
Abstract
Our study examines brokering of situated knowledge within an organizational context, characterized by professional hierarchy. We examine how professional affiliation and associated power differentials impact upon knowledge brokering at the individual and group levels within an organization. Our empirical case, which combines social network analysis and qualitative fieldwork, is set in healthcare with a focus upon integration of management, psychosocial and clinical component knowledge domains deemed necessary for treatment of a long-term condition. Our study shows that peer-to-peer knowledge brokering, which is framed by professional hierarchy, remains pervasive with respect to medical knowledge brokering. However, social structures might be mediated through developing architectural knowledge, reflected in both formal and informal organizational routines and schema, which engenders community tendencies that transcend professional hierarchy, so that knowledge brokering is more widely distributed to benefit patients.
Keywords
Introduction
The management of knowledge across occupational boundaries has become widely accepted as amenable to intervention in pursuit of improved organizational performance (Swan & Scarbrough, 2001). Within this broader agenda to intervene in the management of knowledge, there has been a more recent focus upon internal knowledge brokering, which aims to ensure the right knowledge is in the right hands at the right time (Delmistri, 2005; Fernandez & Gould, 1994; Hargadon & Sutton, 2000; Verona, Prandelli, & Sawhney, 2006). Despite its emergence as a more specific construct within the broader knowledge management field, much of the knowledge-brokering literature remains prescriptive, with little evaluation of the interaction of knowledge brokering and social structure (Hargadon, 2002). Further, literature focuses upon the external brokering of knowledge into the organization, as opposed to emphasis upon internal brokering of knowledge within the organization, and examines knowledge brokering at the individual level, rather than group level, of analysis.
As a starting point in our study of knowledge brokering, we delineate the knowledge broker (individual-level analysis) from knowledge brokerage (group-level analysis). We also take a more critical, practice-based and collective perspective upon knowledge (Blackler, 1995; Cook & Brown, 1999; Gherardi, 2001; Gherardi & Nicolini, 2000; Lave & Wenger, 1991; Orlikowski, 2002), to focus upon the interaction of internal knowledge brokering, at the individual and group levels of the organization, with occupational structures in a professional bureaucracy (Mintzberg, 1979). With reference to the influence of the power of professional groups, we address a research gap regarding our understanding of the interaction of structure and agency in internal knowledge brokering (Shi, Markoczy, & Dess, 2009). In our study we develop a framework to better understand the micro-mechanisms that underlie effective internal knowledge brokerage at the individual and group levels of analysis, with a focus upon professional cultures, power and legitimacy that underpins knowledge mobilization across knowledge domains.
Our empirical case study is set in healthcare, where, globally, policy makers seek to ensure that knowledge is more effectively brokered through workforce reconfiguration, so that delivery of service is more integrated (Currie, Finn & Martin, 2010a). While somewhat distinctive, we argue that healthcare represents an exemplary empirical site for our study of knowledge brokering, from which we can generate transferable lessons for other organizations. Specifically, first, healthcare exemplifies the organizational archetype, the professional bureaucracy, in which a core group of professionals are dominant (Mintzberg, 1979). Second, healthcare is a context where social structures produce institutionalized occupational boundaries, which represent a significant challenge for knowledge brokering because formal specialization and occupational subcultures create an intra-organizational network that is rich in structural holes (Burt, 1992, 2001, 2005). Relatedly, distinct epistemic communities, which cohere around professional domains, impact upon knowledge brokering (Ferlie, Fitzgerald, Wood, & Hawkins, 2005). Finally, as with many other professionalized organizational contexts, there is a gap in our understanding of the social structures that impact upon knowledge brokering (Greenhalgh, Robert, MacFarlane, Bate, & Kyriakidou, 2004).
Empirically, our study is mixed method and, over three years, we undertook social network analysis (SNA) and 61 semi-structured interviews with all professionals and managers identified in the network, complemented by quarterly observation of team meetings and ward rounds. The combination of SNA and qualitative fieldwork engenders richer insight with respect to the micro-mechanisms that frame internal knowledge brokerage. The integration of SNA and qualitative fieldwork is a relatively novel approach to the study of knowledge brokering, and one which we hope engages the readers.
The article is structured as follows. First, within the literature review, we set out our conception of knowledge, and draw out implications for how knowledge might be managed, emphasizing knowledge brokering. Drawing upon more specific literatures about the sociology of professions and healthcare policy, we then discuss how knowledge brokering is likely to play out in the healthcare context. Second, we present the research design for our study, including an explanation of the English healthcare context in which we examined knowledge brokering. We also explain our use of mixed methods, SNA and qualitative fieldwork. Third, we present our empirical case, and integrate empirical findings from SNA and qualitative fieldwork, to analyse and explain the patterns of knowledge brokering in our healthcare case at the individual and group levels. In the conclusion, we summarize our analysis of the empirical case and outline our theoretical contribution to knowledge brokering which, in turn, drives policy and practice implications that extend beyond our single case. Finally, we make suggestions for further research.
What is Knowledge and Knowledge Brokering?
We regard knowledge as a resource applied by social actors in an attempt to solve problems. It can never be removed from its context, as it is bound to its use, and its user within the organization (Blackler, 1995). Thus, we emphasize knowledge mobilization is situated and intrinsically represents a social and collective phenomenon (Lave & Wenger, 1991; Orlikowski, 2002). Knowledge is not something people ‘have’, but something they ‘do’, with practice connecting ‘knowing’ with ‘doing’; i.e. it is not a codifiable entity, but embedded within and inseparable from practice (Blackler, 1995; Cook & Brown, 1999; Gherardi, 2001, Gherardi & Nicolini, 2000; Lave & Wenger, 1991; Orlikowski, 2002). From this perspective, organizations are distributed knowledge systems, with uncertainty about the knowledge required for any given activity, so that knowledge mobilization processes are dynamic and situated within networks of relationships (Bosch-Sijtsema, Fruchter, Vartiainen, & Ruohonaki, 2011; Nonaka & Nishiguchi, 2001; Tsoukas, 1996; Weick & Roberts, 1993).
Political and normative dimensions of networks of relationships impact knowledge mobilization, and may render social actors less willing and able to broker knowledge than more managerialist literature assumes (Alvesson & Karreman, 2001). At this point, aligned with our emphasis upon the political and normative dimensions of networks of relationships, readers may note our continued use of the term ‘knowledge mobilization’ rather than ‘knowledge management’, as an indication of our predisposition in this direction; i.e. we signal that we regard the term ‘knowledge management’ as rather prescriptive, and which underplays the difficulty of any attempt to ‘manage’ knowledge. While not Foucauldian (Doolin, 2002) or Marxist (Lehr & Rice, 2002), our study is thus broadly positioned within a critical literature, which highlights the significance of power and legitimacy upon knowledge mobilization (Crilly, Jashapara, & Ferlie, 2010). In positioning our study in this way, we seek to counter more managerialist prescriptions for knowledge management, specifically highlight the challenge of mobilizing experiential or tacit knowledge, distinctive to any professional practice, for organizational advantage.
Within this more critical, situated perspective upon knowledge mobilization, we view knowledge brokering as the translation of knowledge in the course of day-to-day professional practice. Knowledge brokering through situated interaction is crucial for the more contextualized nature of tacit knowledge, which underpins professional practice (Lave & Wenger, 1991; Polanyi, 1966). We highlight our focus upon ‘internal’ knowledge brokering (Cillo, 2005), as distinct from ‘external’ knowledge brokering. The former relates to the type of practice-based knowledge we have highlighted thus far, with tacit knowledge brokered within the organization at a local level. Internal knowledge brokering occurs as participants in any collective practice share understandings about what they are doing and what this means in real time, and knowledge is co-constructed by participants through socially shared ‘webs of belief’ (Brown, Collins, & Duguid, 1989). The latter, meanwhile, is likely to relate to brokering more formal or codified knowledge from outside the organization (for example, best practice from other organizations, evidence produced through research) into practice. While, recently, there has been an emphasis upon external knowledge brokering of formal evidence, produced through research, into practice within healthcare (see, for a systematic review, Crilly et al., 2010), the importance of internal knowledge brokering has been less recognized.
Contextualized knowledge linked to specific professional practice domains constitutes component knowledge. The integration of component knowledge domains requires the development of architectural knowledge. Architectural knowledge brings together professional skills to fulfil a given task and collective knowledge about how different professionals should work together (Balogun & Jenkins, 2003; Galunic & Eisenhardt, 2001; Henderson & Clark, 1990). Whereas component knowledge is based in localized professional practice, architectural knowledge may consist of organizational and management routines, schema or knowledge that structures interactions by local-level actors.
Different component knowledge is commonly a feature of professional bureaucracies, where ways of organizing are focused upon individualistic, functionally segmented and hierarchical knowledge structures. In some professionalized contexts, such as healthcare, component knowledge is myriad and interacts in complex ways. As such, the delivery of the professional service may require that knowledge is embedded in non-hierarchical organization, glued together by shared values (Lam, 2000). More organic ways of organizing may constitute the necessary architectural knowledge to integrate disparate component knowledge domains. Knowledge brokering is likely to engender the development of architectural knowledge on the basis that it links professional practices, and introduces elements of one practice to another (Wenger, 1998). For example, brokering may link practices by facilitating inter-professional transactions and thus facilitate the creation of a shared vocabulary that can be utilized by different actors, even where meanings for the same term may differ across those actors (Michaels, 2009).
Much of the knowledge-brokering literature focuses on the role of the individual in mobilizing knowledge through using their inbetween vantage position to connect, recombine and transfer to new contexts otherwise disconnected pools of ideas (Hargadon & Sutton, 2000; Verona et al., 2006). A brokerage role allows those in linking positions to mediate the flow of resources or information between two other unconnected actors (Burt, 1992). At the individual level, the brokerage role can be delineated into a number of roles (Fernandez & Gould, 1994), as set out in Table 1.
Typology of knowledge-brokering roles

[tfn]Source: Fernandez & Gould (1994)
Within this typology of knowledge-brokering roles, we highlight the distinction between those brokering knowledge into a group to which they belong (i.e. representative, gatekeeper, coordinator) and those that broker knowledge into a group (consultant) or across groups (liaison) to which they do not belong. In line with our research concerns, Fernandez and Gould (1994) show that power differentials or ‘status gaps’ influence knowledge brokering, with more powerful stakeholders able to enact the full range of knowledge-brokering roles beyond their group affiliation. This suggests liaison and consultant knowledge-brokering roles may prove more difficult to enact, particularly where framed by power differentials. In support of such assertions, Shi, Markoczy and Dess (2009) highlights that peer-to-peer knowledge brokering is more effective, on the basis that legitimacy is a key requirement for knowledge brokering.
While, more recently, attention has been paid to knowledge brokering at the individual level, there is a dearth of empirical studies examining possibilities for knowledge brokering at group level as a way of moderating the effect of macro-level social structures upon knowledge mobilization, despite emphasis upon knowledge as residing at, or being embedded in, collective, as much as individual, practice (Lave & Wenger, 1991). Our study seeks to address this gap, and to examine knowledge brokering as a group-level phenomenon, as well as to apply and elaborate upon literature examining individual-level knowledge brokering, with an emphasis upon how power and legitimacy frame prospects for knowledge brokering at both individual and group levels.
Knowledge mobilization and brokering in healthcare
Healthcare has reflected an upsurge of interest regarding knowledge mobilization and knowledge brokering (Canadian Health Research Foundation, 2003; Clark & Kelly, 2005; Davies & Nutley, 2000; Dobbins et al., 2009; Lomas, 2007; Martin, Currie, & Finn, 2009; Van Kammen, de Savigny, & Sewankambo, 2006; Verona et al., 2006; Ward, House, & Hamer, 2009a, 2009b), to address ‘wicked issues’ (complex social problems, which are ill-defined and where any solution lies beyond the remit of any organization of professional group) (Rittel & Webber, 1973). However, the extant healthcare literature in this area focuses upon external knowledge brokering, and remains relatively normative. There is little empirical evaluation of the potential for internal knowledge brokering to deliver healthcare more effectively (Dobbins et al., 2009). In particular, there is little consideration of how social structures present barriers to knowledge mobilization in healthcare, and how these might be mediated through internal knowledge brokering (Greenhalgh et al., 2004).
In taking a more critical perspective upon healthcare policy, we argue that policy initiatives aimed to mobilize and broker knowledge are a specific example of how the work of medical, and other health and social care, professionals is framed by managerialist initiatives aiming to erode professional autonomy and established lines of medical power and influence (Freidson, 1984; Harrison & Ahmad, 2000; Reed, 1996). Within the English health and social care context, for example, Labour governments from 1997 to 2010 sought to ‘modernize’ the workforce through re-engineering care pathways, creating new roles and networked, collaborative or team-worked provision of service, that are based on professional accomplishment, rather than traditional jurisdiction (Bourgeault and Darling, 2008; Bourgeault & Mulvale, 2006; Bourgeault, Kuhlmann, Neitermann, & Wrede, 2008; Buchan & Calman, 2005; Currie et al., 2010a; Davies, 2000; Kuhlmann, 2008; Kuhlmann & Saks, 2008; McKee, Dubois, & Sibbard, 2006; Pahor, 2008; Richards, Carley, Jenkins-Clarke, & Richards, 2000; Sibbald, Shen, & McBride, 2004). In essence, policy makers seek ‘to build jobs around patients, rather than around professions’ (Department of Health, 2002, p. 7). The benefits of this so-called (by policy makers and senior organizational managers) ‘patient-focused’ approach, were premised on improved knowledge mobilization, whereby hitherto disparate professional groups exchanged component knowledge across boundaries, thereby fostering a mutual set of objectives and working practices, which ultimately resulted in more streamlined and integrated working (Bate & Robert, 2002); i.e. a change in the formal organization of healthcare pathways was expected to provide the necessary architecture to integrate disparate component knowledge.
The system of professions in healthcare poses a particular challenge to policy attempts at mobilizing and brokering knowledge. The development and maintenance of the system of professions, within and beyond healthcare, are well documented in the sociological literature. Abbott (1988) describes the construction of jurisdictions over which professions claim exclusive authority and defend from competing claims from neighbouring professions. Abbott (1988) highlights how occupational legitimacy and power are established within situated interactions framed by occupational hierarchy within the workplace. Established professions tend to cede their core work only reluctantly, using an armoury of techniques to defend their territory (Abbott, 1988). By making claims to scientific or specialist expertise, for example, dominant professions are able to set the terms of reference of such territorial battles, so that challengers are immediately weakened by the need to appeal to the discursive norms of the dominant professions (Larson, 1990). Particularly within medicine, monopoly over the techniques and competences needed to practise in a given domain, and carefully guarded entry to a profession, assist the endurance of professional power (Freidson, 1970). The accrual of status by a profession, then, is a process ‘in which power and persuasive rhetoric are of greater importance than the objective character of knowledge, training, and work’ (Freidson, 1970, p. 79). The result is that some professionals, and by implication knowledge domains, are positioned as higher status than others. Within healthcare, the dominance of doctors (with more specialist doctors afforded higher status than their generalist counterparts) over other clinicians (Freidson, 1994), specifically the ongoing subservience of nursing and other professions allied to medicine (PAMs) to doctors (Freidson, 1994; Larkin, 1983), is likely to stymie any effort to mobilize knowledge across boundaries; i.e. healthcare professionals, particular the medical group, may be unwilling to mobilize knowledge beyond their immediate ranks.
There is an emerging literature that considers how the dynamics of systems of healthcare professions, outlined above, impacts knowledge mobilization. For example, in evaluating network forms of organization, Addicott, McGivern and Ferlie (2007) reported knowledge mobilization within cancer networks in the English National Health Service to be considerably limited by professional cleavages and power differentials. Similarly, knowledge mobilization in matters of patient quality and safety is inhibited by contestation around professional identities and jurisdictions (Currie, Waring & Finn, 2008; Gherardi & Nicolini, 2000; Waring & Currie, 2009). Other studies illustrate more generally the challenges of mobilizing knowledge across professional boundaries, where healthcare delivery encompasses disparate component knowledge domains. In a study of mainstreaming genetics care, powerful healthcare professionals attempted to retain control of knowledge, through delegating knowledge related to routine clinical activity, but then controlling this through providing education and auditing those to whom routine activity had been delegated; i.e. the latter was positioned as an ‘outreach’ assistant, with the status of the powerful healthcare professional reinforced (Currie, et al., 2010a; Currie, Lockett, Finn, Martin, & Waring, 2012). In all these studies, the ability of powerful professionals to counter policy, which potentially disrupts existing division of jurisdictional responsibility, is evident.
Matters of knowledge mobilization are a cultural as well as political matter. Healthcare practitioners may be also unable, as well as unwilling, to mobilize knowledge across professional boundaries (Currie & Suhomlinova, 2006). Regulatory and normative processes shape the perspectives of healthcare practitioners in such a way that professional affiliation adversely affects the likelihood of finding the ‘common ground’ for collaboration across professions. Divergent education, training, socialization and career structures for professional groups adversely influence knowledge mobilization because the various professionals delivering healthcare may not share perspective, or language, through which to do this. Healthcare professionals follow ‘mindlines’, not ‘guidelines’, in delivering healthcare, with tacit knowledge embedded in practice; i.e. in the healthcare context, the situated nature of knowledge may be more significant. Such mindlines are developed through interaction with peers as any healthcare professional seeks to acquire knowledge from others that benefits them in particular circumstances, for example, when diagnosing a patient (Gabbay & Le May, 2004). Thus, the existence of disparate component knowledge may also be a more significant matter in healthcare, and the development of architectural knowledge to mediate fragmentation of component knowledge domains remains a challenging matter (Finn & Waring, 2006).
In sum, sociology of professions literature, applied to healthcare, suggests mobilizing knowledge across professional domains is no easy task. Regarding knowledge brokering, the development of professional domains that are assiduously defended by its members means that peer-to-peer knowledge brokering is more likely at individual or collective levels. So, at the individual level, a knowledge broker is likely to be affiliated to a profession into which knowledge is being brokered; i.e. representative, coordinator or gatekeeper roles. We also suggest, drawing upon sociology of professions literature, that where a knowledge broker belongs to a relatively powerful profession, they may be able to extend their knowledge brokering role to encompass liaison or consultant, so they broker knowledge into professions to which they are not affiliated (Fernandez & Gould, 1994). In contrast, where relatively low status, it may prove difficult for a healthcare professional to enact a liaison or consultant knowledge-brokering role. Meanwhile, at the collective level, any service domain is likely to be characterized by potentially disparate communities of practice, each of which is based upon occupational affiliation (Lave & Wenger, 1991), with the challenge remaining of how to connect these up.
Drawing upon the literature above, our study seeks to better understand the micro-mechanisms that underlie effective internal knowledge brokerage at the individual and collective level of organization, with a focus upon professional cultures, power and legitimacy that frame knowledge mobilization across occupational domains.
Research Design
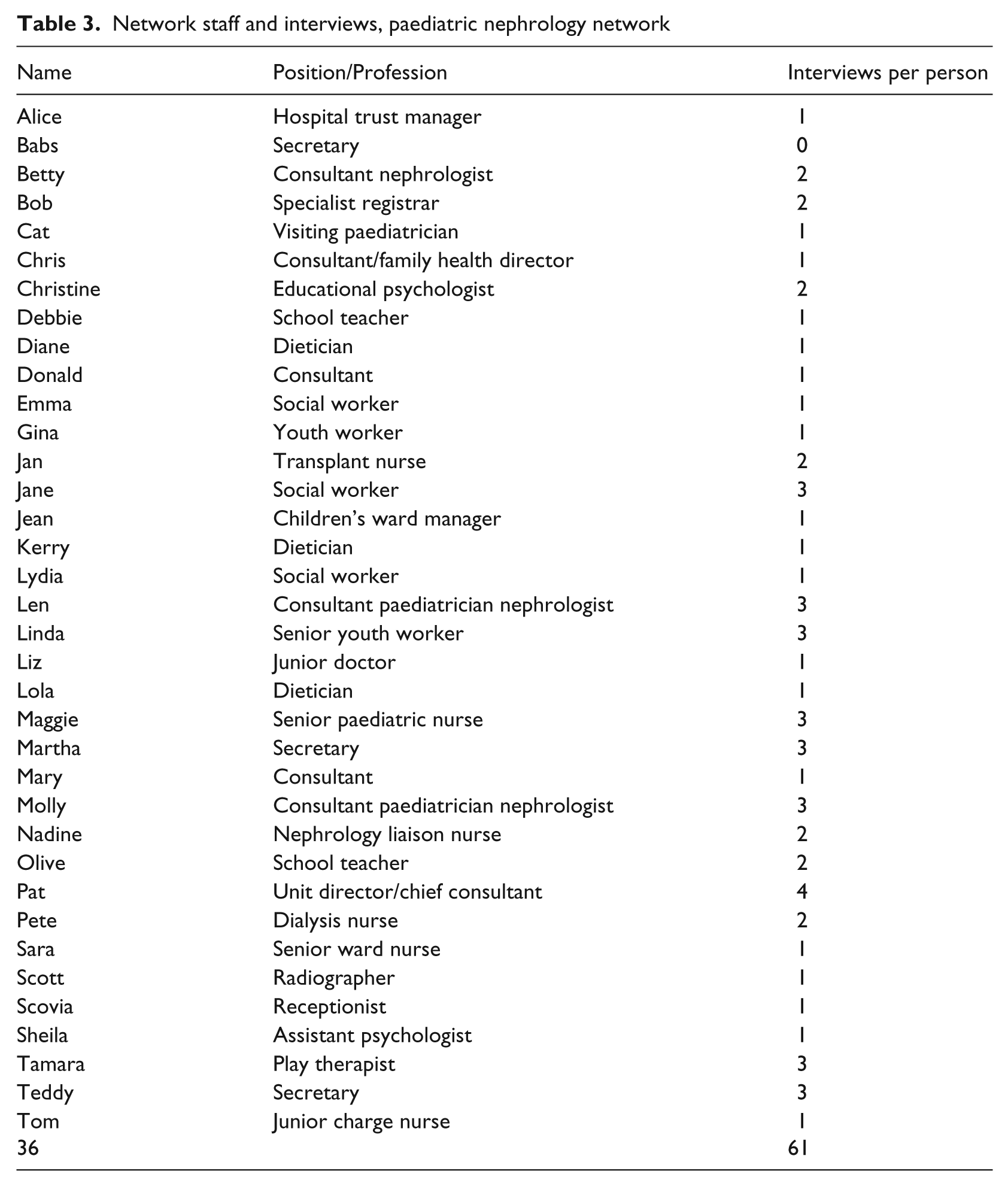
Fieldwork takes place within a single empirical case – the delivery of paediatric nephrology services to children with a long-term kidney problem, which is managed through clinical and psychosocial interventions with the aim of avoiding comorbidities associated with such a condition, and the inevitable necessity for kidney transplant later in life. The service is delivered by a multidisciplinary team, comprising doctors who specialize in paediatric nephrology, but also from other specialties, such as adult nephrology and other areas connected to the comorbidity that characterizes long-term kidney conditions, paediatric and other nurses, educational psychologist, teacher, social workers, play therapists, youth workers and dieticians (see Table 3, which outlines the spread of interviewees).
Single cases are useful to generate rich description and explanation of processes, such as knowledge brokering, which can be theoretically generalized to aid transferability of analysis (Yin, 1994). In the empirical case study, research design mixes methods: social network analysis (SNA) and qualitative fieldwork that encompassed semi-structured interviews and observation. SNA preceded the qualitative fieldwork. SNA aligns with the theoretical and empirical focus of our study, specifically relational issues related to knowledge brokering in settings characterized by professional power and jurisdiction (Lazega, 1992; 2000; 2001; Lazega, Lemercier, & Mounier, 2006).
For the SNA, all paediatric nephrology network staff (36) provided responses. We focused upon three component dimensions of knowledge: clinical knowledge (encompassing medical, nursing and ‘other’ knowledge, e.g. dietetics): psychosocial knowledge (encompassing social work, education and therapy) and management knowledge (i.e. of the organizational structures and processes framing the delivery of care). The first two of these were identified by respondents as related to the nature of the clinical service, that of management of a long-term condition, which necessarily integrated clinical and psychosocial knowledge (in a surgical intervention, for example, only clinical knowledge may be required). For the third dimension of component knowledge, exploratory interviews revealed the importance of the integration of clinical and psychosocial knowledge being held together by more general knowledge about organization, which we empirically labelled ‘management knowledge’, but which we later conceptualized as ‘architectural knowledge’ (Balogun & Jenkins, 2003; Finn & Waring, 2006; Galunic & Eisenhardt, 2001; Henderson & Clark, 1990). To further check our grounding of component knowledge domains, we attended a meeting of the network and presented examples of each category for agreement with our research subjects.
The social network questionnaire was designed with reference to standard social network questions used in other studies (Cott, 1997; Cross & Cummings, 2004; Cross & Sproull, 2004; Fattore, Frosini, Salvatore, & Tozzi, 2009; Scott, 2000). The questionnaire included a roster of names of all staff working in the network at the time of the survey (Marsden, 1990). Using this roster, we asked questions of research subjects about the extent to which a person provides them with management knowledge, psychosocial knowledge and clinical knowledge, e.g. ‘I rely on this person for advice on clinical matters to do my job.’ These items about knowledge-related interactions were collected using a five-point Likert scale. We also collected information on frequency of contact and quality of relationships. The frequency of contact ties were captured by asking ‘How often do you have contact with each named person on the list?’ and respondents were asked to identify frequency of contact, using the scale where 1 = daily, 2 = weekly, 3 = monthly, 4 = rarely, 5 = never. The quality of relationships was collected on a four-point scale, where the ties were measured by asking the respondent to rate the overall quality of the working relationships they have with each person they ticked. To do this, they were asked to circle the number on the scale that best reflects relationship quality, where 1 = poor relationship, 2 = fair relationship, 3 = good relationship, 4 = excellent relationship. The measures and analysis were conducted using the most widely used network analysis software, UCINET (Borgatti, Everett, & Freeman, 2002).
SNA data was used to generate measures at the individual level and the network level of analysis. At the individual level of analysis, first, SNA data identifies central actors (through centrality scores). Table 2 outlines how each score was generated and what each score means. Second, SNA data identifies respective knowledge-brokering roles for central actors. The knowledge-brokerage role for each actor is represented by a brokerage score (Gould & Fernandez, 1989), which for a given actor is computed with respect to a given role (the five roles were described earlier in Table 1 as coordinator, consultant, gatekeeper, representative and liaison). The score is computed as follows. Taking each actor, and having identified the group (nurse, doctor, other) that they belong to, their knowledge-brokering interactions are counted as assigned to different knowledge-brokering roles within or between groups. This score is then normalized, i.e. each actor’s knowledge-brokerage roles are expressed as a ratio of the average of that knowledge-brokering role gleaned from all actors.
How centrality scores are generated and what they mean

[tfn] a Degree-based centrality reflects an actor’s level of network activity or involvement
At the network level, we explore overall density of the network with respect to knowledge brokering, consisting of the overall density of the network, density within each professional group and density of interactions between groups. Density is the most widely cited network measure and is defined as size (or number of ties) relative to the number of possible ties. This gives an indication of the extent to which knowledge brokering represents a collective phenomenon. It should be noted that a density score of 100 per cent means everyone is connected up for the purpose of knowledge brokering, while a density score of 0 per cent means no one is connected up; i.e. a low score indicates heterogeneity. The density scores were computed with UCINET for the whole network, and within and between professional groups. For more detail on SNA methods, please refer to the final report produced by the authorial team (Currie et al., 2010b).
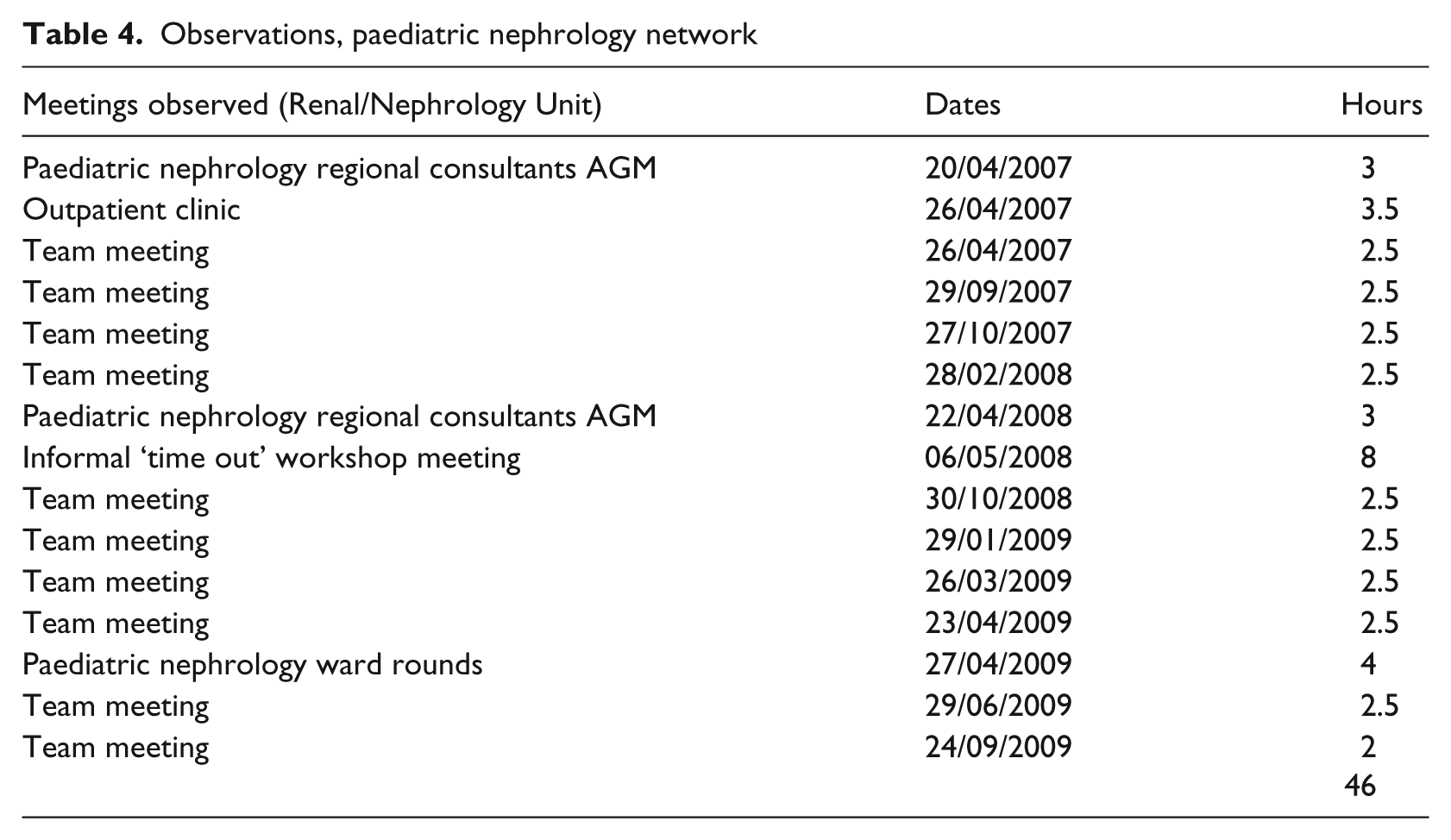
We carried out 61 semi-structured interviews to draw out illustrations of knowledge brokering and the context for this. Some network members were interviewed more than once, where they occupied key brokering positions and were deemed informative regarding issues we wanted to follow up. Complementing this, given knowledge brokering is a situated activity (Currie & Kerrin, 2003; Martin et al., 2009) and that observation contextualizes understanding of knowledge-brokering activity, we engaged in 46 hours of observation of team meetings, clinics and ward rounds (see Tables 3 and 4).
Network staff and interviews, paediatric nephrology network
Observations, paediatric nephrology network
Analysis of data took place as follows. A number of iterations were undertaken by the authors in the development of key themes from SNA, interviews and observation. Patterns of knowledge brokering gleaned from SNA informed the qualitative fieldwork. However, qualitative fieldwork also informed further examination of SNA to examine patterns of knowledge brokering in a more nuanced manner. One of the authors generated SNA, while the other author (supported by the fieldworker) carried out interviews and observation, and then created embedded analytic notes within interview transcripts and observation notes (the latter were recorded on a template that identified actors, knowledge-brokering domain and context, thus reflecting our research concerns). Related parts of the embedded analysis in each interview and observational notes were placed together. One co-author checked and discussed their coding of interview transcripts and observational notes with the other co-author, ensuring reliability of interpretation and enhancing analysis. The analysis of qualitative fieldwork was then combined with SNA, and the combined analysis agreed across the authorial team, with a series of iterations of analysis produced in four half-day meetings, against the overarching research questions. At all stages, authors were alert to counter-evidence to the emergent analytical themes. Finally, to authenticate and elaborate upon our analysis, findings have been presented in written and verbal form to healthcare professionals and policy makers, including the subjects of our study. We have also presented our analysis to a network of health and social care professionals in elderly care, to assess the transferability of analysis to different settings (note our analysis strongly resonated with those working in elderly care).
Knowledge Exchange Processes
We present our data as follows. First, we present data focused on patterns of knowledge brokering at the individual level of the network. Second, we present data focused on knowledge brokering at the network level. Our intention is to consider both individual knowledge brokering and network knowledge brokerage as separate phenomena, but then to examine their interdependence in discussion following our empirical presentation.
Individual-level patterns of knowledge brokerage
Table 5 shows centrality measures at the individual level of the network. High in-degree centrality indicates the importance of certain individuals. In the clinical network centralities, medical consultants (Pat, Len and Molly) have high in-degree status. They are people on whom many other staff depends upon to broker clinical knowledge. With regard to psychosocial knowledge, social workers (Lydia and Jane) are those whom most staff rely on for psychosocial knowledge. Again, we show how knowledge brokering in a particular domain, clinical or psychosocial, is linked to professional affiliation that engenders peer-to-peer interaction (Shi, Markoczy, & Dess, 2009). Meanwhile, high out-degree centrality scores indicate positions important in brokering knowledge to others in the network. As well as Pat (unit director/lead consultant), others seek out a high number of individuals around clinical knowledge, specifically Lydia (social worker), Tamara (play worker) and Anna (dietician). With regard to psychosocial knowledge brokering, Pete (dialysis nurse) joins the medical consultants (Pat, Len and Molly) in seeking out a high number of other individuals. Finally, with regard to betweenness centrality, and in relation to clinical knowledge, Lydia (social worker), Pete (dialysis nurse) and Rachel (senior ward nurse) are actors with the highest values, indicating that they are sitting on many of the shortest routes between other members of staff. In essence, this demonstrates that much of the clinical knowledge exchange passes through them and that they interact with many other individuals in the network. They have a high capacity to broker knowledge among other actors. In relation to psychosocial knowledge, we find Lydia has the highest betweenness score, where she may be controlling the exchange of knowledge relating to psychosocial knowledge, or has the potential to do so. In this knowledge domain, Lydia has the capacity to broker to others.
Centrality measures at individual level of network

In further breaking down the individual-level brokering, Tables 6, 7 and 8 provide the relative brokerage roles for the provision of management knowledge, clinical knowledge and psychosocial knowledge respectively.
Relative brokerage role for management knowledge sharing a

[tfn]a Groupings are: 1, psychosocial; 2, admin.; 3, consultants; 4, nurses; 5, dieticians
Relative brokerage role for psychosocial knowledge sharing a
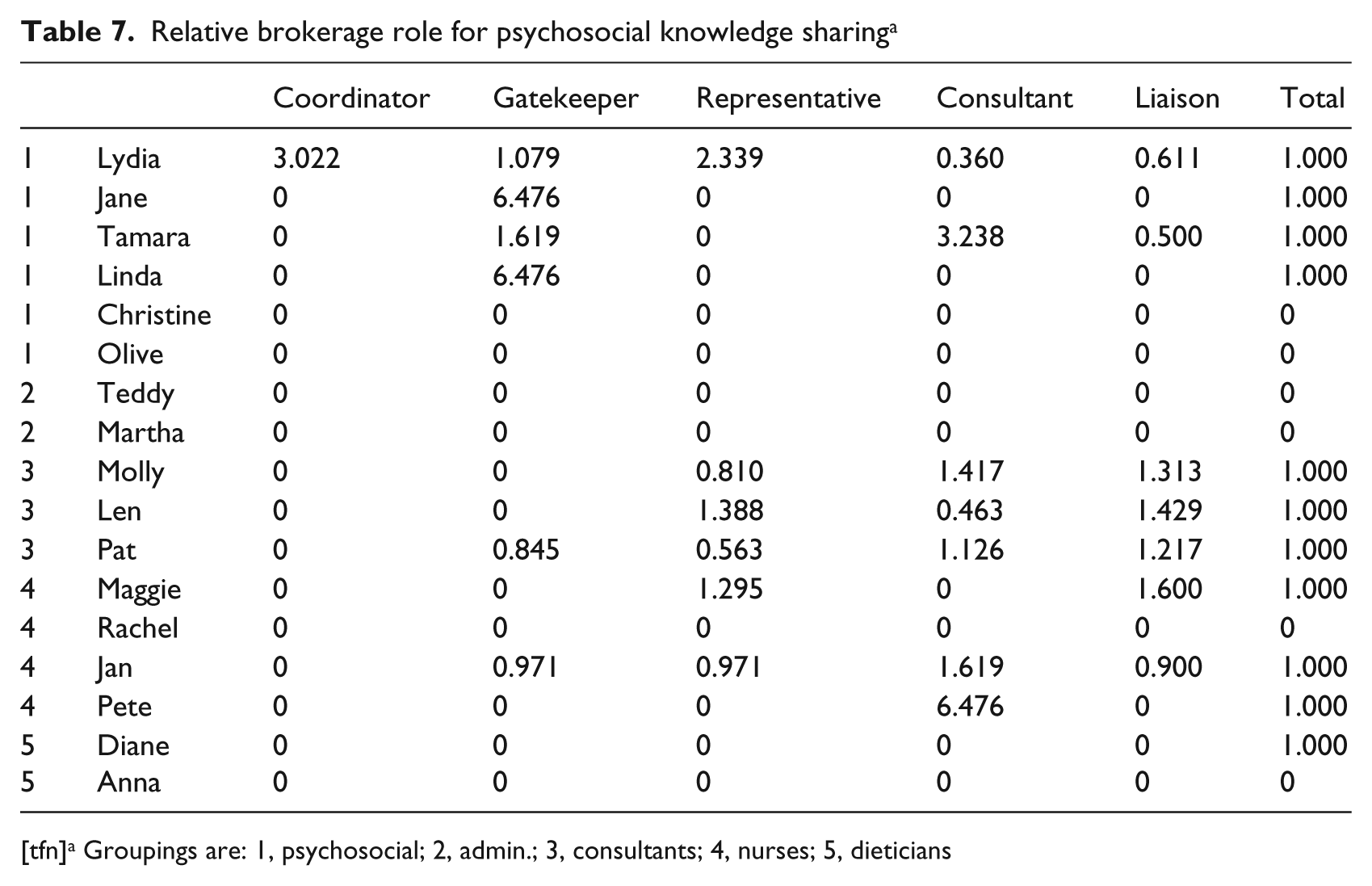
[tfn]a Groupings are: 1, psychosocial; 2, admin.; 3, consultants; 4, nurses; 5, dieticians
Relative brokerage role for clinical knowledge sharing a

[tfn]a Groupings are: 1, psychosocial; 2, admin.; 3, consultants; 4, nurses; 5, dieticians
From Table 6, in terms of management knowledge, everyone seems to have a liaison role (where the relationship is that none of the triad of actors belongs to the same division). Exemplifying distribution of brokerage, the secretaries also have a brokering role (Martha has a liaison role, while Teddy has a gatekeeper role).
The qualitative fieldwork further revealed that management knowledge brokering was distributed, specifically that the role of knowledge broker was not constrained to staff with direct patient contact on the wards or in clinics, but equally taken up by administrative staff: If you need something or want to know something about a patient you just go and ask them [staff delivering care]. Everyone [staff delivering care] will also come and ask me, ‘what’s happening with this patient?’ (Teddy, secretary)
Here, administrative staff are often the first or primary contact for outpatients receiving care at home or attending on-site clinics at the hospital, and also responsible for organizing various staff events and coordinating clinics. Their knowledge of a particular patient is vital to network functioning. In terms of Fernandez and Gould’s knowledge-brokering roles, they enact a liaison role (Fernandez & Gould, 1994).
Similarly, we observed how the youth worker actively emerged as a management knowledge broker over the course of several meetings. One example occurred during a time-out day (May 2008) when network members were thrashing out the details of moving the paediatric nephrology network to another hospital site. In the midst of a major discussion about facilities and space dominated by the clinicians, Linda (senior youth worker) simply just stood up and announced: ‘This is what’s come out of my conversations with young people in our care, which I think is most important.’ She argued for a purpose-built non-medicalized area, a ‘haven’ for teens to get away from family, to just do ‘everyday’ things that they like to do; i.e. ‘chill out’. The value of psychosocial knowledge gained through her professional role was positively received by the network in that, after she had finished speaking, she received a full round of applause accompanied by chants of ‘go Linda go, go Linda’.
When it comes to the psychosocial knowledge-brokering network (Table 7), the senior youth worker (Linda) also enacts a knowledge-brokering role as gatekeeper, i.e. brokering knowledge from outside into her peer group. A social worker (Jane) also plays the gatekeeper role for her peer group. Meanwhile, another [senior] social worker (Lydia) has a coordinating brokerage role, i.e. with her peers. She also represents the interest of her group to others (representation role). Perhaps most intriguingly, since it lies outside the confines of professional peer affiliation, the play therapist (Tamara) and dialysis nurse (Pete) are significant brokers of psychosocial knowledge between group members, but for a group they are not affiliated to (consultant role). Indeed, the play therapist, whom we might position as low status in professional terms, brokers knowledge for a higher-status group (confirmed as doctors in our qualitative fieldwork). Confirming her consultant knowledge-brokering role (Fernandez & Gould, 1994), the play therapist commented: Sometimes because I am in more informal contact with the child and their family, I actually input to decisions made by more important staff, such as doctors, who have to know how family circumstances impact upon clinical care. It’s a bit strange for ‘little old me’ to do this. (Tamara, play therapist)
In the process, Tamara came to ‘recognize the importance of what I do, whereas before, in other jobs, the doctors downgraded it as unimportant’. We consider how the knowledge-brokering role of Tamara, and of other non-clinical professionals (Jane, social worker, Christine, educational psychologist, and Linda, senior youth worker) extends beyond professional affiliation, below, in discussing the integration of clinical and psychosocial knowledge to combat patients resisting medication or injections.
When it comes to clinical knowledge (Table 8), however, the role of knowledge brokers is framed by professional affiliation and hierarchy. The lead medical consultant/director (Pat) and other medical consultants (Molly and Len) play liaison roles. So do the dieticians (Diana and Anna). The senior paediatric nurse (Maggie) and senior dialysis nurse (Pete) coordinate clinical knowledge within their group (coordinator role) and the educational psychologist (Christine) plays a gatekeeper role, again in relation to brokering clinical knowledge to peers.
When observing network meetings, we noted that brokering clinical knowledge beyond the confines of professional hierarchy proves challenging. Consistent with our SNA findings, non-clinical staff explained in more detail how professional hierarchy was necessarily concentrated in clinical settings, but subsequently transformed into multi-professional collaboration in non-clinical settings: At both clinics and ward rounds, the patients get their medical bit sorted out and they get their medical condition monitored and checked. We [non-clinicians] come into the picture either during the rounds, if we’re on the ward, brought in by one of the consultants or a nurse, or else directly after we’ll hear about it at meetings and get involved. (Jane, social worker)
The above is further illustrated within our observations of ward rounds (April 2009) and outpatient clinics (April 2007), which provided valuable insight into the distinctive way that knowledge was concentrated, or brokered, in various contexts, so that there is knowledge brokering within groups as doctors enact a coordination role (Fernandez & Gould, 1994). For example, professional hierarchy and more clinically bound knowledge-brokerage activities were particularly visible on ward rounds, with discussions confined to interactions between doctors. The need for such knowledge to remain concentrated was particularly manifest in cases where patients were under shared care (i.e. combined care under paediatric nephrology and other specialist units due to multiple health issues). When these situations arose, only the lead (medical) consultant and registrar would enter a patient’s room, with the remaining nephrology team standing just outside the door. This seemed to occur largely because the consultants from another specialist unit, as well as their staff, were already occupying the room and conducting their own ward rounds. However, when the lead consultant and registrar announced their arrival, staff from the other specialist unit immediately stepped back and ‘opened ranks’ to allow the former to stand shoulder-to-shoulder next to their medical peers at the patient’s bedside. In shared case situations, overseeing patient treatment and decision making remains foremost with the specialist area deemed to have medical jurisdiction, based on the patient’s specific medical conditions and care requirements. What transpired was a professional exchange of knowledge between consultants from each specialism that collectively focused on the overall status and future care of the patient. Within shared-care arrangements, there was much more siloed knowledge exchange within the medical group, as participants in knowledge exchange enacted a coordination role (Fernandez & Gould, 1994).
However, we also observed that clinical knowledge brokering may be more distributed. Regarding dietary concerns and weight loss or gain, a pervasive issue for patients with chronic kidney disease, we observed how the lead consultant and dietician reciprocally brokered clinical knowledge. This surfaced through our observation that the lead consultant reiterated several times over the course of the rounds: ‘When you come on this ward round or do ward rounds with me, you focus on weight.’ Correspondingly, we noted how the lead consultant would talk to the parents of a patient about the medical implications of ongoing feeding problems and voiced concern about weight issues. However, upon exiting the room, he would then engage with the dietician for advice on how best to deal with the problems in wider dietician terms. They discussed several options, with the dietician conveying what the patient had been consuming to date. She gave her professional opinion about how to improve nutrition using certain foods she felt would best counter this particular patient’s feeding problems. In turn, the lead consultant acknowledged how this course of dietician-led action should support the desired medical outcome. Although ward rounds are primarily focused on medical treatment and thus largely consultant-led, gleaning additional knowledge from other professions was nonetheless brokered through a reciprocal exchange. Evident was the apparent willingness on the part of the consultant to openly broker knowledge across different professional boundaries to deliver integrated care via multi-professional collaboration.
We suggest that the challenge of brokering clinical knowledge beyond professional affiliation and hierarchy is not insurmountable. We observed a marked example of how Christine (educational psychologist) used her knowledge-brokering skills in one meeting (October 2007), where the consultants were discussing two different patients and the medical implications of both having had poor histories of taking vital medication or refusing injections. The discussion then turned to the related psychological implications of both situations and therefore shifted to Christine for her professional input. First Christine provided an update on both children; i.e. one child who had difficulty swallowing tablets was now able to swallow 3 out of 5 pills, and the second child who was needle phobic had now agree to an injection. However, she stressed that the progress made was the result of collective efforts and went on to broker further discussion around the table with other professions/individuals that included a social worker, the play therapist and the youth worker. Each elaborated on the professional contribution they had made alongside the psychological treatment rendered by Christine. For example, the play therapist (Tamara) highlighted using distraction therapy to help deal with the needle phobic issue; the social worker (Jane) detailed how she spent time educating the respective parents of each patient to foster their understanding and support; and the senior youth worker (Linda) provided respite for the patients’ siblings to help take the additional strain off them and their families. In this instance, effective brokering by Christine culminated in providing a bridge between psychosocial knowledge and medical knowledge, enabling knowledge to be transferred easily from one professional domain across several domains. This perfectly illustrates how the pursuit of integrated care for patients, which encompasses its clinical and psychosocial dimensions, can become the common ground for learning and professional collaboration.
Also of interest during our observations was that, when ward rounds were taking place, the senior nurse would continually liaise with the registrar and then relay medical information onto a receptionist on the ward who would then electronically update patient files. Here, the nurse enacted a liaison role (Fernandez & Gould, 1994) between a high-status and a low-status group, neither of which she was a member of. In addition, the senior nurse would also exchange knowledge with the dietician and consultant, and make the necessary notifications to the unit’s catering staff to modify a patient’s dietary requirements accordingly. In this context, the senior nurse assumed a key liaison knowledge-brokering role between specialist professions to achieve a common goal. This particular brokering activity required one’s capability or, as evidenced here, one’s role as a senior nurse, to translate or reframe clinical knowledge from one profession or domain to non-clinicians to engender mutual understanding; i.e. the senior nurse had developed an understanding of different occupational worlds to facilitate such translation. This liaison role appears consistent with professional hierarchy (in contrast to the consultant role enacted by the play therapist we described earlier).
Network-level patterns of knowledge brokerage
Table 9 reveals a dense network in relation to management knowledge, where almost everyone in the network is interacting with each other. At the network level, the structure in terms of high density is an indication of the strength and quality of knowledge brokering (Hansen, 1999). Indeed, 90 per cent of all possible ties are made across the whole network and, within professional groups, up to 100 per cent of possible ties are made, with corresponding dense interactions between professional groups. However, when it comes to brokering psychosocial or clinical knowledge, we find different patterns in the relationships between the actors. In the domains of psychosocial and clinical knowledge brokering, the network is less dense, across different professional groups, and with a particular orientation towards professional hierarchy in the case of clinical knowledge.
Summary of knowledge network characteristics

In considering the effect of high density upon knowledge brokerage, on the one hand, a dense network may enhance knowledge brokerage, due to the high number of actors connected and therefore the better opportunities for coordination of their actions. On the other hand, a dense network produces redundant information, which lessens knowledge-brokerage opportunities and the effectiveness of knowledge brokerage (Burt, 1992). In relation to our data, the densest networks are those that are composed of the same profession, with connections at their densest among medical consultants; i.e. they are more likely to broker knowledge between each other. Networks between professions are less dense, indicating a lack of mutual linkages between certain professions. However, between medical consultants and nurses, and between medical consultants and dieticians, the density measures were high for clinical knowledge; similarly for psychosocial knowledge, the density measures were high between medical consultants and psychosocial workers. But the linkages in terms of general management knowledge are important, particularly between professional groups. At the network level, we found that within professional group density was high, thus indicating effective coordination and brokerage. Across professional groups, the network is less dense, which may avoid the problem of redundant information and facilitate interactions where one group of professionals taps into the knowledge network of another group. Note what we perceive are locally dense professional groups, specifically medical consultants, connected by few bridging ties of key individuals, and this has implications for the network as a whole, which we further explore below. In summary, knowledge-brokering patterns appear more distributed overall than we might expect in a professionalized organization. Our qualitative fieldwork provides insight into why this might be so.
First, our qualitative fieldwork highlights that institutional barriers to knowledge brokering appear mediated because of co-location, or failing this, disparate professionals seek out situated interaction: We’re all in a fairly close geographical area and walk in to each other’s offices fairly easily and often. It takes a while just to get used to doing things this way and know people but then you learn how to freely share information with everyone else. (Mary, consultant)
Geographically, while all members are located on one hospital site, there is some dispersion within this hospital site. Clinical (i.e. all consultants, other doctors, and nurses) and some non-clinical staff (secretaries, play therapists and youth workers) are situated in relatively close proximity, whereas other staff, including dieticians and other non-clinical staff (teachers, social workers and educational psychologist) are located in other areas of the hospital. Conceivably this might pose a barrier to knowledge brokering, particularly for those who do not work side by side on a regular basis. However, knowledge brokering across the network was nevertheless marked, with staff seeking out each other informally on a voluntary ‘as and when’ basis for advice or information: Everybody’s involved on an informal level with each other and everybody knows everybody very well and everybody seems to get on quite well, so I might catch someone in a hallway or coming out the office or whatever. There’s no sort of like, ‘I need to have a meeting about such and such’. (Pete, dialysis nurse)
Second, differences between specialists within the network are acknowledged and respected. Consistent with our SNA findings of a decentralized and well-connected network, knowledge brokering is underpinned by recognition across the network of the legitimacy of a range of non-clinical professions in the delivery of patient care. Specifically, consultants accepted the legitimacy of others’ knowledge (outside the medical group), something that was engendered in their early training and socialization within the paediatric nephrology network: Collaboration depends on what your exposure is during your training. I worked in different specialties as a trainee. This is the only unit I can say truly and effectively works together. Most units have consultants at the top and the rest just kind of branch down, and it just doesn’t work. Everyone talks about multidisciplinary care, only here do we really provide multidisciplinary care. (Molly, consultant)
Further effort to encourage mutual regard for different professional specialists across the network was also exerted during informal indoctrination practices. For example, while most interviewees (i.e. nurses, play therapists, dieticians and psychologist) had been involved in the network for a considerable length of time and so had taken on board the need to exchange knowledge on a cross-professional basis, incoming junior doctors were ‘shown the ropes’ by consultants as a routine part of their induction process: At the orientation done by the consultants, it’s stressed quite clearly at the beginning that we are a multidisciplinary team, so please involve or ask dieticians or specialist nurses or whomever, their advice, and always think, ‘Who else should be involved? What can they add to what we already know?’ (Liz, junior doctor/registrar)
The socialization described above was buttressed by the lead doctor in developing and presenting ‘evidence’ about the benefit of collaboration. He engaged in applied research, to audit the service, on the basis that: Healthcare professionals respond to evidence. In our case, this is less about showing clinical outcomes, since ultimately these are avoiding a kidney transplant twenty years down the line, and more about psychosocial outcomes, such as participation and success in mainstream education, or reported patient and family experience, as gauged through our survey. (Pat, lead consultant, unit director)
Third, an informal rather than management-driven policy of knowledge brokering engendered a better working atmosphere. Collaborative relationships, focused upon the patient, seemed to cut across professional boundaries and counter traditional hierarchies which, in other clinically bound settings, orient towards knowledge silos: It’s such a relaxed environment for me to get the job done, it is just so open. That brings out the best in everybody and that can only benefit the patients. People have the patient’s best interests at heart and aren’t at all protective here, as I have found in other clinical areas, about sharing their knowledge. (Diane, dietician)
The preceding views are perhaps unsurprising, given that they stem from professionals (i.e. Pete, dialysis nurse, and Diane, dietician), located among the lower echelons of the professional hierarchy. We note, however, that this collective rather than individualistic acceptance for an ‘ad hoc’ participative culture of learning and open-door policy seemed equally supported by medical consultants within the network: I prefer to see other staff face to face to exchange information. It’s an informal thing and I think that it is kind of more human in a way, because people talk to each other across all professions and levels within our network. (Molly, consultant)
The advantages of informality described above were observed by the research team at first hand on several occasions, while conducting interviews with individual members in their respective offices. We observed how, regardless of anyone’s specific profession or location, staff would simply turn up at each other’s offices unannounced, or in response to a previous fleeting conversation in a corridor, brief telephone chat or email request. Exchanges varied from imparting information about a particular patient or a recent event on the ward, to conveying professional advice or an opinion about a specific situation. Some examples we observed included: a play therapist showing up in the specialist nursing office to advise a senior paediatric nurse of her availability for distraction therapy to help with a specific patient scheduled for treatment later that same day; an impromptu visit by a dietician to a consultant as she was passing his office, in response to an email she had received earlier about dietary concerns he had about a particular outpatient. As discussed further in this section, knowledge brokering is culturally embedded within the network through informal socialization and learning, which drives a willingness to cross professional boundaries through knowledge brokering to the benefit of patients.
Non-clinicians, such as teachers, elaborated how informal knowledge brokering in the paediatric nephrology network bore scant resemblance to their previous experience of teaching in clinical settings where jurisdictional boundaries and divisional hierarchies were the accepted norm: It can be quite difficult because you have each got your role and it is where your role stops that becomes the shady area. We work closely with the nurses in the dialysis bay and we are always asking them, ‘Is he up to doing this in your opinion as a nurse?’ Or reporting back to them: ‘This child isn’t feeling too good, is there a reason for this?’ That has been very difficult for me in jobs before here, because you might be seen as interfering, but here things are different. (Olive, teacher)
Fourth, formal managerial arrangements complemented these more informal tendencies described above. Meetings were calendared on a regular basis. The meetings comprised a weekly psychosocial meeting and also an amalgamation, during the last meeting of each month, of both psychosocial and clinical updates across the wider network membership. Additionally twice-weekly ward rounds were conducted and then immediately followed up by collective discussion aimed at disseminating the results of the rounds, i.e. case meetings. The commonly shared view regarding the importance of psychosocial input to care empowered non-clinicians to participate credibly within such meetings, and encouraged them to broker knowledge. In line with our SNA findings, our observations of meetings, in tandem with interviews, provide a nuanced understanding of how and why non-clinicians seemed to play more salient roles in brokering knowledge within the network, in particular, the play therapist, the senior youth worker and the educational psychologist. A contributing factor is that non-clinicians appear to have frequent interactions with patients on a daily basis, much more so than doctors in particular, so that the knowledge brokerage enacted by non-clinicians within the context of meetings constitutes giving patients a voice: A massive part of my role has been educating the team about youth work. Just simple things like setting up a ‘youth room’ on the ward. Clinical staff wanted to call it an ‘adolescent room’. Well, the young people [patients] thought it sounded like a punishment room because it’s a very medical term. So I was able to feed their views back to the renal team in meetings, who then understood and supported the idea. (Linda, senior youth worker)
There were very diverse professions and individuals who attended meetings, some of whom were more vocal than others, as evidenced in the preceding analysis. Of note, however, is that although meetings were usually overseen by Pat (lead consultant/unit director), professional domination was not a problem that we observed over the course of study. The structure of all the meetings seemed to mediate this. Pat would go around the room asking the lead from each profession, one by one, for their views; e.g. ‘Right, so Tamara [play therapist], what’s happening with your services? Linda [youth worker], what’s happening with youth work? Christine [psychology], what do you know about this child?’ and so forth. This appeared conducive to facilitating knowledge brokering, especially when it came to individuals or professions that were relatively new: When I first started, I was absolutely petrified of Pat [lead consultant] and the other consultants. I didn’t used to like saying anything at the psychosocial meetings. I would sit, listen and make notes, and then go and see the relevant people afterwards. I didn’t feel confident at first in telling other professions, whereas now I will contribute to the meeting no problem. (Tamara, play therapist)
In the above, we see how the play therapist (Tamara), despite commanding a salient knowledge-broker role as evidenced by our SNA and qualitative fieldwork findings, in both liaison and consultant roles, nevertheless had initial reservations about her professional standing within the network. She admitted that she had to overcome her traditional assumptions of professional hierarchy based upon previous work in other healthcare settings, and that she took time to adapt to the distinctive open knowledge brokerage within the paediatric nephrology network.
However, we highlight that it was not merely the team climate promoted by the lead doctor at the local level which gave rise to a receptive context for knowledge brokering across professional boundaries. There were two significant factors at a more institutional level. First, paediatric nephrology was described as ‘under the radar, and not subject to the sort of intense measurement of outcome that surgeons are bound by … and this gives us space to operate in less visible way, to managers and commissioners, and do things differently’ (Pat, lead consultant, unit director). We cannot assume that all clinical areas are free of such constraint. Second, linked to this, while policy was concerned to structure all clinical areas around a smaller number of ‘centres of excellence’, because paediatric nephrology was ‘under the radar’ the professional body for paediatric nephrology took the lead in reflecting a policy drive that was more pronounced in other areas. Reflecting the actions of the lead doctor above in use of ‘evidence’, the concern of the professional body emphasized ‘patient-focused care’ and quality of service as assessed by the ‘patient experience’, as much as formal evidence, that integration of clinical and psychosocial care was desirable. This, in the words of one the doctors, ‘sold collaborative working on the basis of good professional practice, rather than a policy-driven initiative’ (Len, consultant).
Conclusion
Our empirical case confirms political and cultural challenges of knowledge brokering (Alvesson & Karreman, 2001). In essence, knowledge-brokering roles are influenced by professional hierarchy, particularly in the case of clinical knowledge and even more so with medical knowledge (Freidson, 1994; Larkin, 1983). Consequently, knowledge-brokering roles are enacted in line with professional legitimacy, with medical consultants very visible in the network. On this basis, the advance of policy aimed at mobilizing knowledge across professional boundaries, through workforce reconfiguration, is likely to be resisted by the medical profession (Reed, 1996).
At the same time, we see how social structures might be moderated. We highlight that knowledge brokering may allow less powerful professional groups and individuals to advance their position in the network and/or promote something they value, such as more integrated patient care that encompasses psychosocial knowledge; i.e. knowledge brokering is shaped by, but also enacted to change, power dynamics. In part, this relates to the type of knowledge brokered, with consultant knowledge-brokering roles, which transcend professional hierarchy, enacted with respect to management knowledge, and to some extent psychosocial knowledge (Fernandez & Gould, 1994).
In understanding how social structures might be mediated, our study suggests that knowledge brokering is as much, if not more, a group phenomenon, rather than enacted by individuals. Consequently, we might better talk of ‘knowledge brokerage’ rather than individual knowledge brokers. This may seem to be a semantic point, but it draws attention to how such a group-level phenomenon is engendered, which then allows less powerful professionals to enact knowledge-brokering roles at the individual level.
Situated learning across professional groups is necessary in the delivery of care because problems arise in real time within very specific contexts (Lave & Wenger, 1991) that require integration of clinical and psychosocial knowledge. Group identity appeared strong for those delivering paediatric nephrology services in our empirical case, and this transcended, or at least equalled, professional affiliation. Staff tended to talk about the paediatric nephrology ‘team’, rather than referring to the ‘network’. They gave their time voluntarily to the ‘team’ beyond what might be expected in the everyday routine of their roles. A focus upon the patient, from which arose a distinctive way of working, provided the bedrock for staff identification with a community of practice (Lave & Wenger, 1991); i.e. the network took on a form that tended towards an ideal type of network, which engendered effective knowledge exchange through more distributed knowledge brokerage (Ferlie, Addicott, Exworthy, & Fitzgerald, 2010). What stood out as a feature of the paediatric nephrology network was the acceptance by all staff, including powerful doctors, that all professions and administrators held knowledge that potentially improved quality of care. This allowed for the development of understanding across clinical and psychosocial worlds of others’ perspective. When held together with the glue of a focus upon patients, this provided a powerful driver for collaboration, so that the network was networked. Tagliaventi and Mattarelli (2006) confirm the importance of working side by side and that common organizational values are important bases for knowledge brokering across professional groups. Within this managerial arrangement, knowledge brokers at the individual level developed understanding of different knowledge domains, built effective relationships with others that underpinned knowledge exchange across these domains, and so were able to effectively tailor specialist knowledge for non-specialists (Bowen, Martins, & Need to Know Team, 2005; Dobbins et al., 2009; Landry, Amara, & Lamari, 2001).
In seeking to draw out the organizational and management factors that frame knowledge brokering, we highlight the importance of ‘team atmosphere’ on knowledge outcomes of self-managed teams (Zarraga & Bonache, 2005). First, rather than extrinsic factors such as reward, we show that it is ‘soft mechanisms’ that engender a ‘high care’ environment which, in turn, allows for knowledge brokering across professional boundaries (Zarraga & Bonache, 2005). We highlight the importance of socialization processes that encompass both those relatively high-status actors in inter-professional terms (e.g. junior doctors) and those of relatively low status (e.g. play therapist), which is ‘validated’ through feedback from colleagues and a role model, the team leader, in the formative stages of their career (Pratt, Rockmann, & Kaufmann, 2006). The resultant team atmosphere is one in which social interaction, mutual trust and understanding are evident across professional boundaries, even in the presence of professional hierarchy, in line with workforce development policy initiatives towards integrated healthcare (Bourgeault & Darling, 2008; Bourgeault & Mulvale, 2006; Bourgeault et al., 2008; Buchan & Calman, 2005; Currie et al., 2010a; Davies, 2000; Kuhlmann & Saks, 2008; Sibbald et al., 2004). Second, we also illustrate how the team leader engages in research, which is relatively applied, to produce ‘evidence’ (patient and carer satisfaction surveys) that brokering clinical and psychosocial knowledge to integrate care gives rise to an enhanced patient experience, and so ‘convince’ others in the network to interact across professional boundaries (Pahor, 2008). It is this argument that the ‘quality of patient and carer experience is enhanced’ that drives knowledge brokering, and the lead doctor links this to the need for ‘patient-focused care’, which is encompassed within professional body ‘advice’ that paediatric nephrology teams encompass the necessary clinical and psychosocial dimensions of care. In essence, collaboration is viewed in a positive light, as various professionals embrace change towards more distributed knowledge brokering. Third, regarding formal aspects of the organizational context, we highlight the following as salient: paediatric nephrology is not a mandated network, so it is not as managerialized, for example, as cancer networks where learning and knowledge mobilization appear to be driven out by centralized performance regimes (Addicott et al., 2007). Anyway, in the case of paediatric nephrology, consequences of poor performance are longer-term; e.g. kidney transplant. As such, paediatric nephrology is ‘under the radar’ regarding visible performance, and represents a space in which knowledge brokering across medical, other clinical, psychosocial and managerial domains may be rather more distributed. To emphasize, framed by the organizational and management context above, knowledge brokering appears driven more by notions of what represents ‘good’ professional practice on the ground, as professionals place the patients first (Saks, 1995). In response to policy-driven workforce development, the organizational and management context ensures that exclusionary and more inclusive patterns of professional interaction do not simply coexist, they release new dynamics of knowledge brokering (Kuhlmann, 2008).
Theoretically, our study provides more detail regarding the micro-sociology of internal knowledge brokering (Shi et al., 2009) at the collective level, and elaboration of various knowledge-brokering roles at the individual level identified by Fernandez and Gould (1994). Specifically, our study illustrates the interaction of individual- and collective-level internal knowledge brokerage with institutional context, and the way that group-level characteristics or managerial arrangements facilitate knowledge brokerage.
On the one hand, our study signals how professional claims to a legitimate monopoly on knowledge and jurisdiction interact with resilient institutionalized power differentials to facilitate resistance to any policy and individual-level challenges to the division of labour, and ensure reforms or managerial initiatives reproduce, rather than reconfigure, existing structures of professional control (Martin et al., 2009). This is likely to result in a prevalence of liaison, representation, coordination or gatekeeper knowledge-brokering roles (Fernandez & Gould, 1994).
On the other hand, our study shows that, even in one of most institutionalized contexts, such as healthcare, where professional hierarchy is all-pervasive, social structures may be mediated. Our study reveals that peer-to-peer knowledge brokering, associated with professional legitimacy, is undoubtedly important (Shi et al., 2009), but suggests that the group affiliation that frames this may be a more malleable matter; i.e. we can move beyond occupational affiliation. Thus, we are optimistic about possibilities for knowledge brokering across disparate component knowledge domains, where attention is paid to informal and formal managerial arrangements at the group level as a way of moderating the effect of macro-level social structures; i.e. this represents architectural knowledge that facilitates the integration of component knowledge domains (Balogun & Jenkins, 2003; Finn & Waring, 2006; Galunic & Eisenhardt, 2001; Henderson & Clark, 1990). With respect to group-level managerial arrangements, empirically, our case exhibits characteristics of a community of practice (Lave & Wenger, 1991), with knowledge ‘embedded’ in collective practice that integrates potentially disparate sets of component knowledge. Knowledge brokering requires immersion in practice and rich social interaction so that trust and insight into others’ knowledge domains and practices are engendered (Lam, 1997, 2000). Following the development of architectural knowledge, knowledge-brokering roles such as the consultant role (Fernandez & Gould, 1994) may transcend power differentials.
We thus highlight that individual-level and collective-level knowledge brokering are interdependent, as each facilitates the other; i.e. it is as much, if not more, about the development of collective organizational routines and schema, constituted as ‘management knowledge’, to engender knowledge brokering, rather than the role and position of individual-level knowledge brokers in the professional hierarchy.
Regarding transferability of our analysis, on the one hand, we might perceive our single empirical case as rather distinctive. For example, the climate of the particular team under study is set by a high-status individual, the lead doctor. His orientation towards knowledge brokering might be viewed as contrasting with other clinical settings. Within the latter, high-status individuals do not necessarily encourage knowledge brokering across professional groups, and may seek to protect their jurisdiction (Currie & Suhomlinova, 2006; Ferlie et al., 2005; Waring & Currie, 2009). We have highlighted that paediatric nephrology is less managerialized than other healthcare domains, with some of the latter subject to heightened visibility for poor outcomes, which may limit collaboration across professional boundaries, and concentrate rather than distribute knowledge brokering, as new vulnerabilities impact doctors (Kuhlmann & Saks, 2008). In short, we recognize that there were local-level factors at play. On the other hand, our focal case exemplifies a long-term condition, where clinical and psychosocial knowledge needs to be integrated for patient benefit. So our analysis and prescriptions have wider resonance, for example, to elderly care. Regarding healthcare settings generally, it is characterized by a mosaic of professions arranged more hierarchically than most other contexts, and thus healthcare may represent a distinctive case of patterns and explanations for knowledge brokering. Consequently, we suggest some caution is required in interpreting and applying our analysis beyond our relatively narrow setting. Notwithstanding our note of caution, we suggest our analysis is one that might be applied to other professionalized organizations, both regarding institutional factors, specifically professional power, that might concentrate knowledge brokerage, and ways in which this is moderated (e.g. through co-location, situated interaction, education and socialization of staff to accept the legitimacy of others’ knowledge, all of which engender architectural knowledge to orientate professional staff towards a group affiliation that transcends their silos). Indeed, such challenges and solutions may exist in most firms, where there is occupational differentiation, yet integration of disparate knowledge domains is necessary to deliver a service or product.
This last point provides a springboard for further research. We suggest that more studies on the interaction of knowledge brokering with institutional context are required to empirically ground aspirations for more effective internal knowledge brokering in organizations. Additionally, one of the novel features of our research design was combining SNA with qualitative fieldwork. This has value in that SNA informs the ‘what’ question regarding knowledge-brokerage patterns, while qualitative fieldwork, in conjunction with an organization studies literature, provides richer description and explanation of these patterns. At the same time, SNA may be revealing of knowledge-brokerage patterns, less visible through qualitative fieldwork. For these reasons, we encourage other academics to build mixed methods into studies of knowledge brokering.
Empirical case epilogue
As an epilogue to our fieldwork, and of interest analytically, is that rationalizing tendencies of policy makers and organizational management towards cost savings and more efficient organization of clinical services have come to prominence recently in the more parsimonious climate for public services provision in England. Following formal data collection, and writing up of the case, we revisited the site in early 2011. While not part of our formal data collection, our visit and informal interviews with two key stakeholders revealed that financial cutbacks have impacted the network in such a way as to reduce knowledge brokerage within the network. In particular, brokerage of clinical and psychosocial knowledge across the network appears much reduced as hospital management, in the face of limited resources, concentrates upon clinical care, with some key brokers, such as the play therapist and social worker, no longer funded. On our visit, one of the senior paediatric nephrologists stated: We are driven towards following best practice guidelines from evidence-based medicine. These don’t necessarily encompass some of the important dimensions of our care, which extend beyond medicine, but medicine ‘rules the roost’ when it comes to resource allocation, and to get resource we need to show we are following so-called ‘best practice’.
The statement is particularly revealing for our theoretical analysis. We suggest that our empirical assertions above, which highlight collective-level brokerage, may no longer hold to the same extent, as component knowledge held by the most powerful professional group, doctors, is privileged, and internal knowledge brokering of collective, practice-based knowledge is displaced by external brokering of formal medical knowledge into more individualistic practice in pursuit of legitimacy to obtain the necessary resource to sustain service. The extent to which collective brokerage is resilient over time appears questionable in our empirical case.
Footnotes
Notes
Funding
This project was funded by the National Institute of Health Services and Delivery Research (NIHR HS&DR) programme (project number 08/1718/149). Visit the HS&DR website for more information.
Department of Health disclaimer
The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the HS&DR programme, NIHR, NHS or the Department of Health.
Author biographies
Graeme Currie is Professor of Public Management at Warwick Business School. He researches organizational change in healthcare and other public services settings, focusing upon issues of knowledge mobilization, leadership, workforce development and translation of innovation. Current funded research examines the role of middle-level managers in brokering knowledge to ensure high-quality elderly care. Prior to becoming an academic, he worked in organization development roles within the English NHS and the UK car manufacturer, Rover.
Leroy White is Professor of Management in the Department of Management, University of Bristol. His main research interests are operational research, problem structuring methods, social network analysis, strategic partnerships, large group decision-making, public and community involvement, third sector and health services management. His current funded research work is upon the impact of the third sector.