
Abstract
This study investigated the psychometrics of a recently developed global rating measure of videotaped parent-infant interaction, the Manchester Assessment of Caregiver–Infant Interaction (MACI), in a normative sample. Inter-rater reliability, stability over time, and convergent and discriminant validity were tested. Six-minute play interactions were blind-rated by trained coders in 147 healthy mother-infant dyads at 3–10 months postpartum using the MACI; 51% were re-assessed 4 or 7 months later. Infant cognitive functioning, language and temperament, parent-reported infant warmth and invasion, parental mood, and the parent’s own recalled experiences of being parented were measured. We report the internal psychometrics of the MACI, evidence of stability as predicted, and inter-rater reliability. MACI caregiver sensitive responsiveness showed convergent validity with parental state of mind (mood at 3–4 months; report of own childhood care and overprotection), while MACI infant affect (but not the caregiver scales) was associated with parent-rated infant warmth. All MACI scales showed discriminant validity with concurrent cognitive and language developmental status, and most temperament dimensions. In conclusion, the MACI demonstrates utility, reliability and preliminary validity data in a normative sample, which complements previous work using the MACI. Follow-up is needed to test predictive validity. The findings inform further improvements to the tool, and may guide those looking for a relatively brief way to examine the global qualities of parent, infant and dyadic interaction.
Keywords
In recent years, epigenetic evidence that the early social environment shapes development at a neural level (Curley, Jensen, Mashoodh, & Champagne, 2011; Weder et al., 2014) and the development of new techniques for studying potential biomarkers of parenting (Swain, 2012) have fuelled interest in quantifying parent-infant interaction quality outside of the study of socioemotional development. This early environment, conceptualized as parent-infant interaction, plays an important role for a child’s social, cognitive and language development (Shin, Park, Ryu, & Seomun, 2008). Although attachment theory propelled the concept of “maternal sensitivity” into the research limelight, infant and dyadic features are also integral to interaction quality; infants influence caregiver behaviour (Feldman, Greenbaum, Mayes, & Erlich, 1997; Mills-Koonce et al., 2007) and vice versa, and the emergent qualities of the interaction may tell us more than the sum of each partner’s behaviours (Cohn & Tronick, 1988; Moore et al., 2013).
To a researcher or clinician new to this field, the array of existing measures of parent–infant interaction, spanning the fields of psychology, medicine and nursing, can be bewildering. Lotzin et al.’s (2015) systematic review identified 906 potentially relevant tools, the majority developed and used within single published studies or research groups. Measures differ substantially in their framework and specific variables of interest, and most lack norms and have limited published validation.
Manchester assessment of caregiver–infant interaction (MACI)
The MACI was designed as a global rating measure, covering general features of parent, infant and dyadic qualities of interaction. The aim was to encapsulate the quality of the infant’s likely early social environment as provided by the caregiver in continuous interaction with the infant’s behaviour. Its theoretical basis aligns with the transactional model of development (Sameroff, 2009) which emphasizes bidirectional processes at the level of gene–environment interactions, on the one hand, and at the level of parent–infant interactions (as a key part of the early environment), on the other, which probabilistically alter the child’s developmental trajectories. Since interaction quality is key to many areas of child psychological development, a global (rating) measure was selected, which, unlike most microanalytic measures, does not require special equipment, apart from video recording. Trajectories in, for example, socioemotional, cognitive or language development, are shaped by continuous parent–infant transactional processes, so a child’s developmental status is conceived as being somewhere along a continuum. Thus, a first requirement for a new measure was that its constructs and scale distributions would be suitable for high- and low-risk populations, since “high-risk” does not necessarily denote a negative outcome; the characterization of the full range of interactions is of interest. Many tools, by contrast, are developed for clinical or screening purposes, so are not designed to capture variation in the normative population. A second key requirement for this measure was that it would be relatively brief and valid for a wide age range across infancy in order to use repeatedly in longitudinal and evaluation studies.
The MACI was developed out of the need to encapsulate overarching (as opposed to fine-grained) qualities of the early caregiver–infant environment. Existing measures that offer breadth tended to involve multiple or complex scales, which are very time and/or resource-consuming to use, while brief measures tend to be specific, often focusing exclusively on caregiver behaviour (e.g., Ainsworth, Bell, & Stayton, 1971; Priddis & Kane, 2013; Svanberg, Barlow, & Tigbe, 2013). Of the 24 measures identified in Lotzin et al.’s (2015) systematic review of measures of parent and infant aspects of interaction, only five could be considered “brief” (< 10 items); these were either micro-analytic, designed for hospital or screening contexts, or specific in focus (e.g., on responsiveness). Furthermore, multi-scale measures tend to be later aggregated, and parental behaviour components are often highly concordant (Lohaus, Keller, Ball, Voelker, & Elben, 2004; Rueger, Katz, Risser, & Lovejoy, 2011). Since its development in 2008, and following extensive piloting and refinement, the MACI was finalized as a seven-scale measure, and used in several studies (Elmadih et al., 2014; Elsabbagh et al., 2015; Green et al., 2013, 2015; Wan et al., 2012, 2013, 2014), most notably in infants with familial risk of autism (see Supplementary material for further information).
This paper reports on the internal psychometric characteristics of the MACI in 147 healthy parent-infant dyads at 3–10 months postpartum, inter-rater reliability, consistency over several months, and convergent and discriminant validity. If the MACI taps into parent–infant interaction qualities, then a relatively consistent relational pattern is expected (excepting major life changes). Parental sensitivity is known to be moderately stable over time (Bigelow et al., 2010; Else-Quest, Clark, & Tresch Owen, 2011), while lower stability might be expected in infant interactive behaviour which is influenced also by developmental changes. Validity of the MACI was tested in the following ways: (1) Convergent validity 1: As parental cognitions concerning their infant’s relational behaviour are expected to be moderately correlated with observed interactive behaviour, is caregiver sensitive responsiveness or infant affect positively associated with parent-reported infant warmth? Are caregiver nondirectiveness and infant affect negatively associated with parent-reported infant invasiveness? (2) Convergent validity 2: As the psychological state of the parent is known to impact on parent-infant interaction (e.g., Murray, Fiori-Cowley, Hooper, & Cooper, 1996; Priddis & Kane, 2013), are MACI caregiver and dyad scales associated with general mood (particularly in the early postpartum) and parents’ perceived own experiences of being parented (as purported by the concept of the intergenerational transfer of the inner working model by attachment theory; Ainsworth, Blehar, Waters, & Wall, 1978)? (3) Discriminant validity: On the basis that the MACI has specificity to the caregiver-infant relationship, is the MACI independent of infant temperament, general developmental level and language skill?
Method
Sample
Three community-based samples in London and Manchester, UK, were recruited as part of larger projects aimed to understand aspects of parent–infant interaction in the normative population. Background and recruitment characteristics for the overall sample and by each “originating” sample are outlined in the Supplementary material. The samples were combined to maximize statistical power and to create a more representative sample than each individual sample would. Analyses of variance, controlling for infant age and socioeconomic status (highest occupational status in household), showed no significant differences between samples in any MACI scale (see Supplementary material). Of the 147 parent–infant dyads, all parents were the biological mother, aged 18–46 years (mean = 32.10; SD = 6.22) and their infants (80 female [54.4%]; 67 male [45.6%]) were aged between 3 and 10 months (mean = 5.44; SD = 1.81). Participants provided informed consent to be videotaped for the study as given a favourable opinion by the National Research Ethics Service Local Research Ethics Committees.
Parent–infant interaction recording procedure and the MACI
An episode of unstructured play interaction was video recorded with the parent–infant dyad sat on a floor mat either during a home visit or on university or clinic premises. The parent was instructed to engage in play as they would normally do at home for around 6–20 minutes (depending on the study), using a supplied set of developmentally appropriate toys, if they wished. Recording generally started following a brief period of familiarization, and was interrupted if the infant was distressed for an extended time (to be completed on another research visit, if possible).
Manchester assessment of caregiver–infant interaction
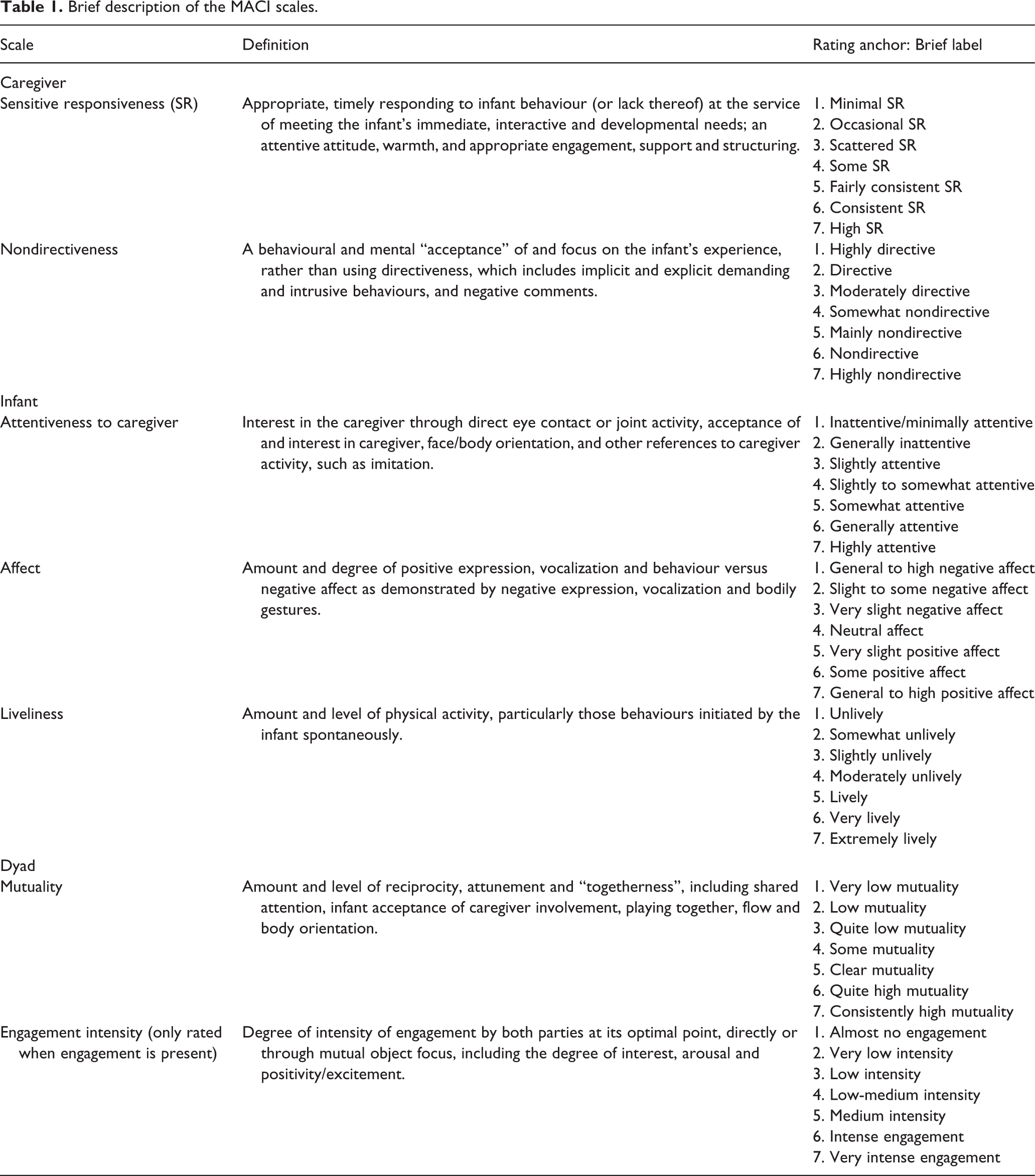
Seven rating scales cover broad aspects of interaction between a primary caregiver and their infant, each with a seven-point scale (Table 1; Manual outline available on request). Based on existing validated rating scales (Matias, 2006, Murray et al., 1996), the MACI has been modified and refined since 2008 to order to be suitable for 3–15-month-old infants, with a comprehensive coding manual and a training package (see Supplementary material for development and training details). Evaluation is based on 6 minutes of video-recorded continuous play interaction, starting once the dyad is settled in interaction yet the situation is still relatively new for the infant. Each recording is typically reviewed twice or more, pausing often to note the observational sequence and initial ratings in consultation with the manual, and then re-reviewed to finalize ratings.
Brief description of the MACI scales.
In the current study, parent–infant play interactions were also recorded at a second time point (“Time 2”) in 51% (N = 75) of the overall sample, comprising two subsamples, one at a mean interval of 16 weeks when infants were 7–9 months old (N = 30; 37.5% of the original group) and another at a mean interval of 29 weeks when infants were 12–14 months old (N = 45; 95.7% of the original group). All video recordings were rated by trained and reliable graduate research assistants, blind to all family information, and a randomly-selected subsample (30%; N = 44) was independently blind rated by one of three trained raters to test inter-rater reliability. Of all cases rated at Time 2, 32% (N = 24) were independently re-rated by one of two raters.
Other measures
The following measures were parent completed (except the Mullen Scales of Early Learning) on the same research visit.
Mother object relations scale – short form (MORS-SF; Oates & Gervai, 2003)
This screener identifies potential areas of difficulty in the early relationship by asking mothers about their perceptions of their infant’s behaviours, cognitions and emotions, producing two domains: “warmth” (7 items; e.g., “My baby smiles at me”) and “invasiveness” (7 items; e.g., “My baby wants too much attention”). This measure has utility in clinical and research settings (Davies, Slade, Wright, & Stewart, 2008; Milford & Oates, 2009).
The Edinburgh postnatal depression scale (EPDS; Cox, Holden, & Sagovsky, 1987)
This widespread and validated (Gibson, McKenzie-McHarg, Shakespeare, Price, & Gray, 2009) 10-item postpartum depression screen includes items related to own cognitions, affect and behaviours. In the community, EPDS scores show gradual intra-individual decrease over the first year, but also substantial stability (Heron et al., 2004). At 4 months postpartum, even mild EPDS symptomatology is related to lower-quality bonding (Moehler, Brunner, Wiebel, Reck, & Resch, 2006).
Parental bonding instrument (PBI; Parker, Tupling, & Brown, 1979)
This validated measure of an adult’s subjective experience as a child of being parented to the age of 16 years includes 12 “care” items (e.g., “How much did he or she understand your problems and worries?”) and 13 “overprotection” items (e.g., “How much did he or she baby you?”) concerning parenting behaviours received by the adult. The PBI demonstrates stability over a 20-year period (Wilhelm, Niven, Parker, & Hadzi-Pavlovic, 2005). This study used averaged scores between parents for each domain, unless they had been raised by a single parent.
The infant behaviour questionnaire – revised (IBQ-R; Gartstein & Rothbart, 2003)
This validated measure of infant temperament (Parade & Leerkes, 2008) for 3–12-month-olds contains 191 items, averaged to create 14 subscales: Activity level, distress to limitations, fear, duration of orienting, smile/laughter, high pleasure, low pleasure, soothability, falling reactivity, cuddliness, perceptual sensitivity, sadness, approach and vocal reactivity.
Mullen scales of early learning (MSEL; Mullen, 1995)
This standardized test of cognitive and motor development, administered by a trained examiner, contains five scales: Gross motor, Visual reception, Fine motor, Expressive language and Receptive language. Widely used in developmental disorder studies, it was validated originally and recently (Swineford, Guthrie, & Thurm, 2015) in normative samples. The current study focused on the Early Learning Composite (ELC; sum of scales except Gross motor), as a measure of general development, and the language scales.
Results
Internal psychometrics and background characteristics
MACI ratings for each scale were generally well distributed (see Supplementary material). However, infant affect and infant liveliness did not receive any “1” or “7” ratings. Most MACI scales were positively inter-correlated, except infant liveliness, which was correlated only with mutuality (r = .18) (see Supplementary material). Although caregiver sensitive responsiveness and caregiver nondirectiveness were correlated (r = .63), the former was significantly correlated with infant affect (r = .25) and dyad engagement intensity (r = .42), while the latter showed only trend level associations (r = .15 and r = .16, respectively). Mutuality, a dyad scale, was correlated with infant attentiveness (r = .76) and caregiver sensitive responsiveness (r = .76), while dyad engagement intensity was most closely associated with mutuality (r = .67) and infant attentiveness (r = .62).
Controlling for “originating sample”, the following sociodemographic factors were significantly correlated with the MACI: Infant liveliness with infant age (r = .24; p = .003), and caregiver sensitive responsiveness with socioeconomic status (highest occupational status in household) (r = −.26; p = .001). The MACI was not correlated with parent age or birth order; neither did ANOVA’s show infant gender or ethnicity (Caucasian vs. non-Caucasian) effects, after controlling for infant age. All subsequent analyses controlled for “originating sample”, infant age and socioeconomic status.
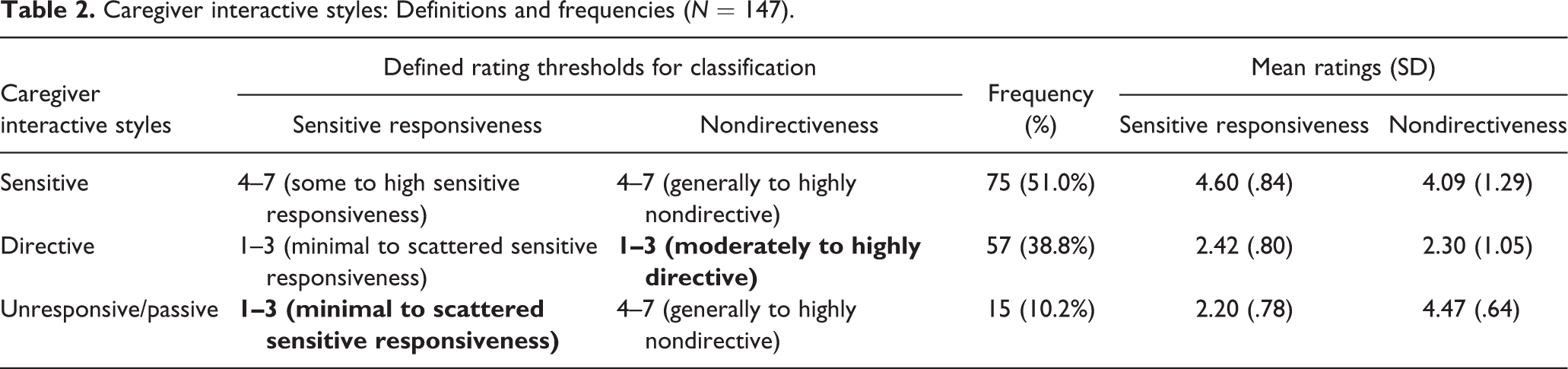
The underpinning rationale for having two caregiver scales in the MACI is that, despite an expected high concordance between these scales, some caregivers would exhibit low “sensitive responsiveness” yet high “nondirectiveness”. This “passive/withdrawn” profile is suggested to show different developmental sequelae from directive patterns (e.g., Field, Hernandez-Reif, & Diego, 2006; Hart, Jones, Field, & Lundy, 1999). Using simple conceptually-defined thresholds on these two scales (Table 2), we derived three caregiver interaction “profiles”: sensitive, directive, and unresponsive/passive. Consistent with this notion of three profiles, while most low-sensitive responders were directive, 10.2% were classed as unresponsive/passive. Further supporting the three profiles, none were rated as both directive and sensitively responsive.
Caregiver interactive styles: Definitions and frequencies (N = 147).
Inter-rater reliability
Intraclass correlations (ICC), as recommended for ordinal/interval data (Hallgren, 2012), in a two-way random effects model (single measures, absolute agreement) yielded the following: [Time 2 in square brackets]: Caregiver sensitive responsiveness: r = .75 [.77]; caregiver nondirectiveness r = .66 [.80]; infant attentiveness to parent: r = .67 [.74]; infant affect: r = .72 [.78]; infant liveliness: r = .62 [.52]; mutuality: r = .77 [.70]; engagement intensity: r = .70 [.64]; all p < .001. For ICC cut-offs for agreement levels of qualitative ratings, Cicchetti (1994) recommended that r = .40−.59 is fair, .60−.74 is good, and .75+ is excellent.
Consistency over time
Based on N = 75 with repeated MACI measurement, the caregiver scales overall showed quite high consistency, particularly for the 16-week interval (between a mean of 4 months and 8 months) in the younger subsample (Table 3). Infant attentiveness and the dyad scales demonstrated low to moderate consistency, this time the older subsample showing stronger age-to-age correlations than the younger group. No consistency was found in infant liveliness (trend only) or infant affect.
Consistency of parent-infant interaction in two samples, controlling for infant age at first measurement and interval between assessments.

†p < .1; *p < .05; **p < .01; ***p < .001. aControlling also for originating sample.
Convergent and discriminant validity
Descriptive and other statistics for all variables measured to test the validity of the MACI are provided in the Supplementary material (Table A3).
MACI and MORS-SF are proposed measures of parent-infant relations: MORS-SF examines parents’ self-reported regard for her infant as “warm” and/or “invasive” as an indirect measure of relational difficulties between the parent and infant; these constructs sit closest theoretically to sensitive responsiveness and “directiveness” (low nondirectiveness) respectively on the caregiver’s side of the interaction, and “affect” on the infant side. Analyses were performed for two age groups: 3–4 months (N = 63) and 5–10 months (N = 34), given the possible impact of parental role adjustment in the early postpartum and/or of infant age. MORS-SF “warmth” was positively correlated with infant affect in the 3–4-month group (r = .38; p = .002), while MORS-SF “invasiveness” was negatively correlated with infant affect in the 5–10-month group (r = −.38; p = .03). Neither MORS-SF dimension was correlated to the caregiver scales.
To test whether parental and dyadic aspects of interaction were associated with parental mental state, we used the EPDS and PBI. Seven parents screened positive for depression (EPDS >12), so scores were used as a continuous measure of depressed mood. In the 3–4-month group (N = 66), EPDS was negatively correlated with caregiver sensitive responsiveness (r = −.29; p = .02) and, at trend level, mutuality (r = −.23; p = .07). No effects were found in the 5–10-month group (N = 34). Of those measured on PBI (N = 80), sensitive responsiveness was correlated with PBI care (r = .31; p = .006) and at trend level with overprotection (r = −.21; p = .07). Without controlling for SES, their correlations were stronger: r = 33. p = .003 and r =−.23; p = .04, respectively. A negative association emerged between mutuality and PBI overprotection (r = −.25; p = .03), while it was unrelated to PBI care.
Discriminant validity was tested by correlating the 14 IBQ temperament dimensions with MACI (N = 45). Three of 98 calculations were significant: Cuddliness with sensitive responsiveness (r = .32; p = .03), falling reactivity/recovery from distress with nondirectiveness (r = .31; p = .04), and sadness with liveliness (r = .32; p = .04). Therefore, the MACI was unrelated to most affective (e.g., high intensity pleasure, low intensity pleasure, distress to limitations, and soothability) and socially-related dimensions (e.g., vocal reactivity, duration of orienting, smile and laughter). Approach showed trend associations with infant attentiveness (r = .27; p = .08), mutuality (r = −.28; p = .07) and engagement intensity (r = −.29; p = .06), and fear with MACI infant affect (r = −.28, respectively; p = .08). MACI ratings were not associated with concurrently measured MSEL ELC standard scores, receptive language or expressive language (N = 47).
Discussion
Overall, the MACI scales demonstrated a range of evidence for consistency, reliability and validity in a relatively large normative sample. This was strongest in caregiver sensitive responsiveness, which showed convergent validity with three variables concerning parental state of mind: mood at 3–4 months postpartum, reported parental care received by own parents at 3–4 months postpartum, and reported (low) overprotection received by own parents and at 5–10 months. These associations were moderate, as we might expect from a normative sample. Moreover, both caregiver scales evidenced discriminant validity with infant developmental level, language and all temperament dimensions, except for two moderate associations with emotion-related areas of temperament (cuddliness and falling reactivity). Such correlations are perhaps unsurprising given that parental interactions may be affected by these infant tendencies, or that such infant tendencies may partially be determined by parental response.
We expected parent-rated infant warmth and invasiveness to be related to how parents actually interact with their infant, but our findings suggest that they reflect infant affect during play interaction instead (see in what follows). This could be because the MORS was designed specifically for identifying those at risk of relational difficulties, such that we would only expect an association with parental behaviour where relational difficulties existed. Although we selected the MORS-SF as an indirect measure of parent–infant relations designed to minimize social desirability bias (by asking the parent about the infant’s behaviour and affect towards her, rather than asking directly about how she feels about the infant), a more suitable test of validity would be a direct observational measure not designed for clinical purposes.
Although the two caregiver scales were highly correlated, as previously found (Wan et al., 2014; Elsabbagh et al., 2015), our findings in this relatively large sample confirm that they are useful to differentiate, firstly because we theorized and confirmed that a proportion of those rated as low-sensitively-responsive would have a passive “profile” and therefore show high nondirectiveness, and secondly because sensitive responsiveness was associated with infant affect and engagement intensity, while nondirectiveness was not. The current findings suggest that four in every five low-sensitively responsive parents are directive while one in five tends to be passive. The maternal depression literature has emphasized this distinction as carrying different developmental consequences (e.g., Field et al., 2006; Hart et al., 1999); further longitudinal work is needed to verify whether these MACI profiles hold predictive validity and for a fuller developmental picture.
The infant scales were less related to one another than the caregiver scales, each with somewhat differing characteristics, and all independent of general developmental level and language. Infant attentiveness to caregiver was the only infant scale to show stability, in older infancy, and as might be expected, it was quite highly correlated with caregiver sensitive responsiveness. By contrast, infant affect demonstrated no stability, which may suggest situational specificity; however, it showed convergent validity with parent-reported infant warmth and (inversely with) parent-reported infant invasiveness, and discriminant validity with emotional dimensions of temperament. On the other hand, infant liveliness seemed to be independent from all other MACI scales, also found previously in infants at risk of autism (Wan et al., 2012). In the current study, liveliness was positively correlated only with temperamental sadness, an unexpected finding that could be explained by a larger variance in liveliness in a normative sample accounted for by negative behaviours, such as restlessness and fretfulness rather than positive aspects of interaction; only microanalytic procedures could confirm whether this is the case.
Our findings inform further refinements to the MACI. Notably, inter-rater agreement was good or excellent (Cicchetti, 1994) on all scales at 3-10 months and at follow-up (7-9 or 12-14 months), with the exception of later infant liveliness. By re-examining clips with the raters, we found that this was due to raters’ differentially accounting for developing motor skill in their evaluations, further supported by the fact that liveliness was the only MACI scale to show an age effect. The coding manual and training have since been adjusted to more definitively take into account motor-skill changes. Secondly, coders found infant affect to be difficult to code on a single construct from negative to positive when infants often presented varying degrees of both. Subsequently, affect has been separated into two scales, positive affect and negative affect, allowing clearer, finer grained ratings.
However, several limitations must be considered in the interpretation of the results. Firstly, although we found no MACI differences by ethnicity in this sample, our sample was predominantly non-Caucasian. One recruitment stream had excluded non-Caucasian mothers, thus limiting external validity. Secondly, play interaction location was not consistent across (or even within) the originating samples, and sometimes changed between time points. As such, stability over time might have been higher had the setting remained the same, although no significant MACI differences emerged by originating sample, and within-sample differences in location were mostly due to parental preferences. Thirdly, tests of validity relied mostly on parent reports and parent measures, which limited validation of the infant and dyad MACI scales. Direct child social and socioemotional measures are needed to test the concurrent and predictive validity of the MACI.
The MACI is a brief rating tool that offers breadth by assessing infant and dyadic as well as parental interactive behaviours. Its conceptual roots in Sameroff’s (2009) transactional model of development emphasizes the dyadic experience in the early social environment, rather than implicating attachment difficulties per se. However, as a global measure, the MACI is not designed to identify specific behaviours or capacities within interaction, or to delineate temporal processes, for which numerous microanalytic and detailed measures are available (Lotzin et al., 2015). In this report, the MACI demonstrated utility, reliability and encouraging evidence of convergent and discriminant validity in the normative population, strengthening previous work of its use in at-risk and small community samples (e.g., Wan et al., 2012, 2013, 2014). The findings inform refinements to the measure and further understanding of its psychometrics. Going forward, further work is needed to test the MACI in relation to future social, socio-emotional and cognitive developmental trajectories, and the development of a modified MACI for toddlers has been developed to facilitate longitudinal studies.
Footnotes
Acknowledgements
We are very grateful for the participation of the families, which helped contribute enormously to the development of this measure. In part, the research is supported by UK Economic and Social Research Council (RES-000-22-3525) to M.W. Wan and J. Green, The UK Medical Research Council (G0701484) and the BASIS funding consortium led by Autistica (![]() ) to M.H. Johnson. We thank Hanna Venton-Platz and Faye Plummer for their valuable coding work. Substantial contributions were made to data collection by The BASIS team (in alphabetical order): Simon Baron-Cohen, Rachael Bedford, Patrick Bolton, Susie Chandler, Tony Charman, Mayada Elsabbagh, Janice Fernandes, Holly Garwood, Teodora Gliga, Kristelle Hudry, Mark Johnson, Greg Pasco, Evelyne Mercure, Leslie Tucker, and Agnes Volein.
) to M.H. Johnson. We thank Hanna Venton-Platz and Faye Plummer for their valuable coding work. Substantial contributions were made to data collection by The BASIS team (in alphabetical order): Simon Baron-Cohen, Rachael Bedford, Patrick Bolton, Susie Chandler, Tony Charman, Mayada Elsabbagh, Janice Fernandes, Holly Garwood, Teodora Gliga, Kristelle Hudry, Mark Johnson, Greg Pasco, Evelyne Mercure, Leslie Tucker, and Agnes Volein.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: The research is supported in part by UK Economic and Social Research Council (RES-000-22-3525) to M.W. Wan and J. Green, The UK Medical Research Council (G0701484) and the BASIS funding consortium led by Autistica (![]() ) to M.H. Johnson.
) to M.H. Johnson.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.