
Abstract
Coping research has consistently shown that accommodative coping is positively correlated with individuals’ health. Until now, however, there have been little to no studies on the prognostic impact of accommodative coping on health, and only a few studies investigating its buffering effect on the relation between stress and health in childhood and adolescence. Thus, two main research questions were tracked in two longitudinal studies: Study 1 investigated if accommodative coping is indeed a functional resource that longitudinally predicts well-being in a sample of N = 403 adolescents (aged 12–15 years at Wave 1). Study 2 examined the function of accommodative coping under stressful conditions by investigating its buffering effect on the negative impact of school-related stress on well-being in a sample of N = 86 children (aged 9–12 years at Wave 1). Study 1 revealed accommodative coping longitudinally predicting well-being, and, conversely, there was no prediction of well-being through accommodative coping over time. Study 2 revealed a significant moderating effect and gives a first indication that accommodative coping buffers the negative impact of school-related stress on well-being in childhood. The results indicate that accommodation is a functional coping resource in adolescence that diminishes the negative impact of specific stressors. All main and further results are discussed, and implications for further research are given.
Not only adults, but also children and adolescents, are confronted with daily hassles (e.g. a quarrel with a friend), normative (e.g. the transition to school in childhood) or non-normative (e.g. the dead of a beloved person) critical life-events that can negatively influence individuals health (Aldwin, 2011; Compas, Connor-Smith, Saltzman, Thomsen, & Wadsworth, 2001; Fields & Prinz, 1997; Seiffge-Krenke, 1995). Thus, it is a central task in childhood and adolescence to learn to cope with these events. Coping comprises a huge variety of “how people mobilize, modulate, manage, and coordinate multiple aspects of the self under stress (or fail to do so)” (Aldwin, Skinner, Zimmer-Gembeck, & Taylor, 2011, p. 564), and involves all possible efforts (e.g. behavioural, cognitive) to manage the problem and all processes to regulate its upcoming emotions and cognitive disturbances and to reduce the emerging stress. A vast amount of studies on coping and emotion regulation in childhood and adolescence (e.g. Aldridge & Roesch, 2007; Compas, Orosan, & Grant, 1993; Connor-Smith & Compas, 2004; Garnefski, Koopman, Kraaij, & Cate, 2009; Garnefski, Legerstee, Kraaij, Van Den Kommer, & Teerds, 2002; Garnefski, Rieffe, Jellesma, Meerum Terwogt, & Kraaij, 2007; Gonzales, Tein, Sandler, & Friedman, 2001; Hampel & Petermann, 2006; Sanchez, Lambert, & Cooley-Strickland, 2013; Sandler, Tein, & West, 1994; A. H. Thomsen et al., 2002), has shown that coping processes (e.g. active problem-solving or positive reappraisal) have important consequences for the individual’s mental and physical health (as e.g. well-being, no somatic symptoms, the lack of internalizing and externalizing symptoms, life satisfaction). However, not all coping and emotion regulation efforts are positively associated with individuals’ health. For instance, while cognitive change or problem-solving in general show positive correlations to mental and physical health, suppression, rumination or avoidance in general show negative correlations with these health outcomes (Aldao, Nolen-Hoeksema, & Schweizer, 2010; Compas et al., 2001; Fields & Prinz, 1997; Webb, Miles, & Sheeran, 2012).
Accommodative coping and its relevance for health: Empirical evidence
One particular coping resource that is expected to contribute to individuals health is accommodative coping (Brandtstädter, 2006; Brandtstädter & Rothermund, 2002; Skinner, Edge, Altman, & Sherwood, 2003; Skinner & Zimmer-Gembeck, 2007; Zimmer-Gembeck & Skinner, 2011). Especially in unalterable or uncontrollable situations accommodative coping resources can help the individual to resolve problems that are not directly solvable with active or direct problem solving strategies. Accommodative coping means changing ones view of a problem, e.g. through cognitively switching the focus on the good aspects of the worrying situation, downward comparisons, positive reappraisal, or through focusing alternative goals. Several approaches that are closely related to accommodative coping can be found in coping and emotion regulation research: secondary control coping (Band & Weisz, 1990; Heckhausen, Wrosch, & Schulz, 2010; Santiago & Wadsworth, 2009), goal dis- and reengagement (Wrosch, Scheier, Miller, Schulz, & Carver, 2003) and several strategies of emotion regulation and coping such as cognitive change, (positive) reappraisal, putting into perspective, positive refocusing, or acceptance (Aldao et al., 2010; Garnefski et al., 2007; Gross, 1998a, 1998b; Webb et al., 2012).
Studies with adult participants that focus on accommodative coping resources (or on related concepts or processes) have consistently shown that accommodative coping is positively correlated with health outcomes such as positive affect, self-esteem, life satisfaction and well-being as well as lower depressive symptoms and less health problems (Gross & John, 2003; Haase, Heckhausen, & Wrosch, 2013; Wrosch, 2011; Wrosch, Miller, Scheier, & de Pontet, 2007). Moreover, accommodative coping buffers the negative impact of stressful experiences (Brandtstädter & Greve, 1994; Brandtstädter, Wentura, & Greve, 1993; Greve & Enzmann, 2003; Greve, Enzmann, & Hosser, 2001). Two meta-analyses on the effectiveness of affect and emotion regulation strategies in adulthood support these results (Augustine & Hemenover, 2009; Webb et al., 2012). Based on 99 comparisons and a sample size of 3,570 individuals from studies with an experimental design, Webb and colleagues (2012) revealed a small-to-medium average effect of cognitive change on experiential, behavioural and physiological emotional outcomes (d+ = 0.36). Moreover, a closer look revealed exclusively positive effects on emotional outcomes for specific accommodative strategies of cognitive change (e.g. reappraising the emotional response: d+ = 0.23, reappraising the emotional stimulus: d+ = 0.36, reappraisal using perspective taking: d+ = 0.45). It supports the finding that Augustine and Hemenover (2009) reported in their meta-analysis years before (based on only two effect sizes): Reappraisal revealed as one of the two most effective regulation strategies, producing large hedonic shifts in affect (d+ = 0.65).
Investigations with adolescents support these findings. Most of the studies reveal a direct relationship between accommodative coping resources (or related strategies) and health outcomes, expressed by negative correlations between accommodative coping and internalizing, externalizing and somatic symptoms, or emotional and behavioural problems (Connor-Smith, Compas, Wadsworth, Thomsen, & Saltzman, 2000; Fear et al., 2009; Garnefski, Kraaij, & Spinhoven, 2001; Garnefski et al., 2007; Hampel & Petermann, 2006; Hsieh & Stright, 2012; A. H. Thomsen et al., 2002; Turner-Sack, Menna, & Setchell, 2012). There are, however, also a few studies that report no or even a slightly negative relationship (Hsieh & Stright, 2012; Legerstee, Garnefski, Verhulst, & Utens, 2011; Pinquart, Silbereisen, & Wiesner, 2005), a result which might be due to the investigation of specific samples (e.g. from individualistic vs. collectivistic cultures) and different measurement methods (e.g. accommodation assessed by reappraisal scales vs. accommodation assessed by the decrease of a desired state across 1 year). A meta-analysis on the relationship of emotion-regulation strategies (assessed by self-reports) and symptoms of psychopathology in adolescence and adulthood (Aldao et al., 2010) also indicates a positive relation of accommodative coping and health with small to medium effect sizes. In particular, reappraisal (as one central facet of accommodative coping) was significantly negatively associated with psychopathology (r = −.14), based on 15 comparisons, whereas acceptance was negatively (but not significantly) associated with psychopathology (r = −.19), based on seven comparisons. Few studies corroborate the findings known from adult samples of an indirect effect of accommodative coping resources. In a study with 1,310 adolescents (M = 18 years, SD = 3.2), Kraaij and colleagues (2003) revealed that reappraisal buffers the negative impact of the experience of negative life events on depression. Moreover, Santiago and Wadsworth (2009) highlighted the moderating role of secondary control coping in the relationship between family conflict and internalizing symptoms in a sample of 82 adolescents (M = 13.5 years, SD = 1.98).
Accommodative coping and its relevance for health: A research gap
The results of the aforementioned studies emphasize the importance of accommodative coping resources for health. However, despite the cumulated evidence of positive effects for health, several research questions remain to be investigated. First, studies on accommodative coping and health primarily focus on samples in adolescence or adulthood. Although there are some studies that investigate accommodative coping resources in children (Curry & Russ, 1985; Spirito, Stark, Grace, & Stamoulis, 1991; Thurber & Weisz, 1997), only a small number examine the relation between accommodative resources and health (Band & Weisz, 1990; de Boo & Wicherts, 2009; Losoya, Eisenberg, & Fabes, 1998). Second, while studies with adult samples focus on both the effects of accommodative coping resources on positive (e.g. self-esteem, well-being, life satisfaction) and negative (e.g. depression, somatic symptoms) health outcomes, studies with younger samples primarily concentrate on the connection of accommodative coping and negative health outcomes (e.g. internalizing and externalizing symptoms, emotional and behavioural problems) and only few studies take the connection to positive health outcomes into account (de Boo & Wicherts, 2009; Hsieh & Stright, 2012; Kliewer, 1991; Losoya et al., 1998; Pinquart et al., 2005). Third, there are very few studies that investigate the moderating role of accommodative coping resources for possible effects of stress on health in adolescence (as already mentioned: Kraaij et al., 2003; Santiago & Wadsworth, 2009) and we found no studies which examine whether accommodative coping resources diminish the detrimental impact of stress and simultaneously provide positive health outcomes. Fourth, even though there are longitudinal studies that include the measurement of accommodative coping resources (Eisenberg, Fabes, Nyman, Bernzweig, & Pinuelas, 1994; Frydenberg & Lewis, 2000; Kliewer, 1991; Losoya et al., 1998; Tolan, Gorman-Smith, Henry, Chung, & Hunt, 2002; Vierhaus & Lohaus, 2009), none of these addresses the question concerning the longitudinal prediction of accommodation on health. Furthermore, neither of the studies in the aforementioned meta-analysis (Aldao et al., 2010) examines the longitudinal effect between reappraisal and adolescent health outcomes. However, if we take existing correlational findings about the relation of accommodative coping and health into account, not one but two possible directions of prediction could be assumed: On the one hand, accommodative coping, as a functional coping resource, could lead to better health (as mostly interpreted). On the other hand, it could also be assumed that it might be easier for healthier children and adolescents to cope in an accommodative way, because a healthy and satisfied life facilitates to adjust preferences or to see good aspects in bad situations. Only one longitudinal study (Wrosch & Miller, 2009) with adolescent females gives an empirical hint on the longitudinal relation of accommodative coping and negative health outcomes (here: goal disengagement and depression). The study highlights two interesting points: While high baseline levels of depressive symptoms increased the occurrence of goal-disengagement over time, the increase of goal-disengagement decreased following depressive symptoms. The results of the study indicate that accommodative coping resources are not only predicted by (very) low mood but also positively predict negative health outcomes in adolescent females. To specifically investigate the direction of prediction based on longitudinal designs is of crucial importance if we want to promote successful development (e.g. through prevention and intervention programs).
The present studies and hypotheses
The two following longitudinal studies with children and adolescents mark a first step towards filling some of these gaps by, first, investigating the prognostic effect of accommodative coping on health and, second, the moderating effect of accommodative coping on the impact of stress on health.
In Study 1, we investigated if accommodative coping is indeed a functional coping resource, predicting adolescents health (here: well-being) 1 year later. To examine the direction of relation between accommodative coping and well-being we used a cross-lagged panel design in a sample of seventh-grade adolescents (at Wave 1). Here, accommodative coping at Wave 1 is expected to affect well-being at Wave 2. In turn, if accommodative coping is indeed a functional resource that promotes health in adolescence, its availability at Wave 2 should not be affected by previous well-being at Wave 1. These assumptions lead to Hypothesis 1: Accommodative coping is a positive predictor for well-being, whereas well-being does not predict accommodative coping in adolescence.
In Study 2, we investigated the function of accommodative coping by focusing on its effect on well-being under a situation that is experienced as stressful or burdening. Here, we chose a sample of children on the verge of transition to a new school(-track): In middle childhood, after fourth grade, students transfer from elementary school to one of three secondary school tracks (Gymnasium, Realschule, Hauptschule). The transition poses a lot of stress: In particular, the new social environment requires a higher level of performance with respect to social, environmental and organizational changes (Chung, Elias, & Schneider, 1998; Griebel & Niesel, 2004). Mastering this transition phase is a sensitive issue to children and young adolescents both subjectively and objectively, because corroboration at the chosen school track has far reaching consequences for future career options. Thus, a decline of achievement level after transition is expected to produce considerable stress (Adams & Adams, 1993; Seiffge-Krenke, 1995) and to negatively predict well-being. According to the studies with adult samples mentioned above, the individuals’ ability to accommodate at that time point should facilitate dealing with this stress by moderating (diminishing) the negative impact of change in achievement on well-being. Therefore, Hypothesis 2 is as follows: Accommodative coping diminishes the negative impact of change in school achievement on well-being in children.
Study 1
Method
Design
Data were collected anonymously on two measurement occasions, at the beginning of the seventh grade (Wave 1) and 1 year later, at the beginning of eighth grade (Wave 2). All data were collected with prior parental consent during a regular school lesson.
Participants
At Wave 1, 535 seventh-grade students aged 11 to 15 years (M = 12.61, SD = .62, 48.31% girls) participated in the study. At Wave 2, 498 students participated, ranging from age 12 to 16 years (M = 13.65, SD = .65, 49.39% girls). After matching the questionnaires (via a self-generated personal code), the longitudinal sample included N = 403 adolescents (concordance rate: 75.33%), ranging from age 12 to 15 at Wave 1 (M = 12.61, SD = .62). N = 209 (51.9%) students were female and n = 193 (47.9%) male (missing data: n = 1). Overall, 21 class groups participated; 13 of these classes came from three academic-track schools (Gymnasium; n = 253; 62.8%) and eight from three intermediate track schools (Realschule; n = 150; 37.2%).
Measures
Accommodative coping
Accommodative coping (AcCo) was measured by means of 15 items of the flexible goal adjustment scale (FLEX: Brandtstädter & Renner, 1990). Since this scale was originally conceptualized for use in adults, a linguistically adapted version for adolescents (Greve & Thomsen, 2013; T. Thomsen & Greve, 2013) was applied in this study. Each of the 15 statements could be rated on a five-point Likert scale (1 = strongly disagree to 5 = strongly agree; example item: “Sometimes things in life don’t go the way you want them to, but I still find it easy to see the good in the unpleasant things in life”). Validity information of the adapted scale for adolescents is given by positive correlations with scales that asses related coping and emotion regulation strategies (e.g. positive reappraisal and AcCo: r = .44**; optimistic thinking and AcCo: r = .33**, T. Thomsen, 2014) or health related quality of life (e.g. self-esteem and AcCo: r = .35**, Greve & Thomsen, 2013). Consistently, studies show a Cronbach’s Alpha of α =.70 for adolescent samples (Greve & Thomsen, 2013; T. Thomsen & Greve, 2013), which is generally lower than in adult samples (e.g. α = .83: Brandtstädter & Renner, 1990). In this study, the adapted scale showed the expected internal consistency by Cronbach’s Alpha of α = .70 at Wave 1 and α = .73 at Wave 2. The mean value was used as the measure for AcCo in all analyses.
Well-being
Well-being was measured using subscales from the self-report version of the Kindl-R-Questionnaire (Ravens-Sieberer & Bullinger, 1998, 2000). There are three age-adopted versions of the Kindl-R; here the Kiddo-Kindl for adolescents aged 13 to 16 was used. Measurement of well-being refers to states of psychological (4 items, e.g. “… I had fun and laughed a lot”) and physiological well-being (4 items, e.g. “… I was tired and worn out”) the participants experienced during the last week. Answers for all items ranged on a five-point Likert scale from 1 (“never”) to 5 (“always”). Convergent validity of the original Kindl-R is examined through correlations with other health questionnaires for children (e.g. CHQ general well-being with Kindl-R psychological well-being: r = .59 or Kindl-R physiological well-being: r = .52 / FLZ life satisfaction with Kindl-R psychological well-being: r = .45 or Kindl-R physiological well-being: r = .40), and discriminant validity is assessed by the comparison of healthy children with children with chronic illnesses (here, healthy children reported a significantly higher well-being than children with chronic illnesses; Ravens-Sieberer & Bullinger, 2000). Internal consistencies for well-being in this study were α = .73 at Wave 1 und α = .68 at Wave 2. The mean value of the scale was used in all analyses.
Results
Bivariate correlations
Cross-sectional bivariate correlations between accommodative coping and well-being were calculated for each wave. All correlations proved to be positive and significant (Table 1), showing that accommodative coping is positively correlated with well-being in adolescents. As well, all longitudinal correlations were significant, whereas accommodative coping at Wave 1 correlated higher with well-being at Wave 2 than accommodative coping at Wave 2 with well-being at Wave 1.
Descriptives and bivariate correlations between accommodative coping and well-being in Wave 1 and Wave 2 for Study 1.

**p < .01.
Autoregressive modelling
Cross-lagged pathways (Hypothesis 1) were tested by calculating autoregressive models using Mplus 6 (Muthén & Muthén, 2010). Its computation allows examining the stability of the constructs over several measurement occasions as well as the influence on each other through cross-lagged pathways (Aldwin, 2007; Geiser, 2010; Kenny, 1975; Kline, 2011). Accommodative coping and well-being were moderately stable over time and significant positively connected at Wave 1 and 2. The pathway well-being at Wave 2 predicted by accommodative coping at Wave 1 proved to be significant, whereas the reverse pathway (accommodative coping at Wave 2 predicted by well-being at Wave 1) was not significant. The model showed a good model fit (Figure 1).

Autoregressive models for accommodative coping and well-being in Study 1: representation of standardized path coefficients (ß) for autoregressive and cross-lagged effects.
Discussion
Correlational results go in line with known findings from adulthood and late adolescence, indicating that accommodative coping is connected to positive health outcomes as well-being in early adolescence. Moreover, results of autoregressive modelling support Hypothesis 1: Accommodative coping is a functional resource in adolescence. The crossed-lagged effects indicate that adolescents’ accommodative coping at an earlier time point has a significant positive impact on well-being 1 year later. Conversely, previous well-being has no effect on the extent of accommodative coping over time. Thus, as postulated, accommodation seems to “work” as an independent resource as it predicts well-being instead of the other way around. However, one might note that the cross-lagged effect is small (β = .14, p < .05). This might become understandable by taking into account the multitude of variables that are known to influence adolescents’ well-being (e.g. social support from parents and peers, competence in domains of importance, stress, illnesses, other coping strategies; e.g. Compas et al., 2001; Harter, 1999; Lewinsohn et al., 1994; Sanchez et al., 2013), but that were not assessed in this study.
Study 2
Method
Design
Data were collected on two measurement occasions, right before (fourth grade, Wave 1) and about 6 months after (fifth grade, Wave 2) transition from elementary to secondary school. Questionnaires were distributed in class context during a regular school lesson. Parental consent was collected in advance for all participants. A personal code was generated for matching the data of the two measurement occasions.
Participants
Longitudinal data was obtained from 86 students aged 9 to 12 years at Wave 1 (M = 10.57, SD = 0.56, 46.5% girls). The sample was the intersecting set of two larger cross-sectional samples (Wave 1: N = 291, aged 9–12, M = 10.54, SD = 0.56, 50.2% girls; Wave 2, N = 449, aged 9–13, M = 11.12, SD = 0.53, 49.2% girls) drawn from 11 elementary schools and five secondary schools, among them two academic-track schools (Gymnasium), one intermediate track school (Realschule), and two schools comparable to comprehensive schools, offering two (Real- and Hauptschule) or all tracks (Integrierte Gesamtschule).
Measures
Accommodative coping
Accommodative coping (AcCo) was measured through the linguistically adapted version of the flexible goal adjustment scale for adolescents (Brandtstädter & Renner, 1990; Greve & Thomsen, 2013; T. Thomsen & Greve, 2013) as described in Study 1. The scale showed an internal consistency by Cronbach’s α = .73 at Wave 1 and α = .67 at Wave 2.
Well-being
Similar to Study 1, the adolescent’s well-being was measured through the KINDL-R-questionnaire (Ravens-Sieberer & Bullinger, 1998, 2000). Here, the Kid-Kindl for children aged 8 to 12 was used. Internal consistencies for well-being were α = .71 at Wave 1 und α = .75 at Wave 2.
Change in school achievement
On both measurement occasions students were asked for their school report grades in the main subjects German, English and mathematics shortly after receiving their report cards (midterm reports at Wave 2). To obtain a measure of change, a difference score (Wave 1 – Wave 2) for average school achievement was computed, a positive value representing an increase, a negative value a decline in achievement (since in the German grade system, higher numbers indicate poorer achievement).
Results
Bivariate correlations
Cross-sectional bivariate correlations for accommodative coping and well-being show low (Wave 1) and low to moderate (Wave 2), but statistically significant correlations (Table 2), indicating that both constructs are positively correlated in childhood. However, correlations between accommodative coping and well-being over both measurement point were non-significant. The change in school achievement was not related to accommodative coping, neither at Wave 1 nor at Wave 2, or to well-being at Wave 1. The bivariate correlation of change in school achievement with well-being at Wave 2 was low, but statistically significant, indicating that a decline in school achievement is associated with lower well-being in fifth grade.
Descriptives and bivariate correlations for accommodative coping, well-being and change of school achievement in Wave 1 and Wave 2 for Study 2.
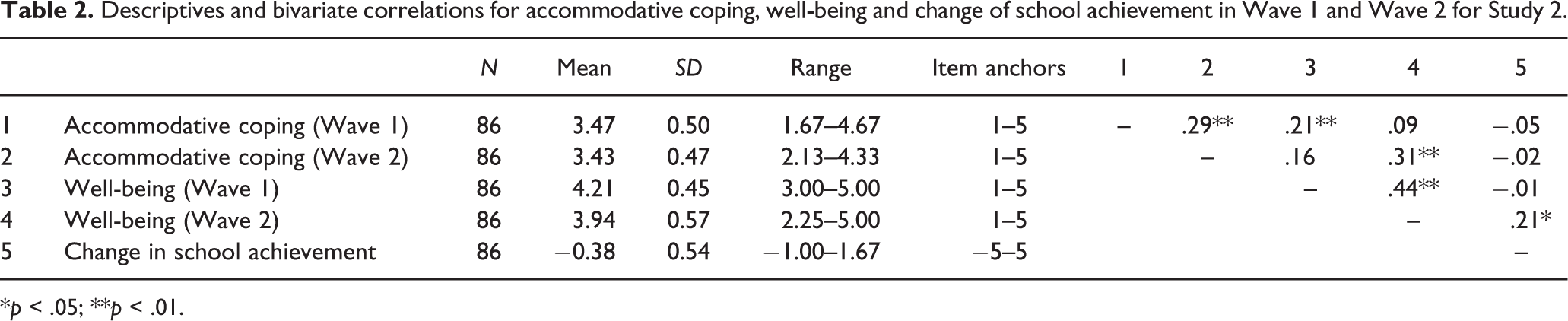
*p < .05; **p < .01.
Moderation effects
Moderation effects (Hypothesis 2) were tested by multiple regression analyses (Baron & Kenny, 1986), using well-being in fifth grade (Wave 2) as criterion and change in school achievement as predictor. AcCo at Wave 2 was used as moderator variable, as accommodative coping is expected to reveal its protecting effect through the experience of stress, which occurs after participants receive their report cards at Wave 2 and realize a decline of school achievement. To test the interaction effect, the product term was included in the model. To avoid multicollinearity, predictor and moderator variables were centred prior to calculating the product term (Cohen, Cohen, West, & Aiken, 2003). Main effects for both change in school achievement and AcCo were significant, indicating that a decline in school achievement and lower values of accommodative coping are associated with lower well-being. Beyond the main effects, the predicted interaction effect was significant as well. However, effect sizes were generally small (Table 3). To visualize the interaction effect, and to make the data easier interpretable, the sample was split at the median of the moderator variable (AcCo), the two lines represent the regression lines for both groups (above and below the median). As illustrated in Figure 2, the negative effect of a decline in school achievement can only be found for children low on accommodative coping. For children scoring high on accommodative coping, a change in school achievement and well-being are not related.

The interaction effect of change in school achievement and accommodative coping at Wave 2 predicting well-being in Study 2.
Multiple regression analyses predicting well-being from change in school achievement, accommodative coping at Wave 2 and their interaction term, as well as effect sizes for Study 2.

Note. N = 85.
*p < .05; **p < .01.
Discussion
Again, correlational results show that accommodative coping is also connected to positive health outcomes (here: well-being) in late childhood. Moreover, the moderating effect indicates that accommodative coping (at Wave 2) diminishes the negative impact of stress (here: change in school achievement) on well-being in children, confirming Hypothesis 2. The negative effect of a decline in school achievement on well-being can only be found for children scoring low on accommodative coping, while children’s well-being is not affected by the decline of school achievement, if they score high on accommodative coping. Even though the sample size of N = 86 participants is not very high and analyses show low effect sizes (which might be due to the fact that other variables are involved to explain well-being in childhood also), our results give a very first indication that accommodative coping in late childhood works as it is known from adult samples: Accommodation seems to serve as a protective resource, promoting health despite of stressful conditions. Beside this result, one limitation should be mentioned: We moreover tested if prior AcCo at Wave 1 could also diminish the negative impact of change in school achievement on well-being. Here, the main effect of change in school achievement turned out to be almost significant (p = .051), but, as correlational analyses already indicated, neither the main effect of accommodative coping at Wave 1 (p = .386), nor the interaction effect (p = .807) reached any significance. This result might be due to the fact that accommodative coping is not yet very stable in childhood (for further discussion, see the General discussion).
General discussion and future implications
Our longitudinal studies on the impact of accommodative coping on well-being in childhood and adolescence show two main findings: Accommodative coping is, first, a functional resource influencing well-being in early and middle adolescence and, second, seems to work as a protective coping resource under stressful conditions in late childhood. The results of our studies mark a very first step to bridge the research gaps mentioned in the theory section: In our studies, data were collected from samples in late childhood and early to middle adolescence. Moreover, both studies focus on positive health outcomes (here: well-being), rather than investigating psychological and physical illnesses. Furthermore, compared with previous studies in this research field, the moderating role of accommodative coping on the relationship between stress and health is examined in more detail. At least, since recent studies on accommodative coping and well-being usually report correlational findings (with the exception of Wrosch & Miller, 2009), both studies are based on longitudinal designs.
Cross-validating problems
Beside our main results, two open research questions resulting from cross-validating analyses need to be mentioned and discussed.
First, after the calculation of our main analyses, we tried to replicate the findings of autoregressive modelling with our adolescent sample of Study 1 in our younger sample of Study 2. Again, we expected accommodative coping predicting well-being (here: half a year later) in late childhood, whereas well-being should not predict accommodative coping. However, the results of Study 1 could not be replicated in Study 2. While accommodative coping and well-being were small to moderately stable over time (β Acco = .27, p < .01 / β WB = .44, p < .01) and significant positively connected at Wave 2 (r = .22, p < .05), but not at Wave 1 (r = .10, n.s.), the autoregressive pathways did not reach significance (Accow1 influencing WBw2: β = .05, n.s. / WBw1 influencing Accow2: β = .14, n.s.). Thus, accommodative coping did not predict well-being in children. Besides methodological arguments (e.g. the small sample size of Study 2; not the same time interval between Wave 1 and 2 compared to Study 1), we suspect that the continuous development of coping strategies could provide an explanation for the lack of replication in our children sample. At a first glance, it seems obvious that accommodation is rather instable in late childhood. While the cross-lagged panel analysis in Study 1 indicates a moderate stability coefficient of β = .45 (p < .01), the stability coefficient in Study 2 is much lower β = .27 (p < .01). A closer look at the age group mean differences supports this finding: An univariate analysis of variance for all participants of Study 1 and Study 2, F(4, 471) = 10.58, p < .01, reveals that the younger age groups score significantly (p < .01, post-hoc Tukey Test) higher on accommodation (M9–10years = 3.69, sd = 1.38 / M11years = 3.95, sd = 1.64) than the older age groups (M12years = 3.25, sd = .47 / M13years = 3.21, sd = .46 / M14–15years = 3.26, sd = .40), resulting in lower stability coefficients in Study 2 (children between 9 and 12 years) than in Study 1 (adolescents between 12 and 15 years). This instability of accommodation in younger age groups might be due to the ongoing development of coping in this age period (T. Thomsen, 2014). Whereas proactive strategies as active problem solving or social support seeking (e.g. from parents, teachers or peers) are used frequently and reliably in middle and late childhood, cognitive strategies (e.g. accommodation or reappraisal) are still in development (Zimmer-Gembeck & Skinner, 2011) and possibly used unsystematically. If a problem, besides the dominance of proactive strategies at this age period, is solved by accommodative coping, it is functional for the current well-being of the child, resulting in positive correlations between accommodative coping and well-being (the autoregressive model of Study 2 indicated a significant correlation only at Wave 2, possibly, because the evaluation of accommodative coping at a very young age is not completely realistic yet). Accommodative coping, however, might not (yet) have a prognostic relevance for later well-being (resulting in the lack of replication of the cross-lagged pathways in Study 2), because there are still other dominant and (maybe more) functional options to solve a problem, as e.g. proactive strategies. In adolescence, however, when knowledge and usage of coping strategies is more consolidated and stable, accommodative coping is gaining functional relevance and thus, has more enduring effects on health, resulting in the longitudinal prediction of well-being (as found in our older age group in Study 1). This instability and ongoing development in childhood might also explain the lack of main and moderating effects in the second moderation analysis of Study 2 with accommodative coping at Wave 1 as moderator (see discussion section of Study 2).
Second, after confirming the moderating role of accommodative coping (at Wave 2) in the relation of school-related stress and well-being in Study 2, we aimed to investigate the buffering effect of accommodative coping in our sample of Study 1, however, under further and more stressful circumstances (e.g. conflicts with friends, a break up with the first love, experience of violence, critical life events; Kraaij et al., 2003; Sanchez et al., 2013; Sandler et al., 1994; Seiffge-Krenke, 1995). Since we assessed the amount of critical life events experienced in the last 12 months in Study 1 (our adolescent sample) at Wave 2, we were able to test if accommodative coping serves as a buffer under more severe and stressful conditions. Here, at Wave 2, students were asked to cross 12 critical life events they experienced in the last 12 months (e.g. death of a loved one, losing contact to somebody important, moving away or change of school, divorce of parents, healing from a longer injury or illness, problems in school, big fight with friends or parents) and created a variable from the aggregated number of all events experienced (min. = 0, max. = 12). Moderation effects were tested according to the procedure described in Study 2. The amount of critical life events served as a predictor, accommodative coping as a moderator and well-being as an outcome variable (all variables measured at Wave 2). Analyses showed main effects for critical life events (β = −.32, p < .01) and accommodative coping (β = .22, p < .01) on well-being, but no interaction effect (β = .00, n.s.). Thus, accommodative coping did not diminish the negative impact of critical life events experienced in the last 12 months on well-being in adolescence. Again, besides possible methodological reasons (e.g. critical life events were assessed retrospectively and could already be weakened through past coping effects) we see three possible explanations for the missing buffering effect: First, it could be assumed that accommodative coping is less effective with serious problems and only diminishes the negative impact of minor problems (e.g. bad grades in school). However, this argument does not seem very plausible as studies with late adolescents and adults prove positive effects of accommodative coping on health even under severe stress (e.g. incarceration, family conflicts, negative life events; Greve & Enzmann, 2003; Greve et al., 2001; Kraaij et al., 2003; Santiago & Wadsworth, 2009). Second, in the phase of adolescence the repertoire of coping strategies increases (Aldwin, 2007; Seiffge-Krenke & Beyers, 2005; Zimmer-Gembeck & Skinner, 2011) and other coping strategies (e.g. rumination, avoidance) are the preferred choice (Aldwin, 2007; Hampel & Petermann, 2005, 2006, Zimmer-Gembeck & Skinner, 2011). Possibly, there are other available and (more) functional ways to cope with severe problems in adolescence than accommodative coping. Third, and most plausibly, it is conceivable that accommodation simply takes longer time to take effect on serious problems. Overcoming critical life events, such as the loss of a loved one or a divorce of the parents, can take plenty of time. The time interval of 12 months covered in Study 1 was possibly not enough to register the expected buffering impact of accommodative coping on the relation of severe stress and health.
Limitations and future implications
The two cross-validating analyses point out that much future research work has to be done. Moreover, some critical points concerning both studies have to be tackled in future. In the first instance, it is inevitable to further replicate the presented findings. Since the results of both studies are specific and thus allow only specific interpretations, the actual understanding about the influence of accommodative coping on health has to be deepened and extended in future. In following studies, it is not only necessary to extend the sample sizes (especially for Study 2) and age groups (especially younger samples are needed), but also the variable pool (e.g. further stressors and indicators for health, moderating variables). Moreover, both studies had only two measurement points. Prospective (cross-lagged panel) designs could include more than two waves (with shorter intervals) to investigate the coping process in more detail. A general limitation concerns the method of data collection: In both studies, data were exclusively assessed via questionnaires. Besides the question whether individuals are in general able to provide reliable and valid information on emotional data (Robinson & Clore, 2002), it remains an open question if our investigated age group (especially in Study 2) has already developed the necessary introspective abilities (Harter, 1999) for providing information on accommodative coping. An indicator for this limitation might be the internal consistencies of the applied scales in both studies. Further studies could include multiple data sources (e.g. implicit measures, judgment by parents or teachers). Moreover, the questionnaire assesses accommodative coping on a dispositional level. Coping reactions and their functionality, however, may be dependent on the specific context (Seiffge-Krenke, 1995; Vierhaus, Lohaus, & Ball, 2007). Upcoming studies should include measures on a dispositional and situational level as well.
Besides further investigation of the functionality of accommodative coping, future studies should also focus on the developmental pathways or shifting points (T. Thomsen, 2014) and the developmental conditions of accommodative coping in childhood and adolescence, as e.g. cognitive, social and emotional developmental conditions (Greve & Thomsen, 2013; T. Thomsen & Greve, 2013) or the impact of low mood or even depressive symptoms (Wrosch & Miller, 2009). Gaining knowledge about the functionality, development and especially the developmental conditions of accommodative coping is important if we want to promote successful development or health in children and adolescents. As children and adolescents are confronted with problems, it is inevitable to strengthen coping competencies that help the individual to overcome these obstacles and that lead to health and better adjustment. Our findings suggest that the support of accommodative coping resources in children and adolescents, e.g. by incorporating them into prevention and intervention programs, could be an important component for promoting individual health.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgment
A great thanks goes to Julia Pilatus (MSc. Psych.) for her help with the acquisition, data collection and statistical analyses of the data from Study 2.