
Abstract
The current study demonstrates the application of an analytic approach for incorporating multiple time trends in order to examine the impact of cohort effects on individual trajectories of eight drugs of abuse. Parallel analysis of two independent, longitudinal studies of high-risk youth that span ages 10 to 40 across 23 birth cohorts between 1968 and 1991 was conducted. The two studies include the Michigan Longitudinal Study (current analytic sample of n = 579 over 12 cohorts between 1980 and 1991 and across ages 10–27) and the Adolescent/Adult and Family Development Project (current analytic sample of n = 849 over 11 cohorts between 1968 and 1978 and across ages 10–40). A series of nonlinear, multi-level growth models controlled simultaneously for cohort and age trends in substance use trajectories. Evidence was found for both age and cohort effects across most outcomes as well as several significant age-by-cohort interactions. Findings suggest cohort trends in developmental trajectories of substance use are sample and drug-specific in the adolescent and early to mid-adult years. Thus, studies that do not control for both trends may confound cohort and developmental trends in substance use. For this reason, demonstration of one analytic approach that can be used to examine both time trends simultaneously is informative for future multi-cohort longitudinal studies where change over time is of interest.
Studies of adolescent substance use have increasingly adopted longitudinal designs to identify developmental patterns of alcohol and drug use. Spanning nearly five decades, this work has shifted the focus of study from understanding rates of substance use at any given point in time to understanding individual differences in trajectories of substance use over time (Chassin, Colder, Hussong, & Sher, 2016; Schulenberg, Maslowsky, Patrick, & Martz, in press; Zucker, Hicks, & Heitzeg, 2016). The study of individual trajectories of substance use within longitudinal studies allows us to make inferences about within-person processes (e.g., what predicts the level and rate of change in substance use within a set of individuals) without confounding selection biases and age differences (as occurs in between-person comparisons using panel designs that compare different people at each age to infer individual patterns of development).
Studies have characterized substance use trajectories with samples that span different age and birth cohorts. Because substance use trajectories may be sensitive to both of these dimensions of time, comparing findings from these studies requires an understanding of how cohort effects impact individual trajectories of substance use (O’Malley, 1994). Few studies have controlled for cohort trends in age-based trajectories (i.e., interaction of cohort and age-based trends) and none have done so while mapping developmental trajectories that span decades (i.e., early adolescence to middle adulthood). The current study demonstrates the application of one analytic approach (i.e., nonlinear multilevel growth models) that allows for the examination of cohort effects in developmental trajectories that span ages 10 to 40 years.
Analyzing developmental trajectories and cohort trends
Two primary approaches to capturing individual differences in trajectories of substance use are widely in use. These include growth mixture modeling (Li, Duncan, & Duncan, 2001; Muthén, 2001; Muthén & Shedden, 1999; Nagin & Tremblay, 2001), and the related techniques of multi-level (Raudenbush & Bryk, 2002; Singer & Willett, 2003) and latent growth modeling (Bollen & Curran, 2006; Duncan, Duncan, & Strycker, 2006; McArdle, 1988; Meredith & Tisak, 1990). Growth mixture modeling defines discrete groups that are posited to reflect meaningfully different developmental trajectories of substance use by parameterizing latent classes that differ in within-person fixed and random effects. Multilevel and latent growth modeling, on the other hand, examine individual differences in developmental trajectories. Although multilevel modeling and latent growth modeling are similar in many respects, multilevel models are traditionally touted for their strength in addressing nested or non-independent data whereas latent growth models are touted for their strength in addressing complex measurement structures estimated via latent variables (Bauer, 2003; Curran, 2003; Raudenbush, 2001). While all three approaches offer somewhat different perspectives on trajectories of substance use (i.e., group vs. individual differences in intra-individual change) and different parameterization within models (i.e., latent variables vs. observed variables), they share a focus on defining change over time in substance use trajectories based on maturation or age of the respondent within longitudinal designs.
Just as longitudinal studies show change at the individual level in substance use patterns over time, panel studies show change at the cohort level. Such cohort effects represent a well-known challenge and potential confound to studies of developmental trajectories. For example, although individual differences in rates of change of substance use over time are typically interpreted as developmental differences in substance use, these differences could at least partially reflect trends in drug popularity and availability (Johnson & Hoffman, 2000; Pampel & Aguilar, 2008).
This confound could be understood in the context of the classic literature on what Schaie (1965) defined as the “multiple clocks” problem. Schaie (1965) defined the influences of age (i.e., the individual effect of maturation), cohort (i.e., the population effect of being born and developing at a given point in historical time), and period (i.e., the total impact of a given environment on individual behavior at a given point in time) as three clocks or timelines that simultaneously shape behavior over time. Although Schaie concluded that these effects were intractably confounded, subsequent advances in statistical modeling yielded various solutions to the co-analysis of these effects (i.e., Mason, Mason, Winsborough, & Poole, 1973; O’Brien, Hudson, & Stockard, 2008; Winship & Harding, 2008; Yang & Land, 2008). Each solution makes different assumptions about what effects are of greatest interest within a given research study (e.g., which “clock” is the primary interest substantively), and whether a given “clock” is a fixed or random effect. In addition, study design is also an important consideration when selecting the time trends that will be examined. For example, time-sequential designs, in which individuals of a particular age are assessed at multiple points in historical time, lend themselves to an examination of age and period effects. Cohort sequential designs, in which several cohorts are followed longitudinally across development, can be used to tease apart age and cohort effects. Thus, methodologists have encouraged researchers to select their approach to the age-period-cohort confound based upon substantive theory and study design.
In the current article, we focus on a specific question within the age-period-cohort nexus, shifting from the study of levels of substance use to the study of trajectories of substance use over time. We evaluate whether substance use trajectories over the early- to mid-life course vary substantially across different birth cohorts. Given the potential for developmental trajectories to serve as informative phenotypes for work in behavioral genetics (e.g., Dick et al., 2009), as an indicator for identifying intervention effectiveness (e.g., Spaeth, Weichold, Silbereisen & Wiesner, 2010), and as distinguishing etiological mechanisms (e.g., Moffitt, 1993), understanding the extent to which developmental trajectories are stable over cohort is of keen interest to a broad audience of addiction researchers. Thus, the current study demonstrates an analytic approach that allows for the simultaneous estimation of cohort effects and age-based trajectories of substance use within a multi-level modeling framework. Our approach was selected based upon the utilization of two cohort-sequential studies, the study’s substantive interest in random age effects and fixed cohort effects, and the inclusion of nested data.
Age and cohort effects of substance use outcomes
Previous studies of age-based trajectories that span adolescence and adulthood tend to find average patterns of substance use that are quadratic in form (e.g., Brennan, Schutte, Moos, & Moos, 2011; Chen & Jacobson, 2012), with significant individual variability in both starting points and rates of change in drug use over time (Chassin et al., 2016). Just as longitudinal studies show significant change at the individual level in substance use patterns over time, panel studies show significant change at the cohort level in substance use patterns over recent decades (Johnston, O’Malley, Bachman, & Schulenberg, 2013). Annual prevalence rates for illicit drug use in the United States generally showed a notable decline from the mid-1980s into the early-1990s, a pattern that appears fairly uniform across age groups (i.e., late adolescence to mid-adulthood; Johnston et al., 2013). However, beginning in the mid-1990s, patterns in illicit drug use began to diverge across age groups and types of drugs. Although US rates have generally held steady or shown modest fluctuations after reaching peak rates for each age group, some drugs showed greater decreases (i.e., inhalants showed notable decreases after 1996 particularly among younger respondents) and others showed greater increases (i.e., sedatives showed staggered increases after 2004 across groups of older respondents). These findings clearly indicate that rates of drug use in the United States diverge across cohort (Jager, Schulenberg, O’Malley, & Bachman, 2013) and vary to some extent by substance.
Providing a strong test of this hypothesis, Jager et al. (2013) examined the impact of cohort effects on developmental trajectories of heavy drinking and marijuana use with a latent growth modeling approach. As expected, systematic changes in trajectory slopes as a function of birth cohort were found, with steeper, increasing slopes across the age 18–22-period for later-born cohorts. The current study extends this work by demonstrating an alternative analytic methodology for examining cohort effects in developmental trajectories, and examines longer developmental periods, different forms of substance use, and the potential for non-linear trends in use over time. Our use of studies which oversampled at-risk youth (i.e., children of alcoholic parents; COAs) allowed for an examination of specific drugs of abuse (e.g., hallucinogens, opiates) due to increased base rates compared to community samples in the United States. Given the sampling design, we do not aim to generalize base rates of various trajectories of substance use but rather to demonstrate an analytic approach that allows for the simultaneous estimation of cohort effects and age-based trajectories of substance use from late childhood to mid-adulthood in order.
Based on prior studies conducted with United States populations, we anticipate that across alcohol, tobacco, marijuana, hallucinogens, opiates, stimulants, and depressants, age trajectories will show increases from adolescence to the early 20s (for alcohol) to mid-20s (for other forms of drug use), with decreases that stabilize after that time into the 30s; inhalants will show a unique pattern with decreasing use across adolescence and into adulthood. We also expect to find cohort trends that vary over drug class and may interact with age in predicting patterns of drug use over time.
Methods
Sample and procedures
The Michigan Longitudinal Study (MLS) used a rolling, community-based recruitment to sample boys aged 3–5 as well as similarly-aged siblings recruited at subsequent waves of data collection (Zucker et al., 2000). As part of a larger data collection effort, all children assessed in this study completed brief annual interviews administered in-home between the ages of 11 and 17 as well as multi-session assessments every 3 years from ages 3 to 30. The current analysis sample was drawn from the seven annual interviews and waves 4–9 of the multiple session assessments. Cohort was defined as birth year, and cohorts with less than 15 participants were dropped (9 birth years or n = 55 participants) to avoid sparseness. The final sample of 579 participants (ages 10–27, 76% COA, 73% male, 98% Caucasian; see Tables 1 and 2) represents 12 cohorts born between 1980 and 1991. Rates of parent alcoholism are higher in the current sample (a subset of the full MLS sample) than in the larger sample. In this subsample, 85% contributed 3 or more data points and participation was unbiased by COA at all included waves.
Demographic characteristics of the analysis samples from Michigan Longitudinal Study and Adolescent and Family Development Project.

Note. aParticipants in the Michigan Longitudinal Study were from a rolling, community-based recruitment sample that initially enrolled target children and afterward their similarly-aged siblings at a later time. This accounts for the similar age ranges across the studied birth years. bRemaining participants self-identified as Hispanic.
Sample size by age and cohort.
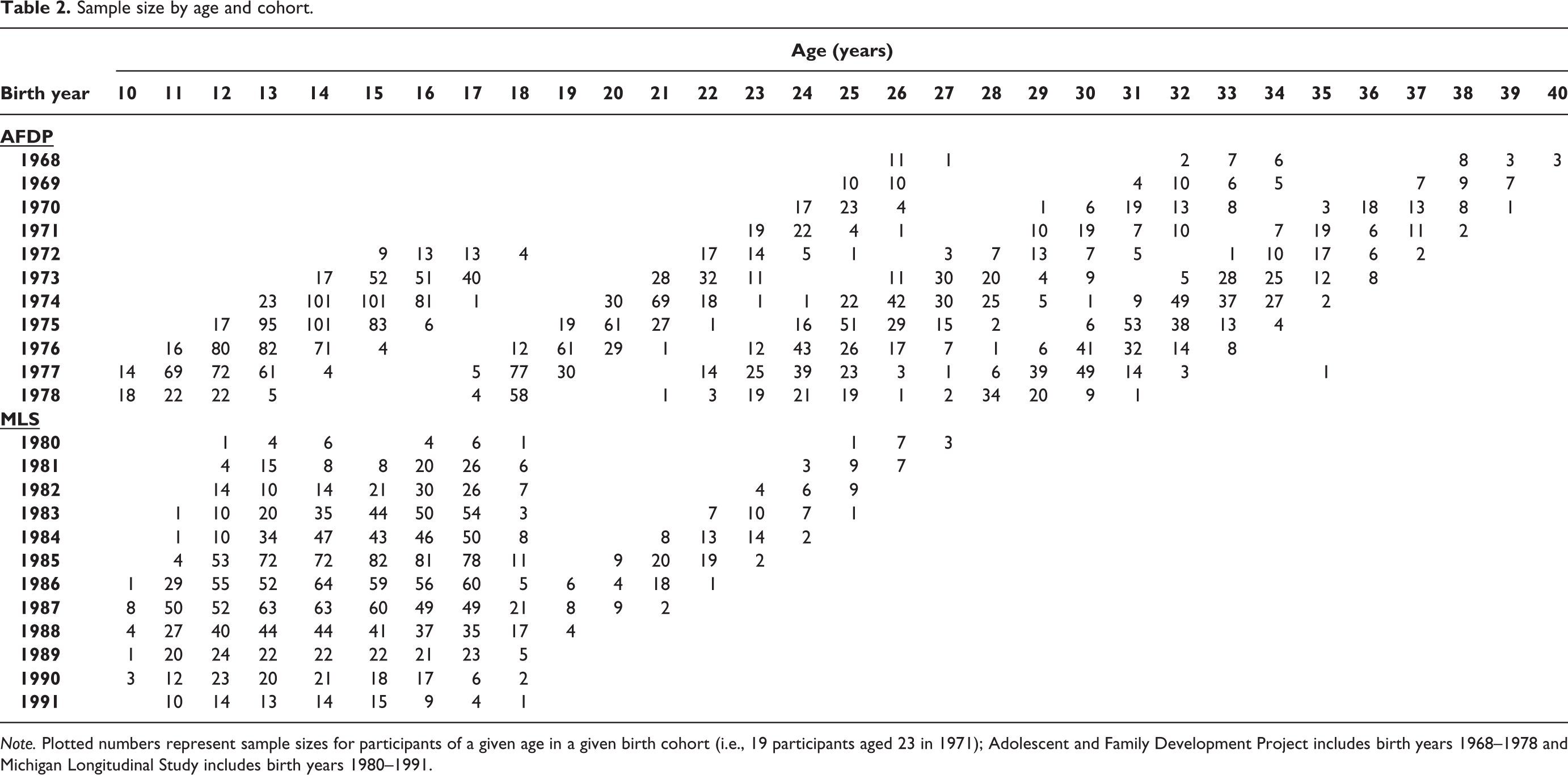
Note. Plotted numbers represent sample sizes for participants of a given age in a given birth cohort (i.e., 19 participants aged 23 in 1971); Adolescent and Family Development Project includes birth years 1968–1978 and Michigan Longitudinal Study includes birth years 1980–1991.
In the Adolescent and Family Development Project (AFDP; Chassin, Flora, & King, 2004), 454 families (50% COA) completed three annual interviews, conducted within the participant’s home or at the university, beginning when the target child was aged 10–15. In two young adult follow-ups occurring at 5-year intervals (approximately ages 18–23 and ages 23–28), 396 full biological siblings were included who were similarly-aged to the targets. The final sample size of 849 participants from 454 families (ages 10–40, 51% COA; 52% male; 71% Caucasian and 29% Hispanic, see Table 1 and 2) represents 11 cohorts born between 1968 and 1978 (after eliminating 1 sparse birth year or n = 1 participant). Latinos in the sample were highly acculturated for the historical period given that inclusion criteria required English proficiency in both parents and teens. Sample retention has averaged more than 90% at each wave and has been unbiased by gender and ethnicity, although somewhat more COAs than controls were lost at Waves 4 and 5, χ2 (1, N = 454) = 5.45 at Wave 4 and = 4.12 at Wave 5, both p < .05).
Parallel analysis of these two studies allowed for the demonstration of an analytic approach that can be used to investigate developmental trends across a broad range of birth cohorts (Brown et al., 2013). Integrating studies within analyses, such as through an Integrative Data Analysis (IDA) approach, was not possible due to the lack of overlap in cohort (i.e., birth years) across MLS and AFDP. General guidance suggests that IDA should only be used when studies clearly overlap in key predictor variables (e.g., age, cohort) and outcome variables (e.g., substance use). Using IDA with a lack of clear overlap in cohort would result in the confounding of study-specific characteristics (e.g., demographic region, ethnicity of participants) with cohort effects (see Hussong, Curran, & Bauer, 2013).
Measures
Participants reported gender (males = 1), ethnicity (Hispanic = 1), and age. Parents reported their educational attainment which was coded using a 6-point scale ranging from “0” less than 12 years/not a high school graduate to “5” completed graduate or professional school.
Parent alcoholism was assessed by parent-report. In the MLS, trained clinicians using DSM-IV criteria made a lifetime Alcohol Use Disorder diagnosis based on baseline parent report on the Diagnostic Interview Schedule (DIS; version III; Robins, Helzer, Ratcliff, & Seyfried, 1982), the Short Michigan Alcohol Screening Test (Selzer, Vinokur, & van Rooijen, 1975), and the Drinking and Drug History Questionnaire (Zucker, Noll, & Fitzgerald, 1988). Inter-rater reliability for the diagnosis was excellent (kappa = 0.81). In AFDP, parents completed a computerized version of the DIS to assess diagnostic status or, when unavailable (21% of fathers and 4% of mothers in the current subsample) spousal report on the Family History Research Diagnostic Criteria (Andreasen, Endicott, Spitzer, & Winokur, 1977) was used.
Substance use was assessed by participants’ self-report of how often they used alcohol, tobacco, or illicit drugs over the past year. For AFDP, participants reported how often they drank beer, wine, wine coolers, or hard liquor as well as marijuana, hallucinogens, opiates, stimulants (i.e., cocaine and amphetamines), depressants (i.e., tranquilizers and sedatives such as barbiturates), and inhalants. During waves 4 and 5, participants also reported on their tobacco use. For the MLS, participants reported how many days a month over the previous six months they typically had a drink of alcohol (i.e., beer, wine, and liquor), and how often they used tobacco, marijuana, hallucinogens (i.e., psychedelic drugs and LSD), opiates (i.e., heroin and narcotics), stimulants (i.e., cocaine and amphetamines), depressants (i.e., tranquilizers, Quaaludes, and sedatives such as barbiturates), and inhalants (i.e., inhalants and nitrates; assessed only during waves 4 and 5). The drug assessment measure was based on the 1978 NIDA/MTF survey (Bachman, Johnston, & O’Malley, 1978). To reduce sparseness in upper-categories, we rescaled alcohol variables to a 3-point range of “0” less than monthly, “1” at least monthly but not weekly, and “2” weekly or more, and tobacco and other illicit drug use items to binary indicators of “1” use versus “0” abstinence in the past year.
Analytic approach
Analyses followed four steps for both studies. First, we used descriptive techniques to examine the endorsement patterns for each substance across age and cohort and to identify the potential functional form of the age and cohort trajectories for each type of substance. Second, we estimated unconditional, non-linear multilevel growth models to test competing functional forms for age-related trajectories for all outcomes including (a) random intercept and fixed linear age, (b) random intercept and fixed linear and quadratic age, and (c) random intercept, random linear age, and fixed quadratic age. Model comparisons were based on AIC and BIC indices, likelihood ratio tests, and examination of fitted versus observed logit plots. Because alcohol use was scaled as a trichotomy, proportional odds cumulative logit models were used. Relative model comparisons suggested that the proportional odds assumption of the cumulative logit model is appropriate. 1 Otherwise, standard binary logit models were used for all other outcomes. Age was centered at the mean for each study (18 in MLS, 25 in AFDP). Third, we added (a) linear and (b) quadratic time trend effects of cohort to the resulting model for each outcome, centered at the mean of each study (1985 in MLS, 1974 in AFDP) as well as the interaction of cohort effects with age in order to define the functional form of the cohort effect. Fourth, we added covariates to the resulting models to isolate unique cohort trends in intraindividual (age) trajectories of substance use after controlling for the effects of parent education, parent alcoholism, gender in MLS and AFDP, as well as ethnicity in AFDP. To test these effects, we used a conservative model building strategy in which covariates were added to each model, followed by interactions of each covariate (i.e., gender, parent alcoholism, parent education, and ethnicity in AFDP) with linear and quadratic age and linear cohort. For example, interaction terms for gender in AFDP included gender by linear age, gender by quadratic age, and gender by cohort. Non-significant terms were trimmed hierarchically and models re-estimated iteratively to ensure stability in estimation.
In both studies, final models for each drug use outcome were extended to include a third level random family intercept to account for nesting within family. Convergence problems occurred for three of these eight outcomes (i.e., opiates, depressants, and inhalants) across both studies indicating no meaningful variability at the third level of nesting. However, models that converged indicated that no substantive differences were present and therefore 2-level models were retained for all drug use outcomes in order to increase stability of estimation.
Results
Examine endorsement patterns to identify potential functional forms
Plots of observed age trajectories (scaled in logits) for each drug by study and cohort suggested that, for both studies, endorsement rates increased with age in a quadratic fashion; however, developmental trajectories shifted by cohort. Inhalant use differed, showing increases from ages 10–16 and then decreases into adulthood.
Test competing functional forms for age-related trajectories
Results of unconditional multilevel models found that a random intercept and linear age trend (indicating significant variability in starting point and rate of change of alcohol use across participants) with a fixed quadratic age effect (increasing alcohol use through adolescence with decreases beginning in the early 20s) best captured changes in alcohol use in both studies.
Best-fitting models for other drugs included a random intercept (indicating significant variability in the starting point of drug use) and fixed linear and quadratic age effects (such that drug use on average increased through adolescence, peaked in young adulthood, and leveled off or declined thereafter). As is common with nonlinear multilevel models, convergence problems were encountered across many binary outcomes, precluding inclusion of a random age component. Non-significant linear and quadratic age effects were found within the inhalant model in MLS and the tobacco model in AFDP; however, for consistency, we retained the same model across substances.
Test competing functional forms for the cohort effect
In models adding cohort effects, main effects of linear cohort were significant across most outcomes. No significant quadratic cohort effect was discovered in any outcome in either study. Thus, the interaction between linear age and linear cohort was examined and found to be significant for alcohol, tobacco, and hallucinogens in MLS and for inhalants in AFDP. These findings suggest that linear cohort effects, linear and quadratic age effects, and the interaction of linear cohort and linear age should be retained in further analyses for all outcomes within both studies in order to obtain conservative model estimates.
Isolate unique cohort trends in intraindividual (age) trajectories
Prior to interpreting these models, we added covariate predictors as well as interactions among covariates and the time trend indicators (linear age, quadratic age, and linear cohort). Non-significant interactions were trimmed iteratively to ensure stability of estimation and for the purpose of model parsimony. Of note, only higher order interaction terms were interpreted (except for our interaction of interest, cohort by age effect) as general guidance suggests that lower order interaction terms should be interpreted within the context of higher order terms effects. Covariate effects for MLS and AFDP models were largely as expected but differed due likely to sample and study differences (see Tables 3 and 4).
Final substance-specific model results for the Michigan Longitudinal Study.
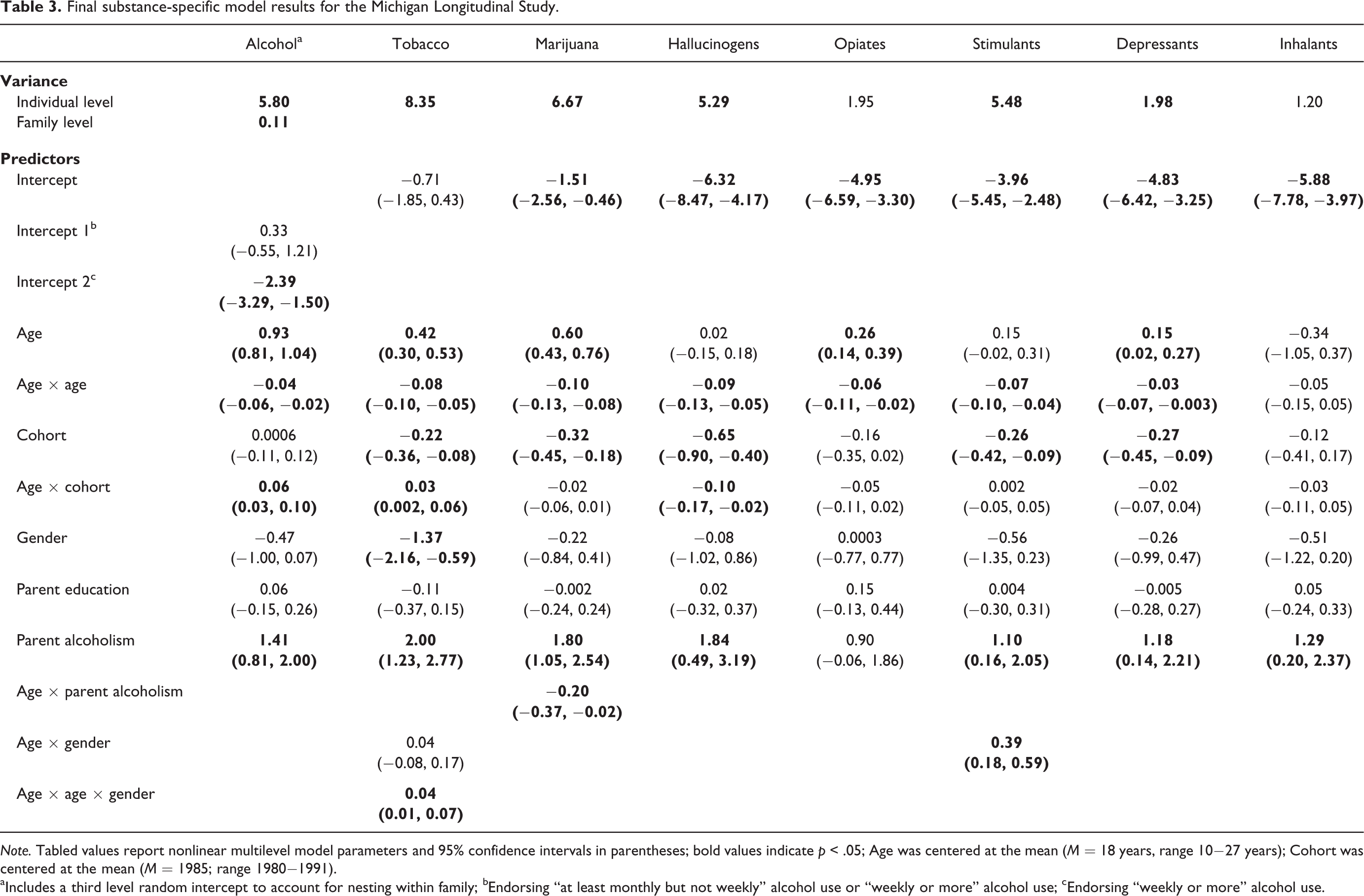
Note. Tabled values report nonlinear multilevel model parameters and 95% confidence intervals in parentheses; bold values indicate p < .05; Age was centered at the mean (M = 18 years, range 10−27 years); Cohort was centered at the mean (M = 1985; range 1980−1991).
aIncludes a third level random intercept to account for nesting within family; bEndorsing “at least monthly but not weekly” alcohol use or “weekly or more” alcohol use; cEndorsing “weekly or more” alcohol use.
Final substance-specific model results for the Adolescent and Family Development Project.
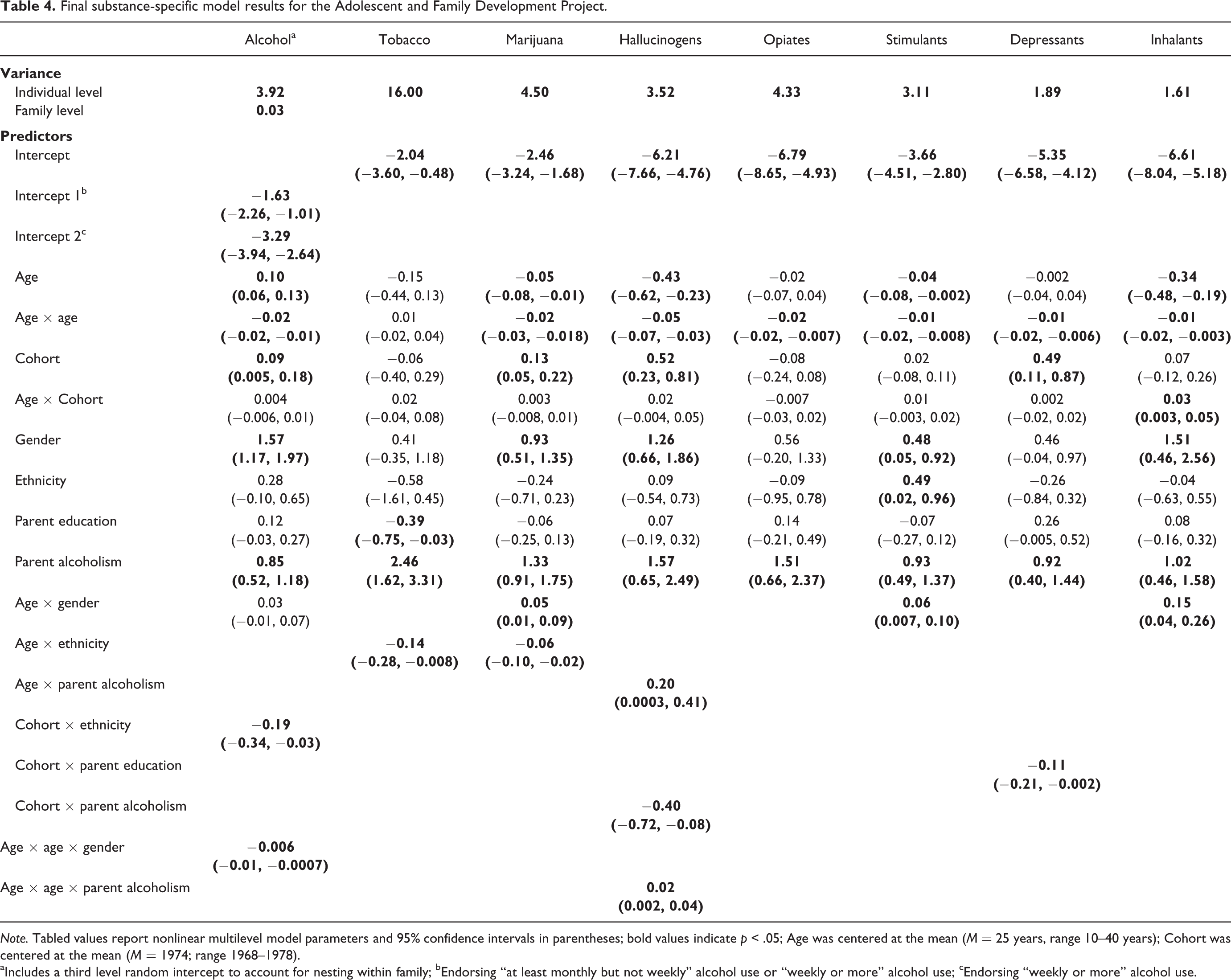
Note. Tabled values report nonlinear multilevel model parameters and 95% confidence intervals in parentheses; bold values indicate p < .05; Age was centered at the mean (M = 25 years, range 10–40 years); Cohort was centered at the mean (M = 1974; range 1968–1978).
aIncludes a third level random intercept to account for nesting within family; bEndorsing “at least monthly but not weekly” alcohol use or “weekly or more” alcohol use; cEndorsing “weekly or more” alcohol use.
Children of alcoholic parents reported greater drug use in both samples (except opiates in MLS) though this effect diminished at older ages in predicting marijuana use (MLS; β = −0.20, p = .03) and increased at older ages in predicting hallucinogen use (AFDP; β = 0.02, p = .03). Across most drugs examined, however, growth trajectories of substance use were not significantly different in children of alcoholics as compared to children of non-alcoholic parents.
Gender and parent education effects were limited. In MLS, the effect of gender on tobacco and stimulants use depended upon age. Specifically, the likelihood that females used tobacco diminished with age (β = 0.04, p = .003) whereas the likelihood that males engaged in stimulant use increased with age (β = 0.39, p = .0002). In AFDP, males reported greater alcohol use with age (β = −0.006, p = .03) and gender differences emerged with increasing age for use of inhalants, stimulants, and marijuana (β = 0.15, p = .008, β = 0.06 p = .03; β = 0.05, p = .007, respectively). Greater parent education predicted lower tobacco use in AFDP (β = −0.39, p = .04). Lastly, Hispanic respondents reported higher rates of stimulant use than non-Hispanic Caucasian respondents (AFDP; β = 0.49, p = .04), and Hispanic respondents decrease marijuana and tobacco use at a more rapid rate than their non-Hispanic counterparts with age (AFDP; β = −0.06, p = .005 and β = −0.14, p = .04, respectively).
After controlling for covariates and age trends, cohort remained a significant predictor in MLS and AFDP models. The typical individual in more recent birth cohorts in MLS reported significantly less marijuana (β = −0.32, p < .0001), hallucinogen (β = −0.65, p < .0001), stimulant (β = −0.26, p = .003), depressant (β = −0.27, p = .004), and tobacco use (β = −0.22, p = .002). In contrast, the typical individual in more recent birth cohorts in AFDP reported higher levels of alcohol (β = 0.09, p = .04), marijuana (β = 0.13, p = .003), hallucinations (β = 0.52, p = .0004), and depressants (β = 0.49, p = .01). Additionally, after controlling for covariates and cohort trends, significant developmental trajectories (age trends) were found for all substance use outcomes with the exception of inhalants (MLS) and tobacco (AFDP).
The age-by-cohort interaction was significant for alcohol (β = 0.06, p = .0001), tobacco (β = 0.03, p = .03), and hallucinogens in MLS (β = −0.10, p = .01) and for inhalants in AFDP (β = 0.03, p = .03) suggesting cohort differences in drug use trajectories may be sample and drug specific. Plots of model-implied logits showed that the typical individual born in more recent birth cohorts in MLS had steeper developmental trajectories than those born in less recent birth cohorts when predicting tobacco and alcohol use and a less steep developmental trajectory when predicting hallucinogen use (see Figure 1). Given the lower intercepts of those born more recently, the overall pattern of alcohol and tobacco use is one of latter-born cohorts more quickly catching up to their counterparts. A plot of model-implied logits showed that the typical individual born in more recent birth cohorts in AFDP had less steep developmental trajectories of inhalant use than those born in less recent birth cohorts (see Figure 2). 2
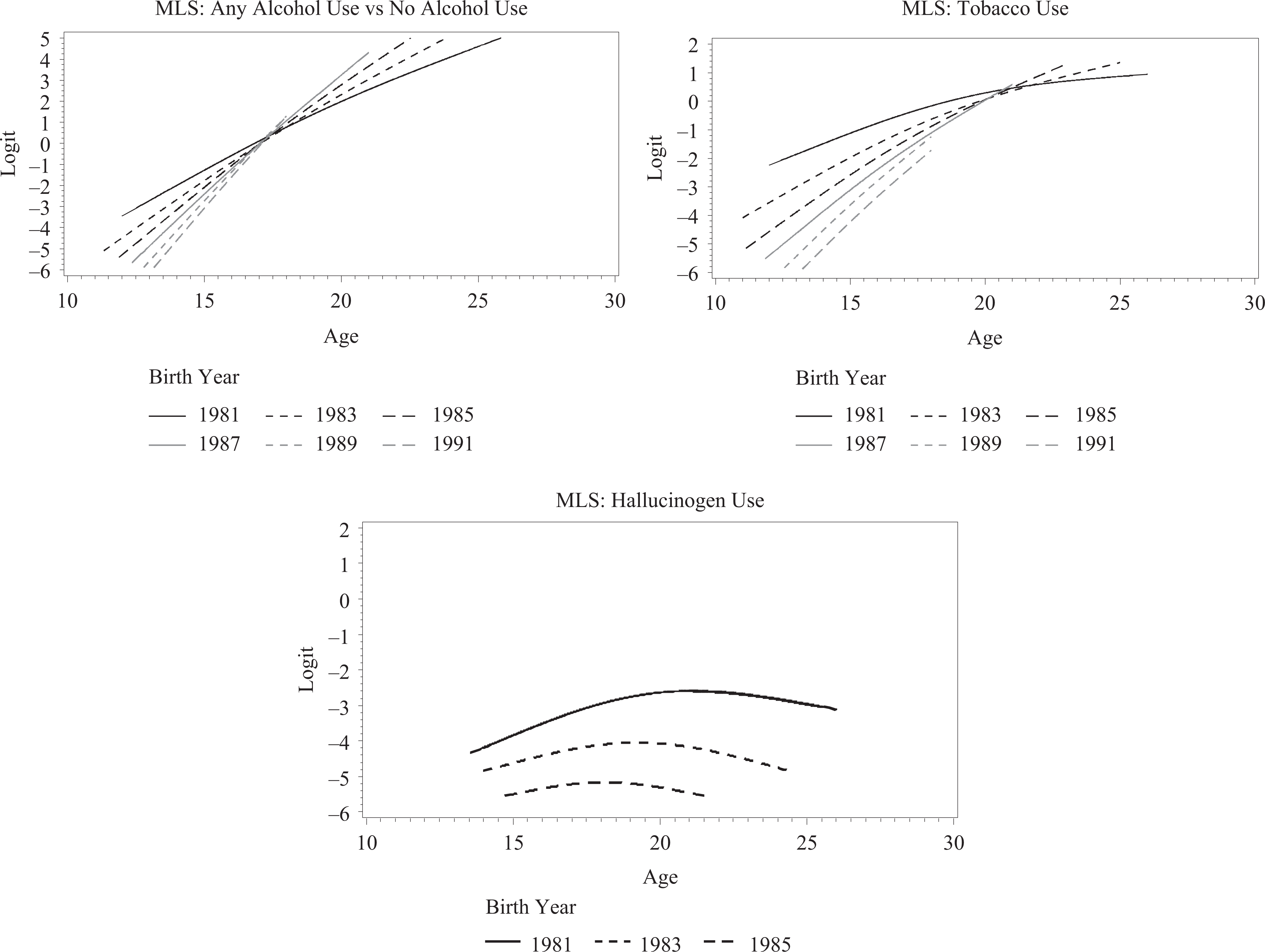
Michigan Longitudinal Study model-implied logits for substance use outcomes with a significant age-by-cohort interaction
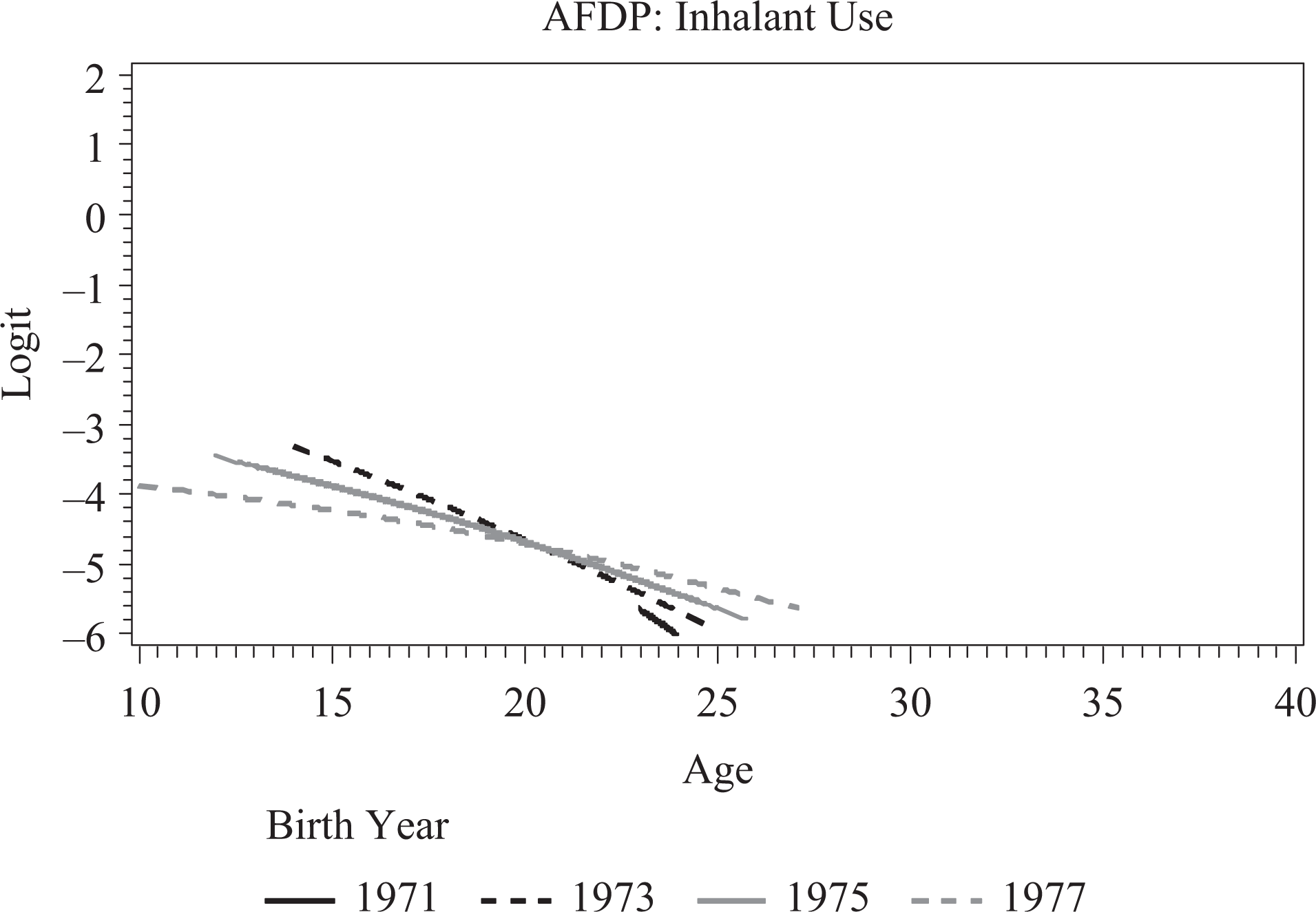
Adolescent and Family Development Project model-implied logits for substance use outcomes with a significant age-by-cohort interaction
Discussion
Given the prevalence of trajectory-based analysis of a variety of outcomes, the current study demonstrates an analytic approach to examine the extent to which age and cohort effects mutually exist in longitudinal, multi-cohort studies and the extent to which age-based trajectories vary over cohorts. The current study outlined a four-step model building approach that utilizes multilevel modeling to incorporate multiple time trends simultaneously.
Results indicated both a significant age trend as well as a cohort trend across a range of substance use outcomes, indicating that above and beyond developmental trends, an individual’s birth year was a significant predictor of substance use. This indicates the important and unique contribution of these two metrics of time. By and large, cohort trends did not significantly dampen age-based trajectory trends. However, for a minority of substances, age and cohort trends interacted in the prediction of substance use suggesting that cohort effects in developmental trajectories may be study- and drug-specific.
Age trends in the current study replicated those reported in US national data (Jager et al., 2013; Johnston et al., 2013) and in previous studies published from these data (Chassin, Curran, Hussong, & Colder, 1996). However, few studies report age-based trajectories that span such a large age range. Consistent with the literature, the age trend of increasing drug use throughout adolescence which levels off and then decreases in the 20s was found across most drugs of abuse, with the anticipated exception of inhalants (Johnston et al., 2013). Peak ages of drug use differed across substances, study, and in some instances cohort, but most occurred around age 25 (with the exception of inhalants). Some drugs showed more significant declines into young adulthood than did others, including inhalants, hallucinogens, and marijuana.
Although individual trajectories of drug use showed expected patterns, more novel in the current study was the examination of cohort effects in these developmental trajectories. Within AFDP, more recent birth years reported significantly more substance use whereas within MLS, more recent birth years reported significantly less substance use. Although apparently counter-intuitive, the birth cohorts assessed in AFDP (1968–1978) and MLS (1980–1991) are not overlapping and significant changes in cohort trends in drug use within the United States are documented by the Monitoring the Future study to have occurred around the break point between these studies. Notably, the direction of cohort effects found in the current study maps roughly onto cross-sectional rates of endorsement found in the Monitoring the Future study (Johnston et al., 2013) for similarly aged samples. For example, rates of drug use show a slow decrease across cohorts in the years covered by the AFDP study; however, those rates become steady or increase in the years covered by the MLS study. Thus, the cohort trends in our high-risk samples correspond roughly with those in MTF.
Multiple factors may account for these cohort trends in the data (see Johnston et al., 2013 for a review) including legislative changes in drinking age (for alcohol; Toomey, Nelson, & Lenk, 2009), changing attitudes regarding specific drugs of abuse (Keyes et al., 2011, 2012), and the introduction of new drugs that impact drug preferences and access. Jager and colleagues (2013) noted that cohort trends in MTF were fairly uniform across age groups until the mid to late 1980s. As others have indicated (Duncan, Duncan, & Hops, 1996), these findings underscore the importance of evaluating cohort equivalence in cohort-sequential studies prior to defining age-based trajectories in the absence of cohort effects. The more general point is that the analytic approach demonstrated in the current study allows for an articulation of these effects so that future studies can capture the relativity of trajectory findings and cohort effects.
However, more complicated to take into account are interactions between age and cohort effects in patterns of drug use over time. This interaction was predicted given that after the mid to late 1980s, MTF cohort trends appeared to stagger across age groups, often impacting younger age groups first. This finding may reflect the vulnerability of younger adolescence to emerging trends in substance use, changing their trajectories of substance use more notably than older adolescents who may already have an established attitude toward and pattern of use. In the current study, several age-by-cohort interactions predicted drug use. Specifically, the typical individual born in more recent birth cohorts had steeper developmental trajectories when predicting tobacco and alcohol use in MLS and a less steep developmental trajectory when predicting hallucinogen use in MLS and inhalant use in AFDP. Although parameter estimates for these interaction effects appeared modest, they indicate the need for researchers to examine such effects in future research studies.
Although demonstrating an analytic approach for examining multiple time trends contributes to the literature on cohort and age effects in cohort-sequential designs, the current study has three primary limitations. First, the two studies examined were not designed with this analysis in mind and therefore have a limited range of birth years and less densely populated age-by-cohort cells than desired for examining multiple time trends. In addition, the lack of overlap in birth years between studies prevented the use of an Integrative Data Analysis. Second, we demonstrate only one possible analytic method for examining cohort effects in age-based trajectories. Future work should demonstrate alternative methodologies (e.g., growth mixture modeling). Third, the samples used in the current study are both high-risk. Although this increases rates of illicit drug use and therefore makes possible the analysis of specific drug classes, rates of endorsement reported are not representative of a normative population and substantive findings should be interpreted with the sample in mind. Moreover, the current study only includes individuals from the United States, limiting substantive conclusions to international populations. However, the analytic methodology demonstrated within this study can be applied to research being conducted internationally.
In conclusion, these findings are particularly relevant for multi-cohort longitudinal studies in which individuals born across a range of years or even decades are examined. Furthermore, future research should extend this work to address cohort effects in pooled data analytic methods, including meta-analysis or integrative data analysis. Such methods often fail to account for or even consider the role of cohort. However, as highlighted in the current study, birth year is a significant predictor of a range of substance use outcomes and should be considered in long-term studies of substance use trajectories. Moreover, outcomes other than substance use may be affected by cohort trends. This methodology provides a simple strategy that could be used to examine multiple time trends with any outcome of interest.
Footnotes
Acknowledgements
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. There are no conflicts of interest to report.
Funding
The current manuscript was supported by Award Numbers R01 DA015398, F31 DA033688, and F31 DA034439 from the National Institute on Drug Abuse. The research studies described were supported by Award Number R01 DA005227 from the National Institute on Drug Abuse and by Award Numbers R01 AA 007065m R37 AA 007065, and R01 AA016213 from the National Institute on Alcohol Abuse and Alcoholism.