
Abstract
The transition to adulthood is a critical juncture in the course of psychopathology. This study examined the ways in which earlier capacity to deal with relationship stress during adolescence contributed to an adaptive outcome in emerging adulthood. In a prospective study of 145 individuals, relationship stress, individual coping capacities, and perceived support from fathers, mothers, and peers were analyzed, when the participants were 13 and 17 years old. The effects of these earlier capacities to deal with relationship stress on health outcomes were examined in young adulthood (age 23). Gendered pathways to young adults’ symptomatology emerged. Females experiencing earlier relationship stress, but also support by mothers, fathers, and friends, showed less symptomatology at age 23. In addition, females’ withdrawal coping mediated the impact of stressful encounters on later internalizing symptomatology. In contrast, earlier coping with relationship stress was not found to be predictive for males. Earlier support from parents or friends was associated with later externalizing symptomatology in young men. Reasons for the gender-specific pathways to symptomatology are discussed.
Several studies have shown that during adolescence the number of stressors and conflicts in close relationships increase, because the time invested in and the quality of existing relationships with parents and peers are altered (Laursen, Coy, & Collins, 1998; Schad, Szwedo, Antonishak, Hare, & Allen, 2008). Simultaneously, support provided by parents and peers may buffer against the detrimental effect of stress on health (Windle, 1992). Given the frequency of conflicts in close relationships with parents and peers, the individual’s capacity to manage these conflicts is critically important to maintain the relationships (Seiffge-Krenke, 2011). Moreover, the ways in which adolescents cope with these stressors will have an impact on current and future adjustment, especially considering that psychosocial stress during this developmental period is a significant and pervasive risk factor for psychopathology (Compas, Connor, Osowiecki & Welsh, 2001).
In fact, the transition to adulthood is a critical juncture in the course of psychopathology and mental health (Schulenberg, Sameroff, & Cicchetti, 2004). Several studies have noted an increase in psychopathology in emerging adults compared to adolescents (Galambos & Kotylak, 2012; Schulenberg, Bryant, & O’Malley, 2004), relating it to the many changes in their social and professional world. The extent that earlier competence and support experienced during adolescence effect later mental health in a developmental period characterized by strong demands is still unclear. To address this lack, we examined the long-term impact of managing relationship stress during adolescence on the individuals’ adaptive outcome in emerging adulthood.
Changes in Relationships with Parents and Peers, Support, and Ways of Coping with Relationship Stress
Studies on North American and European adolescents have shown that stressors in the relationship with parents and peers result from normative developmental changes in the functions and significance of these close relationships (Laursen, Coy, & Collins, 1998; Steinberg, 2001). Adolescents’ attempts to establish more mature, egalitarian relationships with their parents often results in conflictual, stressful interactions (Branje, van Doorn, van der Valk, & Meeus, 2009), particularly when parents intervene in their children’s friendships (Soenens, Vansteenkiste, & Niemiec, 2009). Relationships with peers change dramatically, marked by the emergence of more intimate friendships based on trust and loyalty. Peer rejection is considered to be quite stressful (Sentse, Lindenberg, Omvlee, Ormel, & Veenstra, 2010), and these stressors may add to the stress experienced in parent-adolescent relationships.
Parent-child relationships are characteristically obligatory and hierarchically structured. In contrast, adolescents’ relationships with peers are more voluntary and characterized by more flexibility, mutuality, and willingness to compromise (Adams & Laursen, 2007). These qualitative and structural differences may also have a bearing on the coping strategies adolescents use when coping with stressors associated with these two kinds of interpersonal relationships.
Coping has been defined as an active, purposeful process of responding to stimuli appraised as taxing or exceeding personal resources (Skinner, Edge, Altman, & Sherwood, 2003). Research on adolescent samples has generated a three-dimensional model, including active coping (support-seeking and discussing the problem with concerned persons), internal coping (cognitive ways of dealing with stress such as considering possible solutions and anticipating results), and withdrawal from the stressor (distraction strategies and seeking emotional outlets; Skinner & Zimmer-Gembeck, 2007). Our study draws on this three-dimensional framework that subsumes the voluntary, behavioral, emotional, and cognitive responses adolescents use to cope with relationship stress (Compas, et al, 2001; Seiffge-Krenke, 2011). When confronted with relationship stressors, most adolescents employ two adaptive modes of coping: active support-seeking and internal reflection of possible solutions (Seiffge-Krenke, Aunola, & Nurmi, 2009; Skinner et al., 2003). The frequency of strategy use seems to be dependent on relationship type. In stressful encounters with peers, active coping tends to be used more often than in stressful conflicts with parents. In general, withdrawal strategies are used much less frequently than active support-seeking and internal reflection (Bowker, Bukowski, Hymel, & Sippola,. 2000; Seiffge-Krenke, 2004). However, the long-term use of withdrawal as a coping style in dealing with relationship stress has negative health consequences (Clarke, 2006). Bearing this result in mind, we examined the prospective impact of earlier withdrawal coping on later health outcomes during emerging adulthood.
Although perceived stress in close relationships relates to negative affect, conflicts, and unconstructive negotiation, relationships with parents and peers are also a frequent source of support. Support relates to a sense of interpersonal warmth, closeness, and understanding. The stress-buffering model (Windle, 1992) asserts that social support mitigates the relationship between stressful encounters and adolescents’ internalizing symptoms such as depression. However, supportive relationships with peers and parents during stressful times are differently related to adolescent mental health outcomes (Colarossi & Eccles, 2003). Deficits in parental support but not in peer support predicted future increases in depressive symptoms (Stice, Ragan, & Randall, 2004). Moreover, parents’ consistent and supportive behavior was positively associated with their children’s adaptive coping (e.g. their use of support-seeking coping when relationship stressors emerge), and this adaptive coping, in turn, was negatively associated with adolescents’ symptomatology (Rodrigues & Kitzmann, 2007; Klink, Byars-Winston, & Bakken, 2008).
Given the challenging nature of emerging adulthood, investigating the extent that adaptational processes during adolescence (e.g. coping with relationship stress and parent and peer support in dealing with these stressors) affect health in this later developmental phase is important for this line of research. The evidence is unclear as to whether such adaptational processes during adolescence have a long-reaching influence. Hence, we aimed to analyze their effects on health outcomes six years later on individuals who had become young adults.
The Gendered Perspective
Marked gender differences have been reported for stress perception and the use of different coping strategies. Research converges on findings that females are more sensitive to relationship stress but also more likely to use copings strategies that involve relationships. Compared to males, females report higher levels of stress experienced with parents and peers but also show more active coping in dealing with stressors in these domains (Seiffge-Krenke, 2011; Tamres, Janicki, & Helgeson, 2002; Washburn-Ormachea, Hillman, & Sawilowsy, 2004). Females also score higher in symptomatology, particularly in internalizing symptoms during adolescence (Rescorla et al., 2007) and in emerging adulthood (Schulenberg & Zarett, 2006). The gender differences found in this line of research and the prospective relationships between social support and symptomatology warrants further investigation of differential directions of effects of parent and peer support for males and females.
Despite widespread agreement that parental support predicts important aspects of adolescent functioning, adolescent relationships differ between their mother and father in quality and potential implications for current and future adaptation. Studies have demonstrated that relationships with mothers are closer but also involve higher levels of conflict than those with fathers (Scharf & Mayseless, 2008; Seiffge-Krenke, Overbeek, & Vermulst, 2010). Furthermore, the mother-daughter dyad is much closer than all other dyads in the family (Mayseless, Wiseman, & Hai, 1998). Research suggested that mothers are more effective at meeting emotional needs (Chodorow, 1978) and that fathers are better suited to discipline than mothers (Barber, Stolz, Olsen, & Maugham 2005). These findings seem to suggest that fathers and mothers promote their children’s well-being in different ways. Although both daughters and sons tend to experience closer and more supportive relationships with their mother, and this has been linked to less internalizing behavior (Steinberg, 2001), their father’s support tends to be consistently more predictive of less externalizing behavior, especially for sons (Carlson, 2006). Thus, a father’s role during the adolescent years is characteristically different and complementary to the role of mothers (Russel & Saebel, 1997; Stolz, Barber, & Olsen, 2005) which may also influence their function as support providers.
The Present Study and Hypotheses
Compared to research in North America, Europe has produced a dearth of research in examining adolescent antecedents of adjustment problems in emerging adulthood. We found no published German studies to date that examine the long-term impact of support and coping on adaptation in emerging adulthood. Similar to North American emerging adults, young Germans also have difficulties in balancing often conflicting challenges and demands (Seiffge-Krenke & Luyckx, 2014; Luyckx, Seiffge-Krenke, Schwartz, Crocetti, & Klimstra, 2014), and they experience this period as quite stressful (Seiffge-Krenke, 2015). German nationwide surveys have shown increases from adolescence in prevalence rates of overall symptomatology between the ages of 18 to 30 in which these challenges are mirrored (Lambert et al., 2013). The increases in internalizing psychopathological symptoms such as depression are particularly high, with rates for females two to three times higher than for males (Jacobi & Gross, 2014). The extent that the earlier capacity to manage relationship stress during adolescence impacts adaptation in emerging adulthood is yet to be explored. We therefore conducted this study on young people in Germany, following our cohort over 10 years from the critical period of adolescence until emerging adulthood.
Our longitudinal study examined the contributions of adaptational processes during adolescence on psychopathology during emerging adulthood. Similar to adaptive functioning at emerging adulthood, the interface of social changes and coping is important in adolescence. We focused on two central dimensions of close relationships: perceived support and stress in parent-child relationships and peer relationships, which were assessed at age 13 and 17. During this time, we also explored the capacity of adolescents to competently solve relationship stressors in the domain of parents and peers. To provide information on the long-term impact of managing relationship stress with parents and peers during adolescence on the adaptational outcome in emerging adulthood, we assessed different health indices (i.e. their internalizing and externalizing symptomatology and other symptoms) at age 23. We expected that the ways young people experience support by parents and peers and cope with relationship stressors during the critical period of adolescence would have a bearing on their adaptation in later transition periods, for example, during emerging adulthood.
We approached our research questions from a gendered perspective. In accordance with other studies, we expected adolescent females to report greater relationship stress than males, especially with respect to peer-related stress (Bowker et al., 2000) and that these higher stress levels would later contribute to higher levels in psychopathological symptoms for females. Based on previous studies showing that females are more likely than males to use cooperative, prosocial approaches of coping with relationship stress, especially when peers are involved (Noakes & Rinaldi, 2006; Tamres, et al, 2002), we expected females in our study to generally use more active coping than boys, particularly in the peer domain. In general, we expected that a more dysfunctional coping style (e.g. withdrawal) would later contribute to high levels of psychopathological symptoms for males and females, whereas a more active style in approaching relationship stressors would be linked with low symptomatology. For females, a stable use of withdrawal coping during adolescence would later be linked with high levels of internalizing symptomatology.
Given that adolescents’ relationship with their mothers tends to differ from their relationship with their fathers in quality and potential impact on later outcomes, we planned to run separate models for perceived support from fathers and perceived support from mothers and the long-term implications for internalizing and externalizing symptoms of their offspring. As detailed above, parents are an important source of support during adolescence, but this function may be gradually transferred to peers. Therefore, we ran separate models that included peer stress, perceived peer support, and coping with peer stress during adolescence to assess the extent that these factors predict externalizing behavior, internalizing behavior, and other symptomatology at age 23.
Method
Sample
The sample was part of an ongoing longitudinal study of 198 participants. The complete datasets obtained during a period of 10 years from 145 participants were used for the present study. Assessments were made in a total of eight waves with varying intervals. For this study, data from Wave 1 (n = 198; MAGE = 13.60, SD = 1.40) and wave 2 (n = 169; MAGE = 17.00, SD = 1.32) during adolescence, and from Wave 3 (n = 145; MAGE = 23.00, SD = 1.40) in emerging adulthood were used. The distribution of females (n = 80) and males (n = 65) can be considered balanced. The participants were recruited from 7th-grade classes in German schools. Of all adolescents targeted, 88% agreed to participate. Participation in the longitudinal study was contingent on receiving informed consent from the potential participants’ parents. The original sample for the project was selected according to socioeconomic background, parents’ marital status, parents’ and adolescents’ educational levels, and the number of children in the family (German Federal Bureau of Statistics, 2000). The sample was representative for German samples with respect to parents’ marital status (82% participants lived in intact families; 18% lived with a single parent), number of children in the family (M = 1.24, SD = 0.63), SES (53% middle class), and nationality (93% were German nationals). Education level at age 19 was as follows: 48% of the participants had received their Abitur after 13 years of education (the highest level in the German secondary school system), 23% attended school between 10 and 12 years and 1% had no final school qualification. At age 23, the proportion of those studying (43%), in vocational training (12%), or working (35%) represents a typical distribution for young Germans at this age; 10% were housewives. As is typical for young adult Germans (Seiffge-Krenke, 2006), 29% of the participants were still residing with their parents, 21% lived with a partner, and the remaining participants either lived alone or in shared apartments.
Measures
Parent- and peer-related stress
Adolescent stress at ages 13 and 17 years was measured by the Problem Questionnaire (PQ; Seiffge-Krenke, 1995), which assesses the perceptions of minor stressors in seven stress domains. The instrument consisted of 64 items that earlier studies have frequently named as typical and salient everyday stressors. Adolescents were asked to indicate the stressfulness of a specific problem, ranging from 1 = not stressful at all to 5 = highly stressful. Factor analysis revealed the following seven domains: problems with school, problems with future, problems with parents, problems with peers, problems with leisure time, self-related problems, and problems related to romantic relationships. In the present study, we used seven items pertaining to the domain of parental stress (e.g. “My parents don’t let me make my own decisions”, α = .85) and seven peer stress items (e.g. “I am unsure whether the others will accept me”, α = .79).
Coping with parent- and peer-related stress
At ages 13 and 17 years, participants completed the Coping Across Situations Questionnaire (CASQ; Seiffge-Krenke, 1995), which assesses 20 coping strategies across eight problem domains. Participants mark which of the coping strategies they use frequently in a given domain (0 = strategy not used; 1 = used). For the present study, we selected the parents and peers domain to complement the corresponding stress domains. Participants were required to mark all coping strategies they regularly used when a stressor in the respective domain occurred. Confirmatory factor analysis revealed three different coping styles (Persike & Seiffge-Krenke, 2015). The first style, termed Active Coping, explained 36% of the variance and comprised eight items that assessed coping strategies such as “I discuss the problem with my parents” or “I try to solve the problem with the help of my friends” (α = .85). The second style, termed Internal Coping (22% of variance explained), included four items that tapped coping strategies such as “I think about the problem and try to find a solution” (α = .81). The third style, termed Withdrawal (11% of variance explained), had five items pertaining to coping strategies such as “I withdraw because I cannot change anything anyway” (α = .80). The means of the three CASQ subscales range from 0 (none of the coping strategies constituting the scales are used) to 1 (all coping strategies are used).
Perceived parental and peer support
At ages 13 and 17, participants completed the Network of Relationships Inventory (NRI; Furman & Buhrmester, 1985), responding to items that assessed maternal, paternal, and peer support (the same items were used for each relationship). In accordance with Furman & Buhrmester, we used the following seven of the original 10 subscales: companionship, instrumental aid, satisfaction, nurturance, affection, admiration, and reliable alliance (each with three items). A sample item for the social support scale is: “How much does this person help you when you need to get something done?” Participants rated the items on a scale ranging from 1 (little or none) to 5 (the most). Means were computed for each subscale, creating separate scores for each relationship for each time of measurement. Internal reliability was high for perceived maternal social support (α = .80 to. 82), for perceived paternal social support (α = .82 to .84), and for peer support (α = .81 to .85).
Internalizing, externalizing and other symptomatology
At age 23, the participants’ levels of psychopathology were assessed by their responses to the Young Adult Self-Report (YASR, Achenbach, 1997). This instrument is a 119 item self-report scale that measures problem behavior, with an answer format of 1 = not true, 2 = somewhat or sometimes true, and 3 = often or very often true. The YASR includes broad-band syndromes of externalizing (delinquent, aggressive) and internalizing behavior (anxious/depressed, withdrawn). Symptomatology during emerging adulthood may entail a number of additional symptoms beyond externalizing and internalizing behavior. Thus, we used three narrow-band problem scores of the YASR (i.e. somatic complaints, attention problems, thought problems), for the “other symptomatology” score. All scores were computed as arithmetic means of all comprised items or scales. Cronbach’s alpha was 0.83 for internalizing, 0.89 for externalizing and 0.86 for the third symptomatology score.
Plan of Analysis
Owing to the small sample size, we ran separate two-group models (one for male and one for female participants) for perceived stress, fathers and mothers support at age 13 and 17, and the prospective effects of these factors on internalizing and externalizing and other symptoms (age 23). We expected to find that adolescent females, when they experience parental support and in particular when they experience maternal support for ongoing relationship stress in the adolescent period, would show less internalizing symptomatology as emerging adults. Then, we ran separate models that included peer stress and perceived peer support during adolescence as predictors of symptomatology (externalizing, internalizing, and other symptoms) at age 23. Although existing research is not clear in this respect, we hypothesized that peer support for males and females who simultaneously experienced peer stress during adolescence may buffer the adverse effects of stress and thus contribute to low symptomatology (both externalizing and internalizing) in emerging adulthood. In addition, we ran models in which we controlled for all three coping dimensions and their effect on the outcome variables, although we expected that only the persistent use of withdrawal would have predictive power. Thus, a third path analysis was conducted with perceived stress and coping (active, internal, withdrawal) during adolescence and their prospective effects on health outcomes during two times at emerging adulthood. We expected, in accordance with previous literature, that females’ consistent use of withdrawal during adolescence would be linked with stronger internalizing in emerging adulthood. It is possible, that males’ consistent use of withdrawal during adolescence is linked with stronger externalizing when they become emerging adults. Differences in path coefficients between the male and female groups were measured using Wald tests.
Results
Missing Value Analysis
Combined across all waves of this study, a total of 5.01% of the data was missing. MCAR test of all variables in the path model failed to reach significance (x2 = 32.2, df = 25, p = .151), suggesting that missing data may have occurred at random. Missing values at all waves were therefore estimated using multiple imputation (Schafer, 1997), resulting in N = 145 (n = 80 females) for all subsequent analyses.
Path Modelling
We conducted two sets of path analyses to predict externalizing behavior, internalizing behavior, and other symptomatology at age 23 from a number of variables at ages 13 and 17. Model fit was assessed on the basis of a combined evaluation of multiple fit indices (Cheung & Rensvold, 2002). Fit was considered good, with root mean square error of approximation (RMSEA) < .08, comparative fit index (CFI) > .92, and standardized root mean squared residual (SRMR) < .08.
Descriptive statistics for all variables comprised in the path models are provided in Table 1. Of note are gender differences with larger stress levels in peer-related stress in females and more active and internal coping styles in dealing with peer-related stress at age 13. At age 23, females reported significantly higher scores for internalizing behavior than males.
Group Comparisons for Model Variables.
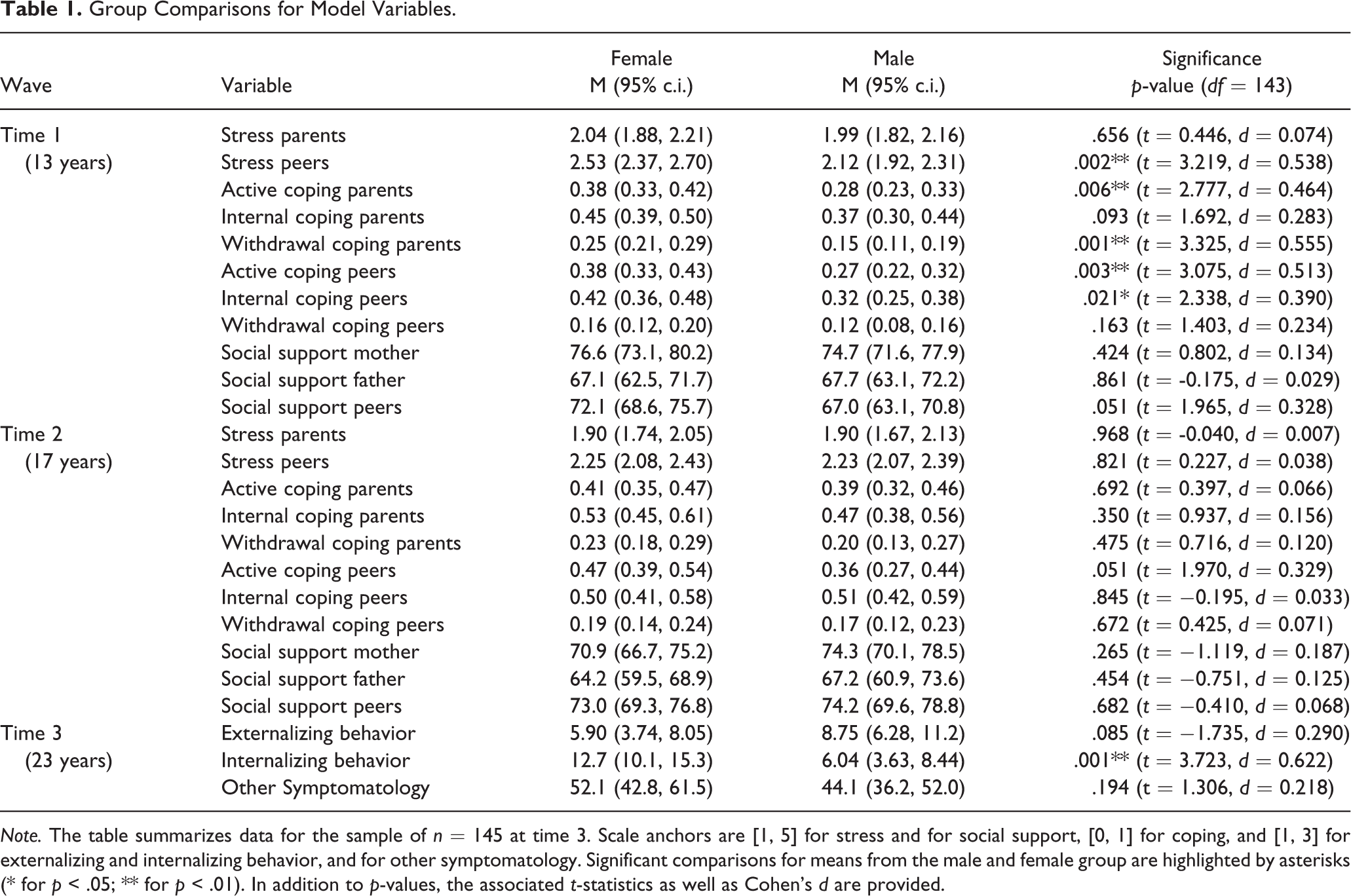
Note. The table summarizes data for the sample of n = 145 at time 3. Scale anchors are [1, 5] for stress and for social support, [0, 1] for coping, and [1, 3] for externalizing and internalizing behavior, and for other symptomatology. Significant comparisons for means from the male and female group are highlighted by asterisks (* for p < .05; ** for p < .01). In addition to p-values, the associated t-statistics as well as Cohen’s d are provided.
Predicting symptomatology from earlier maternal support
The first set of path models analyzed the prediction of internalizing behavior, externalizing behavior, and other symptomatology at age 23 from adolescent relationship stress and parental support at ages 13 and 17. Correlations for all variables in the first set of models are provided in Table 2. The path model for maternal support is depicted in Figure 1.
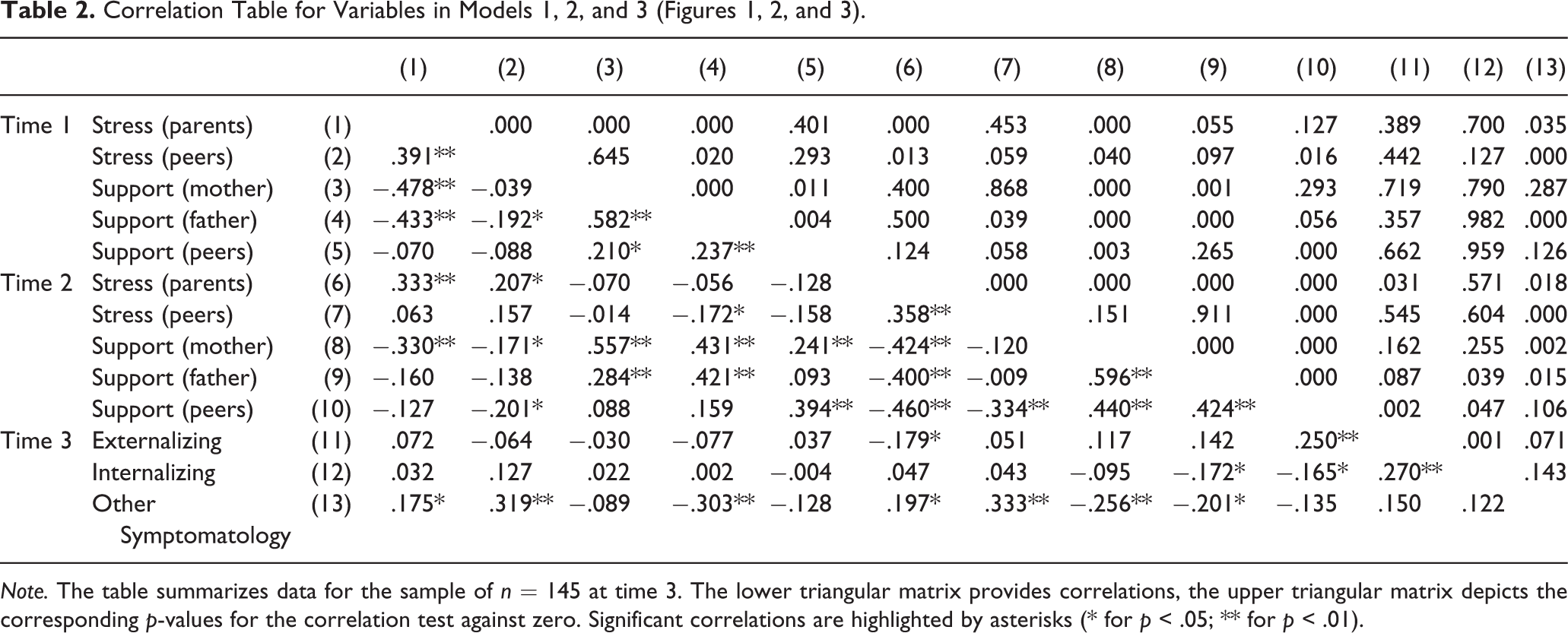
Note. The table summarizes data for the sample of n = 145 at time 3. The lower triangular matrix provides correlations, the upper triangular matrix depicts the corresponding p-values for the correlation test against zero. Significant correlations are highlighted by asterisks (* for p < .05; ** for p < .01).
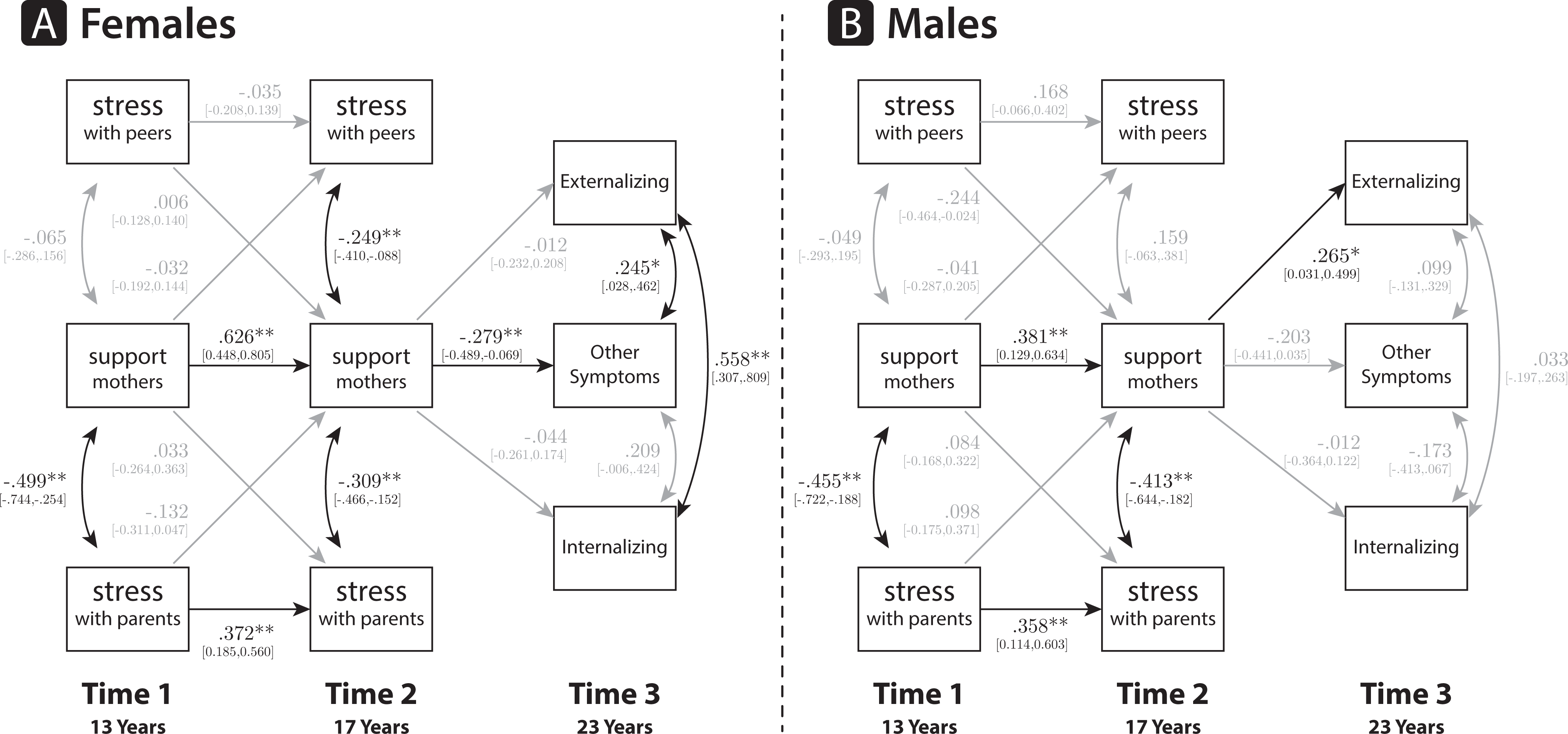
Path Model for Maternal Support (n = 145). Note: Significant paths are shown in black and highlighted by asterisks (* for p < .05; ** for p < .01).
For females, a strong relationship of maternal support at age 13 and at age 17 emerged, which correlated negatively with parent stress at each time point and peer stress at age 17. More social support by mothers was associated with lower perceived stress with parents and peers. Maternal support at age 17 predicted other symptomatology at age 23. Stronger maternal support during adolescence was related to lower symptomatology at later ages. Externalizing behavior at age 23 correlated with other symptomatology such as somatic complaints and internalizing behavior at the same time point.
The path structure for males was less revealing. First, there was no significant relationship between peer stress and maternal support. Second, high maternal support was positively associated with later externalizing behavior. Model fit was good (RMSEA = 0.080, CFI = 0.947, and SRMR = 0.068), and no Wald tests for parameters were significant.
Predicting symptomatology from earlier paternal support
The path model for support by fathers, displayed in Figure 2, shows a similar pattern of path relations as in the maternal model. Fathers’ support over time was consistently related to stress with parents in both the female and male groups. The concurrent relations between the level of paternal support and perceived stress with peers and parents were stronger for females than for males. An association between peer stress and father support at age 13 was only found in the female group. The predictive and concurrent relations at age 23 are identical to the model for maternal support.
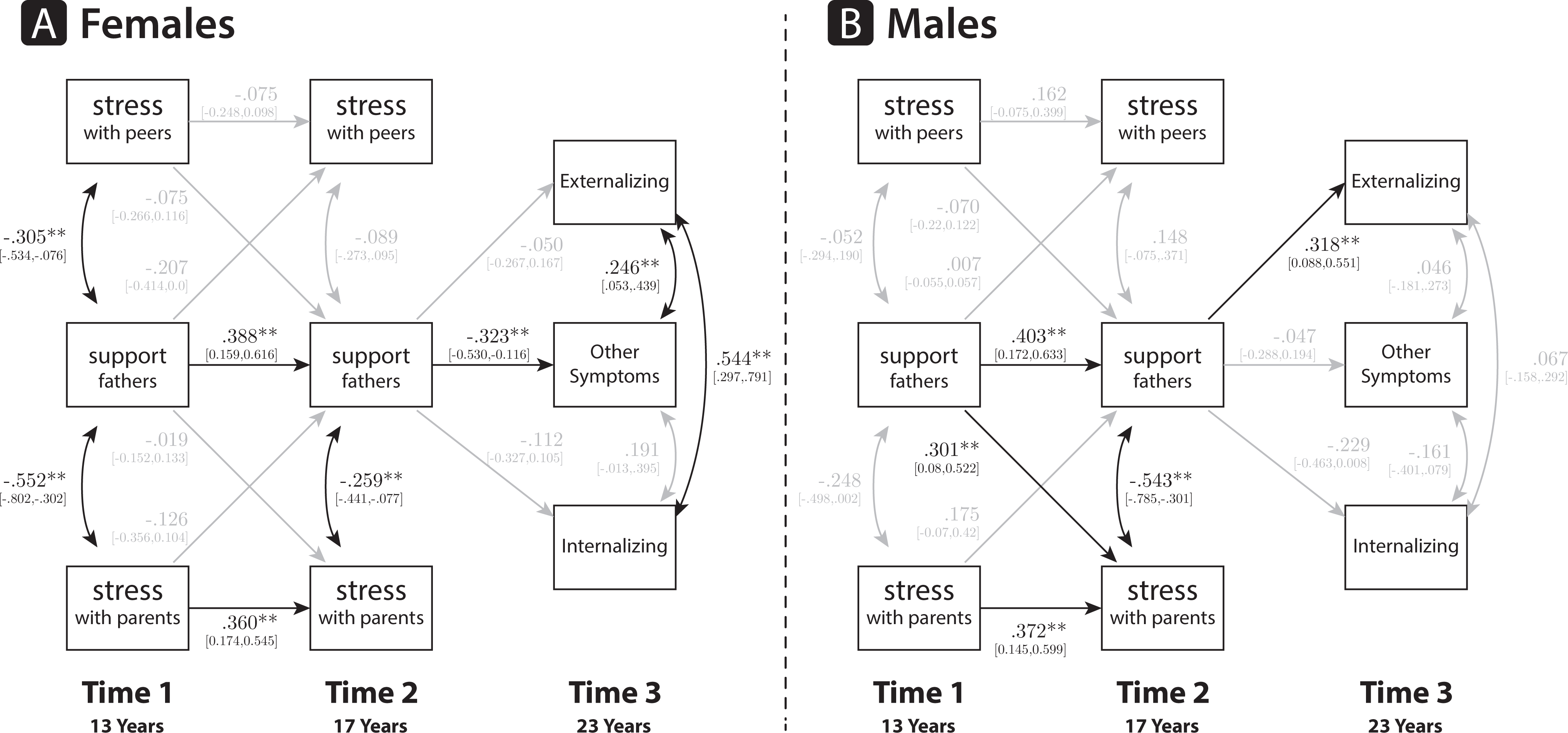
Path Model for Paternal Support (n = 145). Note: Significant paths are shown in black and highlighted by asterisks (* for p < .05; ** for p < .01).
For females, other symptoms such as somatic complaints, attention problems, or thought problems at age 23 were significantly related to support by fathers at age 17, and the relation was stronger than for males (χ2 Δ = 5.028, df = 1, p = .024). Moreover, externalizing behavior correlated with other symptomatology and internalizing behavior at age 23. For males, however, externalizing behavior at age 23 was predicted by fatherly support at age 17, and the relation was larger than for females (χ2 Δ = 4.566, df = 1, p = .032). No significant concurrent relations between outcome variables were present for males at age 23. Model fit was sufficient (RMSEA = 0.093, CFI = .922, and SRMR = 0.077).
Predicting symptomatology from earlier peer support
The path model for social support by peers is depicted in Figure 3. The structure of significant paths is practically identical to the model including maternal support. We obtained a strong positive correlation over time for peer support between ages 13 and 17, and significant correlations between stress level and peer support at each time point. Social support at age 17 predicted other symptomatology (somatic complaints, thought problems, attention problems) at ages 23 for females and externalizing behavior for males. The relation between symptomatology at age 23 and peer support was larger for females than for males (χ2 Δ = 5.458, df = 1, p = .019). Externalizing behavior correlated with internalizing behavior and other symptomatology at age 23 only for females. Model fit was good (RMSEA = 0.060, CFI = .963, and SRMR = 0.076).
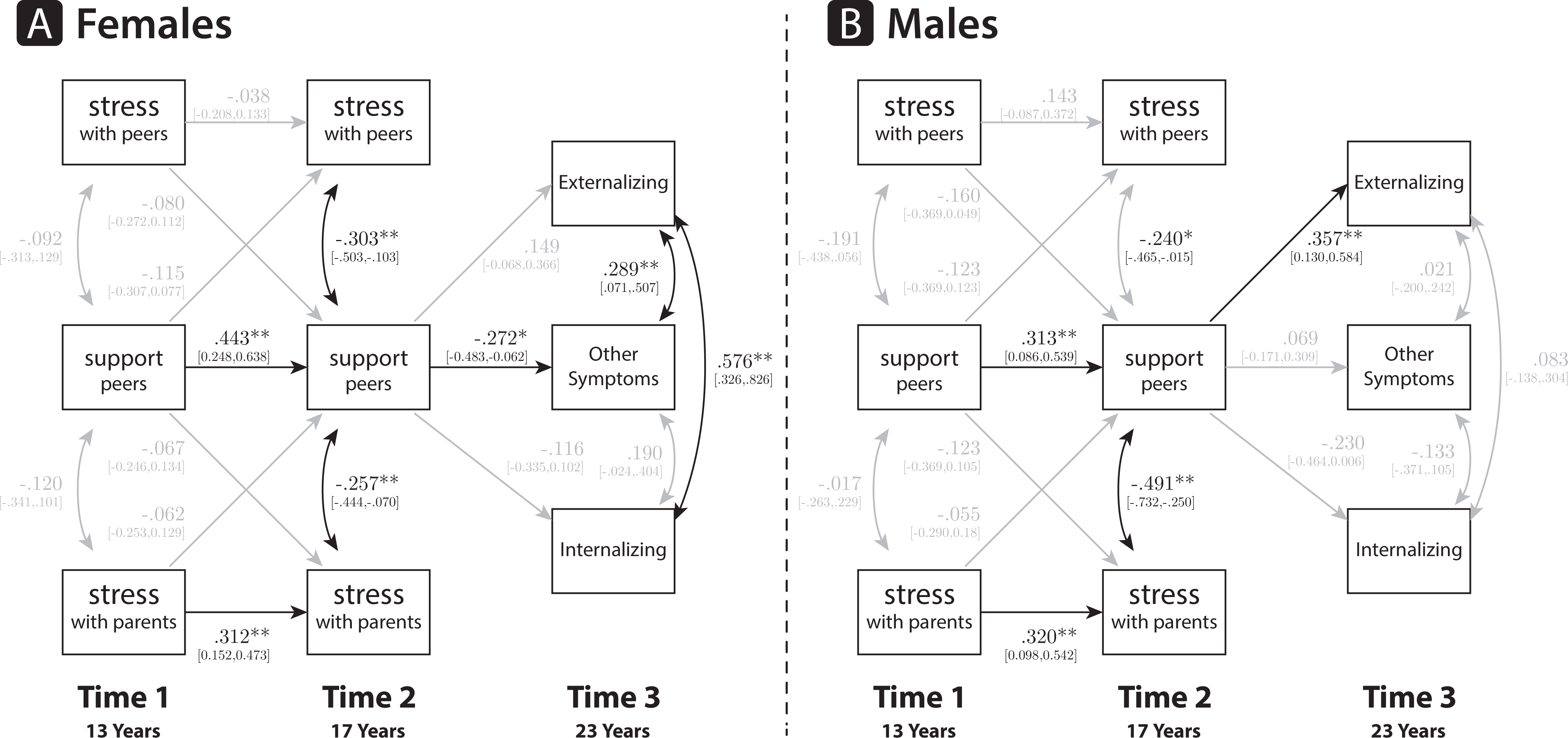
Path Model for Social Support by Peers (n = 145). Note: Significant paths are shown in black and highlighted by asterisks (* for p < .05; ** for p < .01).
Predicting symptomatology from earlier withdrawal coping
The second set of path models related externalizing behavior, internalizing behavior, and other symptomatology at age 23 to different coping styles employed at ages 13 and 17. Correlations for all variables in the second set of models are provided in Table 3. We found identical cross-sectional correlations between stress and withdrawal behavior at ages 13 and 17 (Figure 4). Larger levels of stress with either peers or parents were associated with increased withdrawal in the respective domain. Predictive relations between ages 13 and 17 were different for females than for males.
Correlation Table for Variables in Model 4 (Figure 4).
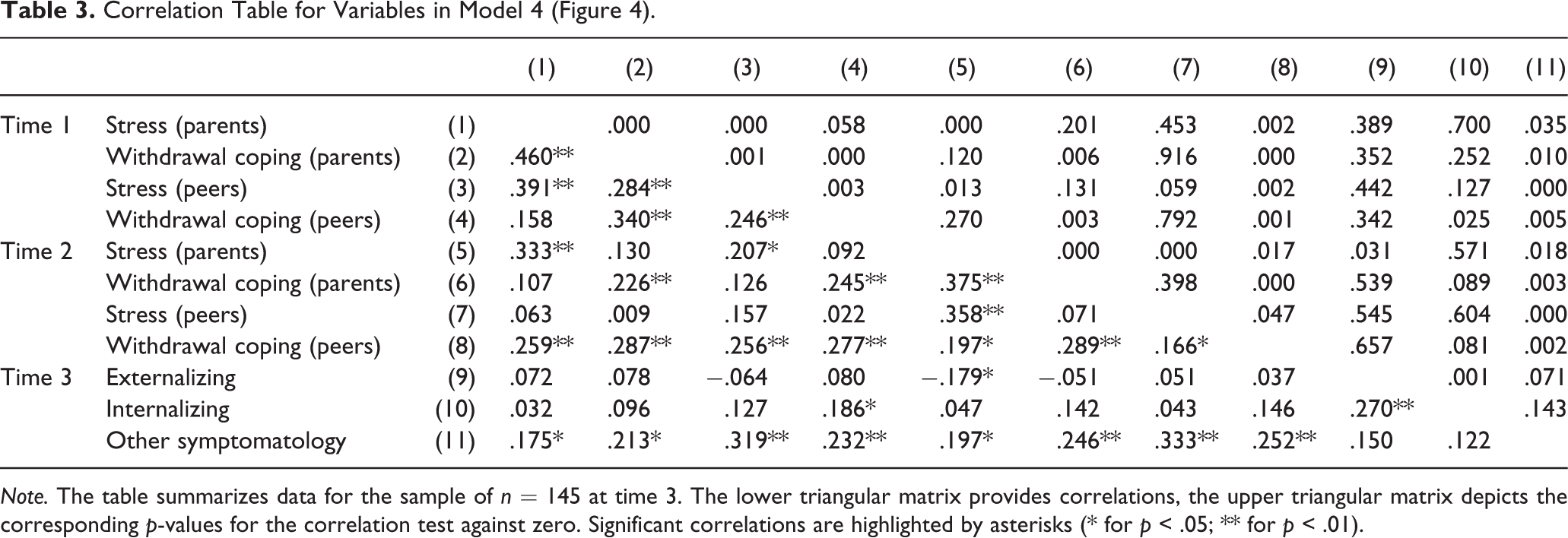
Note. The table summarizes data for the sample of n = 145 at time 3. The lower triangular matrix provides correlations, the upper triangular matrix depicts the corresponding p-values for the correlation test against zero. Significant correlations are highlighted by asterisks (* for p < .05; ** for p < .01).
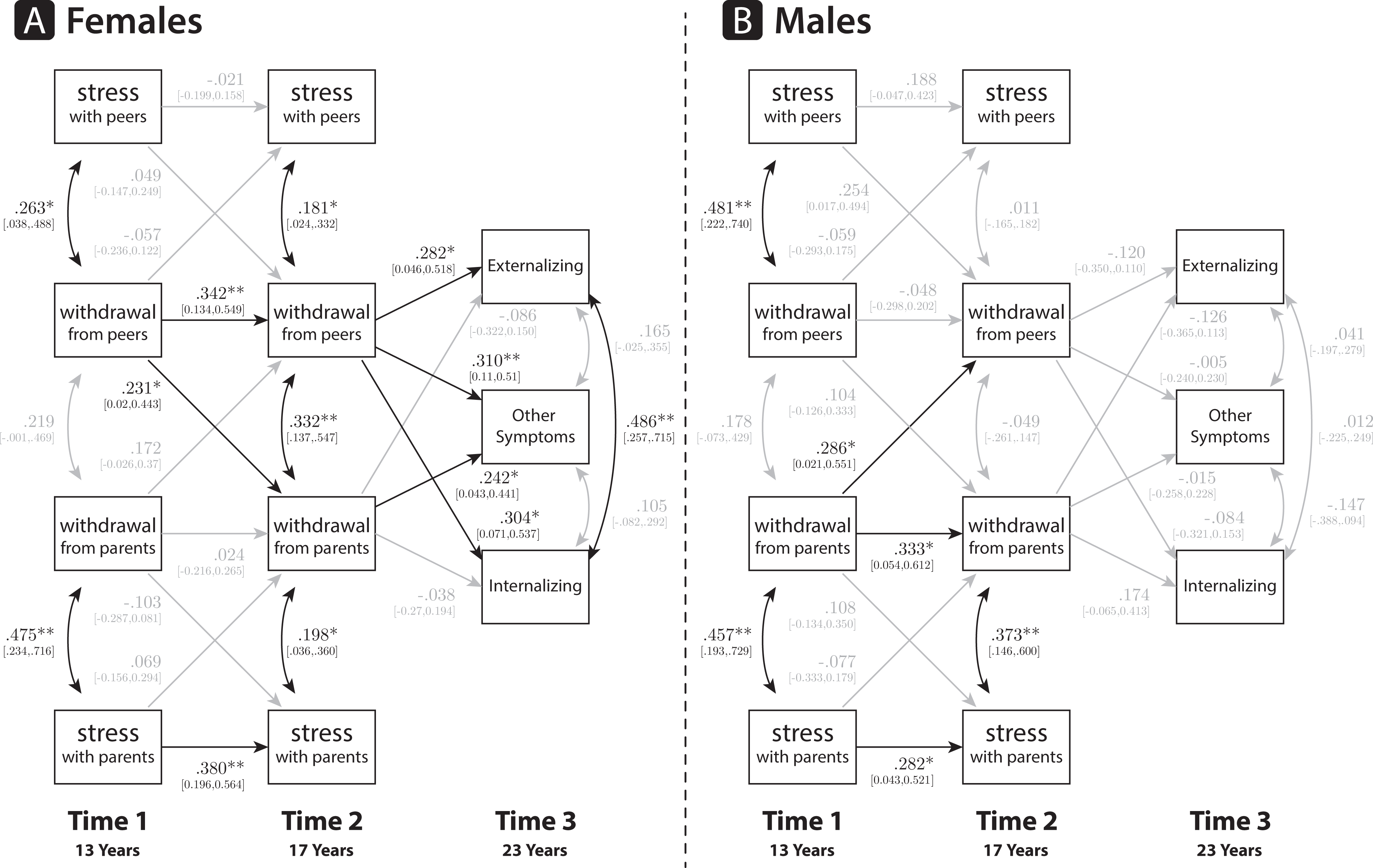
Path Model for Withdrawal Coping (n = 145). Note: Significant paths are shown in black and highlighted by asterisks (* for p < .05; ** for p < .01).
For females, our results revealed a significant association between ages 13 and 17 for withdrawal from peers, which was stronger for females than for males (χ2 Δ = 4.419, df = 1, p = .035). In addition, withdrawal from peers at age 13 predicted withdrawal from parents at age 17 for females. For males, the inverse pattern emerged. Withdrawal from parents at age 13 predicted withdrawal from peers at age 17. For both females and males, parental stress at age 13 predicted parental stress at age 17.
The predictive relations for age 23 also differed between females and males. For females, the earlier tendency to withdraw from peers was positively related to high externalizing and internalizing behavior and other symptomatology at age 23. Relations were stronger than for males on all three outcome variables, externalizing (χ2 Δ = 5.914, df = 1, p = .015), internalizing (χ2 Δ = 6.038, df = 1, p = .014), and other symptomatology (χ2 Δ = 5.516, df = 1, p = .018). Withdrawal in boys, however, exhibited no predictive power for the variables considered at age 23. Model fit was good (RMSEA = 0.052, CFI = 0.961, and SRMR = 0.073). No corresponding models with acceptable model fit could be determined for active or internal coping behavior.
Discussion
Our prospective study advances the work of previous researchers in the domain of stress, coping, and social support, and addresses whether they have a long-reaching effect on individuals’ adaptive outcome in emerging adulthood. The findings shed light on the mechanisms by which peers’ and parents’ support during adolescence contribute to less symptomatology in females when they become emerging adults., They also suggest that supportive relationships with significant others seems to be less beneficial for males’ later adaptation. In addition, the results highlight the central role of females’ earlier withdrawal coping for a non-adaptive outcome in a wider range of symptoms in emerging adulthood.
Managing Relationship Stress during Adolescence and Psychopathology in Emerging Adulthood
Before discussing the main finding regarding the developmental precursors of psychopathology in emerging adulthood, we need to emphasize that our sample resembles other German populations of the same age (Statistisches Bundesamt, 2014; Seiffge-Krenke, 2015). Most of the young people at age 23 in our sample were in transition and had not yet reached adult work status. In this respect they recall the floundering and exploring young adults in the educational and professional domain described by Krahn, Howard, and Galambos (2015). Furthermore, the participants’ living situations were quite diverse (Seiffge-Krenke, 2006). In accordance with North American (Schulenberg & Zarett, 2006) and German nationwide studies (Lambert et al., 2013), the scores for internalizing symptoms were substantially larger in females than in males but did not reach the clinical range.
Gender differences in stress perception and coping style during the adolescent years of our sample were similar to the findings of earlier studies (Tamres et al., 2002; Wasburn-Ormachea et al, 2004). In general, compared to males, females preferred to use active coping strategies (e.g. addressing the problem directly with the person concerned and seeking support from friends (Bowker et al., 2000; Gelhaar et al., 2007; Rudolph, 2002). Of note, early adolescent females in our study reported larger stress levels with peers than males and were quite active in trying to come to terms with it, as is evident in their high values in active coping and internal reflection when managing peer-related stress. A high rate of active, approach-oriented coping is also noticeable in early adolescent females coping with parent-related stress, but they showed a more ambivalent coping pattern. Females apparently try to regulate stress with parents not only by negotiating with parents but also by withdrawing, which reflects the authority gradient that characterizes most parent-adolescent relationships around the globe (Griffiths, Dubow, & Ippolito, 2000; Persike & Seiffge-Krenke, 2015). Given that such differences tend to abate in late adolescence (age 17), these findings might be related to females’ more affiliative and social nature, resulting in a greater sensitivity to relationships stress, particularly in friendships during the formative years of early adolescence (Washburn-Ormachea et al., 2004), or they could be a reflection of parental control, which is typically greater for daughters than sons and decreases during the course of adolescence (Steinberg, 2001).
Managing Relationship Stress during Adolescence as a Precursor to Psychopathology in Emerging Adulthood: A Gendered Pathway
Emerging adulthood resembles the adolescent period: relationship changes occur and a young adult’s agency is at stake when coping with the typical relationship stressors of that period. Furthermore, the period is a critical junction for the development of psychopathology (Schulenberg et al, 2004b). Hence, the contributions of adaptational processes in earlier developmental periods warrant investigation. This study explores the unique contributions of individual competence in coping with stress and perceived support from significant others during adolescence and their impact on emerging adults’ adaptive functioning.
Our findings showed a gender-specific impact of parent and peer support during adolescence on the individuals’ later adaptational outcome. Similar to the findings of Barber et al. (2005), more support by mothers was associated with lower stress levels for females in both relationship domains during adolescence, and it effected symptomatology such as somatic complaints at age 23. This result suggests that positive, supportive relationships with mothers during adolescence are important in times of stress and even have a positive impact on their daughters’ health years later. This finding provides important information for families. Despite numerous conflicts in the mother-daughter relationships (Scharf & Mayseless, 2008; Seiffge-Krenke et al, 2008) and the distancing process that occurs during adolescence (Papini, Roggman, & Andersen, 1991), the long-reaching effect of a mother’s support over six years is remarkable. The effect may be related to a more frequent and open communication between mothers and daughters (Keijsers, 2010; Noller & Callan, 1990), which encourages help-seeking and support-giving behavior. The effect is also reminiscent of maternal sensitivity (Cabrera, Fagan, Wight, & Schadler, 2011), which was found to have an impact on different outcomes for children at all ages.
Paternal support, although concurrently not as consistently associated with relationship stress as maternal support, had the same long-term impact on symptoms (e.g. somatic complaints) when the daughter was an emerging adult. Of note, and in contrast to our expectations, parental support was not related to less internalizing symptoms. We offer three speculations for this unexpected finding. First, somatic complaints, attention problems, and thought problems may be a more direct indication of stress, because they entail a direct physiological reaction to stress, compared to depression or anxiety (internalizing), or aggressive behavior (externalizing), and they signal that the individual is attempting to come to terms with the stressor. Second, according to Achenbach, Howell, McConaughty, and Stanger (1995), the transition from adolescent symptoms to young adult symptoms, as evidenced by research using the YSR and the YASR, suggests a transition from more overt symptoms (e.g. antisocial behavior) to covert symptoms such as somatic complaints. Third, culture may play a role. Depression, for example, is not exhibited in the same way across cultures (Auerbach, Abela, Zhu, & Yao, 2010). In sum, our findings seem to suggest that a stable emotional connection with both parents lays a solid foundation for girls’ adaptation to later challenges. Mothers’ and fathers’ sensitivity and support during adolescence are necessary for the daughters’ adaptive psychosocial functioning at emerging adulthood (Gilligan, 1982). Significant correlations between the different scores of internalizing, externalizing, and other symptoms such as somatic complaints, attention problems and thought problems emerged as correlates. The findings indicate the existence of comorbidity among symptoms.
Although both parents remained quite influential on emerging females’ adjustment, the pattern was apparently different for sons. Remarkably, we could not substantiate a buffering effect of mothers or fathers. Although parental support during adolescence was associated with a concurrent decrease in stress in the parental domain (with a stronger and more consistent effect of mothers’ support), this beneficial effect had no long-term impact. More importantly, support provided by mothers and fathers resulted in higher rates of externalizing behavior, for example, higher rates of aggressive, antisocial behavior in boys when they became emerging adults.
Different speculations may help to explain these findings. Autonomy could possibly be more of a priority for sons compared to daughters (Wray-Lake, Crouter, & McHale, 2010). We deduce this explanation from their hesitation to disclose information to parents, particularly mothers (Noller & Callan, 1990) and their tendency to keep more secrets (Keijsers, 2010). Parental support depends on a child’s disclosure, and under such conditions parents may feel ill at ease, or they may provide inadequate or too much support. Parental support, which can be intrusive, may result in greater stress levels in a child (Barber et al., 2005). The impact of support provided by parents during adolescence on emerging adult males’ externalizing symptoms seems to suggest that they are more sensitive to or feel perhaps spoiled by too much maternal and paternal support. This type of parenting behavior is explained in other studies as nonadaptive, leading to higher rates of delinquency in children (Bailey, Hill, Oesterle, & Hawkins, 2009). In a similar vein, the findings of Caron, Weiss, Harris, and Catron (2006) indicate that parental warmth and involvement, but not monitoring and discipline, were uniquely related to the externalizing behavior of sons. Alternatively, involvement in a peer groups’ delinquent behavior is a frequent motive to escape from overly intrusive, overly supportive parents (Dishion & McMahon, 1998).
Overall, the long-term links between supportive parental behaviors and children’s symptomatology were very different for daughters and sons, resulting in a beneficial role for daughters, but parents’ support for sons was consistently linked with a less adaptational outcome when they became emerging adults. This finding is in line with a number of studies reporting a prospective effect of parental support for girls but not for boys (Windle, 1992, Stice et al. 2004). The novel aspect of our research is that peer support exhibited a similar beneficial prospective effect, highlighting the importance of friendship relationships for girls’ health (Hey, 1997). Although consistent negative associations were found between support provided by parents and peers and stress in close relationships during adolescence for males, support provided by parents and peers predicted consistently stronger externalizing symptomatology in males when they became emerging adults. This underscores the point that autonomy is more prominent for males and that caregivers should be very sensitive to the importance of providing “the right kind of support” that obviates their sons’ feelings of neediness and dependence.
Remarkably, the impact of fathers and mothers was non-specific. Russell and Saebel (1997) substantiated that the roles of fathers and mothers are different and that fathers fulfill a different yet distinctive role in the life of their children. Adolescents may distance themselves from their mothers, but the decline in intimacy is likely to be less than it is for fathers (Steinberg, 2001). We found that perceived support by fathers is lower than support by mothers but equally low for males and females. Thus, we could not argue that fathers are particularly uninvolved with sons and consequently fail to serve as a buffer to poor adaptational outcomes later in life (Dishion, Nelson, & Bullock, 2004).
Parenting remained a gendered activity but one that may be changing, as is clear from research portraying modern fathers as “second mothers” who are more involved and supportive compared to fathers two decades ago (Soenens, Vansteenkiste, & Goossens, 2006). Our findings speak against a unique influence of mothers and fathers. Both seem to parent well for daughters, but these same parenting behaviors have a detrimental effect on sons.
In contrast to earlier studies (Stice et al. 2004), our study revealed a lack of differential direction of effects for parent and peer support for females. Both support providers had similarly beneficial long-term effects, which is a substantial finding. Moreover, perceived support by peers had very contradictory effects on males and females. Females’ supportive peer relationships reduced stress in close relationships and contributed to subsequent better adaptation. As detailed, males’ peer support reduced stress with parents but later contributed to high levels in externalizing behavior when they became emerging adults. Although friendship support may have negative effects on females adaptation, as substantiated in the co-rumination research (Rose, 2002; Sontag, Graber, Brooks-Gun, & Warren, 2008), “having the wrong friends” seems to be more detrimental for males (Dishion & McMahon, 1998; Lundborg, 2006).
Gendered pathways were likewise noticeable with respect to the impact of coping with relationship stress on later pathways to symptomatology. Withdrawal coping was linked with increased stress levels with parents and peers for males when they were 13 and 17 years. However, this constellation had no effect on later adaptation when they were emerging adults. In contrast, a strong, direct, long-term impact of withdrawal coping emerged for females. Withdrawal coping during adolescence when dealing with family and peer stress not only resulted in increases in internalizing and externalizing symptomatology but also in increases in subsequent further symptomatology (including thought problems, attention problems, and somatic complaints) at age 23. Seiffge-Krenke (2011) showed that withdrawal coping can be adaptive in the short- run, but the long-term application of withdrawal in stressful encounters may be detrimental for health. In her meta-analysis on the links between coping with interpersonal stress and psychosocial health, Clarke (2006) suggested that the use of active coping reduces externalizing symptoms, whereas the use of withdrawal coping results in stronger internalizing symptomatology. Our findings indicate gendered pathways and illustrate a strong and pervasive effect of a dysfunctional coping style on a wide range of later psychopathology for females, which is consistent with the results reported by Sontag et al. (2008). We need more studies to analyze why these associations do not hold for males.
Implications for Further Research
The interface between individual competence in coping with stress and perceived support from significant others during adolescence and its impact on emerging adults adaptive functioning is poorly understood. This research found compelling evidence of a gendered pathway to emerging adults’ adaptation, with support patterns provided by parents and peers that serve very different functions for males’ and females’ subsequent psychological health. Only for females, support by parents and peers serve similar protective functions for later health. Moreover, our research highlighted that withdrawal coping in the context of changing and stressful relationships have enormous direct long-term effects for females’ psychological health but not for males’. More studies are needed to clarify why males are quite robust in their defense against the long-term effects of withdrawal coping and react so differently to the support provided by parents and peers. Future studies would profit from using a more detailed scale to measure coping; the dichotomous nature of the CASQ is a limitation. Further studies should also include larger and more ethnically diverse samples when assessing how stressful encounters are perceived and managed (Persike & Seiffge-Krenke, 2014; Seiffge-Krenke & Persike, 2015). Moreover, parenting differs across culture (Brown & Mounts, 2007), and this may have different ramifications on psychopathology (Rescorla et al., 2007). Such studies may help to identify mechanisms that link relationship stressors to adjustment outcomes, depending on cultural background. Replicating our results using a larger sample is also necessary: our sample was too small to analyze in one model the moderating effects of support and coping variables on the path between stress and later symptomatology. An additional important point is that measures of fathering and mothering are often moderately to highly correlated. Thus, the unique portion of explanatory power is generally much smaller than the predictive ability shared with the other parent (Stolz et al., 2006). In particular, we need to focus more than we have in the past on male pathways, because they seem to be more of “a dark continent” than females (to reframe a 1920 quote by Freud).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant of Deutsche Forschungsgemeinschaft DFG, SE 408-14, given to the first author.