sample more representative of the older LGBTQ + population in the US South.
Conclusion
This study highlights significant disparities in subjective cognitive impairment across sexual orientation and gender identity among older LGBTQ + adults, with bisexual and gender non-conforming individuals exhibiting the highest risks. The findings underscore the need for targeted, population-specific interventions to address the unique risks faced by these subgroups. Moreover, the lack of standardized, comprehensive SOGI data collection hampers efforts to accurately assess and address these disparities. National standards for SOGI data collection are essential to ensure inclusive public health strategies and interventions, particularly for those at heightened risk of cognitive decline.
Supplemental Material
Supplemental Material - Variation in Memory Issues Among Older Adults in the US South Based on Sexual Orientation and Gender Identity
Supplemental Material for Variation in Memory Issues Among Older Adults in the US South Based on Sexual Orientation and Gender Identity by Ellesse-Roselee Akré, Kate Miller, Harry Barbee, Regan Harnois, Ebony Toussaint, Tara McKay in Research on Aging.
Footnotes
Funding
Research reported in this publication was supported by the National Institute On Aging of the National Institutes of Health under Award Number R01AG063771. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.