
Abstract
Drawing from dispositional mindfulness research and stress and coping theories, we tested whether adolescents’ dispositional mindfulness was associated with perceptions of peer victimization and exclusion and internalizing symptoms. We further explored the role of dispositional mindfulness as a protective factor buffering the impact of peer victimization and exclusion (PVE) on internalizing symptoms. Participants were 361 (40% boys) adolescents aged between 11 and 18 years (M = 14.9, SD = 1.4) who completed a questionnaire to assess dispositional mindfulness, perceptions of PVE, social anxiety and depressive symptoms, and loneliness. As expected, more frequent experience of PVE was associated with reporting more symptoms of social anxiety, depression, and loneliness. Further, adolescents who reported higher dispositional mindfulness also reported fewer symptoms of social anxiety, depression, and loneliness, even after controlling for gender and experiences of PVE. Dispositional mindfulness was not protective against (i.e., did not buffer) the effects of PVE on internalizing symptoms. Instead, we found that PVE had a stronger association with symptoms of social anxiety, depression, and loneliness when mindfulness was high relative to when it was medium or low. Yet, victimization was associated with greater social anxiety, depressive symptoms, and loneliness at all levels of mindfulness.
Keywords
The practice of mindfulness, traditionally cultivated through mindfulness meditation, aims to increase awareness of present experience, with acceptance (Greenberg & Harris, 2012; Kabat-Zinn, 1994, 2003). A mindful state has been described as maintaining attention to the present moment-by-moment, while accepting things as they present, and doing so nonjudgmentally. Drawing upon this tradition, mindfulness has also been conceptualized as an inherent capacity to view and respond to one’s internal and external environment in a way consistent with a mindful state (Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006; Brown & Ryan, 2003). Researchers have labeled this tendency to be mindful as dispositional (or trait) mindfulness.
Dispositional mindfulness is expected to activate internal mechanisms, including cognitive, emotional, and behavioral flexibility, which facilitate adaptive emotion and behavioral regulation (Shapiro, Carlson, Astin, & Freedman, 2006). Multiple stress and coping theories (Compas, Connor-Smith, Saltzman, Thomsen, & Wadsworth, 2001; Skinner & Zimmer-Gembeck, 2007, 2016) and neurodevelopmental perspectives (e.g., Sanger & Dorjee, 2015) identify flexibility and regulation as parts of the process of successfully attending, responding, and adapting to stressful events. However, there has been limited research focused on whether mindfulness, as a naturally occurring disposition, develops during adolescence in ways consistent with what is known about adolescent development of cognitive and emotional capacities assumed to be associated with mindfulness (Friedel et al., 2015; Warren, Shubert, & Wray-Lake, 2020; Zimmer-Gembeck & Skinner, 2011). For example, mindfulness has been described as a metacognitive skill (Bishop et al., 2004), and metacognition is not fully formed until at least the second decade of life (Kuhn, 2000; Skinner & Zimmer-Gembeck, 2016).
Given the possibility that mindfulness may develop during adolescence, it is not yet clear whether mindfulness is as beneficial to adolescents as it has been found to be for adults (Gu, Straus, Bond, & Kavanagh, 2016; Shonin, van Gordon, & Griffiths, 2016). Although many views on mindfulness as a personal strength and a stress-reduction technique have been applied through mindfulness interventions for children and adolescents (e.g., Emerson, de Diaz, Sherwood, Waters, & Farrell, 2020; Weijer-Bergsma, Formsma, de Bruin, & Bögels, 2012; Zoogman, Goldberg, Hoyt, & Miller, 2015), few studies have examined adolescents’ dispositional mindfulness as a strength when adapting to stressful events. At present, we could locate only a small number of published studies (not involving intervention) that specifically examined adolescents’ dispositional mindfulness and associations with mental health (e.g., Bluth & Blanton, 2014; Calvete, Orue, & Sampedro, 2017; Ciarrochi, Kashdan, Leeson, Heaven, & Jordan, 2011; Ciesla, Reilly, Dickson, Emanuel, & Updegraff, 2012; Marks, Sobanski, & Hine, 2010; Pepping, Duvenage, Cronin, & Lyons, 2016; Xu et al., 2018). In general, these studies have reported that adolescents higher in dispositional mindfulness also exhibit or report better well-being and less emotional distress. In addition, we located one published study that examined dispositional mindfulness and associations with peer stress over time (Riggs & Brown, 2017). This prospective study of young adolescents found that peer victimization was linked to declining dispositional mindfulness over time. However, we could locate no study of whether dispositional mindfulness is protective (i.e., buffers) against the negative effects of peer stress on adolescents’ mental health. To fill this gap, our primary purpose in the present study was to test whether dispositional mindfulness buffers against the negative socioemotional consequences known to be associated with peer stressful events. The stressor domain of study was peer victimization and exclusion (PVE), which encompasses both physical (i.e., overt) victimization, such as hitting and pushing, and relational victimization, including ostracism and a focus on harming relationships with others (Coyne & Ostrov, 2018; Zimmer-Gembeck, Pronk, Goodwin, Mastro, & Crick, 2013). PVE is known to have detrimental effects on social and emotional maladjustment (Zimmer-Gembeck, 2016). As markers of maladjustment, we investigated three forms known to be quite prevalent among adolescents, namely social anxiety, depression, and loneliness (Kessler, Chiu, Demler, & Walters, 2005; Patel, Flisher, Hetrick, & McGorry, 2007; Waters & Craske, 2016).
Dispositional mindfulness, PVE, and internalizing symptoms
PVE and symptoms
PVE is a common adolescent experience, with approximately 17% to 25% reporting some form of bullying once a week or more (e.g., Craig et al., 2009; Cross et al., 2009; Harel-Fisch et al., 2011). PVE seems to peak between the ages of 13 to 16 years, and PVE, or the perception of PVE, can be psychologically damaging and socially isolating (Lopez, & DuBois, 2005; Nansel et al., 2001; Zimmer-Gembeck, Nesdale, Webb, Khatibi, & Downey, 2016). PVE is expected to interfere with the fulfilment of the need for belonging, and when the need for belonging is not fulfilled, negative affect, distress, and self-doubt can be the outcomes (Baumeister & Leary, 1995; Leary, 2001). This may be particularly true during adolescence, when young people are navigating social change and learning to regulate emotions and developing coping strategies to apply in new and challenging social contexts (Sommerville, 2013; Zimmer-Gembeck & Skinner, 2016). Whereas many adolescents adjust and learn adaptive coping and regulation skills, others have difficulties and internalizing symptoms may emerge. For example, the widespread finding that victims of PVE experience poorer socioemotional adjustment, including reporting more loneliness, social anxiety, and depressive symptoms, has been summarized in at least two meta-analyses (Hawker & Boulton, 2000; Reijntjes, Kamphuis, Prinzie, & Telch, 2010).
Dispositional mindfulness and internalizing symptoms
Dispositional mindfulness has been found to be a resource for positive functioning and related to adaptive emotion regulation and coping responses to stressful events, such as PVE. For example, mindfulness has been associated with greater connection and closeness in relationships (Brown & Ryan, 2003; Kabat-Zinn, 1993; Welwood, 1996). In addition, other research (e.g., Barnes, Brown, Krusemark, Campbell, & Rogge, 2007; Carson, Carson, Gil, & Baucom, 2004) has found that positive interpersonal qualities, reduced relationship stress, and healthy relational functioning are all correlates of greater mindfulness. Taken together, this research suggests that dispositional mindfulness should be associated with reduced loneliness, given that the experience of loneliness can result from a lack of close relationships or the existence of close relationships that do not fulfil needs for relatedness (Dykstra & Fokkema, 2007; Rubin, Bukowski, & Parker, 2006).
PVE is an aversive experience that implies a lack of belongingness, and as such it is likely some anxiety, particularly social anxiety or the fear of negative evaluations from others, will co-occur or develop. Children and adolescents who experience PVE report a greater fear of negative evaluation and heightened distress in social situations that may involve evaluation or rejection, and social avoidance is often a common response to the experience of PVE, which itself is linked to increasing social anxiety and other socioemotional problems (Klemanski, Curtiss, McLaughlin, & Nolen-Hoeksema, 2017; Mathews, Kerns, & Ciesla, 2014; Zimmer-Gembeck, 2015). Mindfulness-based interventions have been effective in treating disorders characterized by rejection sensitivity, including social anxiety (Goldin & Gross, 2010). Moreover, in one study of adolescents, dispositional mindfulness was associated with fewer social anxiety symptoms (Hambour, Zimmer-Gembeck, Clear, Rowe, & Avdagic, 2018). In another study of undergraduate students, dispositional mindfulness was associated with less anxiety about rejection and negative affect (Peters, Eisenlohr-Moul, & Smart, 2015).
In addition to the proposed benefits for loneliness and social anxiety, theory suggests that greater dispositional mindfulness may be particularly relevant for lowered depressed mood (Baer et al., 2006). Instead of accepting and not judging personal negative feelings, individuals low in dispositional mindfulness might reject, avoid, brood on, or suppress their thoughts and feelings, resulting in the emergence or escalation of depressive symptoms (Ciesla et al., 2012). Moreover, individuals who are less mindful have been found to report a decreased ability to recognize self-regulation failures and seem to experience more depressive symptoms because of maladaptive coping responses (Ciesla et al., 2012; Pyszczynski & Greenberg, 1987).
Dispositional mindfulness as a stress buffer
Another explanation for the association of dispositional mindfulness with better functioning is the stress buffering hypothesis (e.g., Cohen & Edwards, 1989). In this view, psychological resilience factors, such as dispositional mindfulness, protect or buffer against the negative cognitive or emotional (or even physiological) effects of stressful events but will not give additional health benefits in the absence of stress (Brown, Weinstein, & Creswell, 2012). More specifically, theory suggests that dispositional mindfulness might be a buffer against the negative effects of stress, because mindfulness can bring clarity and richness to current stressful experiences by encouraging moment-to-moment perception of events, free from a dense filtering of experience through biased thoughts (Brown, Ryan, & Creswell, 2007). Therefore, when experiencing an interpersonally stressful event, such as PVE, individuals high in dispositional mindfulness would see things more clearly and completely and be capable of responding in a more coherent, organized, and flexible manner untainted by extreme emotional reactions. Given that a nonjudgmental approach to day-to-day experiences is a key aspect of dispositional mindfulness, adolescents higher in this capacity might also be less likely to focus on or ruminate on who is at fault for PVE; evidence has shown that attributional processes following PVE can play a role in subsequent development of increasing emotional or behavioral adjustment problems (e.g., Zimmer-Gembeck et al., 2016). Dispositional mindfulness may help adolescents to avoid rumination and attributional effort to explain their experiences of PVE, allowing them to disengage from and then, subsequently, reengage with new, more positive social situations or partners. In essence, youth higher in dispositional mindfulness would be protected or buffered from the resulting internalizing problems and feelings of loneliness that could emerge following PVE.
The present study
In summary, evidence, much of it conducted with young or older adults, suggests dispositional mindfulness is a resource that will directly minimize, but also buffer, against symptoms of social anxiety and depression, as well as feelings of loneliness, that have been associated with experiences of stress. However, much of this research has been conducted with adults and, given that adolescents are developing some of the metacognitive skills expected to be necessary to support dispositional mindfulness, it is important to understand if this also occurs for adolescents. More specifically, for the primary analyses, we had two hypotheses:
1. PVE will have positive, and dispositional mindfulness will have negative, unique associations with social anxiety and depression symptoms, and feelings of loneliness among adolescents.
2. Dispositional mindfulness will buffer (i.e., moderate) the effect of PVE on adolescents’ internalizing symptoms and loneliness, which will be revealed by a weaker association of PVE with social anxiety and depressive symptoms and loneliness when dispositional mindfulness is high relative to when it is low or moderate.
Method
Participants
The participants were 361 students (144 boys, 209 girls, 8 identified as other or were missing gender), enrolled in Grades 7 to 12, at an independent public school in an urban area of Australia. Another 40 students attended the survey session, but patterned responding was found or they did not complete most of the survey so were excluded from the analyses. Fifty percent of the student body was randomly selected to participate by the school and, overall, the participation rate was 45% of all students. To our knowledge, these students were representative of the entire student body. The survey session was completed in the last week of the school term. Students ranged in age from 11 to 18 years, with a mean age of 14.9 years (SD = 1.4). Most participants (79%) identified as being White/Caucasian, 5.3% reported Asian origins, 2.8% identified as being Australian First People or Pacific Islander, 5.5% identified as other, while the remaining 7.4% did not report ethnicity. Of all participants, 41% reported some experience with mindfulness or meditation, and 17% engaged in religious or prayer activities. Dispositional mindfulness did not differ between adolescents who did or did not report practice of mindfulness and/or meditation, t(356) = −.77, p = .44.
Measures
Depressive symptoms
Participants completed the Short Mood and Feelings Questionnaire (Angold et al., 1995) to measure self-reported depressive symptoms. The scale contained 13 items (e.g., “I cried a lot”), and students were asked to report their feelings within the past 2 weeks. Each item was rated on a 5-point scale from 1 (not at all) to 5 (all the time), with responses averaged so that higher scores reflected higher severity of depression, Cronbach’s α = .95.
Social anxiety symptoms
Participants completed the Social Anxiety Scale for Adolescents (La Greca & Lopez, 1998) to measure the subjective experience of social anxiety. The scale contained 18 descriptive self-statements (e.g., “I worry about being teased”). Each item was rated on a 5-point scale from 1 (not true) to 5 (very true), with responses averaged so that higher scores reflected higher severity of social anxiety, Cronbach’s α = .95.
Loneliness
Participants completed the Loneliness and Social Dissatisfaction Scale (Asher, Hymel, & Renshaw, 1984; Asher & Wheeler, 1985) to measure subjective feelings of loneliness. The scale contained 16 items in total (e.g., “I don’t have any friends in class”). Each item was rated on a 5-point scale from 1 (not true of me) to 5 (very true of me). Items were averaged to form a composite score, with higher scores indicating greater feelings of loneliness, Cronbach’s α = .90.
Perceptions of victimization and exclusion
Participants completed the Revised Peer Experiences Questionnaire (Prinstein, Boergers, & Vernberg, 2001) to assess the frequency of perceived experiences of physical and relational PVE. The scale contained 9 items, with 4 items assessing physical victimization (e.g., “A teen threatened to hurt or beat me up”) and 5 items assessing relational victimization and exclusion (e.g., “A teen left me out of what he or she was doing”). Each item was rated on a 5-point scale from 1 (never) to 5 (a few times a week), with item scores averaged so that higher scores reflected higher perceived experiences of PVE, Cronbach’s α = .87. Cronbach’s α was .84 for physical and .85 for relational victimization.
Dispositional mindfulness
Participants completed 31 items from the Five Facet Mindfulness Questionnaire (Baer et al., 2006) to measure dispositional mindfulness. The 31 items came from four subscales, including describing (8 items, “I am good at finding the words to describe my feelings”), acting with awareness (8 items, “I am easily distracted”), nonjudging (8 items, “I disapprove of myself when I have irrational ideas”), and nonreactivity (7 items, “I watch my feelings without getting lost in them”). The observing subscale items were not administered given previous evidence that this subscale is relevant for participants who practice meditation, but this subscale may perform differently for nonmeditators (Baer et al., 2006, 2008; Goodall, Trejnowska, & Darling, 2012) and has also been found to perform differently in adolescents (Abujaradeh, Colaianne, Roeser, Tsukayama, & Galla, 2019; Hambour et al., 2018). For example, research has shown the observing subscale has only small (and sometimes negative) associations with other dispositional mindfulness subscales and has been found to have positive associations with symptoms of emotional maladjustment (e.g., Hambour et al., 2018). Items were rated on a 5-point scale from 1 (never or very rarely true) to 5 (almost always or always true) and were averaged so that higher scores indicated greater dispositional mindfulness, Cronbach’s α was .86. Cronbach’s α for items on the four measured subscales ranged from .72 for nonreactivity to .84 for acting with awareness.
Procedure
The survey was completed as a school-related project, whereby the school requested all students to participate, but students had an option to decline. Participants completed paper questionnaires under supervision from a teacher in a designated room on school grounds during class time. There were no incentives offered for participation. The questionnaire took approximately 40 minutes to complete. Human Research Ethics Committee approval was received to analyze the school data for research purposes.
Overview of the data analyses
Ms, SDs, and zero-order correlations between all measures were examined in preliminary analyses. In addition, t-tests were used to compare study variables between boys and girls. Next, we tested the hypotheses by analyzing total PVE as a composite of physical and relational forms of victimization and exclusion and a composite mindfulness score, but also conducted follow-up (i.e., sensitivity) analyses with physical and relational forms separately, and with subscales of dispositional mindfulness.
To test the hypotheses, multiple regression was used to test all associations and the expected interaction effect of the Composite Dispositional Mindfulness Score × the Composite Measure of PVE. The dependent variables (DVs) in the regression analyses were social anxiety symptoms, depressive symptoms, and loneliness. In these models, four independent variables (IVs) were entered, including dispositional mindfulness, PVE, age, and sex (0 = boys, 1 = girls). The interaction effect (Dispositional Mindfulness × PVE) was then entered into each regression equation to test whether the association of PVE with symptoms was weaker for participants higher, relative to lower, in dispositional mindfulness. Variables were centered prior to testing interaction effects.
As a follow-up sensitivity analysis, we regressed internalizing symptoms and loneliness on the four measured subscales of dispositional mindfulness, physical victimization, relational victimization, sex and age. We then tested moderation of mindfulness subscales and either physical or relational victimization, which involved testing eight possible moderation effects (e.g., Mindful Awareness × Physical Victimization, Mindful Awareness × Relational Victimization) in each model (for a total of 24 interactions). We briefly report on the significant interactions from these additional analyses.
Results
Missing values and nonnormality of data
There were 58 participants missing responses to one item, and 26 participants missing responses to between 2 and 6 items (no participant missed more than 6 items). Because missing data were minimal and at random, scores were formed based on the completed items to maintain all participants in the data analyses. As participants’ biological sex was included in all analyses, eight participants who did not report their sex were excluded. The symptom measures (social anxiety, depression, and loneliness) displayed some positive skew. Bivariate correlations were examined before and after a square root transformation of these variables. There was minimal difference in the correlations. Thus, the untransformed symptom measures were maintained for all analyses. The PVE measure displayed very significant positive skew. To address this, PVE was recoded into a dichotomous variable. Participants in the top 25% of PVE scores were categorized into the “high PVE” group (coded as 1, scores of 2.56 or higher) (n = 98), and the remaining 75% of participants were categorized into the other group referred to as “low PVE” (coded as 0) (n = 263). For follow-up analyses, the same procedure was used to dichotomize measures of physical victimization (0 = low, 1 = high, scores of 2.50 or higher) and relational victimization (0 = low, 1 = high, scores of 2.80 or higher). For descriptive statistics and correlations, PVE was maintained as a continuous variable. Additional follow-up analyses were also completed using continuous physical and relational victimization scores.
Correlations between measures, descriptive statistics, and sex differences
Ms, SDs, and Pearson’s correlations between the study variables are shown in Table 1. As expected, individuals reporting higher levels of dispositional mindfulness (composite and subscales) were lower in social anxiety, depression, and loneliness. Also as expected, individuals reporting higher PVE (composite, physical and relational victimization) were higher in social anxiety, depression, and loneliness. Further, individuals higher in composite dispositional mindfulness reported less PVE, as well as less physical and relational victimization. Two of the four mindfulness subscales (awareness and describing) were significantly negatively associated with physical victimization and all subscales of mindfulness were significantly negatively associated with relational victimization. As can be seen in Table 2, girls, relative to boys, had higher average scores for relational victimization, social anxiety, and depressive symptoms and lower average scores for physical victimization and mindful nonreactivity.
Descriptive statistics and bivariate correlations between all study variables (N = 361).
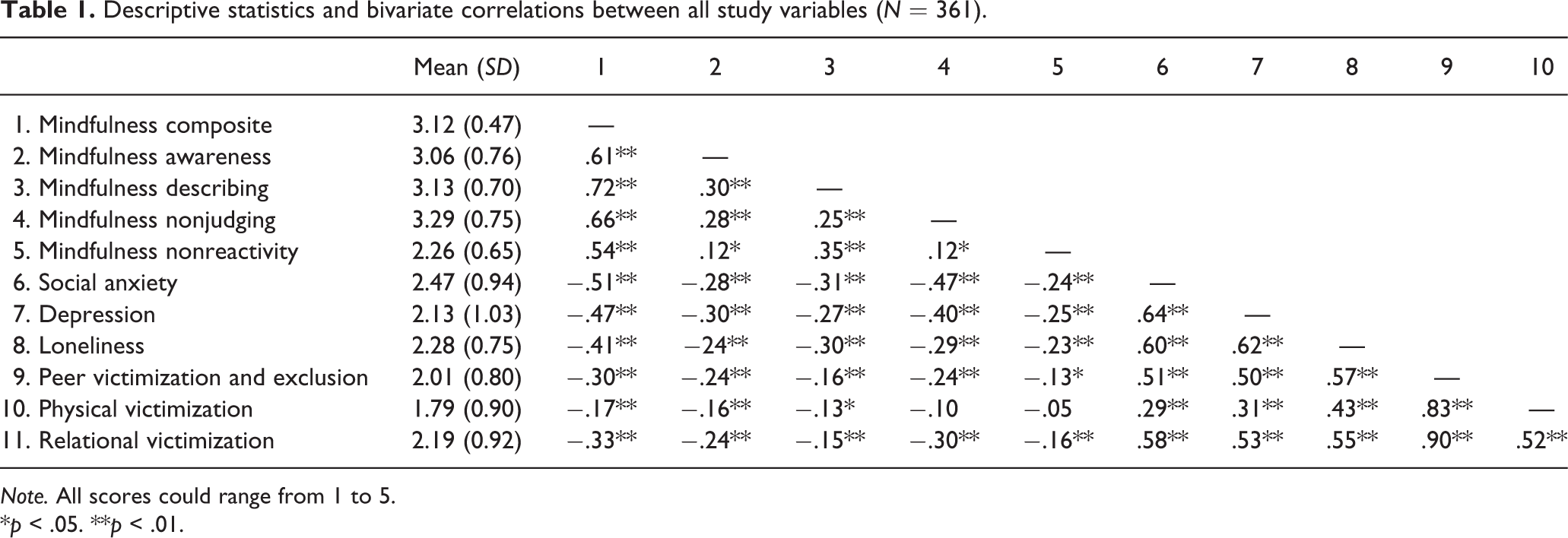
Note. All scores could range from 1 to 5.
*p < .05. **p < .01.
Means and SDs for all students and for boys and girls, and tests of sex differences.
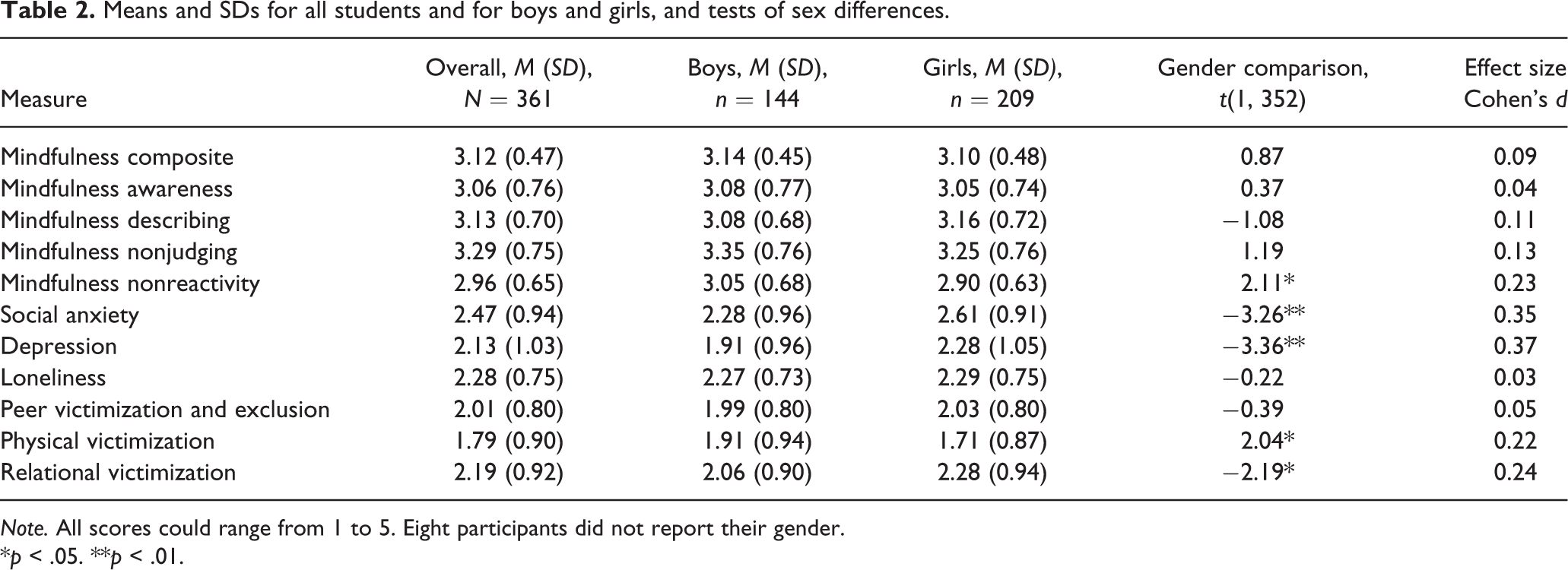
Note. All scores could range from 1 to 5. Eight participants did not report their gender.
*p < .05. **p < .01.
Symptoms as associated with dispositional mindfulness, PVE, gender, and age
Primary analyses: Composite mindfulness and PVE
In the model of social anxiety, the composite dispositional mindfulness score was significantly associated with fewer social anxiety symptoms (see Table 3). Also, composite PVE (dichotomous low/high) and gender were significantly associated with more social anxiety symptoms. Overall, 35.8% of the variance was accounted for by the IVs, F(4, 348) = 48.54, p < .001. When the moderator term was examined in Step 2 of this model, a significant moderator effect was found accounting for a significant 1.53% of the variance in social anxiety symptoms, β = .15, F(1, 347) = 8.46, p = .004. Simple slopes analysis indicated there was a significant positive association between PVE and social anxiety when dispositional mindfulness was low (1 SD below the mean = −.47), B = 0.42, p < .001, and the associations were stronger at a medium level (0), B = 0.70, p < .001, and a high level of dispositional mindfulness (1 SD above the mean = +.47), B = 0.97, p < .001 (see Figure 1).
Results of standard multiple regression analysis regressing social anxiety symptoms, depressive symptoms, and loneliness, on measures of dispositional mindfulness, peer victimization and exclusion, gender, and age (N = 353).
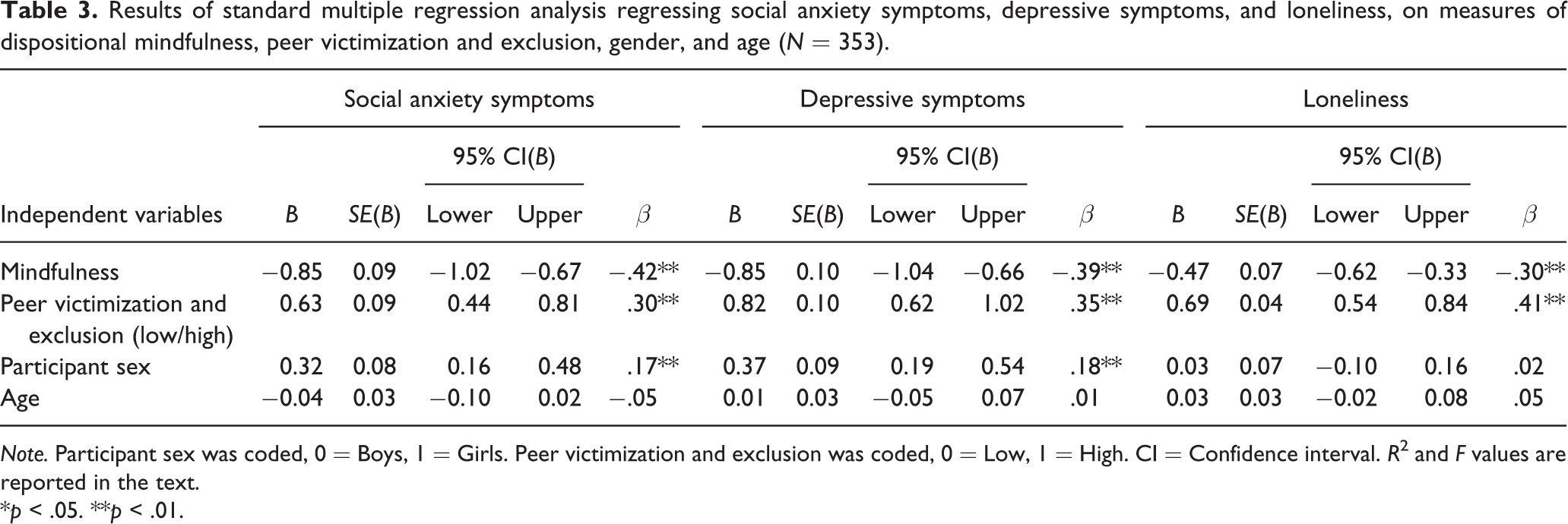
Note. Participant sex was coded, 0 = Boys, 1 = Girls. Peer victimization and exclusion was coded, 0 = Low, 1 = High. CI = Confidence interval. R 2 and F values are reported in the text.
*p < .05. **p < .01.

Associations between peer victimization and exclusion and social anxiety symptoms at low, medium, and high levels of dispositional mindfulness. Low mindfulness, n = 130; medium mindfulness, n = 104; high mindfulness, n = 127.
In the model of depressive symptoms, the composite dispositional mindfulness score was significantly associated with less depressive symptoms, and composite PVE (dichotomous low/high) and gender significantly associated with more depressive symptoms (see Table 3). Overall, 37.6% of the variance was accounted for by the IVs, F(4, 348) = 52.41, p < .001. When the moderator term was examined in Step 2 of this model, it was significant and accounted for a significant 0.91% of the variance in depressive symptoms, β = .12, F(1, 347) = 5.16, p = .02. Simple slopes analysis indicated there was a significant positive association between PVE and depressive symptoms when dispositional mindfulness was low, B = 0.64, p < .001, and the associations were significantly stronger at medium, B = 0.88, p < .001, and high levels of dispositional mindfulness, B = 1.11, p < .001 (see Figure 2).
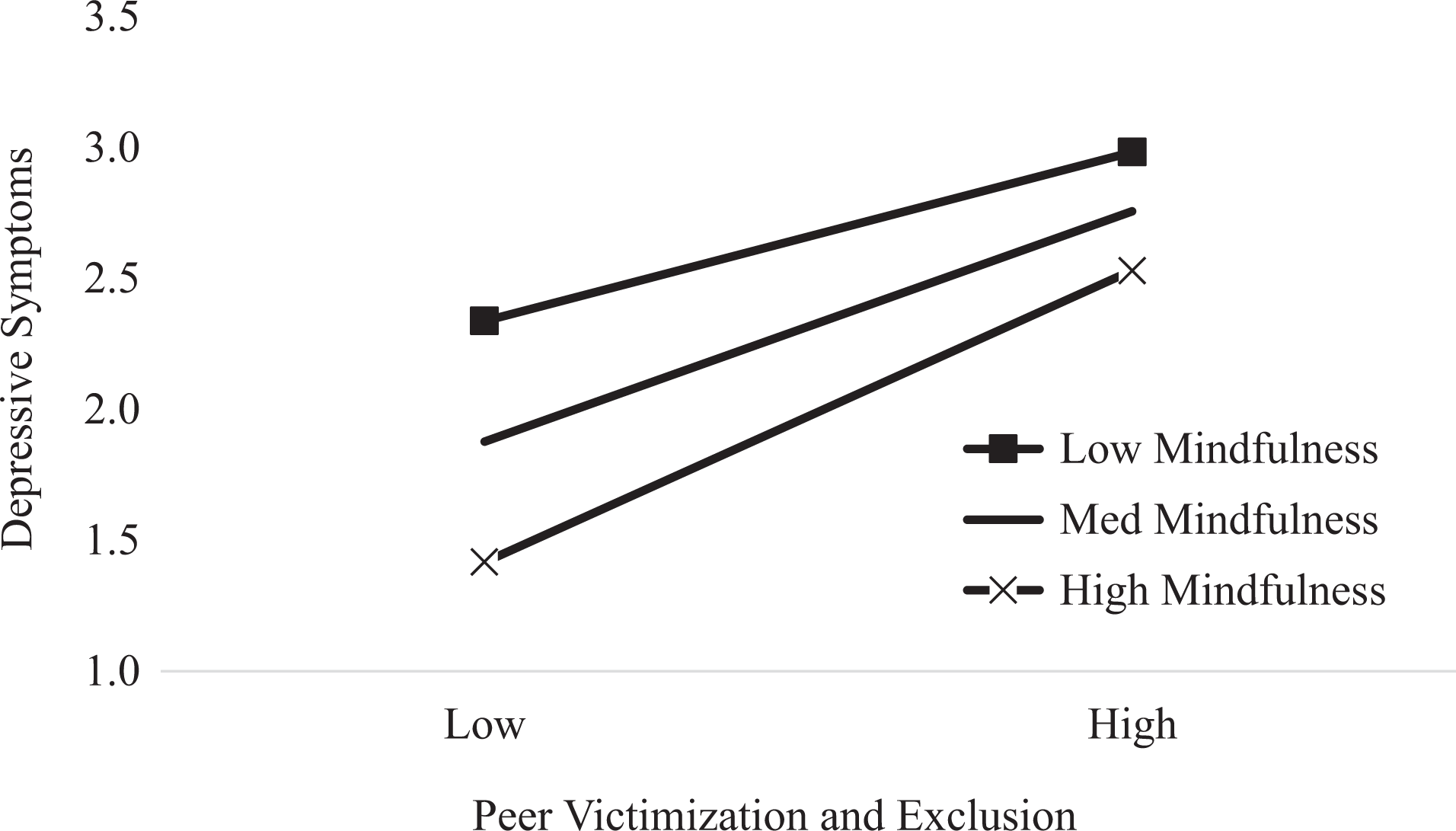
Associations between peer victimization and exclusion and depressive symptoms at low, medium, and high levels of dispositional mindfulness. Low mindfulness, n = 130; medium mindfulness, n = 104; high mindfulness, n = 127.
In the model of loneliness, composite dispositional mindfulness was significantly associated with less loneliness (see Table 3). Also, composite PVE (dichotomous low/high) was significantly associated with more loneliness. Overall, 32.3% of the variance was accounted for by the IVs, F(4, 348) = 41.42, p < .001. When the moderator term was examined in Step 2 of this model, a significant moderator effect was found accounting for a significant 1.0% of the variance in loneliness, β = .13, F(1, 347) = 5.22, p = .02. Simple slopes analysis indicated there was a significant positive association between PVE and loneliness when dispositional mindfulness was low, B = 0.56, p < .001, and the associations were stronger at medium, B = 0.74, p < .001, and high levels of dispositional mindfulness group, B = 0.91, p < .001(see Figure 3).

Associations between peer victimization and exclusion and loneliness at low, medium, and high levels of dispositional mindfulness. Low mindfulness, n = 130; medium mindfulness, n = 104; high mindfulness, n = 127.
The above primary analyses were repeated replacing the dichotomous yes/no indicator for PVE with the original continuous score. In these three models of social anxiety, depression, and loneliness, the interaction (Composite Mindfulness × Composite PVE Continuous Score) was not significant (p ranged from .188 to .959).
Follow-up analyses: Subscales of mindfulness and PVE
As can be seen in Table 4, all subscales of dispositional mindfulness except mindful awareness were uniquely associated with fewer social anxiety symptoms, while relational victimization was uniquely associated with elevated symptoms. In the second model shown in Table 4, the four subscales of dispositional mindfulness were negatively, and both physical and relational victimization were positively, associated with depressive symptoms. Finally, all subscales of dispositional mindfulness except mindful awareness were negatively associated with loneliness, while both physical and relational victimization were uniquely positively associated with loneliness. As previously found, girls reported significantly more social anxiety and depressive symptoms. For social anxiety symptoms, 42.4% of the variance was accounted for by the IVs, F(8, 344) = 31.67, p < .001. For depressive symptoms, 38.7% of the variance was accounted for by the IVs, F(8, 344) = 27.15, p < .001. For loneliness, 37.4% of the variance was accounted for by the IVs, F(8, 344) = 25.71, p < .001.
Results of standard multiple regression analysis regressing social anxiety symptoms, depressive symptoms and loneliness, on subscales of dispositional mindfulness, physical and relational victimization, gender, and age (N = 353).
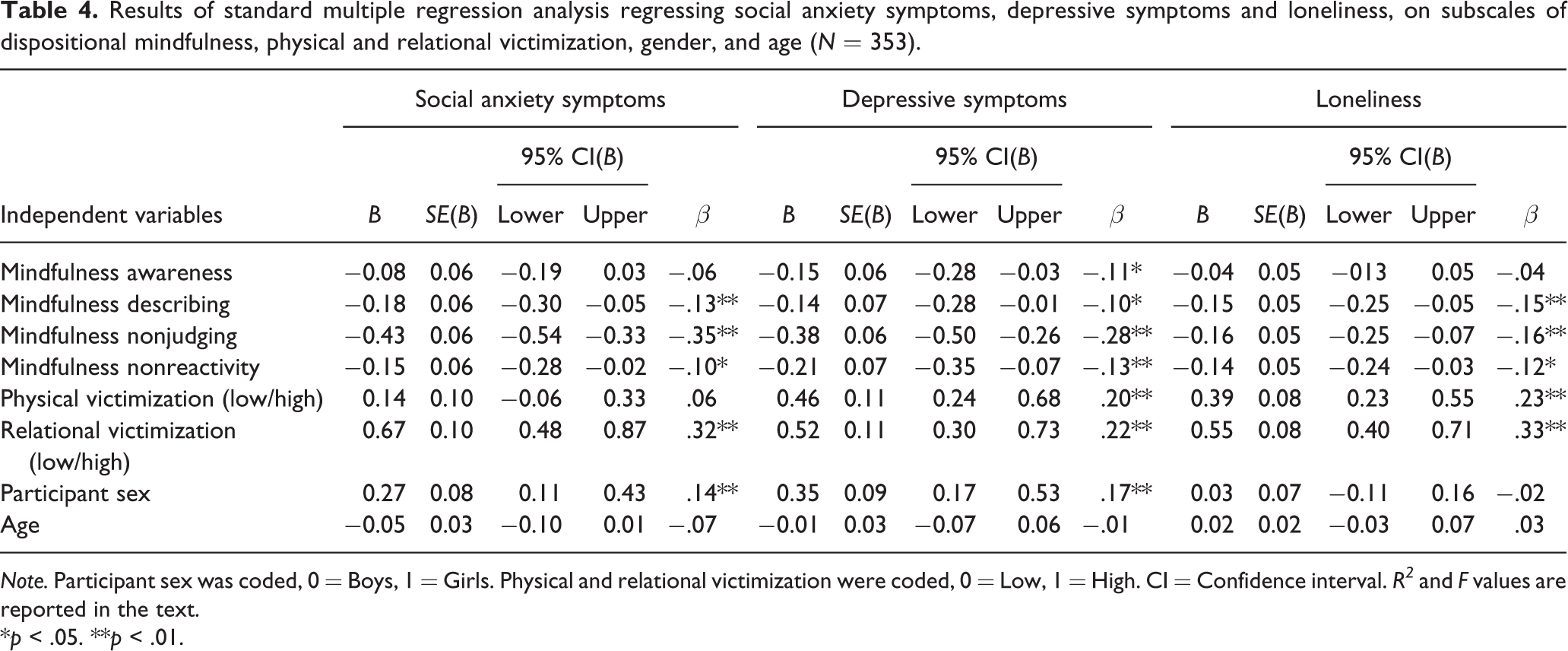
Note. Participant sex was coded, 0 = Boys, 1 = Girls. Physical and relational victimization were coded, 0 = Low, 1 = High. CI = Confidence interval. R2 and F values are reported in the text.
*p < .05. **p < .01.
When tested one at a time in 24 separate models, four of the eight moderator effects tested were significant (or marginally significant) in the model of social anxiety symptoms, one of the eight moderator effects tested was significant in the model of depressive symptoms, and no moderator effect was significant in the model of loneliness. For social anxiety symptoms, the significant interaction effects were Mindful Describing × Relational Victimization (β = .09, p = .06), Mindful Nonjudgment × Physical Victimization (β = .09, p = .05), Mindful Nonjudgment × Relational Victimization (β = .11, p = .02), and Mindful Nonreactivity × Physical Victimization (β = .12, p = .01). The pattern of findings was similar to the pattern shown in Figure 1, showing a stronger association between victimization and social anxiety symptoms when mindfulness (either nonjudgment or nonreactivity) was high relative to low. The one moderator effect in the model of depressive symptoms was Mindful Nonreactivity × Physical Victimization (β = .11, p = .03), and this effect was positive indicating a pattern similar to the pattern shown in Figure 2.
When the above follow-up analyses were repeated replacing the dichotomous yes/no indicators for physical and relational victimization with their original continuous scores, the pattern of results was similar. In particular, moderation effects were significant or marginally significant for four interactions in the models of social anxiety: mindful nonjudgment and nonreactivity across both physical and relational victimization (p ranged from .04 to .09). Also, moderation effects were significant for Mindful Nonjudgment × Physical Victimization and Mindful Nonreactivity × Physical Victimization in the model of depression (p = .04 and .02, respectively). No moderation effect was significant in the models of loneliness.
Discussion
In this study, we tested whether dispositional mindfulness was associated with fewer internalizing symptoms (defined as social anxiety and depression) and feelings of loneliness among adolescents, while simultaneously testing the associations of experiences of PVE with symptoms and loneliness. We found that adolescents who report more PVE (combining both physical and relational) are higher in social anxiety, depression, and loneliness. Moreover, adolescents who reported more physical and relational victimization had a higher level of symptoms and felt lonelier, with adolescents reporting more relational victimization being higher in social anxiety, depression, and loneliness and those reporting more physical victimization endorsing more depression and loneliness. Yet, at the same time, adolescents who scored higher on dispositional mindfulness reported less social anxiety, depressive symptoms, and loneliness, and this generally extended to all of the four subscales of mindfulness we measured, with only a few exceptions.
Further extending on these analyses, dispositional mindfulness was examined as a potential buffer of the negative effect of PVE on symptoms and loneliness. This was done by testing whether the association between PVE and internalizing symptoms was weaker at a high relative to lower levels of mindfulness. Overall, we did find interaction effects across all emotional adjustment measures when PVE, in all its forms, was dichotomized (high/low), but the findings were not consistent with what would have been expected based on a buffering hypothesis. Moreover, interaction effects were more intermittent, involving only some mindfulness subscales and either physical or relational victimization, when victimization was analyzed as a continuous score. Overall, however, when moderation was found, PVE was more strongly associated with symptoms and loneliness when mindfulness (especially nonjudgment and nonreactivity) was high compared to low. Thus, in general, adolescents reporting more mindfulness do also report fewer symptoms and less loneliness, so, on the one hand, mindfulness appears beneficial for adolescents’ well-being. On the other hand, we did not support the notion that mindfulness protects adolescents who report high PVE (relative to their peers with lower PVE) from having elevated social anxiety and depressive symptoms and more feelings of loneliness.
Key findings and future research directions
Dispositional mindfulness, PVE, and internalizing symptoms
The finding that adolescents who report a high level of PVE, both physical and relational, are experiencing more internalizing symptoms and loneliness was anticipated and is consistent with previous research (Ciesla et al., 2012; Hambour et al., 2018; Pyszczynski & Greenberg, 1987). Internalizing symptoms included responses that are common reactions to adverse peer interactions, including PVE, and the associated threat to belonging (Baumeister & Leary, 1995; Leary, 1990). In fact, PVE had quite strong cross-sectional associations with symptoms and loneliness, supporting the widespread finding reported in two meta-analyses that victims of PVE experience poorer socioemotional adjustment (Hawker & Boulton, 2000; Reijntjes et al., 2010).
What has been less frequently studied is the association of dispositional mindfulness with internalizing symptoms and loneliness among adolescents. Yet, as a few previous studies of youth have reported (e.g., Hambour et al., 2018; Lavell, Webb, Zimmer-Gembeck, & Farrell, 2018), dispositional mindfulness appears to be a way of engaging with our internal and external environment and approaching emotion that is an asset for avoiding excessively heightened internalizing symptoms (e.g., Pepping et al., 2016). Accurately describing experience and being aware and in control of actions, two important facets of dispositional mindfulness, has been expected to help adolescents remain in the present on a moment-by-moment basis both when alone and when interacting with others. This is expected to leave little opportunity for rejecting, avoiding, ruminating, or suppressing thoughts and feelings, instead encouraging acceptance and nonjudgment of experiences (Ciesla et al., 2012), directly resulting in fewer symptoms of psychopathology. Overall, findings support mindfulness as a positive resource for many adolescents.
Dispositional mindfulness as a buffer
Dispositional mindfulness was also expected to buffer the detrimental effect of PVE on mental health. Although the results showed that the association of PVE with symptoms and loneliness did differ depending on adolescents’ level of dispositional mindfulness, the pattern of results did not clearly support the buffering hypothesis. Instead, we found that PVE has an association with symptoms and loneliness at all levels of mindfulness, with the association stronger when mindfulness is high relative to when it is lower. When this moderation effect is considered alongside the finding that adolescents higher in mindfulness report fewer symptoms and less loneliness overall, this suggests two possibilities that require future research.
First, the findings suggest that there are harmful effects of PVE for all adolescents at all levels of reported dispositional mindfulness. Adolescents are facing the task of navigating social change and learning to regulate adaptively, while developing coping strategies for new and challenging social contexts (Gunnar, 2017; Johnson, Perry, Hostinar, & Gunnar, 2019; Lupien, McEwen, Gunnar, & Heim, 2009; Zimmer-Gembeck & Skinner, 2016). Rejection is distressing at any age, but there is evidence it could be even more potent during adolescence and this could explain the lack of a mindfulness buffering effect when adolescents are facing PVE (Sommerville, 2013). As adolescents mature and their metacognitive abilities and coping strategies become more differentiated and flexible, it is possible a buffering effect of mindfulness may emerge. Such a developmental question deserves future research attention.
Second, mindfulness can benefit the emotional well-being of some adolescents, but it may be of most (or only) benefit to adolescents who do not report high PVE relative to their peers. This may be because PVE could be partially outside of adolescents’ perceived control. When adolescents perceive little control over a situation, it is likely they attempt to take some control of their response to preserve their self-esteem (Kliewer & Sandler, 1992). Control may oppose mindful acceptance, therefore under distressing high PVE conditions even adolescents reporting high dispositional mindfulness may revert to control strategies rather than mindful acceptance qualities of nonjudging and nonreacting to inner experience, functioning to keep their self-esteem intact. This hypothesis is somewhat consistent with a previous study where peer victimization was linked to declining dispositional mindfulness over time (Riggs & Brown, 2017). The experience of high PVE could redirect a young person’s attention from the present moment to thoughts or rumination of PVE and worry about future PVE events; over time this effect could shift youth from traits of high mindfulness to being less mindful. The investigation of the prominent detrimental effect of PVE on the well-being of adolescents high in dispositional mindfulness could benefit from future longitudinal research to test this possibility.
It is also important to note that our follow-up analyses of dispositional mindfulness subscales, and physical separate from relational victimization, provide evidence that all main effects and interaction effects extend across most mindfulness subscales and to each form of victimization (when scored as dichotomous measures of low/high victimization). However, the findings were most consistent for the mindfulness subscales of nonjudgment and nonreactivity as related to social anxiety and depression. Thus, the associations between PVE and social anxiety and depression were significantly stronger when mindful nonjudgment and nonreactivity were high, rather than low. This suggests that discrepancy or cognitive dissonance (Festinger, 1959) might be important to consider, as well. Adolescents who are highly nonjudgmental and nonreactive may find the experience of PVE particularly inconsistent with their own beliefs, attitudes, and behavior, making it even more difficult to comprehend, dismiss, or adapt to. Thus, nonjudgmental and nonreactive adolescents may be particularly at risk for emotional maladjustment when they experience PVE or other social adversity.
Finally, the findings raise a caution for mindfulness-based programs and intervention for children or adolescents. Such programs should be fully aware of the social circumstances and coping skills of their participants, as intervening to improve mindfulness may not be fully beneficial without additional attention to social adversity and other individual skills and competencies. It also points to the need for future research that can uncover the circumstances that explain exactly why, and especially when, mindfulness is of benefit to adolescents’ well-being.
Limitations, future research, and conclusion
The present study had some limitations. First, all measures were self-reported. Although the reliability and validity of items used were established in past research, social desirability must be considered, and there is the possibility that associations were inflated due to shared method variance. Future research would benefit from using multiple reporters (e.g., peer reports of PVE). Second, all the data used were cross-sectional. Longitudinal research would enhance our understanding of how PVE could impact on later mindfulness and how mindfulness could impact on later PVE and symptoms.
In the present study, we conceptualized mindfulness as a personal internal resource implying that it is similar to and related to adaptive emotion regulation and coping responses; these responses are presumed to be important for supporting positive and productive ways of interacting with others when facing stress. However, although there is evidence that mindfulness is associated with better emotion regulation and coping (Goodall et al., 2012; Roemer, Williston, & Rollins, 2015), we did not directly assess these in response to PVE. We also did not assess interactions with others in the face of (or involved in the) stressful events. Future research may benefit from investigating the role of emotion regulation or coping in the association between dispositional mindfulness, symptoms, and loneliness. In addition, the resulting increased ability to form meaningful relationships with others that is synonymous with being more mindful (e.g., Brown & Ryan, 2003; Kabat-Zinn, 1993; Welwood, 1996) could also contribute to decreased internalizing symptoms and loneliness, although future research is needed to investigate this hypothesis.
Further, we assumed that mindfulness is a naturally varying dispositional resource and did not intervene to examine how improving mindfulness might reduce internalizing symptoms or loneliness. Mindfulness is teachable, and emerging evidence appears promising that practice to increase mindfulness among young people reduces psychological symptoms (Zoogman et al., 2015). This research is important to continue to understand whether mindfulness is a way to help youth avoid psychopathology.
In conclusion, dispositional mindfulness seems to be a personal resource that is associated with fewer symptoms and less loneliness. Nevertheless, although the association of PVE with symptoms of social anxiety, depression, and loneliness did differ depending on adolescents’ level of dispositional mindfulness, the pattern of results did not clearly support the hypothesis that mindfulness would protect or buffer against the negative effects of PVE. Instead, we found that PVE has a stronger association with symptoms when mindfulness was high relative to when it was low, suggesting that mindfulness is generally beneficial to emotional adjustment, but it does not buffer against the negative effects of victimization and exclusion by peers and may provide more benefits when adolescents are facing fewer social threats.