
Abstract
Child care arrangements, costs, and satisfaction among parents of children with emotional or behavioral disorders were examined as compared with parents of children with other disabilities. The current study used a large, nationally representative, and community-based sample of approximately 3,000 parents of children with disabilities aged 3 to 5 years. Results indicate that parents of children with emotional or behavioral disorders did not appear to have significantly different types of child care arrangements or levels of satisfaction with these arrangements as compared with parents of children with other disabilities. Parents of children with emotional or behavioral disorders did appear to spend significantly more on child care as compared with parents of children with other disabilities. Parents of children with emotional and behavioral disorders spent $570 a year as compared with children with other disabilities. The overarching implication for policy would appear to be that special child care subsidies or more publicly fund child care services for parents of children with emotional or behavioral disorders should be provided.
Work and family obligations can be difficult for any parent to balance. For parents of children with disabilities, this balance can be even more difficult to achieve such that parents may have to adjust work and family obligations with respect to the particular needs of a child with a disability (Montes & Halterman, 2008). A pivotal component of achieving work and family balance for all parents is finding appropriate and affordable child care yet finding this child care can be a challenge for parents of children with disabilities (Reichman, Corman, & Noonan, 2008). Appropriate child care is difficult to find as children with disabilities often require special and multifaceted services (Reichman et al., 2008). Affordable child care can be equally difficult to find as parents of children with disabilities earn less income on average (Montes & Halterman, 2008). Additionally, parents have reported their employment decisions as being greatly affected by having a child with a disability (Knoche, Peterson, & Edwards, & Jeon, 2006). Findings from the National Institute for Child Health and Human Development (2005) study of early child care echo extant literature by extension indicating that mothers of children with disabilities delay reentry into the work force and their children spend less hours in care. Given the limited research comparing care for children with and without disabilities, this lack of literature precluded locating research that further dissected differences such as according to ethnicity.
For parents of children with emotional- or behavioral-related disabilities, the issue of finding appropriate and affordable child care can be compounded by the nature of their child’s disability, which may affect interactions with caretakers and other children in the child care setting. For example, research has indicated that prekindergarten programs that are publicly funded expel children with behavioral problems at higher rates as compared with other children (Gilliam & Shahar, 2006). While rates at private child care facilities are unknown, these rates are estimated to be higher as expulsions at these facilities are not subject to the same restrictions as publicly funded facilities (Montes & Halterman, 2008) and the fact that parents of these children have indicated a lack of inclusive child care settings (Knoche et al., 2006). In qualitatively examining work and family obligations of parents of children with emotional or behavioral disorders specifically, Rosenzweig, Brennan, and Ogilvie (2002) found, “a serious lack of community-based services and resources necessary to support work and family obligations in a meaningful way” (p. 415). We review the literature discussing types of child care arrangements, parental satisfaction with these arrangements, and costs associated for parents of children with disabilities, specifically in relation to children with emotional- and behavioral-related disabilities when available. We consider types of and parental satisfaction with child care arrangements to be components related to the appropriateness of child care that can be readily measured while costs to be associated with the affordability of child care in view of household income.
Parental satisfaction would appear to be a salient indicator of whether child care may be considered appropriate also. In a review of the literature, Knoche et al. (2006) noted that child care is often mediocre at best in a majority of centers serving children both with and without disabilities. However, in their own study, Knoche et al. (2006) found quality ratings to be quite high and differences in quality ratings between parents of children with and without disabilities as not being statistically significant. It should be noted, however, that there are varying definitions of quality. Parents may prioritize different criteria when selecting a child care arrangement, thus any measure of quality may be more related to satisfaction with individually developed criteria. Gamble, Ewing, and Wilhlem (2009) reported that parents appear to describe quality based on what they value in a child care arrangement and often what they value is based on their individual child’s needs or their own personal preferences. For instance, Gamble et al. (2009) revealed that parents who reported their children as having more difficult temperament traits were less likely to value school readiness or curriculum options in their child care arrangement(s). Gamble et al. highlighted the complexity that surrounds the decision making process and how satisfaction with child care arrangement(s) may be how parents perceive quality based on their needs and the needs of their child. Thus, the idea of satisfaction and quality are often intertwined in the eyes of parents and satisfaction is often linked to variables, such as cost, location, and convenience (Gamble et al., 2009).
The issue of cost of child care is directly related to the affordability of child care when considering household income. With cost as a factor for all parents in obtaining child care, parents of children with disabilities have additional issues to consider when considering cost with costs of child care generally being higher (Parish & Cloud, 2006). Knoche et al. (2006) reported that parents of children with disabilities tended to have less disposable income even though they were working longer hours as compared with parents of children without disabilities. Higher socioeconomic status has been indicated to mediate the stress related with raising a child with a disability while mothers from higher socioeconomic strata tended to be more knowledgeable about social services available in the community to support working families (Keller & Honig, 2004). Parents of children with disabilities did tend to pay lower fees for child care when compared with parents of children without disabilities as associated with the use of child care subsidies (Knoche et al., 2006). However, there is great variability in the accessibility of child care subsidies that may be a function of a constellation of factors, including but not limited to location of residence, household income, and type of disability (Anderson, Dumont, Jacobs, & Azzaria, 2007).
The purpose of the current study was to examine child care received by parents of children with emotional or behavioral problems as compared with parents of children with other disabilities. In examining this child care, the current study used a large, nationally representative, and community-based sample of parents of children with disabilities aged 3 to 5 years. While children with emotional or behavioral disorders were of particular interest in the current study given the paucity of research for these children (Rosenzweig, Brennan, Huffstutter, & Bradley, 2008), children with other types of disabilities were employed as a comparative group. As most child care facilities are already obligated to have American with Disabilities Act–compliant facilities, which are inspected on at least an annual basis, thus children with physical or sensory disabilities would ostensibly require no further accommodation in child care settings. The current study augments previous research by examining the child care received by parents of children with emotional or behavioral disorders in view of parents of children with other types of disabilities using a large, nationally representative, and community-based sample. Discerning whether parents of children with emotional or behavioral disorders do actually appear to pay more than parents of children with other disabilities is critical in the development of policy as all children with disabilities should not be considered the same in seeking and maintaining child care. To achieve the purpose of the current study, three research questions were examined. First, we examined whether parents of children with emotional or behavioral disorders had significantly different types of child care arrangements than parents of children with other disabilities. We hypothesized that children with emotional or behavioral disorders would not necessarily have different child care arrangements, but this may impact child care costs thus should be examined. Second, we examined whether parents of children with emotional or behavioral disorders spent significantly more on child care than parents of children with other disabilities. We hypothesized that parents of children with emotional or behavioral disorders would spend significantly more on child care than parents of children with other disabilities. Third and finally, we examined the child care satisfaction of parents of children with emotional or behavioral disorders as compared with parents of children with other disabilities. We hypothesized that parents of children with emotional or behavioral disorders would indicate less satisfaction with child care as compared with parents of children with other disabilities.
Method
Sample
The Pre-Elementary Education Longitudinal Study (PEELS) consists of approximately 3,000 children with disabilities aged 3 to 5 years receiving special education services and was designed to provide a nationally representative sample of preschool-aged children eligible for special education services in the United States. Specifically, children with Individualized Family Service Plan thus eligible to receive special education services across the nation provided the sampling frame with approximately 1,000 children in each age cohort (e.g., 3-, 4-, and 5-year-olds) eligible to receive special education services sampled (Carlson, Posner, & Lee, 2008). The average age in the sample as of the first wave of data collection was 55.43 months old with a standard deviation of 9.76 months. All individuals with comorbidities were removed from analysis as the presence of these comorbidities would confound results. Table 1 provides the descriptive statistics for the sample.
Descriptive Statistics.
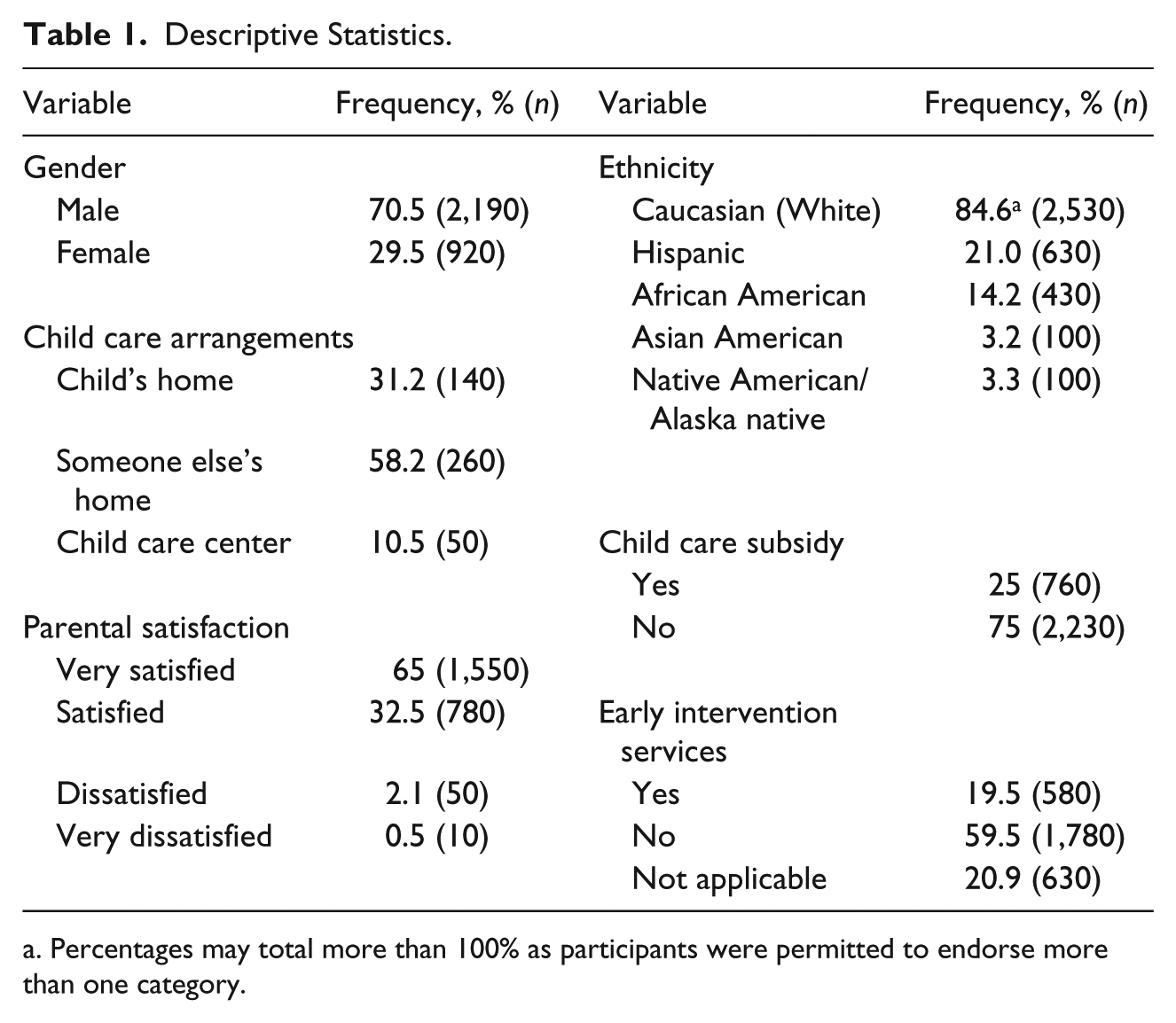
Percentages may total more than 100% as participants were permitted to endorse more than one category.
With regard to having an emotional- or behavioral-related disorder, children having a diagnosis of attention deficit hyperactivity disorder (ADHD), autism, or other emotional/behavioral disorder as reported by the parent and confirmed by school information were considered as an emotional- or behavioral-related disorder for the purposes of the current study. The three disabilities were selected based on the fact that each disability commonly results in the manifestation of problem behavior and the diagnostic criteria for each disorder include the presence of some form of challenging behavior. First, ADHD was included because the diagnostic criteria for ADHD includes several symptoms of problem behaviors, including reluctance to engage in work tasks, difficulty listening when spoken to, running and climbing excessively, talking excessively, acts of impulsivity, and often interrupting or intruding on others according to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.) criteria (DSM-5; American Psychiatric Association, 2013). Each of these behaviors could be considered challenging, particularly in child care facilities in which large groups of children must be managed. In fact, the emotional and behavioral problems presented by children with ADHD have resulted in half of children with ADHD being provided special education under the Individuals with Disabilities Education Act classification of emotional disturbance (Reid, Maag, Vasa, & Wright, 1994; Schnoes, Reid, Wagener, & Marder, 2006). Additionally, previous studies regarding child care needs for children with emotional and behavioral disorders have also included children with ADHD (e.g., Rosenzweig et al., 2002; Rosenzweig et al. 2008). Second, autism spectrum disorder was included because restricted repetitive and stereotyped pattern of behavior is one of the two core diagnostic domains of autism according to DSM-5 criteria (American Psychiatric Association, 2013). Moreover, impairments in communication is a second diagnostic domain of autism, which increases the presence of additional challenging behavior as there is an inverse relationship between communication skills and challenging behavior (Sigafoos, 2005). Commonly reported challenging behaviors among children with autism, include self-injury, physical aggression, elopement, verbal aggression, property destruction, and disruptive behavior (Sigafoos, Arther, & O’Reilly, 2003). Third, the IDEA definition as well as DSM-5 criteria of emotional/behavioral disorders also includes the presence of inappropriate behaviors and the inability to maintain satisfactory interpersonal relationships, which could be viewed as problem behavior in a child care setting. Problem behaviors associated with children with emotional disturbance include defying authority, disturbing others, aggression, and difficulty sharing and playing with others (Hardman, Drew, & Eagon, 2010). In short, we included children with ADHD, autism, and emotional/behavioral disorders as these disorders have emotional and behavioral problems related to them by their own diagnostic criteria per the DSM-5 and results of empirical research as cited above.
Approximately 110 (≈ 4%) of these children had diagnoses of ADHD, 210 (≈ 7%) of these children had diagnoses of autism, while approximately 150 (≈ 5%) of these children had a general diagnoses of emotional disturbance or behavior disorder. In their review of the literature, Brauner and Stephens (2006) estimate that anywhere from 5% to 26% of children have an emotional or behavioral disorder, which is in keeping with the current study. The remaining sample of children may be considered as not having an emotional and behavioral disorder but having rather some other disability out of approximately 40 different categories identified in the PEELS that ranged from asthma to visual impairment. There were no statistically significant differences in the demographic characteristics between children with emotional or behavioral disorders and compared with other children with disabilities.
Measures
Each research question had corresponding measures. All measures from the PEELS used in the current study were collected from questionnaires completed by parents. To answer the first research question, parents were asked to identify the child care arrangement without a parent or guardian present that their child spends the most time, in which there were three choices that a parent could endorse—child’s home, someone else’s home, and child care center. Throughout the rest of the PEELS, this child care arrangement is referred to as the primary child care arrangement. To answer the second research question, parents were asked the amount they spent in dollars on this primary child care arrangement and according to which unit indicating the frequency of payment. For instance, a parent could respond with the amount of $75 and then respond this unit as being “per week.” Thus, child care costs were converted to the common metric of US dollars per day for the purposes of analysis. For this variable of dollars spent per day on primary child care arrangement, there was a mean of $10.28 with a standard deviation of $4.97. We should note that a number of parents received child care subsidies, which decreased the cost of child care out of pocket. For the third and final research question, parents were asked to rate their satisfaction with this child care arrangement along a 4-point, forced choice format as being: “very satisfied,” “satisfied,” “dissatisfied,” or “very dissatisfied.”
Analyses
The amount of missing data was minimal and did not appear to influence results of the current study as this missingness was considered MCAR (e.g., missing completely at random) according to the variables in the current study. To answer the first research question, we performed a 2 × 3 chi-square goodness-of-fit test to examine whether parents of children with emotional or behavioral disorders had significantly different child care arrangements than parents of children with other disabilities. If statistically significant, a phi (Φ) coefficient was calculated as the measure of effect size. Phi coefficient values of .10, .30, and .50 or larger may be viewed as small, medium, and large, respectively. To answer the second research question, we performed a one-way analysis of covariance where we statistically controlled for household income and whether the child received medication to control mood or behaviors. There did not appear to be a relationship of either household income or medication status of the child with types of child care arrangements so we did not control for these variables in the first research question. By collapsing two variables, the variable of household income was statistically controlled for in examining the second research question. The two original variables measured household income less than $25,000 and more than $25,000 to more than $50,000, respectively. We also statistically controlled for whether the child received medication to control for mood or behavior as parents of children with emotional or behavioral disorders were significantly more likely to report their child taking a medication to control mood or behavior (dichotomous variable of yes or no) as compared with parents of children with other disabilities, χ2(1) = 120.8, p < .001, Φ = .20. Further analyses indicate that even when controlling for household income, parents whose children were medicated to control mood or behavior (M = 12.34, SD = 4.96) spent significantly more per day on child care than parents whose children were not (M = 10.25, SD = 4.97), F(1, 2,900) = 7.536, p < .01, d = .42. Thus, we decided to control for medication use as well as household income in examining the second research question. For the third and final research question, we performed a 2 × 4 chi-square goodness-of-fit test to examine child care satisfaction of parents of children with emotional or behavioral disorders as compared with parents of children with other disabilities. There did not appear to be a relationship of either household income or medication status of the child with parental satisfaction so we did not control for these variables in the third research question.
Results
In examining the first research question, we found that parents of children with emotional or behavioral disorders did not appear to have significantly different child care arrangements than parents of children with other disabilities, χ2(2) = 1.57, p = .46. Children with emotional or behavioral disorders did not have significantly different child care arrangements than children with other types of disabilities in terms of being in the child’s home, someone else’s home, or a child care center. Household income, child’s age, nor ethnicity/race was significantly associated with the type of child care arrangements that a parent of a child with an emotional or behavioral disorder.
In examining the second research question, there were significant differences in the child care costs between parents of children with emotional or behavioral disorders and parents of children with other disabilities, F(1, 2,900) = 30.49, p < .001, d =.32. This Cohen’s d value indicates that a medium effect size (Cohen, 1988). Parents of children with emotional or behavioral disorders (M = 11.66, SD = 4.94) spent significantly more on child care than parents of children with other disabilities (M = 10.08, SD = 5.02). In conducting these analyses, we statistically controlled for household income as we reasoned that parents with more disposable income would ostensibly spend more on child care, which there was a small statistically significant association between these variables, r = .109, p < .05. We also statistically controlled for whether the child received medication to control mood or behavior as mentioned previously. From these data, we calculated that parents of children with emotional or behavioral disorders were paying on average $570 more a year than parents of children with any other type of disability. Neither child’s age nor ethnicity/race was significantly associated with child care costs between parents of children with emotional or behavioral disorders and parents of children with other disabilities.
In answering our third and final research question, we examined child care satisfaction among parents of children with emotional or behavioral disorders as compared with parents of children with other types of disabilities. Parents of children with emotional or behavioral disorders did not appear to differ significantly in their satisfaction with child care as compared with parents of children with other types of services, χ2(3) = 3.16, p = .37. This finding is interesting as it appears that parents of children with emotional or behavioral disorders spend more on child care than parents of children with other types of disabilities but are not any more or less satisfied with the services they receive. This finding could be interpreted that all parents of children with disabilities are equally satisfied with their child care arrangements as indicated by the vast majority of parents (97%) endorsing being “satisfied” or “very satisfied” with their child care arrangements. It should be noted that this question appears to be very general in measuring parental satisfaction with child care arrangements. Household income, child’s age, total dollars spent per day on child care, nor ethnicity/race was significantly associated with the satisfaction of a parent of a child with an emotional or behavioral disorder regarding child care.
Discussion
The results of the current study augments the findings of Rosenzweig et al. (2008) by examining child care arrangements in view of the type of child care arrangement, its cost, and parental satisfaction with these arrangements using a large, community-based, and nationally representative sample. The current study explores these issues surrounding, obtaining, and maintaining child care (e.g., arrangements, cost, and satisfaction) among parents of children with emotional or behavioral disorders as compared with parents of children with other disabilities. This study examining parents of children with emotional or behavioral disorders is especially important given the extensive breadth and depth of disability in the human experience (Vash & Crewe, 2004). Thus, individuals with disabilities and their needs are difficult to aggregate and be treated as a composite.
Interestingly, the results of the current study indicate that parents of children with emotional or behavioral disorders did appear to spend significantly more on child care as compared with parents of children with other disabilities. While much literature has found that raising a child with a disability to be more expensive than a child without a disability (Anderson et al., 2007; Parish & Cloud, 2006; Porterfield, 2002), this research only examined children with disabilities as an aggregate. The current study examined the child care costs of parents of children with emotional or behavioral disorders in particular as compared with parents of children with other disabilities. We consider our results to indicate the heightened economic burden experienced by parents of children with emotional or behavioral disorders as compared with parents of children with other disabilities and parents of children without disabilities.
Although our study did not find statistically significant differences in parental satisfaction, satisfaction with child care arrangements is a multidimensional concept and may be considered complex. For instance, parental satisfaction has been indicated as having a relationship with both the number of children in a parent’s care and the severity of the disability of these children (Brennan & Brannan, 2005). The complexity of this relationship of parental satisfaction with other intervening and confounding variables should be examined in future research. While the results of the current study indicate that parents of children with emotional or behavioral disorders have similar levels of satisfaction with child care arrangements when compared with parents of children with other disabilities, the complexity of child care arrangements across parents of children with disabilities cannot be underestimated. With Rosenzweig et al. (2008) finding that child care serves as a limiting factor for employment among parents of children with disabilities, it is a positive sign to find that parents in this nationally representative and community-based sample do not appear to be experiencing significantly different levels of satisfaction when compared with parents of children with disabilities not having emotional and behavioral disorders. Thus, results indicate that while parents of children with emotional or behavioral disorders may experience higher costs associated with care, this finding does not translate into significantly different level of satisfaction with child care arrangements as compared with parents of children with disabilities other than emotional or behavioral disorders.
More objective measures of child care quality other than parental satisfaction such as the ECERS-R (Early Childhood Environment Rating Scale–Revised; Harms, Clifford, & Cryer, 2004), FCCERS-R (Family Child Care Environment Rating Scale–Revised; Harms, Cryer, & Clifford, 2007), and the SACERS-R (School Age Care Environment Rating Scale–Revised; Harms, Jacobs, & White, 1996) should be considered. These instruments would provide context to parental estimates of satisfaction with child care arrangements. The Inclusive Classroom Profile (Soukakou, 2012) would appear particularly applicable as it measures settings in relation to children with disabilities but appears to be address children with disabilities as an aggregate.
The results from the current study do indicate that parents with children with emotional and behavioral disorders in this sample did experience higher child care costs than parents of children with other disabilities. When considered in relation to the growing number of preschool-aged children diagnosed with emotional and behavioral disorders (Egger & Angold, 2006), this finding becomes more practically significant with implications for policy. As previous research has indicated a need for government policies aimed at reducing the cost and increasing the availability of high-quality child care for lower income families with children with any disability (Parish & Cloud, 2006), the results of the current study indicate that this is an even more significant issue for families with children with emotional or behavioral disorders. We suggest three factors that may explain why parents of children with emotional or behavioral disorders may experience higher child care costs: (1) child care providers may demand higher compensation for care of a child with an emotional or behavioral disorder (e.g., in the form of an aide or extra activities); (2) parents may be seeking higher cost child care in order to serve the needs of their child speaking to the issue of appropriate child care (Anderson et al., 2007; Booth-Laforce & Kelly, 2004); or (3) some combination of these two aforementioned factors. For instance, a child care center that provides specialized or individuated services to children with special needs such as emotional or behavioral disorders may simply charge more and parents of children with emotional or behavioral disorders may specifically seek out this care to assist their child. Parish and Cloud (2006) indicated that inclusive child care centers were significantly more likely to be of higher quality than those child centers that were not inclusive, which would in turn be more expensive. We suggest that this combinational approach may best explain why parents of children with emotional or behavioral disorders experience higher costs than parents of children with other disabilities.
With that said, the National Association of Child Care Resource and Referral Agencies (NACCRRA) has reported more than 24 million children younger than 6 years are potentially in need of child care. Parents of children with and without disabilities must choose between regulated child care, such as licensed child care centers or family child care homes; and unregulated child care, such as relative care or babysitters. There are advantages and disadvantages to all types of child care arrangements. For instance, the advantage of unregulated child care can be that it is often considerably less expensive than regulated care (Blau & Mocan, 2002), but to its disadvantage, it can leave parents without a system of accountability or standards of what to expect from their child care. In choosing the type of child care arrangement, cost can appear to be the final determining factor for many families (Blau & Hagy, 1998; Brandon, 1999; Brandon & Hofferth, 2008; Van Horn, Ramey, Mulvihill, & Newall, 2001).
Additionally, certain disabilities, such as emotional or behavioral disorders, may have a certain stigma associated with them. Smart (2009) has noted that individuals with emotional or behavioral disorders often experience the most negative attitudes or highest levels of stigma from individuals without disabilities as compared with individuals with other disabilities. Thus, child care providers, who often care for multiple children, may steer parents of children with emotional or behavioral disorders away from their services because of their own negative attitudes or perceived negative attitudes that they may experience from parents of other children in their care. The issue of perceived liability may also arise for child care providers in terms of what if a child with an emotional or behavioral disorder injures or destroys property of another child. The child care provider may be considered negligent for not meeting a satisfactory duty of care necessary for a child with an emotional or behavioral disorder to protect the individual child and those individuals around the child. Thus, parents of children with emotional or behavioral disorders may be precluded from less expensive forms of care based on the stigma associated with emotional or behavioral disorders. Future research should examine the underlying mechanisms behind this phenomenon.
Several limitations emerged as part of conducting the current study. The first limitation centers on information regarding the quality as externally evaluated by governmental or accrediting agencies. For instance, we did not have information as to whether child care facilities were NAEYC (National Association for the Education of Young Children) accredited, which specifically addresses children with disabilities. Criteria from NAEYC and other licensing/accrediting bodies for child care such as the state may be considered as supplementing compliance with basic federal law concerning individuals with disabilities such as the Americans with Disabilities Act. Additionally, future research may also consider exploring the issues of quality as associated with child care arrangements for children with emotional and behavioral disorders from the perspective of parents and child care providers as the field appears to be mixed with regards to the construct of parental satisfaction. A qualitative approach to studying this issue could provide greater depth to the results found in quantitative studies such as the current study. In particular, a qualitative approach could be used to examine the decision-making process of parents of children with emotional or behavioral disorders with respect to the issue of cost. Given that 10.5% of these children were at a child care center, future research should also consider examining the perceptions of child care centers among parents of children with emotional or behavioral disorders as compared with parents of children with other disabilities.
Another limitation concerns the lack of information as to the perceptions of child care providers regarding children with emotional or behavioral disorders should also be examined to further deconstruct why parents of children with emotional or behavioral disorders experience higher costs as compared with parents of children with other disabilities. Parental perceptions of satisfaction though can be equally limiting to the current study as quality is relative and few parents would be willing to admit that their child has less than satisfactory child care. Another limitation concerns the examination of differences in child care arrangements, satisfaction, and cost according to ethnicity. There was not a sufficient distribution of sample size according to each ethnic group to permit these analyses. Also, we did not have information regarding child care arrangements for nondisabled or typically developing children as there were no typically developing, nondisabled children in the PEELS data set. Additionally, we did not have information on whether the child is participating in psychosocial (i.e., therapy) interventions as part of the PEELS, which presents itself as a limitation to the current study. Finally, patterns for nonresponse in the current study should be examined with respect to individual and state/local education agency–level participation in the PEELS to discern whether these groups responding and not responding may be considered homogeneous. If these two groups are not homogeneous, then the question becomes whether results of the current study may be biased. Future research should also consider examining our research questions in view of state-level characteristics such as political climate and its impact on child policy for parents of children with emotional or behavioral disorders, which may be considered a limitation of the current study. Finally, the interaction between ethnicity and disability would be interesting to examine for future research but the lack of sufficient sample size across cells precluded this analysis.
In conclusion, using a nationally representative and community-based sample of parents of children with emotional or behavioral disorders, the current study examined factors regarding type of child care arrangement, parental satisfaction, and its cost as compared with parents of children with disabilities other than emotional or behavioral disorders. In reviewing extant literature, we could not locate an article that discriminated by disability type as compared with other disabilities in terms of cost, arrangements, and satisfaction. The current study focuses on children with emotional and behavioral disorder as compared with children with other disabilities. We consider our findings to be unique and potentially influential to policymakers in determining the allocation of child care subsidies. Policy makers should not consider all children with disabilities equally when determining the allocation of child care subsidies as child care for children with some disabilities appear to warrant higher costs.
Key messages:
Parents of children with emotional and behavioral disabilities appear to pay more as compared with parents of children with other disabilities.
Parents of children with emotional and behavioral disabilities did not have different arrangements as compared with parents of children with other disabilities.
Parents of children with emotional and behavioral disabilities did not have different levels of satisfaction as compared with parents of children with other disabilities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.