
Abstract
The present study examined the concurrent and prospective, longitudinal effects of childhood negative emotionality and self-regulation on allostatic load (AL), a physiological indicator of chronic stress. We hypothesized that negative emotionality in combination with poor self-regulation would predict elevated AL. Mothers reported on children’s emotionality (N = 239, 116 males) at age 9, and self-regulation was measured at age 9 using a standard behavioural index of delay of gratification. AL was measured at ages 9 and 17. The AL measure captured hypothalamic pituitary adrenal axis, sympathetic adrenal medullary system, cardiovascular, and metabolic activity. Our results confirmed that negative emotionality prospectively predicted increases in AL, but only in children with low levels of self-regulation. The findings suggest that the link between negative emotionality and stress physiology is moderated by self-regulation and contribute to understanding the role of negative emotionality in physiological functioning throughout childhood and adolescence.
Chronic stress has become one of the most widely recognized psychosocial predictors of physical health (American Psychological Association, n.d.). Emotional and physiological arousal associated with stress response takes a toll on the body in adults as well as in children, eventually leading to illness (Cohen, Janicki-Deverts, & Miller, 2007; Shonkoff & Garner, 2012). However, the extent to which an individual is distressed by negative life events varies considerably among people and is believed to be determined, in part, by one’s personality (Semmer, 2006). In particular, negative emotionality—a predisposition to feelings such as fear, anxiety, irritability and frustration—is thought to exacerbate the effects of stress. However, evidence for the link between negative emotionality and objective biological indicators of stress physiology in children and adults is mixed, pointing to the need to rethink how we measure stress physiology as well as the importance of considering potential moderators (Jorgensen, Johnson, Kolodziej, & Schreer, 1996; Schmidt, Santesso, Schulkin, & Segalowitz, 2007).
Most negative emotionality and stress physiology studies have examined single indicators of physiological functioning. This is particularly problematic as emerging research on stress argues for the importance of simultaneously considering multiple indicators of stress physiology (McEwen, 2003). The present, prospective longitudinal study addresses these gaps in the literature by investigating the interaction between children’s negative emotionality and self-regulation in predicting allostatic load, a multisystemic physiological indicator of chronic stress. We hypothesized that negative emotionality will increase allostatic load in children, but only in conjunction with poor self-regulation.
Allostatic load as an indicator of chronic stress
During stress response, the sympathetic-adrenal medullary (SAM) system and hypothalamic-pituitary-adrenal (HPA) axis increase the secretion of catecholamines and glucocorticoids. These hormones in turn affect metabolic and cardiovascular systems in order to help the body mobilize energy to address increased environmental demands (McEwen, 2003).
While the stress response is adaptive in the short term, repeated or chronic over-activation of the SAM system and the HPA axis may lead to dysregulation of interconnected physiological systems, or allostatic load (McEwen & Stellar, 1993). Allostatic load (AL) may manifest itself in such changes as altered diurnal patterns of cortisol secretion, elevated systolic and diastolic blood pressure and visceral fat deposition (Juster, McEwen, & Lupien, 2010). Measures of allostatic load, derived from multiple biological markers, are designed to capture the multidimensionality of physiological changes resulting from chronic stress. Even when singular biological responses are modest and not predictive of health outcomes, the confluence of changes across multiple physiological systems presents a health risk (McEwen & Seeman, 1999; Seeman, Epel, Gruenewald, Karlamangla, & McEwen, 2010; Seeman, McEwen, Rowe, & Singer, 2001). Research has identified high levels of AL as risk factor for cardio-vascular disease, physical and cognitive decline later in life, and mortality (Karlamangla, Singer, & Seeman, 2006; Seeman et al., 2001).
Most existing studies of AL are cross-sectional studies focusing on adults. This research has identified multiple types of stressors as predictors of increased AL, including socio-economic adversity, work stress, social relations, as well as perceived stress (see Juster et al. 2010 for a review). However, AL theory provides a valuable framework for a life-course approach to predictors of long-term physiological functioning, morbidity and mortality (Danese & McEwen, 2012; Taylor, Way, & Seeman, 2011) as the focus is on mechanisms for how accumulation of stress throughout life can lead to poor health. This underscores the need for research on AL in childhood and adolescence, as well as early life precursors of AL; yet such empirical studies are still scarce.
Negative emotionality, stress, and stress physiology
The AL theory posits that the perception of stress, the intensity of stress response and the effects of stress on the body largely depend on a variety of factors, including personal experience, behavioural patterns and genetic make-up, as well as personality (McEwen, 1998). Personality—a set of stable characteristics that affect emotions, thoughts and behaviours—influences the appraisal of and coping with stressful life circumstances (Semmer, 2006) and thereby may moderate the effects of stress on the body (Kern & Friedman, 2011; Smith, 2006). Negative emotionality is one of the traits most often discussed in the stress literature. Specifically, negative emotionality is associated with more intense experience of stress (Ebstrup, Eplov, Pisinger, & Jørgensen, 2011). Predisposition to negative emotions manifests itself early in life and is regarded as a dimension of child temperament (Buss & Plomin, 1984; Kagan, 2008; Rothbart & Bates, 2006). As in adulthood, negative emotionality in childhood is associated with more intense experiences of stress (Compas, Connor-Smith, & Jaser, 2004; Lengua & Long, 2002).
A number of studies have investigated the link between negative emotionality and stress physiology in adults and children. Three cross-sectional studies have addressed the association between personality and AL in adults (Hawkley, Lavelle, Berntson, & Cacioppo, 2011; Kubzansky, Kawachi, & Sparrow, 1999; Sun, Wang, Zhang, & Li, 2007), finding that negative emotionality is a risk factor for increased AL. In addition, a number of studies have investigated the associations between negative emotionality and individual components of AL. In a comprehensive meta-analysis, Jorgensen et al. (1996) reviewed literature on the association between personality and blood pressure. While they find that negative emotionality is positively associated with blood pressure, they also note considerable heterogeneity in effect sizes, underscoring the need to test moderators in the personality–blood pressure relationship.
Researchers have also addressed the link between negative emotionality and HPA activity. Results from these studies are mixed as well. Several studies in children report an association between children’s negative emotionality and levels of salivary cortisol measured at a single time of the day (Schmidt, Fox, Rubin, Sternberg, Gold, Smith, & Schulkin, 2007; Schmidt et al., 1997, 2007). Some adult studies report a positive association between negative emotionality and measures of average daily exposure to cortisol (Nater, Hoppmann, & Klumb, 2010; Van Eck, Berkhof, Nicolson, & Sulon, 1996), while others find no such association (Adler, Wedekind, Pilz, Weniger, & Huether, 1997; Schommer, Kudielka, Hellhammer, & Kirschbaum, 1999). Findings regarding negative emotionality and other measures of HPA-axis activity, such as cortisol awakening response or cortisol reactivity to an acute stressor, have also been inconsistent (for a review, see Gunnar, 2001; Ormel et al., 2013).
The inconsistency of findings is partly explained by considerable variation in the assessment of both negative emotionality and physiological outcomes (Ormel et al., 2013). Research on the HPA axis in particular is characterized by great methodological variability, and the relationships between various cortisol measures remain to be clarified (Adam & Kumari, 2009; Clements, 2013). However, the lack of consistent findings may also indicate that the relationship between negative emotionality and stress physiology is affected by other factors and thus consideration of moderators is essential (Gunnar & Quevedo, 2007; Jorgensen et al., 1996; Schmidt et al., 2007). In the developmental literature, environmental factors, such as sensitive childcare, or social experiences, such as peer acceptance, have been found to modulate the effects of childhood temperament on physiological functioning (Gunnar & Donzella, 2002; Gunnar, Sebanc, Tout, Donzella, & van Dulmen, 2003; Hastings et al., 2011; Tarullo, Mliner, & Gunnar, 2011). Few studies, however, have considered the potential for negative emotionality to interact with other facets of children’s own personality. In this article, we explore the hypothesis that self-regulation, known to play an important role in stress response and coping, may be one personal attribute moderating the link between negative emotionality and physiological functioning.
Self-regulation as a potential moderator
Self-regulation is often defined as the ability to control attention and emotions, to plan, and to inhibit or initiate behaviours that are conducive to achieving one’s goals (Eisenberg, Champion, & Ma, 2004; Mischel & Ayduk, 2004). Although emotionality and self-regulation are often inversely related (Rothbart, Ellis, & Posner, 2004), researchers generally treat them as separate but interacting factors (Murphy, Eisenberg, Fabes, Shepard, & Guthrie, 1999). Indeed, an individual may tend to experience high levels of negative emotions, but be able to effectively regulate them, e.g., recover quickly from them or control the impulses to act upon them (Rydell, Berlin, & Bohlin, 2003). Moreover, theoretical proposals argue that regulatory mechanisms can modify and influence the development of reactive processes of temperament such as emotionality (Denissen, van Aken, Penke, & Wood, 2013).
Self-regulation skills involve top-down processes, which rely on the executive functioning network controlling attention. The activity in higher prefrontal cortex areas subserving executive functioning can attenuate the immediate emotional reactions arising at the fundamental levels of the brain (Ochsner & Gross, 2005). In particular, these top-down processes may modulate the activity of amygdala, which plays an important role in initiating physiological stress response. Thus executive functioning is believed to play an important role in reducing stress-reactivity and facilitating recovery from stress (Beckmann & Kellmann, 2004; Heatherton, 2011). Consistent with these theoretical proposals, research finds that self-regulatory skills correspond to better coping with everyday stress (Lengua, 2002; Lengua & Long, 2002) and better mental and physical health and adjustment in general (e.g., Doan, Fuller-Rowell, & Evans, 2012; Moffitt et al., 2011, Tagney, Baumeister, & Boone, 2004).
Furthermore, studies have found that self-regulation can attenuate the effects of negative emotionality on behavioural problems in childhood and early adolescence (Eisenberg, Fabes, Guthrie, & Reiser, 2000; Oldehinkel, Hartman, Ferdinand, Verhulst, & Ormel, 2007; Rothbart & Bates, 2006). These studies demonstrating the role of self-regulation in stress and the interactive effects of self-regulation and emotionality on psychological outcomes make self-regulation a likely candidate moderator of the link between emotionality and physiological functioning. Specifically, given the mixed evidence on the relationship between emotionality and physiological markers of stress reactivity, we hypothesized that that emotionality might only have detrimental effects on the body in conjunction with poor self-regulation. In other words, we reasoned that it may not be the propensity for heightened negative emotions, but the failure to regulate oneself when those emotions are present, that may present a risk for physiological dysregulation.
To summarize, the present study makes the following contributions to research on personality and stress physiology among children and adolescents: first, the study takes a more comprehensive approach to stress physiology by using a multisystemic index of allostatic load; second, it considers a psychological moderator of the emotionality–allostatic load link, namely self-regulation; third, both concurrent and prospective interrelations between emotionality, self-regulation and allostatic load are examined.
Methods
Participants
The original sample was recruited from rural upstate New York Co-Operative Extension and public school districts, with oversampling of low-income families as appropriate for the study’s focus on poverty and children’s development. For recruitment purposes, the poverty sample was defined as households living at or below the federally-defined poverty line. The average age at baseline was 9.2 (SD = 1.1) years, the age at follow-up was 17.5 (SD = 1.1) years. The sample analysed in the present study consisted of all 239 children (116 females) who took part at age 17.
Informed parental consent and child assent was obtained for all participants. The study was approved by Cornell University Institutional Review Board. Families were paid for their participation.
Measures
Negative emotionality
Negative emotionality was assessed at baseline. Mothers were interviewed about children’s temperament using Buss and Plomin’s (1984) Emotionality, Activity and Sociability (EAS) Survey for Children. The emotionality subscale of the survey, used in the present study to assess negative emotionality, consisted of 5 items: “cries easily,” “tends to be somewhat emotional,” “often fusses and cries,” “gets upset easily” and “reacts intensely when upset.” Each item was scored on a scale from 1 to 5 (1 = “not typical of your child,” 5 = “very typical of your child”), and the average of the 5 items was used as the emotionality score, ranging from 1 to 5 (Cronbach α = .80). Buss and Plomin’s (1984) scale is a widely used measure of child temperament and has been previously utilized to investigate the effects of negative emotionality on mental and physical health in children and adolescents (Goodyer, Ashby, Altham, Vize, & Cooper, 1993; Lindhout, Markus, Hoogendijk, & Boer, 2009; Pilarska & Olszewska, 2009).
Self-regulation
Self-regulation was also assessed at baseline. The present study used a widely accepted measure of self-regulation, namely a variant of Mischel’s delayed gratification task (Mischel, Ebbesen, & Raskoff Zeiss, 1972). Ability to delay gratification has been previously shown to predict socioemotional, cognitive and physical health outcomes, both concurrently and prospectively (Mischel, Shoda, & Rodriguez, 1989; Schlam, Wilson, Shoda, Mischel, & Ayduk, 2013).
Children were tested individually. Every child was presented with two plates of candy, one large and one small, and asked which one s/he preferred. Every child stated that they preferred the larger plate. The larger plate was placed directly in front of the children together with a small bell. The experimenter then told the child that she needed to prepare some materials for the next task in the living room. The experimenter explained that if the child could wait and not get up from his/her chair or eat any candy, s/he would be allowed to have the candy on the large plate when the experimenter returned to the room. However, if the child felt unable to wait, s/he could ring the bell, the experimenter would return, and the child could have the smaller plate of candy. Children were asked to repeat the instructions and the experimenter demonstrated returning to the kitchen when the bell was rung. The experimenter came back after a 30 minutes delay. Whether or not the child was able to wait for the experimenter to return without ringing the bell, eating the candy or leaving his seat was a dichotomous indicator of self-regulation (coded as 0 for delay success and 1 for failure to delay).
Allostatic load
While the AL concept provides a valuable theoretical framework for studying the long-term effects of chronic stress on the body, quantifying AL in empirical studies has been a challenge, and currently there is no gold standard for measuring AL (see Juster et al., 2010 for a review of AL formulations and scoring methods). Consistent with previous studies in adults and children (Evans, 2003; Seeman, Singer, Rowe, Horwitz, & McEwen, 1997), our measure of AL was based on the biomarkers of the SAM system (epinephrine and norepinephrine) and HPA axis (cortisol), as well as biomarkers of cardiovascular activity (systolic and diastolic blood pressure), and metabolic function (body mass index). As stated above, catecholamines and cortisol are primary physiological mediators of stress, while cardiovascular and metabolic system are the systems in which most detrimental changes resulting from chronic stress occur (McEwen, 1998). Previous research has confirmed that AL components representing different physiological systems share common variance, justifying the treatment of AL as a unitary construct (McCaffery, Marsland, Strohacker, Muldoon, & Manuck, 2012; Seeman, Gruenewald et al., 2010).
The same protocol was used at both baseline and follow-up to assess AL. Overnight urine was collected from 8 pm on the evening of the experimental protocol to 8 am the next morning. Samples were stored in an ice container with a preservative (metabisulfite). Total volume was recorded, and four 10-ml samples were randomly extracted and deep-frozen until assays were completed. For the catecholamines, the urine was also acidified. Epinephrine and norepinephrine were assayed by HPCL with electrochemical detection (Riggin & Kissinger, 1977), and cortisol with a radioimmune assay (Contreras, Hane, & Tyrrell, 1986). Creatinine was included as a statistical control for the neuroendocrine assays. Participants’ resting blood pressure was calculated with automated readings (Dinamap Model Pro 100, Critikon) taken every 2 minutes, while participants sat quietly. The second through seventh readings were averaged and used as an index of basal blood pressure (Kamarck et al., 1992). Body mass index was calculated as weight in kilograms divided by squared height in meters.
AL is most typically calculated as a summary index representing the number of biomarkers whose values go beyond a theoretically or empirically defined high-risk threshold (Juster et al., 2010). In the present study, the number of physiological parameters (resting diastolic and systolic blood pressure [BP], overnight cortisol, epinephrine, and norepinephrine volumes, and body mass index) on which participants scored above the high-risk cut-off was calculated, yielding an AL index with a possible range from 0 to 6. For BP and BMI, we used clinically-relevant cut-off points previously established for paediatric population. Specifically, the 90th BP percentile is used in children and adolescents to define pre-hypertension, while the 85th BMI percentile defines overweight. We calculated BP and BMI percentiles based on paediatric norms, which are adjusted for age and, for BP norms, also for height (Himes & Dietz, 1994; National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents, 2004). Because no population norms exist for endocrine biomarkers for children, we used the 75th percentile as the cut-off threshold for cortisol and catecholamines, following the most common practice in AL literature (Evans, 2003; Juster et al., 2010).
Statistical analyses
The interactive effect of negative emotionality and self-regulation on AL at baseline and follow-up was assessed using linear regression analyses. Negative emotionality, self-regulation and their product were entered as predictors of AL. Age, gender, and income-to-needs ratio at baseline were controlled for; analyses of AL at follow-up controlled for baseline AL, thus making our analyses prospective, longitudinal. In addition to testing statistical significance of the interaction between negative emotionality and self-regulation, we probed the slopes of negative emotionality at both values of the binary self-regulation variable (0 = able to delay gratification, 1 = not able to delay gratification).
Two approaches to missing data were used. First we ran the analyses excluding all participants with missing data (listwise deletion). Then we ran the same regression models using full information maximum likelihood (FIML) estimation, thus taking advantage of all information that is available for each participant (Bollen & Curran, 2006). FIML is the method of choice for missing data estimation when insufficient statistical power may be a concern (as is often the case for detecting statistical interaction) (Graham, Olchowski, & Gilreath, 2007). Analyses were conducted in Lavaan-R 3.0.1 using the MLR estimator, which produces standard errors and test statistics that are robust against non-normality. Fit statistics, parameter estimates and standard errors obtained using both approaches are reported.
Results
Of the participants, 25 missed data on negative emotionality, 35 on self-regulation, 48 on AL at baseline and 48 on AL at follow-up. The subsample of participants who had complete data on all variables included 152 children. This subsample did not differ from participants with missing data on baseline or follow-up AL, emotionality, self-regulation, age or gender distribution; however participants with complete data had higher income, t(237) = 3.70, p = .000.
The mean emotionality score was 2.75 (SD = .96). Twenty-eight percent of the participants failed to delay gratification. The mean AL score was 1.02 (SD = .91) at baseline and 1.27 (SD = 1.11) at follow-up. In total, 28% and 34% of participants had AL ≥ 2 at baseline and follow-up, respectively. There was a statistically significant correlation between AL at baseline and AL at follow-up (r = .18, p = .021). The online supplemental material provides further information regarding the individual biomarker components of AL at baseline and follow-up, including descriptive statistics and correlations.
Emotionality was not significantly correlated with AL, either concurrently or prospectively (r = .05 and r = −.01, respectively). Self-regulation was not associated with AL at either time points (both ts < 1), nor was it associated with emotionality (t < 1), suggesting that these are independent constructs.
We further investigated the interactive effects of negative emotionality and self-regulation on baseline and follow-up AL using linear regression analyses. AL was regressed on negative emotionality, self-regulation, and their product, controlling for the demographic covariates; analyses of AL at follow-up controlled for baseline AL. The model was significant for both baseline, χ 2(6) = 12.96, p = .044, R 2= .08 [FIML: χ 2(6) = 23.37, p = .001, R2 = .11] and for follow-up, χ 2(7) = 19.77, p = .006, R 2= .13 [FIML: χ 2(7) = 23.43, p = .001, R2 = .12].
For AL at baseline, the interaction between emotionality and self-regulation was not statistically significant, p = .17 [FIML: p = .26]. The slope of negative emotionality in those who were and were not able to delay gratification was .06, SE =.08 [FIML: b = −.03, SE =.08] and −.16, SE = .14 [FIML: b = −.19, SE= .12], respectively. However, the interaction between emotionality and self-regulation predicted AL at follow-up, p = .016 [FIML: p = .025]. In adolescents who were not able to delay gratification, the slope of emotionality was .37, SE = .18 [FIML: b =.32, SE = .17]. In contrast, in adolescents successful at delaying gratification, the slope of emotionality was −.12. SE = .11 [FIML: b = −.13, SE = .10]. The interaction is illustrated in Figure 1. For participants who had both high negative emotionality (> 1 standard deviation above the mean) and were unable to delay gratification, AL was 1.02 (SE = .48 [FIML: b = 1.03, SE = .45]) higher than for the rest of the sample. Note that this prospective, longitudinal effect is equivalent to adding one more biological parameter above the high-risk threshold.
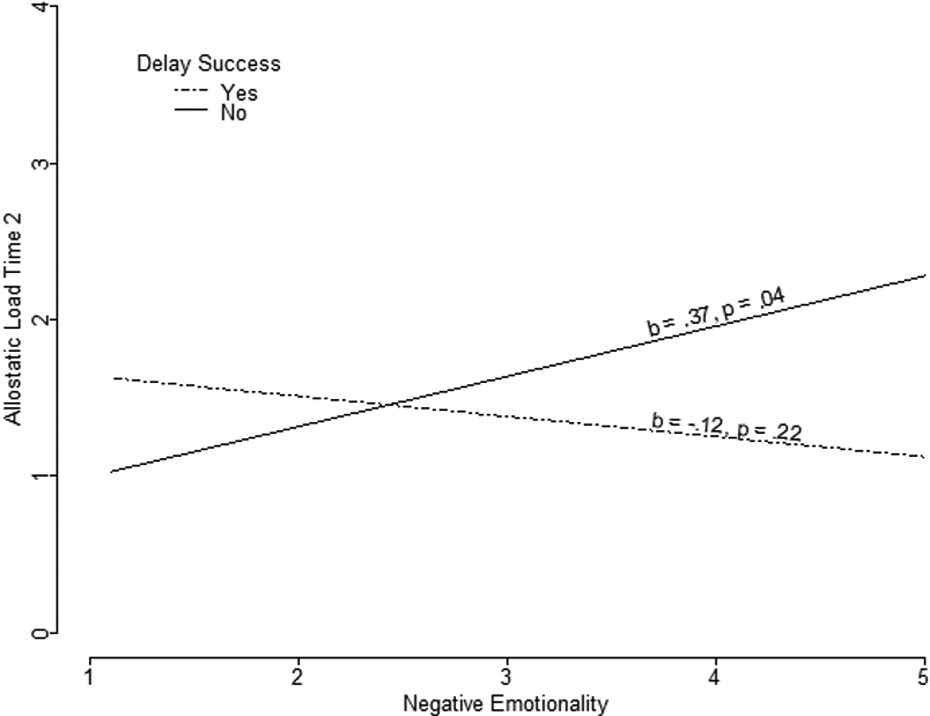
The interaction between negative emotionality and self-regulation (successful delay of gratification) at baseline (age 9) as predictors of allostatic load at follow-up (age 17) in 152 children without missing data.
Discussion
In the current study, we investigated the relationship between negative emotionality, self-regulation and AL, a measure of cumulative burden of chronic stress on the body. Previous research of negative emotionality and stress physiology has produced mixed results, underscoring the need to consider potential moderators; however, existing work on moderators of the link between temperament and physiology has focused primarily on environmental factors. To the best of our knowledge, this is the first study to test the hypothesis that the link between negative emotionality and physiological functioning in children may be moderated by children’s own psychological characteristics, in particular by self-regulation.
Our results showed that negative emotionality alone was not a significant predictor of AL, either concurrently or prospectively. Very small correlation coefficients suggest that this negative finding is due to the absence of the effect rather than insufficient power to detect it. At the same time, negative emotionality was prospectively associated with increases in AL when self-regulatory competencies were low. In children with low self-regulation, the prospective effect of high emotionality was equal to as much as an additional biological parameter above the high-risk threshold in adolescence.
As we discussed in the introduction, negative emotionality is thought to exacerbate perception of stress (Ebstrup et al., 2011), while self-regulation can attenuate these emotional reactions via top-down processes, thus buffering the harmful effects of stress (Beckmann & Kellmann, 2004; Heatherton, 2011). Previous literature has demonstrated that self-regulation can moderate the effects of negative emotionality on mental health and adjustment in early life (Eisenberg et al., 2000; Oldehinkel et al., 2007; Rothbart & Bates, 2006). Our findings suggest that negative emotionality and self-regulation also interact in predicting parameters of physiological functioning in adolescents.
Allostatic load is an established predictor of health and mortality later in life (Ganzel, Morris, & Wethington, 2010; McEwen & Seeman, 1999; Seeman et al., 2001). Given the scarcity of research on AL in early life, the present study contributes to the understanding of early life precursors of stress-related wear and tear of the body and thus improves our knowledge about childhood determinants of long-term health and longevity. Furthermore, by using AL we are not only able to capture a multi-dimensional indicator of physical health, but an objective one as well. In personality and health studies, which are subject to reporting bias, objective measures of the outcomes are crucial, as personality may influence the way individuals perceive and self-report their health (Watson & Pennebaker, 1989).
By considering a psychological moderator of the link between negative emotionality and physiology in children and adolescents, this study makes a contribution not only to understanding of early life predictors of physiological functioning, but also to the discussion of the role of negative emotionality in health. Indeed, negative emotionality is often cited as a risk factor for mental and physical health (Smith, 2006). Our results underscore the need for a more nuanced understanding of the role of this psychological factor in health. In particular, it suggests that negative emotionality may only be a risk factor in some people and that it affects health in conjunction with other psychological attributes, such as low self-regulation. In sum, our research suggests that personality characteristics do not operate in isolation. Future research is needed to identify whether there are other individual psychological characteristics, e.g. intelligence, self-efficacy, or social competence to name a few, which might buffer effects of negative emotionality on health. Our findings have also practical implications, suggesting that children high in negative emotionality may benefit particularly from efforts designed to improve self-regulation skills.
Previous studies on the physiological correlates of negative emotionality in early life have been primarily cross-sectional, focusing on infancy and early childhood and investigating reactivity to acute stressors. The prospective effects of childhood emotionality on physiological functioning in adolescence, the time of increased negative affect (Larson, Moneta, Richards, & Wilson, 2002), remain largely unknown. The present study addressed this gap in literature. We observed interactive effects of negative emotionality and self-regulation on AL only at age 17, but not concurrently at age 9. These results may be due the fact that the effects of temperament on physiological dysregulation may not appear until later in life. Indeed, health-damaging effects of childhood psychosocial factors are not always detectable in early life and sometimes do not appear until well into adulthood (Miller, Chen, & Parker, 2011; Taylor et al., 2011). AL, the outcome of interest in the present study, measures the accumulation of stress-related changes in the normal functioning of several biological systems. This wear and tear of the body resulting from chronic stress accumulates slowly throughout life. At early ages, any such changes will probably be small, making moderate effects of psychosocial factors difficult to detect. Furthermore, the fact that the effects of negative emotionality and self-regulation do not arise until after puberty points to the possibility that these factors only affect physiological functioning in conjunction with the biological, psychological, and social challenges that adolescence face during puberty. In other words, it is possible that major changes brought about by this developmental stage might exacerbate the effects of negative emotionality on physiology, while making self-regulation even more important. Future research needs to address whether potentially harmful effects of negative emotionality and beneficial effects of self-regulation vary depending on the developmental period.
Several limitations of the study ought to be mentioned. Missing data is a problem in any longitudinal study. To evaluate the sensitivity of our findings to the impact of missing data, we analysed the results in two different ways: excluding participants with missing data and estimating the missing data. These two approaches yielded comparable results. Because the present study was conducted among white, rural children in upstate New York, generalizability to children from affluent families, urban children, as well as individuals from other ethnic and cultural groups is limited. Furthermore, self-regulation is a multi-faceted attribute involving, for example, behaviour, emotion and attentional components. Future research using multiple methods for tapping this multidimensional construct is called for. Multiple ways of assessing self-regulation exist. In the present study, we used a behavioural measure; however, research in young children has also assessed self-regulation via adults’ reports (Eisenberg & Morris, 2002). Future research is needed to ascertain whether questionnaire measures of self-regulation among children would show the same pattern of results.
As discussed earlier, considerable variation exists in the methods of AL assessment and therefore the comparability of our results to findings from other studies may be limited. While the approach we used to calculating AL is among the most common, it does not account for the fact that inadequately low values of some of the biomarkers, in particular cortisol, may also reflect dysregulation resulting from stress (Glover, 2006). Alternative formulations have been proposed to account for both extremely low and extremely high biomarker values (Seplaki, Goldman, Glei, & Weinstein, 2005). Further research needs to test the reported associations using alternative AL formulations.
To conclude, the present study adds to our understanding of how emotionality can affect physiological functioning and health throughout childhood and adolescence. Although in early life the relationship between negative emotionality and physiological functioning appears to be weak, in combination with other individual characteristics, such as poor self-regulatory skills, negative emotionality indeed presents a risk for physiological dysregulation as early as 17 years of age. Future studies are needed to further clarify how emotionality interacts with both environmental experiences and individual characteristics to create health outcomes not only in youth but throughout the life-course.
Footnotes
Acknowledgements
We are grateful to the families who participated throughout this research. We thank Jana Cooperman, Kim English, Missy Globerman, Matt Kleinman, Rebecca Kurland, Melissa Medoway, Tina Merilees, Chanelle Richards, Adam Rohksar, and Amy Schreier for their assistance with data collection.
Funding
This work was supported by the W. T. Grant Foundation, the John D. and Catherine T. MacArthur Foundation Network on Socioeconomic Status and Health, and the National Institute on Minority Health and Health Disparities (5RC2MD00467).