
Abstract
Using COVID-19 as the backdrop, this article investigates different trade-offs in terms of pecuniary and time costs in drug development across different branches of medicine. South Asian countries as well as China have a rich history of practicing traditional and alternative medicine. However, modern biomedicine as well as traditional medicine comes with certain procedural requirements, which make immediate responses to a pandemic difficult. Clinical trials in biomedicine are costly, mostly in terms of time. On the other hand, a lack of these standards, as in the case of many alternative medicines, does not come with the promise of low-cost cures for the viral pandemic. Any modification of the standards in pharmaceutical testing has resulted in avoidable controversies at all stages of drug discovery, be it in research papers, or in clinical trials, or in the sale of actual medicine itself. Non-pharmaceutical intervention, with different economic impacts, becomes imperative.
Introduction
COVID-19 (or SARS-CoV-2 1 ) has been an unprecedented challenge to the medical community worldwide due to its novelty, rapid spread across a hyper-connected world, and extreme reactions across the globe, such as entire cities being locked down for months. While the chase to find a cure to the virus is on globally, two options with different costs for public health management emerged within a few months of the pandemic. The first is the medical route, which is an ongoing search for short-term cures in the form of effective drugs (Vellingiri et al., 2020) and the longer-term preventive of vaccines (Lurie et al., 2020b) and the second is the nonmedical option of lockdown of affected populations along with social distancing and other behavioral modifications to prevent the viral spread. 2 The purpose of this article is to argue that in retrospect of events that occurred between December 2019 to early 2021 (which we label the first phase of the pandemic), the core lesson of the COVID-19 pandemic is that the second options of nonmedical interventions, though economically very expensive, appear inevitable for future incidences of a similar nature.
COVID-19 Pandemic
As the COVID-19 saga unfolded in late 2019 in Wuhan, China and then, all across the world, some key facts emerged, which point to the difficulties of an immediate medical cure for treating symptoms of the virus. We summarize these below.
The Novelty of the Virus: in terms of its varied clinical presentation in the human population, symptomatic as well as asymptomatic cases emerged simultaneously and fatality rates have showed major variation across countries (Undela & Gudi, 2020) and age deciles (Sudharsanan et al., 2020). Many aspects of the disease are yet unfolding even in 2021, such as new strains of the virus. 3
Viral Pandemics Often Do Not Need Medical Intervention: The recent history of viral epidemics reveals that many of these occur as sharp outbreaks with limited areas of spread (e.g., the Ebola outbreak in various regions described in Table 1 4 ) or with the population developing herd immunity even without any medication (e.g., the case of H1N1 flu (swine flu) containment in Norway through natural immunity and vaccinations during 2010–2011 5 ). In the initial days of the pandemic, COVID-19 presented a lower mortality rate compared to some past viral outbreaks summarized in Table 1, 6 but it had a very high degree of infectiousness (the Ro number [reproduction number] of the disease in India is 1.11. 7 This number signifies the number of people an infected person can pass the disease to, on an average. 8 Horton (2020) notes that this was around 2.4 in the beginning of the outbreak in Wuhan, China). Some parts of the population (the vulnerable, viz. diabetics, old aged, and those with compromised immune systems (Horton, 2020; Huang, et al. 2020; Lian, et al. 2020) are affected disproportionately more than the rest of the population.
A Brief History of Viral Pandemics in the Twentieth Century
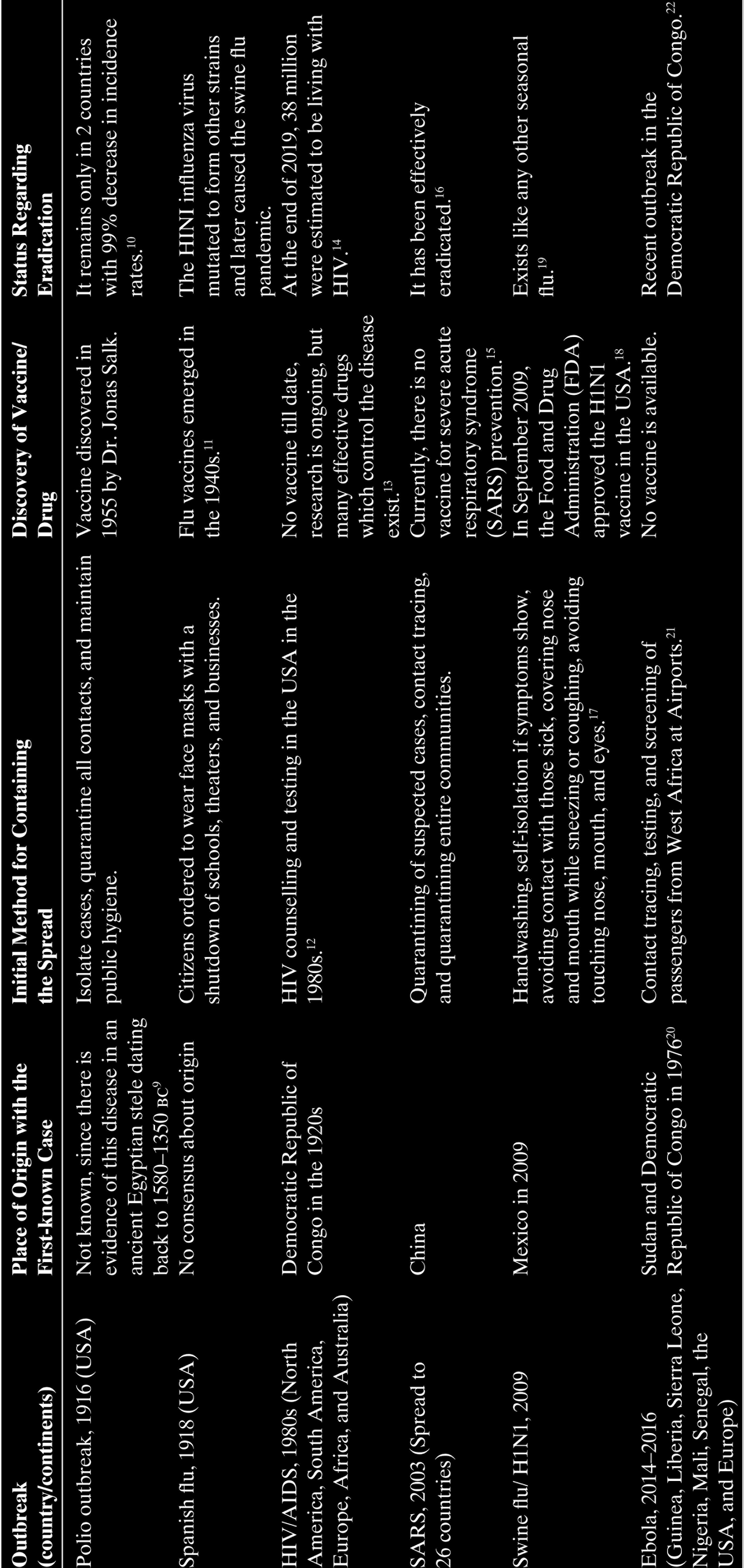
Finding a Cure Is Not the Same as Controlling the Disease Spread: some cities were controlling the spread of the disease using nonmedical interventions 23 —lockdowns and stringent imposition of public hygiene habits such as sanitization of public spaces, social distancing, hand-washing, and wearing masks.
The first two facts presented in Table 1 show the challenge to the medical community in discovering drug or vaccine-based cures for the pandemic, 24 but the last one is related to a non-medicinal alternative toward disease control, though it has its own economic costs. 25 The first set of challenges is present in all branches of medicine, be it biomedicine or traditional/ alternative medicine. 26 In fact, one of the driving reasons for writing this article is to show the nature of controversies around medical cures for COVID-19 that emerged in the first phase of the pandemic. These have arisen across all the medicinal systems: traditional ones with thousands of years of application but without a clear protocol to clinically test efficacy and side effects of drugs as well as biomedicine at the opposite end of the spectrum (Table 2).
While we draw on international experience for discussing the implications of the facts we presented above, most of our policy conclusions pertain to India. We do this for a number of reasons. For one, India has one of the most prolific generic drug manufacturers in the world, providing cheap medicines as alternatives to patented formulations to large parts of the world. 27 However, in terms of per capita expenditure on healthcare, the country has a minuscule current per capita expenditure of US$72.83 for the year 2018 in comparison with US$151.69 for Vietnam, let alone the much larger figure of US$10,623.85 for the USA. 28 With an overall population density of 455 29 people per square kilometer in 2018, and cities with densely populated areas (e.g., Dharavi, known as the biggest slum in Asia, has a population density of 354,167 30 people per square kilometer), the pandemic, despite a low fatality rate, had the potential to bring the weak medical infrastructure to its knees without stop-gap measures like lockdowns and contact tracing procedures, which we discuss in detail later. Honigsbaum (2020) notes that “India is the big unknown” as far as the denouement of the current pandemic is concerned.
However, there is a larger takeaway which relates to the economics of clinical trials (CTs) and cost of developing cures that need attention from public policy. This, in fact, goes beyond the immediate imperatives of the COVID-19 pandemic. This relates to the preparedness of medical communities to handle future pandemics similar to the current one, either due to excessively rigid safety standards (as is the case for biomedicine) or the vagueness regarding these standards (as is the case with alternative medicines). The majority of approved drugs (including vaccines) in modern biomedicine goes through a vastly complicated process of randomized double-blinded CTs, which have rigid protocols and large demands on time to market. As an instantaneous response to viral pandemics, the premise that a medicinal cure will be effectively available is not valid, unless compromises are made to these standards of efficacy. The latter tends to jeopardize the safety of consumption of these drugs or vaccines. Even if we broaden the search for medicinal cures to alternative medicines like Ayurveda, we find that it is unlikely that these will yield a timely cure for the virus. Though traditional medicine comes with the promise of making the symptoms mild or generate a generalized immune response, the overall effect of their use might not be more than a placebo, or there might be more serious side effects, 31 which are untested a priori through biomedicine standards. We discuss these issues along the following lines in this article: the second section discusses the overall trade-offs in drug development across systems of cure; the third section puts together all controversies across different branches of medicine and interprets them as some of resolution of the trade-offs; the fourth section contrasts the developments in biomedicine against traditional medicine in terms of COVID-19 cures; and the fifth section 5 concludes.
Trade-offs in Drug Development: Time, Money, and Regulatory Costs
As far as biomedicine is concerned, CTs have become the standard to prove efficacy of the medication as well as unintended side effects. While ClinicalTrials.gov is a database with studies from all 50 states of the USA and 216 countries worldwide,
32
most countries have their own registries to record CTs. India has a CT registry wherein it is compulsory by law to register all CTs conducted in India, starting from June 15, 2009, onward.
33
The ClinicalTrials.gov website maintained by the US National Library of medicine
34
outlines the activities that define CTs as follows:
In a clinical trial, participants receive specific interventions according to the research plan or protocol created by the investigators. These interventions may be medical products, such as drugs or devices; procedures; or changes to participants’ behaviour, such as diet. Clinical trials may compare a new medical approach to a standard one that is already available, to a placebo that contains no active ingredients, or to no intervention. Some clinical trials compare interventions that are already available to each other.
Pocock (1983) classifies CTs into four phases, which corresponds to the The United States Food and Drug Administration's (USFDA’s) classification. To summarize, phase 1 trials are used to rule out any toxicity and essentially used to determine the safety of the drug intervention; phase 2 trials are a preliminary clinical investigation for treatment effects in a small sample size of participants; phase 3 trials are a full-scale evaluation of treatment with a much larger sample size; and phase 4 trials involve post-marketing surveillance and can be conducted after the regulatory approval to monitor any side effects. Thus, the requirement of research funding increases with a drug intervention going through phases 1, 2, and 3 across all therapeutic areas, but the average costs of phase 3 and phase 4 trials are equivalent (Sertkaya et al., 2014).
Double-blinded randomized, placebo-controlled CTs are considered as a “Gold Standard” when it comes to proving the effectiveness of a drug (David & Khandhar, 2019; Misra, 2012). This variety of trials involves a random distribution of trial participants into an experimental group that receives the drug intervention and a control group that receives the placebo, with neither the trial researchers nor the participants having knowledge of whether they received the intervention or the placebo.
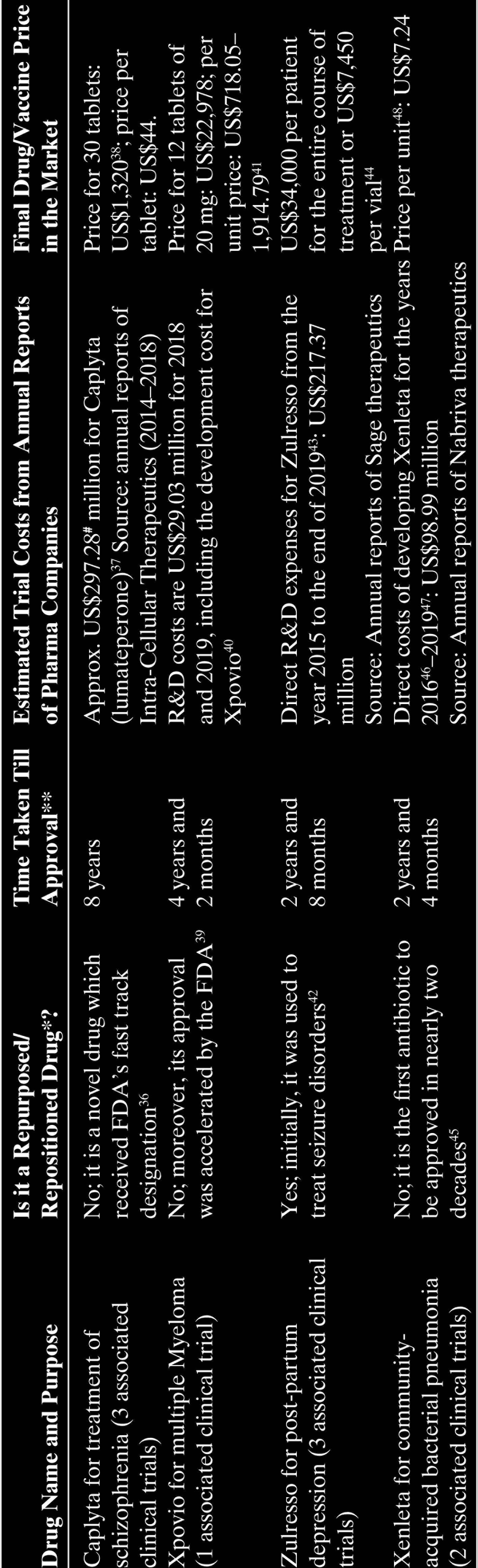
Table 2 gives a brief about some recent CTs and the costs and drugs that emanated from them. Note that many CTs do not result in a final drug, as the possibility of the trial failing is live even in the 3rd stage, as was the recent case with tocilizumab for COVID-19. 35 As per our calculations, the ranges for time taken to approve the relevant drug vary from close to 3–8 years.
Examples of Successful Clinical Trials for FDA-Approved Drugs in 2019
** Denotes time calculated from the start of the earliest clinical trial to month of FDA approval.
Note that most of the drugs that were out as part of COVID-19 treatment worldwide are repositioned drugs whose original purpose was to cure some other disease condition. Often previously known drugs which have either been approved or failed at some stage of development are tested for different health conditions other than their original intended purpose. This strategy of drug discovery is known to bring down both costs and time involved in drug development (Osakwe & Rizvi, 2016). While the timeline for a repurposed drug might be shorter (as we see from Table 2), the CT costs are typically higher than US$100 million. Therefore, it might seem as a very costly option for finding cures in times of pandemics.
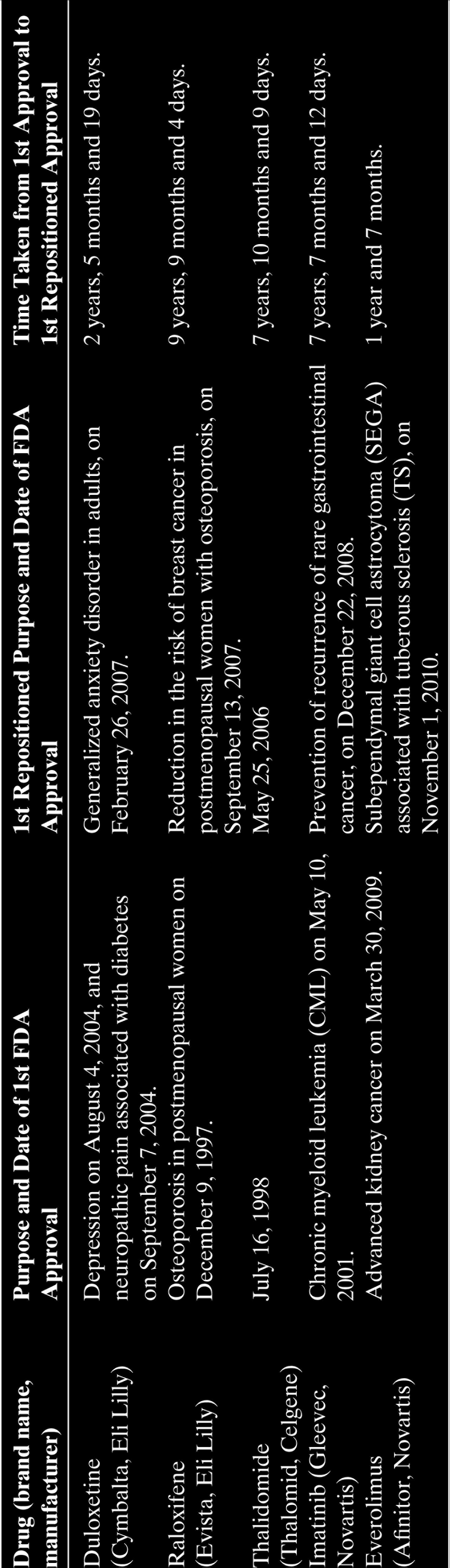
CTs are required not only for discovering new drugs (such as daratumumab, Laubach et al. [2014] or valbenazine, Müller [2015]) but also for repositioning drugs, which have been around for a long period of time, such as remdesivir, itolizumab, and Hydroxychloroquine (HCQ), for treating COVID-19. The moment this route is taken to prove efficacy of treatment, we are beholden to the standards set by the institution of CT itself. 49 The expected timelines for such CTs should realistically be kept at something more than a year, as we see from Table 3 for repurposed drug CT timelines.
Examples of Successful Repositioned Drugs with Time Taken to Reposition
In fact, there are several critiques of the randomized controlled CT, not only from an ethical point of view (Szajewska, 2018) point out the lack of external validity of CTs; that is, the results cannot be extrapolated to other populations, and this is particularly problematic when trials are conducted on infants) but also the very conduct of the CT, which is later taken as a standard of proof of efficacy (i.e., during this pandemic, it had been difficult for doctors to withhold treatment for serious COVID-19 patients on humanitarian grounds 50 ). Despite their initial criticism (Matthews, 1995), CTs have now become the norm and their largest cost comes in terms of the budget for clinical procedure costs, administrative staff costs, site retention costs, site monitoring costs, and central laboratory costs (Sertkaya et al., 2014). Given that conducting a CT does not guarantee the discovery of a drug (Fogel, 2018), the large uncertainty in terms of time as well as the cost of conducting (Ibrahim et al., 2015; Logan & Scott, 1996), it is understandably very high at a time like the current pandemic. Modern biomedicine has become captive to its own set standards of efficacy (through controversies around CTs), and COVID-19 has revealed many gaps in what a desirable standard itself is.
Historically, vaccine development has been a time-consuming process with many bottlenecks (Drury et al., 2019). Taking a step back, historically, vaccine development has had a very long timeline. Though the first case of poliovirus was recorded in 1789, the severe manifestation of the disease, which led to epidemics at regular intervals in the USA and many European countries, occurred in the early twentieth century. Though many attempts were made to produce a vaccine in the interim period, it was Jonas Salk, using the virus grown on monkey kidney cells, who eventually succeeded in 1954. After placebo-controlled trials, the USA adopted the vaccine in 1955 (Baicus, 2012).
Though a lot of procedures were streamlined to meet the state of emergency in the first phase of the pandemic, trials, ideally, should not compromise on safety protocols without causing damage to the reputation of vaccines. Lurie et al. (2020a) reports that in the US, a poll of 1056 individuals revealed that only 49% were planning to receive a COVID-19 vaccine, 31% are uncertain, and 20% refuse to receive a vaccine due to safety concerns. Thus, the authors suggest a more transparent approach with all protocols set by drug regulatory authorities to be followed stringently so as to keep the public well-informed, since large-scale phase 3 trials require a favorable opinion and information about the safety of the potential vaccine. Since vaccines are also administered to healthy individuals, safety studies conducted in phase 1 and 2 trials gain utmost significance.
Arora and Das (2020) note that out of a total of 108 ongoing CTs in the first phase of the pandemic, 100 were in the preclinical stage and 8 in phase 1 or 2 CTs. Since then, newspaper reports have indicated that 125 potential COVID-19 vaccines were at the preclinical phase, 51 15 were in phase 1, 10 at phase 2 trials, and 4 were at phase 3 trials. We get an idea of the standard costs for conducting CTs from the statement of the Principal Scientific Adviser to the Government of India, Professor K Vijay Raghavan. In a press briefing, he pointed out that the normal timeline to develop a vaccine is 10–15 years with costs around US$200–300 million. 52 However, during this pandemic, the desired timeline was 1 year which, according to him, would raise the costs substantially, that is, costs of fast tracking the regulatory processes, expanding manufacturing capacity, and building on distribution systems.
Diluting these time costs is not feasible due to the nature of the medicine itself: while the side effects of the drug in one particular disease condition might be of a certain kind, those in another disease might be drastically different even for the same patient; for instance, hydroxychloroquine, which is an FDA-approved drug to treat malaria, lupus, and rheumatoid arthritis was initially used to treat serious COVID-19 patients, but now, it has been discontinued because of serious cardiac side effects. 53 Remdesivir, on the other hand, was a repurposed drug to treat coronaviruses (Hendaus, 2020) in the initial phase of the pandemic, and unlike hydroxychloroquine, it did not perform well for hepatitis C 54 and Ebola (Eastman et al., 2020).
Other than time costs, the early phase of the pandemic brought out another issue: that of exorbitant prices of designated drugs for treating COVID-19 symptoms. Again, consider remdesivir. Previously investigated for Ebola treatment without significantly positive results, it had shown promising results in phase 3 CTs, 55 as part of treatment for serious COVID-19 patients. In India, it was approved for emergency use, and Indian companies like Cipla and Hetero Labs received approvals to sell and manufacture the same. 56 The shortage of this drug in India led to it being sold on the black market at exorbitant prices. 57 The Department of Pharmaceuticals asked manufacturers to increase production. 58
Even though this drug was proven to only reduce the recovery time of COVID-19 patients 65% of the time, in the absence of other options, doctors opted to prescribe it more often than not. Even the US-based company, Gilead Sciences, which is the original maker of drug remdesivir, was in news for charging sky-rocketing prices in developed countries. It fixed a price of US$2,340 per patient in wealthy nations with an even steeper price for US patients with insurance. 59 Gilead has the reputation of charging high prices for its breakthrough drugs. 60 Gilead’s pricing incentives, which are aligned with making profits for its shareholders, had raised concerns among US democrats in the early days of the pandemic. 61
Medicines apart, the cost of testing for COVID-19 was not without controversies, with significant geographical differences in prices within the same country (as in the case of India). 62 The cost of testing and delays in report availability claimed many a victim. 63 Over the span of the pandemic, since the last days of 2019, this issue of pricing medicinal cures, be it for testing or drugs or vaccines 64 (which were being considered almost a year after the pandemic broke), has been a significant concern for public health authorities. The fact that affordability of designated medicines/vaccines meant regulatory caps and the onslaught of the pandemic meant reduced attention to other medical conditions and related expenditure, an undesirable spillover effect of increased drug prices for conditions other than COVID-19 for profit-seeking pharmaceutical firms, was inevitable. 65 For a pandemic which comes with an informational blitzkrieg, 66 a casualty is neglected disease conditions other than COVID-19. 67 It is imperative for health policy-makers in the future to deal with not only pricing of medicines related to the pandemic but also management of neglected disease conditions.
Our discussion above underscores the fact that modern medical solutions for viral pandemics require a framework that is more flexible and yet reliable than what we have at present in most countries. Some simple procedures, such as repositioning an existing drug for usage in a new viral condition, do not allow any shortcuts, such as testing on smaller samples, to decide the effects of the drugs. This is the essential trade-off when it comes to establishing biomedicinal cures: timely approval of a drug versus its appropriate testing through well-designed randomized CTs.
As a standard, randomized double-blinded CTs are not only expensive (Dimasi et al., 201668,69; Sertkaya et al., 2014), but their standards are inflexible and time-consuming oftentimes resulting in failures. However, as there are no alternative benchmarks of drug efficacy, CTs have become an inescapable norm worldwide for drug development (Poongothai et al., 2014). Any attempt to modify the CT standards arbitrarily results in controversies, as has been the case for most of the medicinal cures for the current pandemic. We discuss this next section.
Controversies Around COVID-19 Medicinal Treatments Across Medicinal Branches
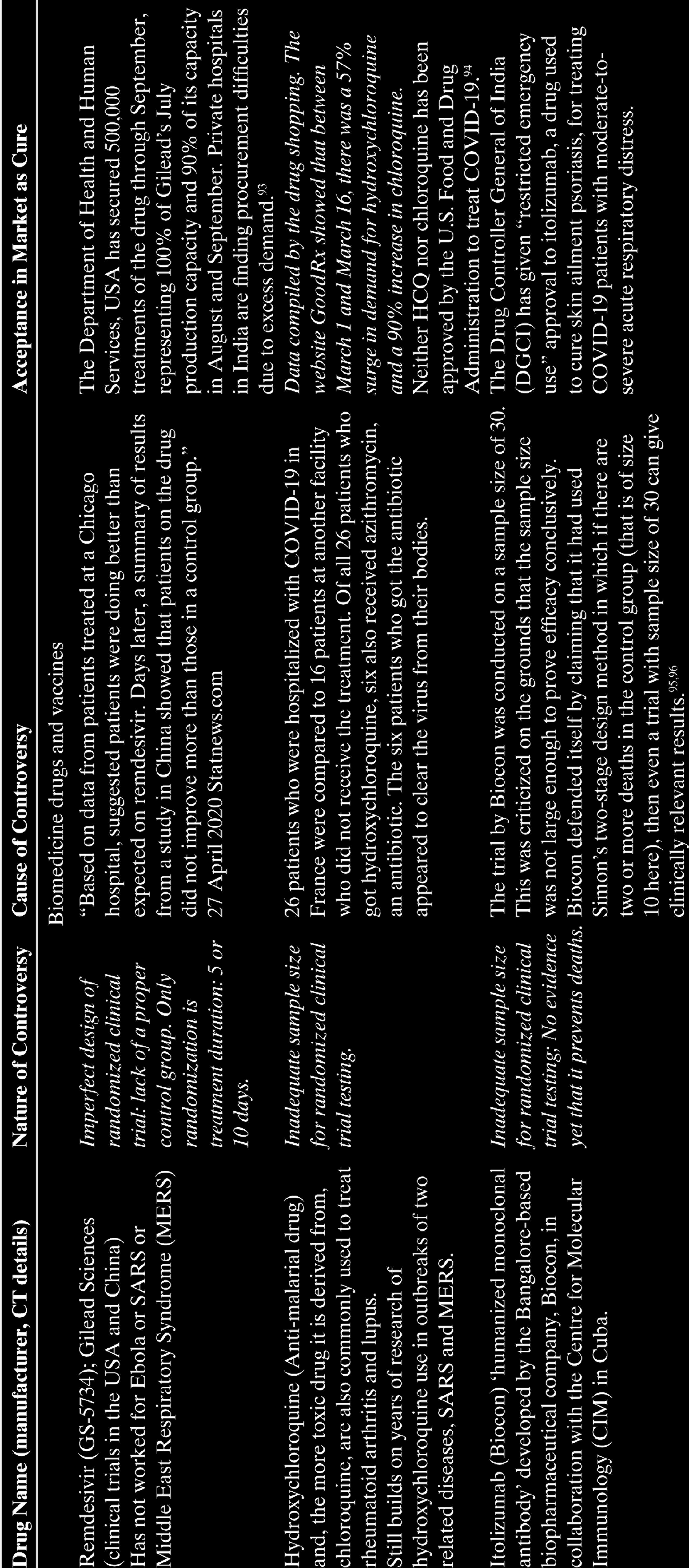
Table 4 (on page 349) elaborates some of the controversies that arose worldwide regarding medicinal treatments for COVID-19 in the early phase of the pandemic (late 2019 to mid-2020). However, we note that these controversies were not limited to biomedicine alone. Table 4 comprehensively puts together all these instances of lack of clarity and confusion that arose in all branches of medicine. In the light of these controversies, CTs appear to be more of a necessary evil. For the biomedicine drugs and vaccine, it was the design of the trial itself, whereas for other branches of medicine, the controversies revolved around a lack of these trials or other similarly accepted proof of efficacy of treatment.
It was in 2001 that the Indian drug manufacturer Cipla offered a fixed dose combination of three drugs (stavudine, lamivudine, and nevirapine) to combat the AIDS pandemic in Africa at a price of US$1 per day per patient
70
or US$350 per year as against the US$10,000–15,000 set by pharmaceutical giants like Bristol Myers Squibb, Merck, Roche, GlaxoSmithKline (GSK) and Boehringer Ingelheim.
71
It is also noteworthy that India has the largest vaccine manufacturer in the world: The Serum Institute of India Private Limited, Pune produces close to 70% of all vaccines in the world (see
In this context, we need to discuss alternative mechanisms of cure which are provided by traditional and complimentary alternative medicines (TM/CAM). Alternative medicines have a large faith-based following 72 (see Pandey et al., 2013; World Health Organization Report, 2003). Reports from China, where the viral outbreak was first noted in December 2019, indicated successful usage of traditional Chinese medicine (TCM in short) for treating patients in Wuhan, the center of the pandemic; for instance, Ni et al. (2020) document the usage of a combination of Western medicine and Chinese traditional patent medicine Shuang-Huang-Lian oral liquid (SHL) for three cases in a single family in Wuhan, though it mentions the necessity of “further clinical trials” for the traditional medicine. Medical systems such as Ayurveda, Siddha, and Unani have been around in the South Asian subcontinent, particularly in India, for thousands of years and have in their vast cornucopia a large basket of formulations that can enhance immunity. The expectations of traditional medicinal systems to provide cures for COVID-19 in India were apparent from the discussions in the public space in the early phase of the pandemic, just as TCM was for China. 73
The nature of medicines and the manner in which these systems approach disease conditions are in contrast with biomedicine. As pointed out by practitioners in an interview to The Hindu, 74 Ayurveda does not view all human beings as similar to each other and, hence, has multiple cures for the same disease to be prescribed on a person-to-person basis. As far as the pandemic was playing out in early 2020, Ayurveda in India was being used as an immunity booster and a palliative for reducing severe symptoms. 75 On the other hand, modern medicine considers a cure to work similarly on most human beings and, hence, conducts CTs. The results of CTs are assessed using statistical analysis, which is dependent upon the sample size of patients who have been part of the trial. This gives rise to the oft-asked question: Can these drugs be held to the modern standard of CTs to prove efficacy of cure?
Instead of asking the difficult question of equivalence of proof for TM/CAM, practitioners should provide realistic answers to what these medicines can achieve in the context of a pandemic like COVID-19? In our understanding, the functional approach of these formulations is similar to that of repositioned drugs from biomedicine, such as itolizumab (repurposed from the original intention of reducing psoriasis symptoms). Most of the promising herbs proposed for CTs by the Ministry of Ministry of Ayurveda, Yoga & Naturopathy, Unani, Siddha and Homoeopathy (AYUSH), Government of India, such as Ashwagandha (Withania somnifera) have been used for thousands of years to control immune system responses and to strengthen immunity. The cytokine storm that was seen as an aggravated COVID-19 symptom resulted from immune system overreactions (Catanzaro et al., 2020; Felsenstein et al., 2020). If immune system balancing is at stake, then TM/CAM can be an option to strengthen immunity (coupled with breathing exercises from yoga and other traditional systems) bypassing the necessity of CTs. Of course, this means that marketing drugs like Coronil, with the specific claim that it was a “100%” COVID-19 cure would be impossible (this relates to the Coronil controversy of Patanjali, as described in Table 4).
While the time cost of prescribing immunity boosters is lower, there is nonetheless a different set of costs, which are also time-consuming. Understanding the presentation of the disease in terms of the logic of traditional systems like Ayurveda is itself an uphill task. Rammanohar et al. (2020) have elaborated on this point and have attempted to characterize symptoms of COVID-19 in Ayurvedic terms (“vātakapha dominant sannipātajvara of āgantu origin with pittānubandha” which loosely translates to delirious fever (sannipātajvara) attributable to the fire element (āgantu origin) in the body with disbalance of the basic humors related to wind and phlegm (vātakapha) along with biliary conditions (pittānubandha) using biomedical case reports from 14 patients under treatment at a hospital in Gurugram, National Capital Region (NCR). The combination of allopathic treatment with Ayurvedic formulations, as was the case for the Ni et al. (2020) study for TCM, first requires this collaboration between different streams of medicine to share data, so that the clinical profiling of the disease is effectively done within the respective medicine domain. As mentioned earlier, Gupta et al. (2020)’s proposition of using curcumin, “the predominant curcumoid in turmeric,” is based on its influences on multiple signaling pathways. They claim that it has “been found to possess anti-inflammatory, anti-oxidant, antimicrobial, hypo-glycemic, wound healing, chemo-preventive, chemo-sensitizing and radio-sensitizing properties,” and its bioavailability can be enhanced using “newer technologies such as adjuvant, nanoparticles, liposomes, micelles and phospholipid complexes…in the process of drug development.” Such a claim rests on a clear understanding of the signaling pathways affected by SARS-CoV-2 in Ayurvedic terms and, therefore, an evaluation of the appropriate herbs for alleviating symptoms. Similarly, the claim of Tillu et al. (2020) emphasizing the therapeutic potential of Ayurvedic formulations to curb the increase in the number of coronavirus patients and relieve the pressure on the health system requires a precise Ayurvedic understanding of the disease. The challenge is that the disease presentation was significantly different from the symptomatic cases from the asymptomatic cases, as we mentioned earlier. Though the symptomatic cases appeared as distressed patients, most of the spread of the disease happened through asymptomatic cases (Ali et al., 2020; Avoi et al., 2020). Controlling the pandemic requires medical systems to assess and treat not only the symptomatic cases, but the asymptomatic ones as well. Hence, generalizing the clinical condition of the disease, which has presented a variety of symptomatic 76 as well as asymptomatic responses, requires collaborative ventures across systems of medicine for innovative responses. Among the set of controversies, we mention Tamil Nadu’s claim of successful deployment of Siddha formulations without any backing from CTs. Among the few published studies on Siddha treatment, Kiran et al. (2020) found that in in silico molecular docking studies for 37 compounds, 9 showed effectiveness in terms of their ability to bind to the SARS-COV-2 spike protein. Their proposal, which tests the official Siddha formulation of Kabasura Kudineer and the “novel herbal formulation JACOM,” is a combination they term “SNACK-V.” However, this study has been conducted through computer-based simulations using the Cresset Flare software and is not the equivalent of a CT on human volunteers.
Thousands of years of historical evidence of effective management of immune system responses, as Ayurveda or Siddha promise, should be kept as a line of defense, but prescribing formulations from these systems of cure also require a kind of standardization: a clear understanding of the disease symptoms in terms of the disciplinary bounds of these branches of medicine. This comes with a different kind of trade-off: faith-based prescription of TM/CAM formulations vs. time-consuming detailed collaborations between biomedicine and alternative medicine to understand the clinical presentation of the disease. The former faith-based approach explains the kind of controversies that TM/CAM formulations have witnessed during the pandemic, as detailed in Table 4. Avoiding these controversies requires these branches of medicine to be able to present lucidly to the medical community as well as the policy-makers what is to be rationally expected from their formulations in terms of symptomatic relief from COVID-19 distress for different age deciles of the population. This requires empirical evidence in terms of patient profiling: whom the disease is affecting and to what degree. As the much of the information about the nature of COVID-19 symptoms has come from biomedicine hospitals, a serious effort to understand it through the lens of alternative medicines requires this collaboration cost. 77 A first-best scenario would be the CT route. However, as we discussed, it comes at a much larger cost of time and money.
Other than these controversies, another incident which came to light in early June of 2020 was the retraction of studies on the effectiveness of anti-malarial drugs such as chloroquine and hydro-chloroquine administered to symptomatic COVID-19 patients by reputed medical journals such as the Lancet and the New England Journal of Medicine (NEJM). The Lancet study claimed that on the basis of data from 671 hospitals in 6 continents, the use of these drugs caused higher mortality in coronavirus patients. 78 This question on safety had caused the WHO to momentarily stop the CTs undergoing on these drugs (Sengupta, 2020), but soon enough, questions were raised on the reliability of the data, and the authors could not verify the data. Hence, the study was retracted. Similarly, the article in NEJM found that certain blood pressure medications were safe to use on coronavirus patients. Again, the study did not hold after data could not be verified. These incidents are indicative of how hastening the peer review process followed by journals can lead to unfavorable outcomes and a loss of reputation for both the authors as well as the journals.
Biomedicine Versus Traditional Medicine as Treatments for Coronavirus
A perusal of these controversies indicates that during times of desperation for finding a cure, the difference between faith-based medicines and clinically tested biomedicine is often obscure. Nothing exemplifies this better than the demand data that we present in Table 4 for biomedicines, which have not fully passed the stringent efficacy proofs of CTs or are products of imperfectly designed trials, such that the standard of proof itself is weak. This is most starkly shown in the case of the laboratory-grown monoclonal antibodies, tocilizumab and itolizumab. The COVACTA trial showed no significant reduction in death rates for tocilizumab relative to a placebo. By July 2020, Hoffmann-La Roche (the trial sponsor) announced that the results of phase 3 of the randomized trial revealed no significant improvement for pneumonia conditions induced by the novel coronavirus in comparison to a placebo. While this transparency in reporting failure is to be lauded (the risk is borne by the pharmaceutical firm for this experimentation), it brings us back to our contention that new or old repurposed drugs have to pass the stringent test that these CTs make them face. That a timely response for the pandemic is unlikely for such ponderous checks on effectiveness and safety should be the main lesson for the general public who are reluctant to modify lifestyles to adjust to pandemic times. 79 The Indian Council for Medical Research (ICMR) noted the same for itolizumab. 80 Despite this, there is excess demand for these formulations in private hospitals in India, as we note in Table 4.
The fact that trial standards were not being strictly implemented for biomedicines opens up the obvious counter: why not use medicines from traditional systems whose consumption has to date not been subject to CTs. Traditional medicine in India has always had lax regulations with a blind eye turned toward strict implementation. The manner in which research in Ayurvedic herbs is conducted has limited itself to respecting modern publication standards, leaving content largely unchanged (Saha & Vasuprada, 2020a). Modern medicine in India is monitored by the Drug Controller General of India (DCGI) and has a strong standard setting body, that is, the Central Drugs Standard Control Organisation (CDSCO) which sets mandatory standards for sale of drugs as well as medical devices. 81 On the other hand, traditional medicine systems are governed by the Ministry of AYUSH alone and are not as strictly monitored, with only two slightly outdated key laws that govern the sector. 82
However, to what extent can a public healthcare system function in a pandemic of the scale of COVID-19 purely on the strength of traditional medicinal systems. For one, we point out that collaborations across branches of medicine are essential for these alternative systems of medicine to understand the disease presentation in their own terms, which has its own costs. Second, and more critically, once the condition is understood in terms of the discipline, how safe is it to prescribe medicines off-the-shelf of the large pharmacopeia of traditional systems, be it Ayurveda or Chinese medicine? Are there no side effects of these medicines? Traditional medicinal systems come with what can be termed “historical capital” (Saha & Vasuprada, 2020b), which leads to a general acceptance of formulations from these systems without formal testing. Much of this is also beholden to the historical pharmaceutical methods in these systems where the doctor was also the pharmacist. Faith in the healer translated into faith in natural formulations that were personalized and prescribed without a prescription. The latter is a mechanism needed to convey the message of the doctor to the pharmacist, who is not in communication directly, as is the benchmark for biomedicine. Unlabeled medicine bottles with traditional medicines are accepted by many consumers in South Asia, without questioning potential harm or a mere placebo effect of the formulation (Saha & Vasuprada, 2020b).
Edzart Ernst’s British Medical Journal (BMJ) blog article 83 titled “The ‘natural’ equals safe fallacy” carefully points out the inconsistencies in this argument. Having held the position of the world’s first professor of alternative medicine 84 (see Nature, 2011), Ernst has always argued for “critical assessment” of traditional systems and his voice of warning in Nature (May 6, 2020) about Chinese Traditional Medicine (TCM) “We are dealing with a serious infection which requires effective treatments. For TCM, there is no good evidence, and therefore its use is not just unjustified, but dangerous” has to be heeded carefully. It cannot be that no formal testing of these medicines is good news, and one can march with historical and individual case evidence as a first line of defense for any pandemic. Consider the research article by Tan et al. (2019) which concludes “TCM injections pose graver risks to the paediatric population than the adult population. To achieve optimal benefits and minimal risk to children treated with TCM injections, we suggest re-evaluating the effectiveness and safety, monitoring the risks, and promoting rational use of TCM injections in Chinese children.” This is clearly what Ernst has pointed out in his blog article of 2012. In this context, the Coronil controversy of the Patanjali pharmacy is especially worrisome. Ayurveda enjoys a certain loyal clientele who may decide to take formulations like “Coronil” and wait for their symptoms to improve while avoiding hospitalization. By the time the patient gets admitted to the hospital with aggravated symptoms, it may be too late to save his or her life.
Large-scale adoption of alternative medicine requires it to face the same efficacy standards as modern medicine. Some moves have been made during this pandemic for herbs and medications from traditional systems of medicine such as Ayurveda, Siddha, Homeopathy, TCM to be part of CTs. Though the AYUSH ministry has released guidelines on the conduct of CTs 85 in Ayurveda which suggest an integration of modern-day practices with traditional practices to arrive at evidence-based practice of traditional medicine, these guidelines are not binding on traditional medicine drug manufacturers for a variety of reasons pointed out by Singh et al. (2014). The authors argue that since herbal formulations are mostly unpatentable, the costs of CTs may not be recoverable, and also, there are inherent challenges in the conduct of CTs on herbal medicines because of the incomparable nature of herbal extracts or even different batches of the same extract. Often, the timing of collection of raw material as well as the place of collection may cause differences in different batches of the same extract. Thus, CTs have to address these challenges. The CT registry of India has seen the registration of a plethora of traditional medicine COVID-19 trials but of low quality. 86 Most of these CTs that are non-randomized and single arm do not yield the comparative results that a double-blinded randomized trial does. Hence, the results obtained from these studies will not conclusively establish efficacy.
Modern testing procedures for effectiveness of medicines and approval for drugs have been designed with the highest safety protocols in mind. Attempts to quicken the drug development process have only led to different controversies. However, if anything has been exposed by the coronavirus pandemic, it is the fact that modern medicine itself is captive to these standards which are time-consuming and has no quick response shortcuts for fast disease spreads in a globalized world. These controversies are a reminder that procedures and protocols to be followed in a pandemic are yet to be defined. It is imperative for medical communities worldwide and national governments to collaborate across medicinal disciplines to work out special norms of efficacy during times of fast spreading pandemics. Solutions which take too much time are of no use, but untested cures with potential side effects are a disaster. More than 9 months to the start of the pandemic, Russia approvedtwo drugs (Coronavir and Avifavir), both based on favipiravir, developed in Japan for viral treatments, as well as a vaccine 87 without conducting phase 3 trials on humans 88 (around September 2020). The second half of 2020 and the beginning of 2021 saw a rush to immunize the public, starting with Russia. 89 The UK, the US, as well as India were a part of the global rush toward immunization with vaccines with troubled histories of testing efficacy and CT design. 90 History will judge how effective these vaccines were and the overall preparedness of public health systems across the world to cope with COVID-19. In the concluding section, we underscore the central lesson from the early days of the pandemic: irrespective of the medical solution, nonmedical interventions (some of which are as innocuous as hand-washing, wearing masks and social distancing) cannot be dispensed with.
Discussion and Conclusion
The first phase of the pandemic was marked by events unprecedented in peaceful times in the pretext of nonmedical solutions to control the pandemic, such as the lockdown of cities worldwide (as mentioned earlier) to prevent the viral spread. These were economically extremely costly for all countries, making public health officials impatient for a medicinal cure for the pandemic. Lea (2020) examines the costs of the lockdown to the UK economy using figures on retail sales and other indicators such as government borrowings and de Oliveira (2020) studies economic costs due to the lockdown in the southern-most state in Brazil, while Dutta and Hussain (2020) conduct a cost-benefit analysis of the lockdown implemented in India and find that there have been negative net benefits revealing the costs to be predictably very high. Another way to contain the spread of the virus and to break the chain of infection has been contact tracing. As pointed out by Kretzschmar et al. (2020), if lockdowns have to be eased, then effective contact tracing is very important. Again, countries have used different digital tracking methods 91 to trace people who came in contact with an infected person. However, given the nature of the trade-offs in the drug discovery process, we contend that a medical solution to the pandemic is likely to take its own time, and each country has to experiment with other methods such as social distancing awareness campaigns, face mask and hand-washing campaigns, and even the most drastic economically devastating step of city or country-wide lockdowns.
Medical communities across the world struggled through this pandemic with the burden of efficacy standard or lack of it for helping scores of people affected by the fast-spreading virus. Some experimental techniques, such as plasma therapy were also employed. Under this treatment, the recovered COVID-19 patients donated blood which contained antibodies to COVID-19. The plasma from this blood was given to serious patients through an injection or drip. As on date, the evidence regarding this therapy is inconclusive. 92 By-passing standards for effectiveness or potential side effects is not a solution for any branch of medicine, and the necessary time for devising medicinal cures, be it bio-medicine or appropriately tested traditional medicine, must be accorded by public health officials. In the meantime, nonmedical interventions such as contact tracing, increased testing, awareness campaigns for social distancing, handwashing, and wearing masks have to bear the burden of containment of infection, if not the economically more expensive strategy of area-wide lockdowns.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix
Potential Cure and Related Controversy and Market Acceptance
| Drug Name (manufacturer, CT details) | Nature of Controversy | Cause of Controversy | Acceptance in Market as Cure |
| Biomedicine drugs and vaccines | |||
| Remdesivir (GS-5734); Gilead Sciences (clinical trials in the USA and China) Has not worked for Ebola or SARS or Middle East Respiratory Syndrome (MERS) |
Imperfect design of randomized clinical trial: lack of a proper control group. Only randomization is treatment duration: 5 or 10 days. | “Based on data from patients treated at a Chicago hospital, suggested patients were doing better than expected on remdesivir. Days later, a summary of results from a study in China showed that patients on the drug did not improve more than those in a control group.” 27 April 2020 Statnews.com |
The Department of Health and Human Services, USA has secured 500,000 treatments of the drug through September, representing 100% of Gilead’s July production capacity and 90% of its capacity in August and September. Private hospitals in India are finding procurement difficulties due to excess demand. 93 |
| Hydroxychloroquine (Anti-malarial drug) and, the more toxic drug it is derived from, chloroquine, are also commonly used to treat rheumatoid arthritis and lupus. Still builds on years of research of hydroxychloroquine use in outbreaks of two related diseases, SARS and MERS. |
Inadequate sample size for randomized clinical trial testing. | 26 patients who were hospitalized with COVID-19 in France were compared to 16 patients at another facility who did not receive the treatment. Of all 26 patients who got hydroxychloroquine, six also received azithromycin, an antibiotic. The six patients who got the antibiotic appeared to clear the virus from their bodies. | Data compiled by the drug shopping. The website GoodRx showed that between March 1 and March 16, there was a 57% surge in demand for hydroxychloroquine and a 90% increase in chloroquine. Neither HCQ nor chloroquine has been approved by the U.S. Food and Drug Administration to treat COVID-19. 94 |
| Itolizumab (Biocon) ‘humanized monoclonal antibody’ developed by the Bangalore-based biopharmaceutical company, Biocon, in collaboration with the Centre for Molecular Immunology (CIM) in Cuba. | Inadequate sample size for randomized clinical trial testing; No evidence yet that it prevents deaths. | The trial by Biocon was conducted on a sample size of 30. This was criticized on the grounds that the sample size was not large enough to prove efficacy conclusively. Biocon defended itself by claiming that it had used Simon’s two-stage design method in which if there are two or more deaths in the control group (that is of size 10 here), then even a trial with sample size of 30 can give clinically relevant results.95,96 | The Drug Controller General of India (DGCI) has given “restricted emergency use” approval to itolizumab, a drug used to cure skin ailment psoriasis, for treating COVID-19 patients with moderate-to-severe acute respiratory distress. |
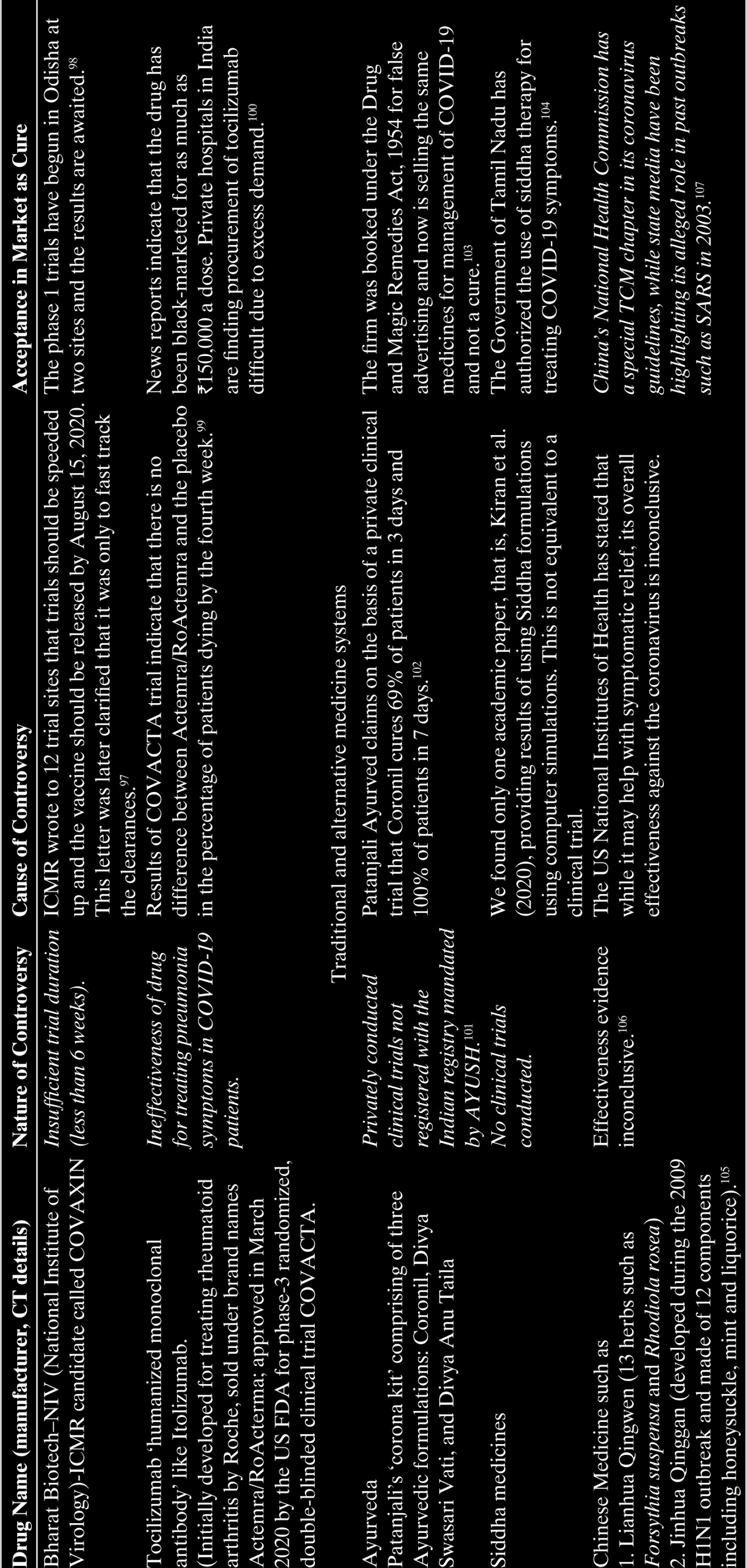
| Bharat Biotech–NIV (National Institute of Virology)-ICMR candidate called COVAXIN | Insufficient trial duration (less than 6 weeks). | ICMR wrote to 12 trial sites that trials should be speeded up and the vaccine should be released by August 15, 2020. This letter was later clarified that it was only to fast track the clearances. 97 | The phase 1 trials have begun in Odisha at two sites and the results are awaited. 98 |
| Tocilizumab ‘humanized monoclonal antibody’ like Itolizumab. (Initially developed for treating rheumatoid arthritis by Roche, sold under brand names Actemra/RoActerma; approved in March 2020 by the US FDA for phase-3 randomized, double-blinded clinical trial COVACTA. |
Ineffectiveness of drug for treating pneumonia symptoms in COVID-19 patients. | Results of COVACTA trial indicate that there is no difference between Actemra/RoActemra and the placebo in the percentage of patients dying by the fourth week. 99 | News reports indicate that the drug has been black-marketed for as much as ₹150,000 a dose. Private hospitals in India are finding procurement of tocilizumab difficult due to excess demand. 100 |
| Traditional and alternative medicine systems | |||
| Ayurveda Patanjali’s ‘corona kit’ comprising of three Ayurvedic formulations: Coronil, Divya Swasari Vati, and Divya Anu Taila |
Privately conducted clinical trials not registered with the Indian registry mandated by AYUSH. 101 | Patanjali Ayurved claims on the basis of a private clinical trial that Coronil cures 69% of patients in 3 days and 100% of patients in 7 days. 102 | The firm was booked under the Drug and Magic Remedies Act, 1954 for false advertising and now is selling the same medicines for management of COVID-19 and not a cure. 103 |
| Siddha medicines | No clinical trials conducted. | We found only one academic paper, that is, Kiran et al. (2020), providing results of using Siddha formulations using computer simulations. This is not equivalent to a clinical trial. | The Government of Tamil Nadu has authorized the use of siddha therapy for treating COVID-19 symptoms. 104 |
| Chinese Medicine such as 1. Lianhua Qingwen (13 herbs such as Forsythia suspensa and Rhodiola rosea) 2. Jinhua Qinggan (developed during the 2009 H1N1 outbreak and made of 12 components including honeysuckle, mint and liquorice). 105 |
Effectiveness evidence inconclusive. 106 | The US National Institutes of Health has stated that while it may help with symptomatic relief, its overall effectiveness against the coronavirus is inconclusive. | China’s National Health Commission has a special TCM chapter in its coronavirus guidelines, while state media have been highlighting its alleged role in past outbreaks such as SARS in 2003. 107 |