
Abstract
Evidence suggests an impact of the COVID-19 pandemic on mental health, particularly among emerging adults. However, theories on altruism born of suffering or adversarial growth suggest that we might also see prosocial behavior as a function of the pandemic, which may protect against mental health challenges. Because cultural values are central in determining prosocial behavior, the current study explored how cultural values were differentially associated with adaptive prosocial behaviors that might protect against mental health challenges. Participants for the current study included 5,682 young people aged 18–25 years from 14 different countries around the world (68% female, 62% college students). Path analyses suggested that there were few differences in patterns as a function of culture, but revealed that horizontal individualism and horizontal and vertical collectivism were indirectly associated with lower levels of depression via prosocial behavior toward family members. Discussion focuses on the importance of coping by strengthening family relationships via prosocial behavior during the pandemic.
Mental health challenges are a major global concern at present (World Health Organization) and may be particularly salient for emerging adults (ages 18–25 years) due to developmental characteristics of this time period that increase risk (Arnett, 2015; Arnett et al., 2014). Recent research points to the possibility that COVID-19 could exacerbate these already disturbing trends (McArthur et al., 2021; Rogers et al., 2021; Thakur & Jain, 2020). Thus, it becomes important to understand what might help individuals and families to be resilient, or to cope, in the midst of crisis. While many studies seek to identify risk and protective factors for pandemic-related mental health struggles, few explore agentive protective factors (i.e., prosocial behavior), and fewer still have done so cross-culturally or cross-nationally, which limits generalizability.
It is the case that levels of prosocial behavior (i.e., behavior intended to benefit another; Eisenberg et al., 2015) have been shown to differ across countries as a function of culture in terms of motivation (e.g., cultural values), frequency (e.g., more prosocial behavior toward family in some cultures), and type (e.g., higher rates of altruism in some cultures; Carlo & Padilla-Walker, 2020). We know less about how cultural values might impact different types of prosocial behavior or how the protective role of prosocial behavior might vary as a function of country. Thus, the current study explored associations between cultural values, prosocial behavior, and mental health during the transition to adulthood, and how these patterns might vary across 14 different countries during the global pandemic.
Emerging Adulthood and Mental Health During COVID-19
Described by some as a “global psychological pandemic” (Thakur & Jain, 2020), COVID-19 has impacted the mental health of the already psychologically susceptible emerging adult population. While many emerging adults flourish during the best of times, one study found that upwards of 30% flounder as experimentation leads to increased drinking, drug use, and internalizing problems (Nelson & Padilla-Walker, 2013). Taken together with the instability of this time period (e.g., financially, socially, geographically), the somewhat normative increase in externalizing and internalizing behavior creates elevated risk for some emerging adults. Indeed, a developmental stage characterized by experimentation, instability, and self-focus (Arnett, 2015), emerging adulthood boasts the highest levels of psychiatric disorders of any age group (40% of 18- to 29-year-olds; Arnett et al., 2014) and the measures taken to restrict the spread of the COVID-19 virus (i.e., physical distancing, closures, quarantining) may exacerbate this trend by removing the social support emerging adults depend on, especially if they live alone (Lannutti & Bevan, 2021).
Recent literature is beginning to capture how the pandemic is negatively impacting the mental health of individuals globally (Kwong et al., 2020; McArthur et al., 2021; Rossi et al., 2020; Sabato et al., 2021; Thakur & Jain, 2020), including emerging adults (Evans et al., 2021; Halliburton et al., 2021; Parola et al., 2020; Solomou & Constantinidou, 2020). For instance, research has found a significant increase in depressive symptoms among students from the United Kingdom (Evans et al., 2021) and increases in anxiety, depression, withdrawal, internalizing, and externalizing problems among Italian emerging adults (Parola et al., 2020). Recent research has also found that 18- to 29-year-olds reported the highest levels of anxiety and depressive symptoms in a sample of adults in Cyprus (Solomou & Constantinidou, 2020) and a study in the United States found that two-thirds of emerging adults claimed anxiety and depressive symptoms in the moderate to severe range, with approximately one-third reporting suicidality (Halliburton et al., 2021). While the pandemic has clearly exacerbated negative health outcomes among many emerging adults, existing research on natural disasters suggest it is also possible that crisis activates resilience and agentic coping (altruism born of suffering; Vollhardt, 2009), which may be reflected in emerging adults’ positive or prosocial behavior.
Prosocial Behavior and Mental Health
Resilience theory (which describes the experience of positive adaptation in the context of significant adversity; Masten et al., 2002) provides a framework with which to explore potential protective factors to mental health risks in the face of crisis. Perhaps more important than understanding which inherent and unadaptable individual factors contribute to resilience is the desire to understand the role that might be played by factors within one’s control: actions or behavior. A growing body of research is documenting the positive role that prosocial behavior plays in both mitigating negative outcomes (i.e., lower internalizing and externalizing symptoms; Memmott-Elison et al., 2020) and promoting positive outcomes (i.e., self-efficacy, Schacter & Margolin, 2019; social support, Qin et al., 2016).
Although the beneficial effects of prosocial behavior on mental health are increasingly documented, much of the literature still characterizes the relationship as nebulous (Hay & Pawlby, 2003; Memmott-Elison et al., 2020). This perspective may be attributable, at least in part, by the tendency to not take into account the multidimensionality of both prosocial behavior and mental health. For instance, a recent meta-analysis studying the associations between prosocial behavior and internalizing symptoms found a negative, albeit weak, link between prosocial behavior and depression, but no association between prosocial behavior and anxiety (Memmott-Elison et al., 2020). Also, the relationship between prosocial behavior and mental health toward different targets is complex, with research finding that prosocial behavior toward strangers (but not other targets) was significantly negatively related to depression (Padilla-Walker et al., 2020), while prosocial behavior toward friends was linked to increases in anxiety (Padilla-Walker et al., 2015). These findings clearly suggest a need for additional research that considers the multidimensionality of both prosocial behavior and internalizing problems. Furthermore, theoretical emphasis on the importance of culture in prosocial development (Carlo & Padilla-Walker, 2020) and the global nature of the pandemic suggest importance in considering the role of culture in the link between prosocial behavior and mental health outcomes.
Cultural Values, Prosocial Behavior, and Mental Health
Theoretically, a cultural developmental approach suggests that prosocial development cannot be fully understood without considering both the cultural context in which prosocial behavior is socialized, and the developmental life stage of the individual (Jensen, 2008, 2011). One’s moral worldview, or how that person thinks about moral issues, is influenced by cultural values and tenets (as well as developmental characteristics; self-focus, instability), which in turn shape moral and prosocial behavior. Empirical research supports these theoretical notions by consistently highlighting the importance of cultural values as predictors of prosocial behavior (e.g., familism; Carlo & Padilla-Walker, 2021). Taken together with resilience theory, during times of great stress and struggle (i.e., a global pandemic) we would expect that cultural values influence how resources are used to activate resilient behaviors. There is some evidence that collectivistic value orientations are generally more prosocial than individualistic orientations (Lampridis & Papastylianou, 2017), with the suggestion that prosocial behavior necessitates an orientation toward the needs of others (Davis et al., 2019). However, understanding the multidimensionality of prosocial behavior (Padilla-Walker & Carlo, 2014) helps to elucidate the relationship of prosociality and individualism. For instance, in defense of their assertion that “individualism is not antithetical to community involvement and prosocial action,” Kemmelmeier et al. (2006, p. 328) found that individualists are highly likely to behave prosocially based on motivations (i.e., a sense of personal responsibility and desire to live one’s life as an ethical actor) and targets (individualists were found to be especially helpful to strangers), which may differ slightly from those of collectivists.
Furthermore, researchers suggest that these broad cultural value orientations might be even better understood when subdivided into horizontal and vertical dimensions (Singelis et al., 1995). Essentially, “horizontal” refers to when one is equal in status to the selves of others, while “vertical” refers to when one is seen as different and distinct from other selves. Therefore, horizontal individualism suggests that the self is autonomous but equal in status to others, while vertical individualism maintains an autonomous self but expects difference and inequality. Similarly, horizontal collectivism maintains the self as an interdependent part of the group, with equality as a central focus, while vertical collectivism values interdependence of the group but acknowledges differences, including differences in status, with special importance placed on one’s status within the family. Given the focus on equality and community, we expected that horizontal collectivism would be most consistently associated with prosocial behavior, but this may vary as a function of the multidimensionality (e.g., target) of the prosocial behavior.
Current Study
Taken together, the current study sought to better understand adaptive prosocial responding among emerging adults from 14 different countries during the global pandemic. Although many of our research questions were exploratory in nature, we did have a number of tentative hypotheses. Our primary research question explored associations between cultural values (horizontal and vertical individualism and collectivism), prosocial behavior (toward strangers, friends, and family), and mental health outcomes (depression and anxiety). Based on past research we hypothesized that horizontal (compared with vertical) individualism and collectivism would be more consistently associated with prosocial behaviors. Although specific links with targets of prosocial behavior were difficult to hypothesize due to a lack of existing research, we expected that collectivistic values would be especially strongly associated with prosocial behavior toward family members. As a second research question, we sought to understand whether these associations would be moderated by country (acknowledging that country is not completely synonymous with culture). Past research has found that emerging adult samples are more similar developmentally (because of developmental similarities and socioeconomic status [SES] of those who attend college) than they are different culturally (e.g., Haidt et al., 1993), so we expected that we may see minimal variability as a function of country.
Method
Participants and Procedures
Participants for the current study included 5,682 young people aged 18–25 years from 14 different countries around the world (68% female). Countries included Argentina, Chile, China, Finland, France, Germany, Ireland, Italy, Lithuania, Spain, Taiwan, the Netherlands, Turkey, and the United States. Participants from most countries considered themselves members of the majority group in terms of race/ethnicity (79%), with the exception of the United States (38% majority). Participants from most countries were also college students (62%), with the exception of China (48%), Ireland (37%), and the United States (29%). See Table 1 for individual participant information for each country.
Descriptive Statistics of Study Variables by Country.
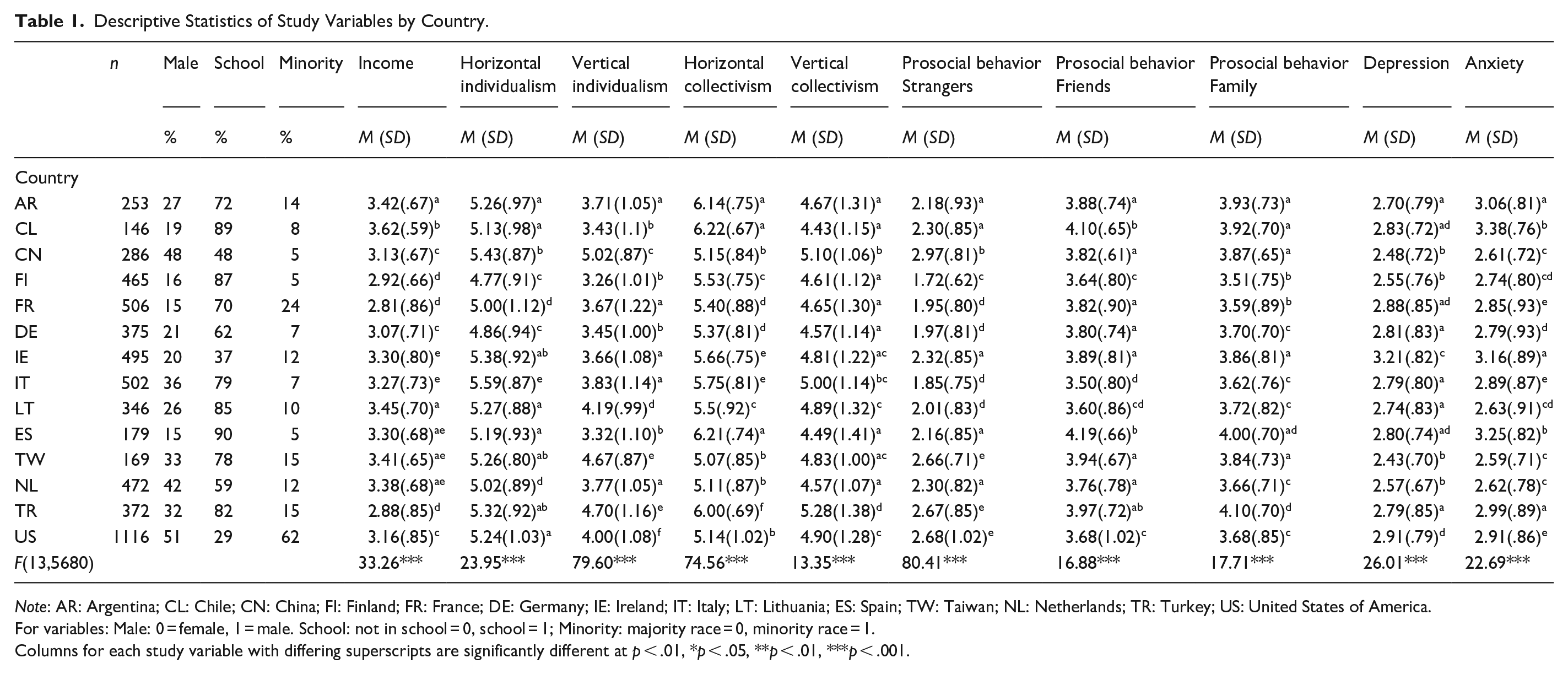
Note: AR: Argentina; CL: Chile; CN: China; FI: Finland; FR: France; DE: Germany; IE: Ireland; IT: Italy; LT: Lithuania; ES: Spain; TW: Taiwan; NL: Netherlands; TR: Turkey; US: United States of America.
For variables: Male: 0 = female, 1 = male. School: not in school = 0, school = 1; Minority: majority race = 0, minority race = 1.
Columns for each study variable with differing superscripts are significantly different at p < .01, *p < .05, **p < .01, ***p < .001.
Institutional review board (IRB) approval was obtained from the Ethics Committee of the Faculty of Social and Behavioral Sciences at Utrecht University (20-298). Procedures for data collection varied slightly by country, but all participants completed a 20-min online survey with questions about their experiences with COVID-19, prosocial behavior, and mental and social health. In most countries, faculty distributed the survey in Qualtrics (or comparable platform, e.g., survey monkey) via university and social networks, and there was minimal or no compensation for participation. However, in the United States, participants were contacted via Bovitz (a market research firm that draws national samples from existing panels), and a larger sample with equal numbers of four racial groups (African American, Latinx, Asian American, European American) was obtained.
Measures
Participants completed measures assessing their cultural values, their prosocial behavior toward strangers, friends, and family during the pandemic, and their depression and anxiety. The measures to assess cultural values, and to assess depression and anxiety, were available for use in most of the countries (respectively, 71% and 86%), but the prosocial behavior measure was only available in English. The measures were translated by faculty collaborators if there was no version in the country’s primary language available.
Cultural Values
Participants reported on orientation toward collectivism versus individualism using 16 items from the Culture Orientation Scale, four items for each subscale (Triandis & Gelfland, 1998). Respondents rated the extent to which various statements about cultural orientation reflected their values using a Likert scale of 1 (strongly disagree) to 7 (strongly agree), with higher scores reflecting greater vertical individualism (“It is important to do my job better than others” α ranged from .51 to .72), horizontal individualism (“I’d rather depend on myself than others” α ranged from .57 to .68), vertical collectivism (“It is important to me that I respect the decisions made by my group” α ranged from .59 to.79), and horizontal collectivism (“It is my duty to take care of my family, even when I have to sacrifice what I want” α ranged from .53 to .78).
Prosocial Behavior
Prosocial behavior toward different targets was measured using 15 items assessing behavior toward strangers (5 items, α ranged from .71 to .79), friends (5 items, α ranged from .70 to .88), and family members (5 items, α ranged from .70 to .89; adapted from Padilla-Walker et al., 2018). The original measure was adapted slightly by asking participants to respond about the frequency of their prosocial behavior “since the start of the COVID-19 pandemic.” Responses were based on a 5-point Likert-type scale ranging from 1 (never) to 5 (very often). Items were very similar across targets save for slight modifications with reference to the individual target (e.g., “I helped people I didn’t know (my friends/my family), even if it was not easy for me,” “I went out of my way to cheer up people (my friends/my family) who seemed sad, even if I didn’t know them.”
Depression and Anxiety
Participants responded to items regarding their depression and anxiety “since the start of the COVID-19 pandemic” using 9-items from a measure of psychosocial functioning (Goldberg & Williams, 1988). Respondents rated how frequently various statements about mental health reflected their experiences using a Likert-type scale of 1 (never) to 5 (very often), with higher scores reflecting higher depression and anxiety. Five items were indicative of depression (α ranged from .77 to .86; e.g., “felt unhappy and depressed,” “been thinking of yourself as a worthless person”) and four of anxiety (α = .54–.75; e.g., “felt constantly under strain,” “lost much sleep over worry”).
Control Variables
Age was explored as a control variable but was not associated with any variables in the analyses, so it was dropped for parsimony. Control variables included biological sex (What was your biological sex at birth?), which was coded (0 = female, 1 = male), whether or not the participant was currently at a college or university (What is currently your main activity?) coded as (0 = not in school, 1 = in school), whether the participant felt they were a racial minority in their country (Do you consider yourself to belong to the majority or minority in your country based on ethnicity/race) coded as (0 = majority group, 1 = minority group), and income. Income was assessed by asking for the participant’s comfort in coping on their present income on a scale ranging from 1 (very difficult on present income) to 4 (living comfortably on present income).
Analysis Plan
We conducted all analyses using MPLUS (Muthén & Muthén, 1998–2017). Our first step was to assess factorial invariance by conducting confirmatory factor analysis (CFA) with multiple group analysis (by country) for each measure. If there was a significant Wald test (using the MODEL TEST command) when constraining all factor loadings to be equal across country, we carefully considered items for theoretical relevance and if warranted, we explored and ultimately dropped individual items if they were contributing to poor model fit or not loading above .40 for multiple countries. Adequate model fit for all models is when comparative fit index (CFI) >.90 and root mean square error of approximation (RMSEA) <.08 (Little, 2013).
After exploring factorial invariance, we averaged all indicators within constructs and used mean variables for the final model. To address our first and second research questions (our main model and moderation by country) we conducted path analysis to explore the relations between cultural values, prosocial behavior toward family, friends, and strangers, and participants’ depression and anxiety. Controls in all models included biological sex (0 = female, 1 = male), whether or not the participant was currently at a college or university (0 = not in school, 1 = in school), whether the participant felt they were a racial minority in their country (0 = majority group, 1 = minority group), and income. First, we explored direct paths between cultural values and depression and anxiety, and then we added prosocial behavior to the model. Again, we used multiple group analysis to determine whether the model varied by country. If constraining the full model to be equal across country resulted in a significant Wald value, then we explored paths one at a time and left them free to vary if constraining that path to be equal across any of the countries resulted in a decrease in model fit. This analysis included 26 paths tested for the main model and 20 paths for control variables. We then assessed indirect effects using 500 bootstrap samples and the IND command in MPLUS, with 95% confidence intervals.
Results
Factorial Measurement Invariance
There were three measures that displayed a decrease in model fit when all factor loadings were constrained to be equal by country, including the measure for horizontal individualism, prosocial behavior toward strangers, and depression (see supplementary materials for fit statistics of constrained and unconstrained models). For horizontal individualism, the item, “My personal identity, independent of others, is very important me” explained the decrease in model fit and loaded below a .40 for all countries except Lithuania, the Netherlands, Turkey, and the United States. Because this item was theoretically unique from the others, speaking specifically of independence, and statistically did not load for the majority of countries, we dropped the item and averaged the remaining three items, all of which could be constrained to be equal across countries without a significant decrease in model fit. For prosocial behavior toward strangers, the item, “I am kind to others, even if I don’t know them” explained the decrease in model fit and loaded below a .40 for all countries except Ireland and the United States. Because this item assessed kindness toward strangers, which may be interpreted quite differently as a function of culture as opposed to helping and volunteering represented in the other items, and because statistically it did not load for the majority of countries, we dropped this item and averaged the remaining four items, all of which could be constrained to be equal across countries without a significant decrease in model fit. For depression, the reverse-scored item “since the pandemic I have been able to face up to my problems” explained the decrease in model fit and loaded below .40 only for the Netherlands and the United States. Because this item seemed theoretically relevant, and statistically loaded well for all but two countries, we retained the item and constrained the remaining items to be equal across countries, which did not result in a decrease in model fit.
Descriptive Statistics
Table 1 includes means and standard deviations on all study variables. We also explored mean differences on variables as a function of country and it is of note that mean levels of horizontal individualism were highest in Italy; vertical individualism was highest in China; horizontal collectivism was highest in Argentina, Chile, and Spain; vertical collectivism was highest in Turkey; prosocial behavior toward strangers was highest in China and lowest in Finland; prosocial behavior toward friends was highest in Chile and Spain; prosocial behavior toward family was highest in Spain; depression was highest in Ireland and anxiety was highest in Chile and Spain.
Path Model of Cultural Values, Prosocial Behavior, and Depression and Anxiety
First we explored direct links between cultural values and depression and anxiety. Initial model fit was adequate, but constraining all paths to be equal across countries resulted in a significant decrease in model fit. Thus, we constrained each of the 8 direct effects (four cultural values to depression and anxiety) and 8 control variable direct effects (sex, school, minority, and income to depression and anxiety) to be equal one by one across all 14 countries. Only 6 of the 16 paths could be constrained to be equal across all countries (2 main effects, 4 control paths). The final direct model had adequate model fit—χ2(191) = 278.04, p < .001, CFI = .98, RMSEA = .03 [.026–.040], standardized root mean square residual (SRMR) = .03. We then explored the full model, adding the 12 paths from the four cultural values to the three types of prosocial behavior, and the 6 paths from prosocial behavior to anxiety and depression, as well as the 12 paths from controls to the three types of prosocial behavior. Constraining paths to be equal and using the Wald test suggested that 19 of the 30 paths could be constrained to be equal across all countries (11 main effects and 8 control paths). The final full model had adequate model fit—χ2(566) = 745.11, p < .001, CFI = .981, RMSEA = .028 [.022–.033], SRMR = .040. See Table 2 for beta values and for main effects that were constrained to be equal.
Path Model of Cultural Values, Prosocial Behavior, and Depression and Anxiety.
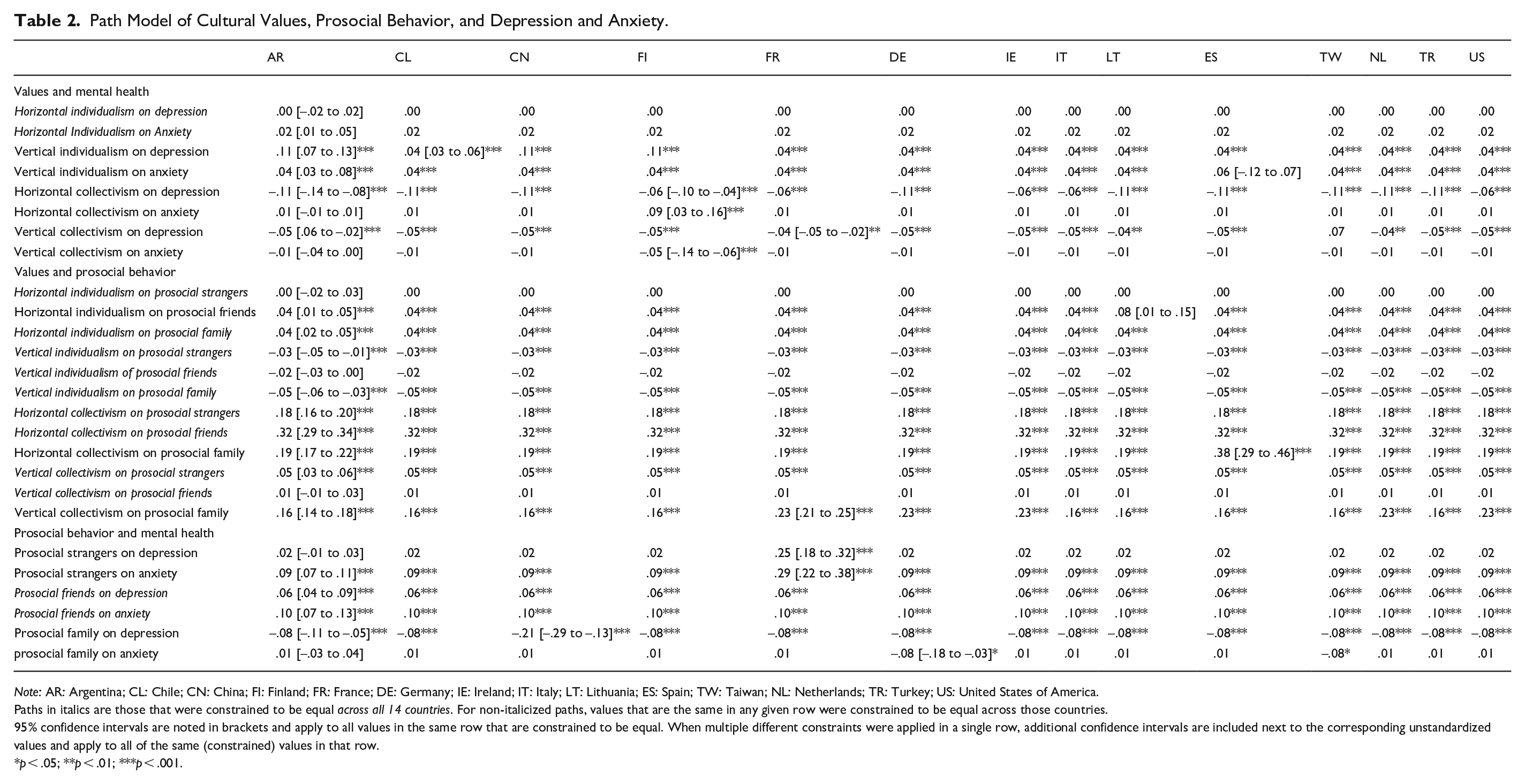
Note: AR: Argentina; CL: Chile; CN: China; FI: Finland; FR: France; DE: Germany; IE: Ireland; IT: Italy; LT: Lithuania; ES: Spain; TW: Taiwan; NL: Netherlands; TR: Turkey; US: United States of America.
Paths in italics are those that were constrained to be equal across all 14 countries. For non-italicized paths, values that are the same in any given row were constrained to be equal across those countries.
95% confidence intervals are noted in brackets and apply to all values in the same row that are constrained to be equal. When multiple different constraints were applied in a single row, additional confidence intervals are included next to the corresponding unstandardized values and apply to all of the same (constrained) values in that row.
p < .05; **p < .01; ***p < .001.
Direct Paths from Cultural Values to Depression and Anxiety
Horizonal individualism was not directly associated with either depression or anxiety in any country. In all countries vertical individualism was positively associated with depression, but this was stronger for Argentina, China, and Finland (b = .11, p < .001) compared with all the other countries, which were constrained to be equal to one another (b = .04, p < .001). Vertical individualism was also positively associated with anxiety in every country (b = .04, p < .001) except Spain (b = .06, p = .21). In all countries horizonal collectivism was negatively associated with depression, but this was weaker for Finland, France, Ireland, Italy, and the United States (b = –.06, p < .001) compared with all other countries, which were constrained to be equal to one another (b = –.11, p < .001). Horizonal collectivism was not associated with anxiety in any country (b = .01, p = .74), with the exception of Finland (b = .09, p < .001). Vertical collectivism was negatively associated with depression for all countries except Taiwan (b = .07, p = .08), but this was weaker for France, Lithuania, and the Netherlands (b = –.04, p < .01) compared with other countries, which were constrained to be equal to one another (b = –.05, p < .001). Vertical collectivism was not significantly associated with anxiety in any country (b = –.01, p = .21), with the exception of Finland (b = –.05, p < .001). See supplemental materials for in text results regarding links between control variables and depression and anxiety.
Paths from Cultural Values to Prosocial Behavior
Horizontal individualism was not associated with prosocial behavior toward strangers for any country, but was positively associated with prosocial behavior toward friends (b = .04, p < .001) and family (b = .04, p < .001) in all countries (with the exception of prosocial behavior toward friends in Lithuania (b = .08, p = .063). Vertical individualism was negatively associated with prosocial behavior toward strangers (b = –.03, p < .001) and family (b = –.046, p < .001) but not toward friends (b = –.02, p = .068) in all countries. Horizontal collectivism was associated positively with prosocial behavior toward strangers (b = .18, p < .001), friends (b = .32, p < .001), and family (b = .19, p < .001) in all countries, but the link with prosocial behavior toward family was particularly strong in Spain (b = .38, p < .001). Vertical collectivism was positively associated with prosocial behavior toward strangers (b = .05, p < .001) and was not significantly associated with prosocial behavior toward friends in any country (b = .01, p = .256). Vertical collectivism was positively associated with prosocial behavior toward family in France, Germany, Ireland, The Netherlands, and the United States, which were constrained to be equal to one another (b = .23, p < .001), and positively but less strongly associated with prosocial behavior toward family in all the other countries (b = .16, p < .001). See supplemental materials for in text results regarding links between control variables and prosocial behavior.
Paths from Prosocial Behavior to Depression and Anxiety
Prosocial behavior toward strangers was not significantly associated with depression (b = .02, p = .205) but was positively associated with anxiety (b = .09, p < .001) in all countries except France, where prosocial behavior toward strangers was positively associated with both depression (b = .25, p < .001) and anxiety (b = .29, p < .001). Prosocial behavior toward friends was positively associated with both depression (b = .06, p < .001) and anxiety (b = .10, p < .001) in all countries. Prosocial behavior toward family was negatively associated with depression (b = –.08, p < .001) in all countries, and more strongly in China (b = –.21, p < .001); and was not significantly associated with anxiety (b = .01, p = .744) except in Germany and Taiwan (b = –.08, p < .05), where prosocial behavior toward family was negatively associated with anxiety.
Indirect Effects of Cultural Values on Depression and Anxiety via Prosocial Behavior
In all countries, horizontal individualism was negatively associated with depression indirectly via prosocial behavior toward family (indirect effect = –.003 [–.005 to –.001], p = .007). Horizonal collectivism was positively associated with depression (indirect effect = .02 [.01−.029, p < .001) and anxiety (indirect effect = .03 [.02−.04], p < .010) indirectly via prosocial behavior toward friends. Horizonal collectivism was negatively associated with depression (indirect effect = –.02 [–.022 to –.010], p < .001) indirectly via prosocial behavior toward family. Vertical collectivism was negatively associated with depression indirectly via prosocial behavior toward family (indirect effect = –.01 [–.019 to –.009], p < .001).
Discussion
Recent research reveals a rise in mental health problems after the emergence of the COVID-19 pandemic (Evans et al., 2021; Kwong et al., 2020; Rossi et al., 2020), especially among emerging adults (Parola et al., 2020; Solomou & Constantinidou, 2020). Yet, the crisis situation also called for prosocial action, as many people were in need of physical, financial, or emotional help and the ubiquity of difficulty during such a crisis can often elicit prosocial action (Vollhardt, 2009). What is more, engaging in prosocial behavior might protect against mental health challenges (Qin et al., 2016; Vollhardt, 2009). Therefore, this study investigated how prosocial behavior toward strangers, friends, and family was related to symptoms of anxiety and depression during the COVID-19 pandemic. Furthermore, we examined the direct link of collectivistic and individualistic values to mental health, and the indirect link via emerging adults’ prosocial behavior, and whether associations differed across 14 different countries.
Prosocial Behavior and Mental Health
Regarding our main research question, we indeed found, and replicated across 14 countries, that emerging adults who engaged in more prosocial behavior toward their family members reported lower levels of depressive symptoms. This finding is in support of the notion that being able to show positive behaviors in the context of adversity is an indication of behavioral resilience, and as such protects against negative adjustment (Masten & Reed, 2002). In particular, during the COVID-19 pandemic when normative social interactions were seriously restricted, engaging in prosocial behavior toward family may have been important in fostering social support, which in turn helped emerging adults to cope with the situation and diminished depressive feelings (Qin et al., 2016). This finding is consistent with the results of a recent meta-analysis that also revealed a negative association between prosocial behavior and depressive symptoms for adolescents (Memmott-Elison et al., 2020), and our results extend this finding to the transition to adulthood. Remarkable is that the finding of a negative association with depressive symptoms only applied to prosocial behavior toward family, whereas previous research has shown that prosocial behavior toward strangers was linked to better mental health as well (e.g., Padilla-Walker et al., 2015; 2020). This may be explained by the context of the current study; due to restrictive measures during the pandemic, the opportunities for emerging adults to interact with strangers or friends, and thus to engage in prosocial behavior, were likely scarce. Our research highlights the crucial role of family during challenging times like the COVID-19 pandemic. While emerging adulthood generally is the period in which young people enlarge their social horizon and extend their network outside the family, during the pandemic social contacts outside the family inevitably have been limited. Therefore, providing help and support to family members likely facilitated emerging adults’ close relationships within the family and helped them cope with the consequences of the COVID-19 pandemic.
Also in line with findings of earlier research (Memmott-Elison et al., 2020; Padilla-Walker et al., 2020), we did not find a significant negative association between prosocial behavior and anxiety symptoms. However, as suggested by Padilla-Walker and colleagues (2020), it might be the case that the reported anxiety levels in a relatively well-adjusted sample like the current, are indicative of healthy anxiety or normative stress. Even more, when being exposed to a global pandemic like COVID-19 it might be more adaptive to experience some symptoms of anxiety than to experience no worries or stress at all. This may also explain our findings that prosocial behavior toward strangers was related to higher levels of anxiety, and prosocial behavior toward friends was related to higher symptoms of both anxiety and depression. By helping strangers or friends, individuals step outside their own bubble and are confronted with the unsettling consequences of the pandemic, which may cause worries about others and themselves, resulting in feelings of anxiety or depression.
Links between Cultural Values, Prosocial Behavior, and Mental Health
Regarding the role of cultural values, this study showed that individual differences in levels of individualism/collectivism values are indeed related to differences in helping behavior, and in turn to mental health. Even though the direct associations of cultural values to anxiety and depression were inconsistent, our results indicate that having a cultural orientation that facilitates young adults to engage in prosocial behavior toward family promotes mental health.
In line with our expectations, collectivism showed a consistent positive link to prosocial behavior in all of the 14 countries. This is in accordance with previous studies that show higher individual levels of collectivism (Lampridis & Papastylianou, 2017), or characteristics thereof (Armenta et al., 2011; Knight et al., 2018), to be positively related to prosocial tendencies. In our study, emerging adults who reported higher levels of horizontal collectivism showed higher levels of prosocial behavior toward strangers, friends, and family. Individuals who hold a horizontal collectivistic point of view see themselves as an interdependent part of the group, have a sense of duty toward their group, and feel that all members of the group are equal (Singelis et al., 1995), and as such have a high tendency to engage in prosocial actions toward all others in their society. Emerging adults who reported higher levels of vertical collectivism also showed higher levels of prosocial behavior toward strangers and family, but not toward friends. Both indirectly, via its link to prosocial behavior toward family, and directly, higher levels of vertical collectivism were related to lower levels of depressive symptoms. Like a horizontal collectivistic orientation, a vertical collectivistic orientation also implies that the individual sees oneself as aspect of a group and has a sense of duty, but inequality and differences between group members in status are accepted in this orientation. As such, emerging adults who report high levels of vertical collectivism may in particular direct their prosocial actions toward others in vertical relationships, such as older family members and strangers. This way, having a vertical collectivistic orientation facilitates young adults’ mental health via their higher tendency to engage in prosocial behavior toward older others (in this case, family members).
Although prosociality generally has been found to be lower in societies that are characterized by individualism than in societies characterized by collectivism (see Feygina & Henry, 2015), higher individual levels of individualism may still promote certain forms of prosocial behavior. Previous studies revealed that in individualistic cultures, people engage more often in informal and in spontaneous types of prosocial behavior, such as helping someone who is in distress or helping in case of an emergency (Kemmelmeier et al., 2006). This is consistent with our finding that emerging adults high in horizontal individualism reported higher levels of prosocial behavior toward friends and family during the COVID-19 pandemic, a time during which there likely were ample situations in which their friends and family were in distress or called for spontaneous help. This way, having high levels of horizontal individualism was indirectly protective against emerging adults’ mental health challenges, as horizontal individualism was negatively related to depressive symptoms via prosocial behavior toward family. Also consistent with previous findings is the result that emerging adults who reported higher levels of vertical individualism were less likely to engage in prosocial behavior. Vertical individualism is characterized by acceptance of inequality and by competition (Singelis et al., 1995), and these generally seem to suppress prosociality (e.g., Hudson et al., 2019; Lanzetta & Englis, 1989).
Comparisons across Countries
Our findings appeared robust across the 14 countries that were involved in this study. There were only few meaningful differences in associations as a function of country, and most of these were differences in strength of associations. This consistency across countries suggests that the roles that cultural values and prosocial behavior play in emerging adults’ mental health are highly similar in different societies. With regard to the role of cultural values in prosocial behavior, this is in line with previous research that revealed that even though there are differences in mean levels of prosocial behavior between individualistic and collectivistic countries, differences between individuals’ collectivistic and individualistic orientation still predict prosocial tendencies (e.g., Barrett et al., 2004; Knight et al., 2015). Moreover, although our participants came from different countries and cultures, they were all in the same developmental stage (i.e., emerging adulthood) and many of them were college students. During emerging adulthood, which is characterized by increasing independence, the similarities in individuals’ behavior due to the shared developmental stage may be larger than are the differences due to cultural variations (Jensen, 2008). Furthermore, due to the COVID-19 pandemic, the challenges that participants faced during the time of the data collection were highly similar across all countries, and this may also have resulted in increased similarity (for instance, great reliance on family due to containment strategies).
Conclusions and Limitations
Despite the large international sample, there were some study limitations. First, due to the correlational and cross-sectional design, we cannot determine the direction of effects observed in this study. While normative (and perhaps even slightly elevated) levels of anxiety may lead to prosocial behavior, it is unlikely that depression motivates prosocial behavior, but future research should also explore direction of effects by utilizing longitudinal designs to explore these associations. In addition, while our large sample size allowed us to detect small effects, it is worth noting that these effect sizes were often weak, and should therefore be interpreted with caution. Furthermore, the measures were all self-report questionnaires, which raises concerns regarding shared method variance and self-presentational demands. However, as the constructs we assessed mainly concerned internal processes (i.e., values, symptoms of anxiety, and depression), emerging adults themselves are likely the best informants. Yet, it is possible that participants’ overestimation of their prosocial actions caused some bias in our results. Although more objective data would be obtained when adding other-reported or observational measures, the measures have been validated and frequently used in previous studies. That being said, there was variability in the reliability of measures across countries, especially in relation to the measures of cultural values, which should therefore be interpreted with caution. Finally, although our sample included emerging adults from 14 regions of the world, the sample was relatively homogeneous with regard to education level and ethnicity, as 62% were college students and 79% considered themselves to belong to the majority group in their country. That being said, some of the variability in measurement in the current study may have been due to variability in minority status by country, and future research should carefully consider links between prosocial behavior and internalizing problems in minority groups. As previously noted, country is not indicative of culture, and ideally future studies would carefully draw on theory to study cultures within countries, and how specific and unique cultural values are associated with prosocial behavior and internalizing problems. For these reasons, we must be cautious about generalizing the current findings to more diverse populations of emerging adults.
Nonetheless, the present findings advance our understanding of the roles of broad cultural values and prosocial behavior in emerging adults’ mental health during the COVID-19 pandemic. Among emerging adults from 14 regions across the world, prosocial behavior toward family members appeared to be important during the COVID-19 pandemic. While in normative times emerging adults would venture out on their own, during the pandemic many were more or less tied to their home and family. Given that social participation is a key aspect of an individual’s ability to cope (Winsor & Skovdal, 2011), providing help and support to family members during this time likely strengthened relationships within the family and contributed to resilience, reflected in diminished depressive feelings. Interestingly, both higher levels of vertical and horizontal collectivism and higher levels of horizontal individualism seemed to protect against depressive symptoms, in part because both of these orientations promoted prosocial behavior toward family. However, feeling compelled to help others might also have led to extra stress and strain during the COVID-19 pandemic. In particular helping friends appeared to be related to higher levels of anxious and depressive feelings. Emerging adults who engaged more often in helping others outside their own family may have been more harshly confronted with the consequences of the pandemic, which may have given rise to feelings of anxiety and depression. The results of this study highlight the importance of distinguishing between different targets of prosocial behavior, as helping others potentially may protect against—but also may induce or exacerbate—mental health symptoms.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254221084098 – Supplemental material for Emerging adults’ cultural values, prosocial behaviors, and mental health in 14 countries during the COVID-19 pandemic
Supplemental material, sj-docx-1-jbd-10.1177_01650254221084098 for Emerging adults’ cultural values, prosocial behaviors, and mental health in 14 countries during the COVID-19 pandemic by Laura M. Padilla-Walker, Jolien Van der Graaff, Katey Workman, Gustavo Carlo, Susan Branje, Alexia Carrizales, Maria Gerbino, Zehra Gülseven, Skyler T. Hawk, Paula Luengo Kanacri, Belén Mesurado, Paula Samper-García, Yuh-Ling Shen, Laura K. Taylor, Jessica Trach, Maarten H. W. van Zalk and Rita Žukauskienė in International Journal of Behavioral Development
Footnotes
Acknowledgements
The authors thank the many collaborators who assisted in gathering data for this study, including Christian Berger, Pontificia Universidad Catolica de Chile; Gian Vittorio Caprara, Department of Psychology, Sapienza University of Rome, Italy; Claire F. Garandeau, INVEST Research Flagship University of Turku, Finland; Goda Kaniušonytė, Mykolas Romeris University, Lithuania; Asiye Kumru, Ozyegin University, Turkey; Anna Llorca-Mestre, University of Valencia; Vicenta Mestre-Escrivà, University of Valencia; Elisabeth Maloda-Vidal, University of Valencia; Concetta Pastorelli, Sapienza University of Rome, Italy; Maria Cristina Richaud, Universidad Austral, Argentina; and Anna T Rovella, National University of San Luis, Argentina.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.