
Abstract
Families formed through multipartner fertility, where children with a common biological mother were conceived by different biological fathers, represent a growing share of all families in the United States. Using data from four waves of the Fragile Families Child and Wellbeing Study (N = 3,366), I find that women who have engaged in multipartner fertility are more likely to experience parenting stress and depression compared with mothers whose children share the same biological father. Mothers’ depression is explained in the short term by poor relationship quality with the father of her prior children and in the longer term by indicators of boundary ambiguity in complex families. Mothers’ parenting stress was only weakly explained by variation in perceived kin support, father involvement, or boundary ambiguity.
Families formed through multipartner fertility, where children with a common biological mother were conceived by different biological fathers, represent a growing share of all families in the United States. In one study of children born in large U.S. cities, more than one third of births occurred to parents, where the mother or father had at least one child with a previous partner (Carlson & Furstenberg, 2006) and administrative data from Wisconsin show that 60% of firstborn children with unmarried parents had at least one half-sibling through their mother or father by age 10 (Cancian, Meyer, & Cook, 2011). Complex family formation through multipartner fertility reflects the dynamic nature of contemporary family structure in the United States: Nonmarital childbearing, cohabitation, union dissolution, and remarriage have increased the likelihood that women will bear children with more than one romantic partner during their lifetime.
I consider whether women in complex families characterized by multipartner fertility are more likely to experience compromised well-being relative to mothers whose children share the same biological father on two dimensions: parenting stress and depression. The expectation that maternal well-being will be compromised by family complexity emerges from family stress theory (Boss & Greenberg, 1984; Hill, 1949; McCubbin & Patterson, 1982). Family stress theory posits that stressful events that occur within or outside of a family system are potentially destabilizing to a family’s equilibrium. The resources and coping strategies available to individuals and families shape how they adapt in response to those stressful events. In this case, the entry of a new child into a household through birth or new union formation represents a potentially stressful and destabilizing event to parents and prior children (Belsky & Kelly, 1994; Miller & Myers-Walls, 1983). Family stress theory would predict that the entry of a new child through multipartner fertility will disproportionately challenge mothers to adapt to family disequilibrium if mothers in complex families have fewer resources and a narrower set of coping strategies compared with mothers whose children share a biological father. In particular, mothers’ adaptation to complex family formation may be compromised because of diminished involvement by the biological father of prior children following the birth of a new child, lower kin support, and more role ambiguity in complex families compared with nuclear families or families where the children of an unpartnered mother share a biological father.
Data come from the Fragile Families and Child Wellbeing Study, a longitudinal study of children born in large U.S. cities between 1998 and 2000 and their parents. Complex families are defined here as those where a mother reports being pregnant or having had another birth with a different biological father by the time the focal child is 3 years old. These families may or may not include other children a spouse or romantic partner brings to a union. Mothers in complex families are compared with mothers who have had no other children or whose subsequent children share the focal child’s biological father when focal children are 3 years and 5 years old to assess the short- and long-term effects of complex family formation. I use the term “complex family” throughout the article to refer to families where a mother has children who do not share a biological father, regardless of whether the mother is actually partnered with the father of any of her children at any wave in the study.
Background
Childbearing in Complex Families
For mothers, the first years of child rearing are regarded as physically taxing but emotionally rewarding and socially validating (Edin & Kefalas, 2005; Nelson, 2009). Despite being a normative life stage, the largely private process of adapting to family formation is often stressful. Pregnancy intendedness, expectations about motherhood, relationship quality with a child’s biological father, and a mother’s physical and emotional health condition her response to pregnancy and child rearing (Belsky & Kelly, 1994; Dew & Wilcox, 2011; Nelson, 2009). Income, physical and psychological health, institutional resources, and social support provide means to cope with associated stressors (McCubbin & Patterson, 1983).
The absence of normativity regarding multipartner fertility in itself potentially makes the event more stressful than higher parity births shared with a single partner (McCubbin & Patterson, 1983). Furthermore, a mother may have diminished access to resources that enable her to effectively manage potential stressors associated with raising two or more children. While multipartner fertility is recognized as an increasingly frequent context for family growth, societal expectations and formal institutional standards that define roles and responsibilities in complex families are only beginning to emerge. New fathers’ responsibilities toward a mother’s other children, a former partner’s perception about his relevance in his child’s growing new family, and a mother’s perception of the support she may rely on from extended kin related to each biological father are examples of how multipartner fertility complicates the transfer of resources to mothers. Here, I evaluate father involvement, kin support, and the presence or absence of role ambiguity in complex families as indicators of resources that are available to mothers adapting to multipartner fertility.
Father Involvement in Complex Families
A variety of studies have documented that nonresident father involvement is related to mothers’ as well as children’s well-being. First, cooperative coparenting is associated both with fathers’ stronger ties with children (Sobolewski & King, 2005) and with lower maternal stress and better mental health (Carlson & Hognas, 2010). Second, nonresident fathers’ provision of formal or informal child support is a consistent predictor of future father–child contact and children’s cognitive development and academic performance (Argys, Peters, Brooks-Gunn, & Smith, 1998; King, 1994; Nepomnyaschy, 2007). The additional household income provided by child support also potentially improves mothers’ mental health and reduces parenting stress by improving material conditions.
While nonresident fathers have less involvement with biological children and more negative coparenting relationships with mothers compared with coresidential fathers (Argys et al., 1998; Furstenberg, 1995; Sobolewski & King, 2005), there is substantial within-group variation (Cheadle, Amato, & King, 2010). In particular, father involvement, represented by time investments and instrumental support provided to children and child support payments to mothers, is more likely to decline when either parent repartners compared with when both parents remain single, and is more influenced by mothers’ than fathers’ new relationship formation (Tach, Mincy, & Edin, 2010). Explanations for diminished nonresident father involvement when a mother has repartnered include fathers’ uncertainty about their roles in children’s lives when a new coresident social father begins caregiving (Guzzo, 2009; Townsend, 2002), maternal gatekeeping (Fagan & Barnett, 2003), changes in the quality of the parental relationship (Carlson, McLanahan, & Brooks-Gunn, 2008; Ryan, Kalil, & Ziol-Guest, 2008; Sobolewski & King, 2005), and fathers’ apprehension about potentially supporting nonbiological children in a new blended family (Cancian & Meyer, 2010).
Kin Support
Kin support is defined as access to instrumental, economic, and emotional support from relatives who may be related by blood, marriage, or marriage-like relationships (Rossi & Rossi, 1990). Examples of kin support include financial gifts or loans, free or reduced-cost child care and housing, job-seeking assistance, and transportation. For mothers, access to kin support is associated with increased employment (Angel & Tienda, 1982; Harknett, 2006) and reduced hardship (Henly, Danziger, & Offer, 2005), and the perception that one has sufficient kin support is associated with mothers’ greater optimism and lower depression (Taylor, Seaton, & Dominguez, 2008) compared with mothers who lack adequate kin support.
Access to kin support is expected to be lower in complex families compared with families with two biological parents or a single mother. Using longitudinal data from the Fragile Families and Child Wellbeing Study, Harknett and Knab (2007) reported that mothers’ perceived kin support decreased after having a child with a new partner. The authors concluded that although multipartner fertility connected mothers to multiple kin networks through the fathers of their children, those networks were either more diffuse or were characterized by greater boundary ambiguity in which patterns of responsibility and reciprocity were less clearly articulated compared with other systems of family organization. These findings inform the expectation that diminished kin support may contribute to mother’s compromised emotional well-being in families characterized by multipartner fertility.
Role Ambiguity in Complex Families
For mothers, biological fathers, and social fathers, complex family organization introduces uncertainty about roles, relationships, and responsibilities to each other and to children (Cherlin, 1978; McLanahan, 2010). Such boundary ambiguity represents an increasingly salient variable in applications of family stress theory (Boss & Greenberg, 1984; Stewart, 2005). When a mother has a child with a new partner, she must negotiate a host of changing dynamics within the reconstituted family, particularly where the new partner becomes a social father to her older children. First, the biological father may become less certain of his role and identity when a new father figure assumes his former responsibilities (Guzzo, 2009). Second, the social father may introduce competing ideas about child rearing or provide different levels of care for his biological children compared with nonbiological children in the household. Third, a mother’s relationship with her older children may change in response to her new caregiving responsibilities as well as the management of her relationship with their biological father and the father of her youngest child.
Demographic and Social Correlates of Multipartner Fertility
Women engaged in multipartner fertility are more likely to be materially disadvantaged than women whose children share a biological father, a set of circumstances that may exacerbate the strain of interpersonal dynamics in complex families. Among mothers in large U.S. cities, those whose children do not share a biological father are significantly more likely to have more children, to be Hispanic or African American (vs. non-Hispanic White), to have been 18 years old or younger at their child’s first birth, and are less likely to be married at their most recent birth (Carlson & Furstenberg, 2006). Mothers who have conceived by multiple partners are also more likely to have partnered with a man who also went on to have more children, potentially reducing the material and time investments he is able to make in the children they share (Cancian et al., 2011). Women who have experienced multipartner fertility also may be more disadvantaged in terms of socioemotional resources to start with. Turney and Carlson (2011) found that among mothers, depression was unrelated to prior multipartner fertility in fixed-effects models (but was related in random-effects models), and depression observed at one point predicted later multipartner fertility, suggesting a reciprocal relationship between maternal well-being and childbearing context.
Long-Term Effects of Family Stress
Early formulations of family stress theory hypothesized that the impact of a stressful event like the addition of a child to a family would recede with time as families used available resources to cope with the stressor and to adapt to a changed environment (Hill, 1949). Under that formulation, referred to as the ABCX model, maternal well-being in the context of multipartner fertility would be most compromised shortly after a child’s birth, and would rebound over time. This theoretical model has been empirically supported by research on the consequences of divorce, which has demonstrated that parents and children recover from family structure change within 2 years of the event (Hetherington & Kelly, 2002).
However, later considerations of the family stress model focused on the aftermath of a stressful event have posited that stressors may occur in contexts where families have already experienced prior strain and where the family may experience new stressors as a consequence of the initial stressor (McCubbin & Patterson, 1983). As a result, a family’s ability to respond to a stressor may be compromised by cascading changes in circumstances that follow. Under that scenario, the stress of a normative event like childbearing may compound over time if the resources available to respond are already absent or are diminished in the context of multipartner fertility and indicators of strain would become more apparent with time. This alternative specification is referred to as the Double ABCX model. The Double ABCX model was initially developed to interpret variation in how families responded over the long term to Vietnam War–induced family separation caused by a husband/father being held captive or listed as missing in action (McCubbin, Olson, & Patterson, 1983; McCubbin & Patterson, 1983). The model remains salient in understanding responses to the uncertainty that accompanies contemporary family change, including couple dynamics in the context of nonmarital fertility (Ryan, Tolani-Brown, & Brooks-gunn, 2009), parenting stress following mothers’ entrance into or exit out of a union (Cooper, McLanahan, Meadows, & Brooks-Gunn, 2009), and responses to multipartner fertility (Harknett & Knab, 2007; Turney & Carlson, 2011).
I extend applications of family stress theory here to assess maternal well-being associated with multipartner fertility during pregnancy or shortly after a birth (in Wave 3 of the Fragile Families study, when the focal child is 3 years old) and approximately 2 years later (Wave 4, when the focal child is 5 years old). Specifically, I consider whether levels of father involvement, kin support, and role ambiguity covary with multipartner fertility over time to explain disparities in maternal well-being by multipartner fertility status.
Measures of Maternal Well-Being
I consider two indicators of maternal well-being that are expected to vary by whether a mother has engaged in multipartner fertility: depression and parenting stress. Here, depression is regarded as an internalizing disorder measured by self-reported feelings of recent sadness or emptiness or by a loss of interest in activities that once gave pleasure (Kessler, Andrews, Mroczek, Ustun, & Wittchen, 1998). Maternal depression is consequential for women and families because of its association with union stability and children’s compromised academic, social, and emotional development (Augustine & Crosnoe, 2010; Downey & Coyne, 1990). Depression is common among women with young children (Kumar & Robson, 1984) and may result from stressors related to family growth, or from the absence of economic and social resources to cope with those stressors (Rafferty, Griffin, & Robokos, 2010; Taylor et al., 2008).
Parenting stress reflects a parent’s sense that he or she lacks sufficient resources or skills to meet the demands of parenting (Cooper et al., 2009). A mother’s parenting stress is associated with her own greater psychological distress and compromised parenting skills as well as children’s diminished developmental competence and more frequent subsequent union dissolution compared with families where mothers report less parenting stress (Anthony et al., 2005; Crnic & Greenberg, 1990). In complex families, parenting stress may be greater where there are fewer social supports to carry out responsibilities associated with parenting (Crnic & Greenberg, 1990), or where role ambiguity complicates the articulation of parenting expectations and responsibilities.
Data and Method
The Fragile Families Child and Wellbeing Study is a longitudinal birth cohort study including nearly 5,000 children born between 1998 and 2000 in hospitals in 20 U.S. cities with populations of 200,000 or more. Mothers of the children were interviewed in person within 48 hours of the child’s birth and by telephone when the children were 1, 3, and 5 years old. The response rate at baseline was 82% for unmarried mothers and 87% for married mothers. The response rate is calculated as the percentage of all eligible mothers who provided complete interviews. Seventy-five percent of all mothers participated at all four waves (Bendheim-Thoman Center for Research on Child Wellbeing, 2008). This sample of families living in large U.S. cities at the focal child’s birth is relatively more disadvantaged than the U.S. population as a whole in terms of educational attainment and socioeconomic status, and is of interest to family policy advocates and scholars studying social inequality. Prior research has established the relatively high prevalence of family instability, multipartner fertility, and complex family formation in the Fragile Families Study, making it an attractive sample for considering the consequences of the dynamic nature of family structure for parent and child well-being.
The analytic sample (N = 3,366) includes mothers who have participated in each survey wave and whose focal child has lived with them at least half-time at each wave. Cases with missing data on any independent variable were excluded (N = 386). Women who have engaged in complex family formation are compared with women who have had no more children or whose higher parity children share the focal child’s biological father. Mothers who have had children with a new partner but who are not living with or married to that partner are included in order to separate out the effects of multipartner fertility from new union formation.
The analytic design proceeds in two stages. First, a comparison of group means provides an initial assessment of the association between family complexity and maternal well-being. Second, multivariate regression describes that association after accounting for potential confounders and hypothesized explanatory mechanisms. The log-odds that a mother has experienced a major depressive episode in the last year are estimated using binary logistic regression methods, and a mother’s mean parenting stress score is estimated using ordinary least squares regression.
Dependent Variables
Maternal outcomes were assessed at the third and fourth waves, when focal children were 3 years and 5 years old. A dichotomous measure of depression indicates whether the mother experienced a major depressive episode lasting at least 2 weeks in the previous year. The dichotomous indicator is a summary measure based on responses to 15 items included in the Composite International Diagnostic Interview–Short Form. A mother was coded as having experienced a depressive episode if she endorsed three of eight items pertaining to dysphoria (depression) or three of seven items pertaining anhedonia (inability to enjoy what is pleasurable), or if she volunteered that she was taking medication to treat depression.
Parenting stress was computed as an average score based on responses to four statements pertaining to the challenges and responsibilities of parenting. Likert-style response categories were reverse-coded so that a higher score indicated greater agreement with a statement that parenting is challenging, unrewarding, or exhausting. Scores on the items were averaged for all participants who responded to at least three of the four statements. Scores at each wave range in value from 1 to 4 and are roughly normally distributed, with skewness scores below .5.
Key Independent Variables
Complex family formation is measured as a focal child’s mother either being pregnant with or having given birth to a child other than the focal child’s biological father by the time the focal child was 3 years old (i.e., by the time of the Wave 3 interview). Pregnant mothers are included in the definition because pregnancy may affect parenting stress and mental health, particularly if a pregnancy is unintended, mistimed, or has significant physical side effects. Furthermore, a woman’s pregnancy with a new partner may be a concrete indicator to her former partner that their relationship has ended, potentially prompting father involvement (Guzzo, 2009) and kin support (Harknett & Knab, 2007) to recede even before a new child is born.
I expect that perceived kin support, father involvement, and family boundary ambiguity will mediate the association of complex family formation with each of the dependent variables. Perceived kin support is a summed index of responses to questions about three types of social support. Mothers were asked if they would have someone to go to for help if in the next year they needed a loan of $200; if they needed a place to stay; or if they needed emergency child care. Each item is a dichotomous indicator measuring the presence or absence of the perceived type of support. The perceived kin support measure ranges from 0, indicating an absence of support, to 3, indicating that all types of support are available to the mother. The question wording does not specifically pertain to kin-based support. However, prior work has established that a substantial amount of social support exchanges occur between kin (Rossi & Rossi, 1990), and the items used here have been used in an earlier study to document the absence of social support in expanded kin networks that emerge from complex family formation (Harknett & Knab, 2007). Consistent with Harknett and Knab (2007), I focus on perceived rather than actual support. Analyses of actual support indicate that women who are embedded in social networks may not receive support because they do not need it, rather than because they lack the potential to use it.
Father involvement was measured by three attributes: provision of formal or informal child support, how frequently he sees the focal child, and the mother’s assessment of their relationship quality and coparenting style. In families with nonresident biological fathers, formal child support is characterized as cash transfers provided by the father in compliance with a legal agreement or child support order. Informal child support is defined as cash transfers provided by the father in keeping with an informal, nonbinding agreement established between a child’s parents. A nonresident father is considered not to be providing child support if the mother explicitly states that there are no such transfers, or if she does not know the identity of the biological father, the father does not know about the child, or paternity has not been established. Mothers receiving no support or formal or informal support from a nonresident father are compared with mothers who coreside with the child’s biological father.
Frequency of visitation by a nonresident biological father is based on the mother’s report of how frequently he saw the focal child in the previous 30 days, and was collapsed into four ordinal categories: never, less than once a week, at least once a week, and daily. Mother–father relationship quality is a summed index based on two items: First, global relationship quality was scored 1 if the mother reported that her relationship with the father was excellent, very good, or fair, and 0 otherwise. Second, coparenting is represented by a dichotomous measure summarizing the mother’s response to six items about whether she could trust and rely on the father to care for their child and to support her child-rearing decisions. If her average response indicated that coparenting sometimes or always occurred, the dichotomous indicator was scored 1, 0 otherwise. The summed index had a range from 0 to 2.
Family boundary ambiguity was measured by four indicators. First, the presence of a new partner’s own biological children in a focal child’s household (i.e., stepsiblings) represents a source of ambiguity about role responsibility within a child’s household. Second, mothers reported on the frequency of parent–child activities in which the biological father and, where relevant, her new partner, participate. Activities were computed as an average score based on a mother’s reported count of how frequently the father or partner engaged in a range of age-appropriate activities with the focal child in a week (0 = never, 7 = every day). At the Wave 3 interview, 12 activities included singing together, telling stories, and showing affection to the focal child. The Wave 4 scale included seven similar items. At Wave 3, one item in the roster of activities, helping child with eating, was excluded because its inclusion reduced the alpha reliability statistic for the composite scale. At Wave 4, watching television or videos together was excluded. Fathers and partners who participate in at least half of the rostered activities 3 or more times a week were categorized as highly involved. Biological fathers with whom the child had no contact were categorized as not involved. A four-category measure was created from those two indicators: (1) A single mother reported the biological father was not highly involved or (2) was highly involved; (3) a partnered mother (either with the focal child’s biological father or another man) reported that either the father or the partner (or both) was highly involved; and (4) a partnered mother reported that neither the father nor her partner was highly involved in activities with the focal child. The absence of involvement by any father figure is expected to be associated with the mother’s compromised well-being. Third, the mother’s multipartner fertility prior to the focal child’s birth is indicative of more entrenched family complexity and family boundary ambiguity. Finally, the biological father’s multipartner fertility after the focal child’s birth indicates another source of family complexity and cause of potential disengagement from the focal child.
Control Variables
Family complexity and maternal well-being potentially covary with parents’ sociodemographic attributes and family backgrounds. Marital status at birth is strongly predictive of later family complexity, with single or unmarried parents more likely than married parents to engage in later multipartner fertility. Marital status at subsequent interviews is an indicator of union stability as well as a correlate of household income, father involvement with children (whether from coresident biological or social fathers), and kin connectedness. Because family complexity is overrepresented among racial/ethnic minority parents and young parents, I control for mother’s race/ethnicity and age at the focal child’s birth. Indicators of socioeconomic status include completed education and Medicaid enrollment at the focal child’s birth. Family background includes nativity and an indicator of whether the mother lived with both biological parents at age 15. I also control for mother’s parity at the focal child’s birth, the number of romantic partners she had prior to the focal child’s biological father, the mother’s overall health status when the focal child was born, the intendedness of the focal child’s birth (indicated by whether she considered an abortion during her pregnancy), and the focal child’s gender. Models estimating outcomes at Wave 3 control for the same outcome variable obtained at the Wave 2 interview (when the focal child was 1 year old, before any other children were born), and models estimating outcomes at Wave 4 control for those outcomes measured at Wave 3. Because information on parenting stress was not collected in two cities at Wave 2, the N for the model predicting parenting stress at Wave 3 includes approximately 500 fewer observations than the other analytic models.
Results
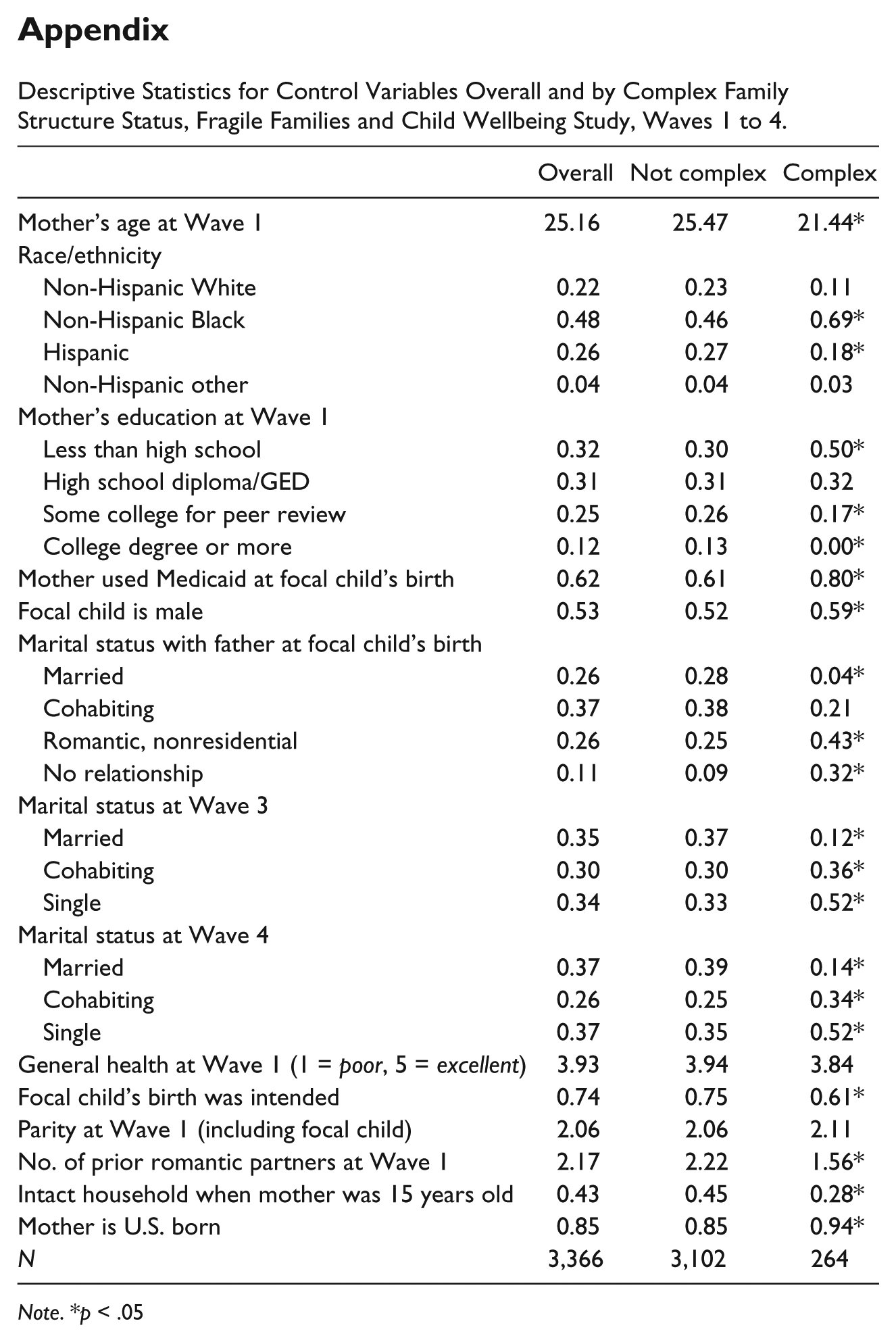
Table 1 provides means and proportions for the dependent variables and explanatory variables overall and by mother’s multipartner fertility status at Wave 3. (Control variables are described in the appendix.) Asterisks indicate group differences that are significant at p < .05. Approximately 8% of mothers (N = 264) had a child with or were pregnant by another father by the time the focal child was 3 years old. Among women who did not engage in multipartner fertility, about one quarter had conceived another child with the focal child’s biological father. Comparisons of group means indicate that mothers engaged in multipartner fertility (i.e., in complex families) were more often depressed and reported higher parenting stress when the focal child was 3 years and 5 years old compared with other mothers. The prevalence of depression decreased for each group between waves, but levels of parenting stress declined only for mothers who had not engaged in multipartner fertility. Group differences in the prevalence of depression were insignificant at Wave 2, when focal children were 1 year old (before any multipartner fertility), but parenting stress was already elevated for parents who eventually had a child with another father.
Descriptive Statistics for Dependent and Key Independent Variables Overall and by Complex Family Structure Status, Fragile Families and Child Wellbeing Study, Waves 1 to 4.
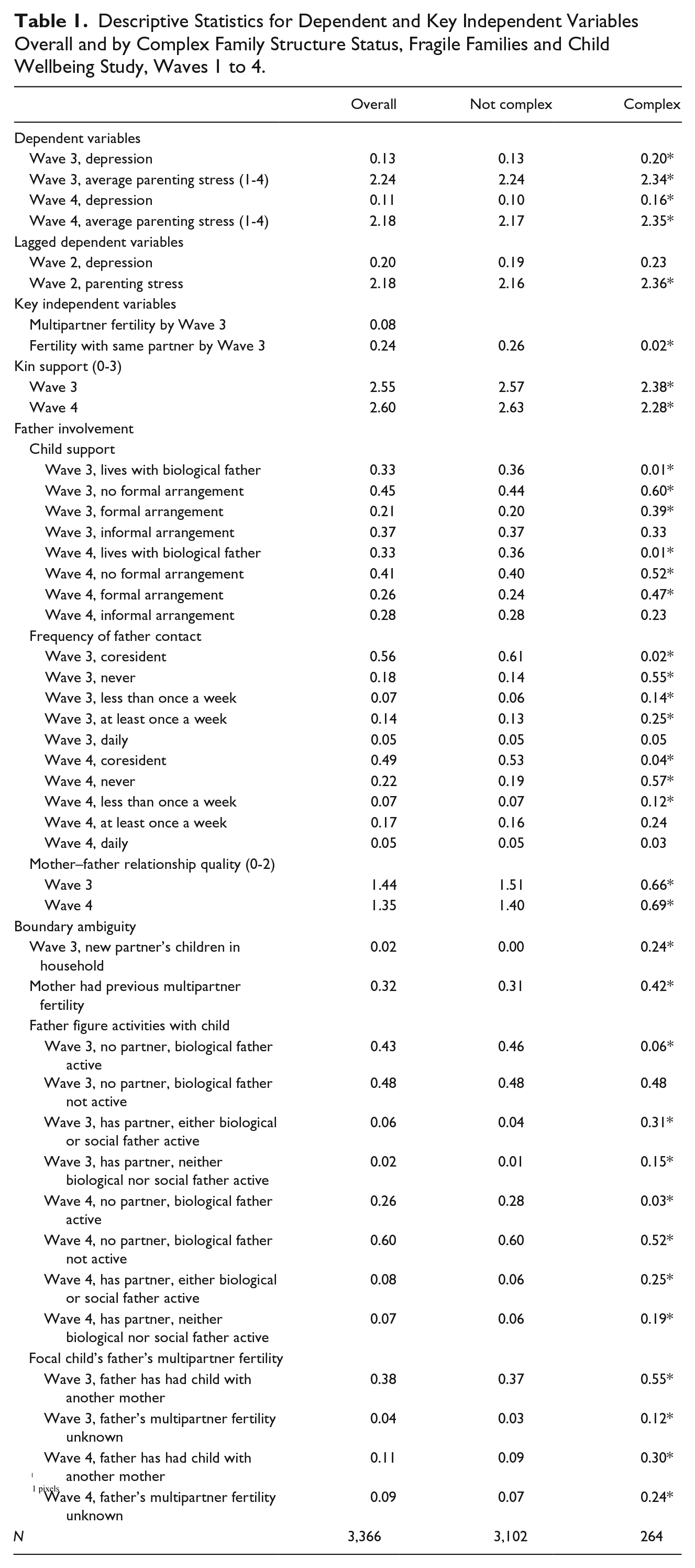
Group differences in explanatory variables support each of the hypothesized mediating mechanisms. At Waves 3 and 4, mothers in complex families reported lower perceived social support and more often had no formal child support arrangement with the focal child’s biological father. Focal children in complex families were more likely than other children to see their biological father never or rarely, and their mothers reported poorer relationship quality with the father. Complex families were also characterized by boundary ambiguity. About one quarter of mothers who had a child with another father were also living with that social father’s own children, and were about one third more likely than other mothers to have experienced earlier multipartner fertility. Biological fathers were also more likely to have had children with another woman when a mother had engaged in multipartner fertility herself. Finally, mothers in complex families were about three times more likely than other mothers to report that no father figure (i.e., neither a biological nor social father) was involved in daily activities with the focal child.
Multivariate Results
Table 2 presents results from multivariate regressions estimating the association between family complexity and maternal well-being when the focal child was 3 years old, before and after accounting for the hypothesized mediating mechanisms. All analytic models include control variables, but associated coefficients are not reported. Panel 1 presents coefficients estimating change in the log-odds that a mother has experienced a major depressive episode for a one-unit change in a given independent variable. Exponentiated values of the log-odds coefficients represent a change in the odds of having experienced a depressive episode. The baseline model indicates that a mother’s odds of experiencing a major depressive episode in the last year is 43% higher (B = .36, exp[B] = 1.43, p < .05) when she had a child with another father or was pregnant by the time the focal child was 3 years old compared with cases where a mother had not had another child. Mothers who had conceived a child with the focal child’s biological father did not have an elevated risk of depression. Models 2 through 4 account for perceived access to social support, father involvement, and boundary ambiguity, respectively. Social support was independently predictive of a lower log-odds of a depressive episode, but had only a mild attenuating effect on the association of family complexity with depression. Indicators of father involvement had a much stronger attenuating effect, reducing the magnitude of the family complexity coefficient by about 40%, below conventional measures of statistical significance. Among the indicators of father involvement, mother’s relationship quality with the father was the strongest mediator. Boundary ambiguity has a similar attenuating effect. The absence of a father figure who participated in daily activities was the strongest mediator among the indicators considered. Model 5 accounts for each set of explanatory factors simultaneously. The frequency of biological father involvement is excluded from the full model because it is highly collinear with the measure of father–child activities used to characterize boundary ambiguity. The effect of family complexity is statistically insignificant, and perceived kin support and relationship quality with the biological father remain negatively associated with the log-odds of having experienced depression.
Multivariate Regressions Estimating Log-Odds of Depression and Predicted Parenting Stress, Wave 3 Fragile Families and Child Wellbeing Study, Waves 1 to 3.
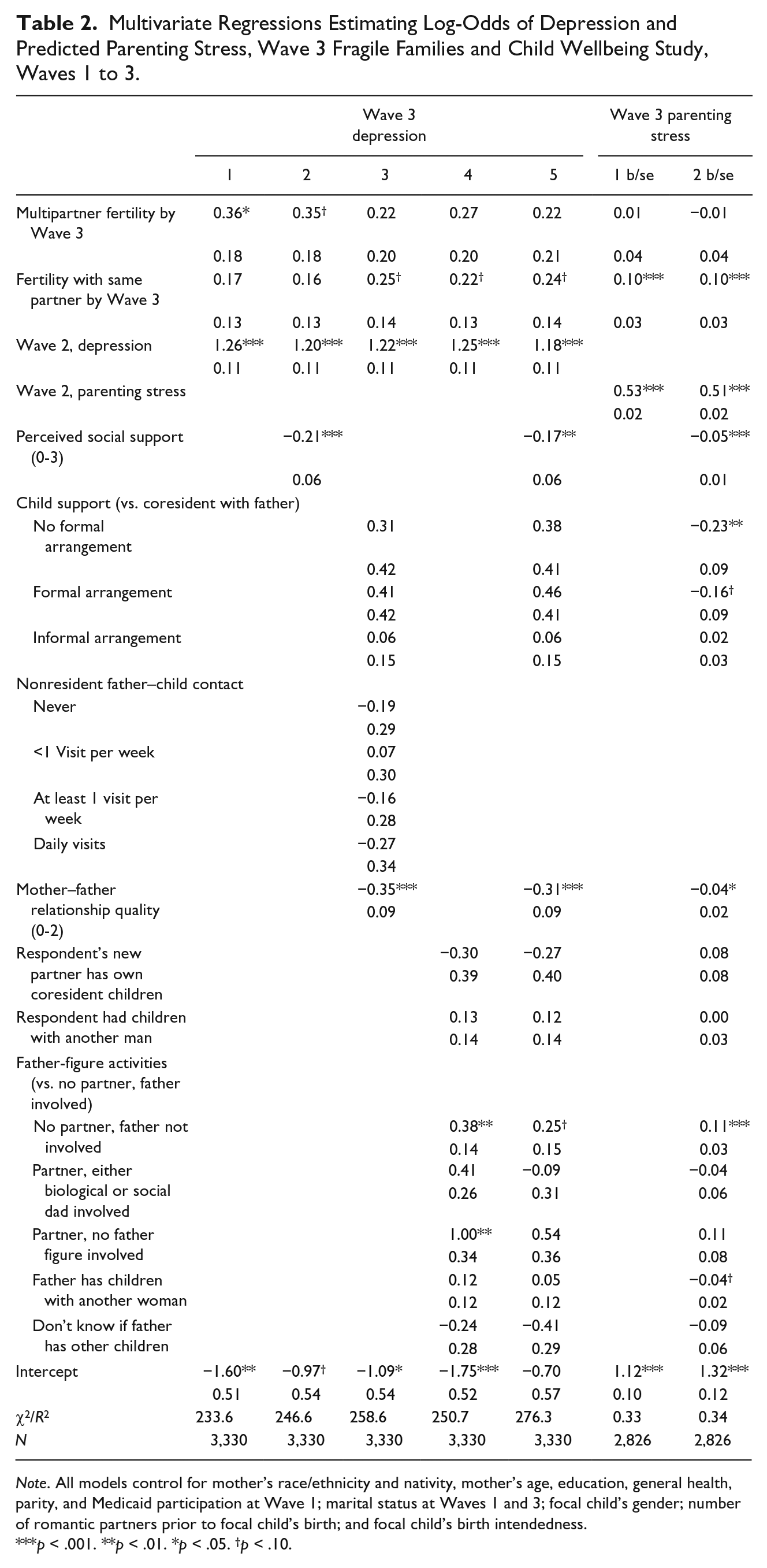
Note. All models control for mother’s race/ethnicity and nativity, mother’s age, education, general health, parity, and Medicaid participation at Wave 1; marital status at Waves 1 and 3; focal child’s gender; number of romantic partners prior to focal child’s birth; and focal child’s birth intendedness.
p < .001. **p < .01. *p < .05. †p < .10.
The second panel of Table 2 presents results from ordinary least squares regression estimates of a mother’s mean parenting stress score at Wave 3. The baseline model shows that after including control variables, there is no statistical association between family complexity and parenting stress. However, subsequent childbearing with the focal child’s biological father is associated with a .10-point increase in a mother’s average parenting stress score (about one sixth of a standard deviation). Because the initial hypothesis about the presence of a relationship between family complexity and Wave 3 parenting stress was not supported, the presentation of results is abbreviated, showing only the full model in contrast to the baseline model. As with depression, perceived access to social support had a direct, negative association and poor relationship quality and the absence of father–child activities had a positive association with parenting stress. However, those factors had no mediating influence on family complexity or on childbearing with the focal child’s biological father.
Table 3 presents results from models estimating maternal well-being at Wave 4 (when focal children were 5 years old), approximately 2 years after complex family formation through multipartner fertility. In the baseline model estimating the likelihood of depression (Panel 1), a mother is about 64% more likely to have had a depressive episode in the last year (B = .50, exp[B] = 1.64, p < .05) when she has had another child through multipartner fertility compared with mothers who have not had other children. The magnitude of the log-odds coefficient is about 40% larger at Wave 4 than at Wave 3 (B = .50 at Wave 4 vs. B = .36 at Wave 3), consistent with McCubbin and Patterson’s (1983) conjecture that stressors compound over time. However, post hoc tests indicate that the coefficients from the two waves are not significantly different from each other. As at Wave 3, mothers who had conceived another child with the focal child’s biological father did not have a greater risk of depression.
Multivariate Regressions Estimating Log-Odds of Depression and Predicted Parenting Stress, Wave 3 Fragile Families and Child Wellbeing Study, Waves 1 to 4.
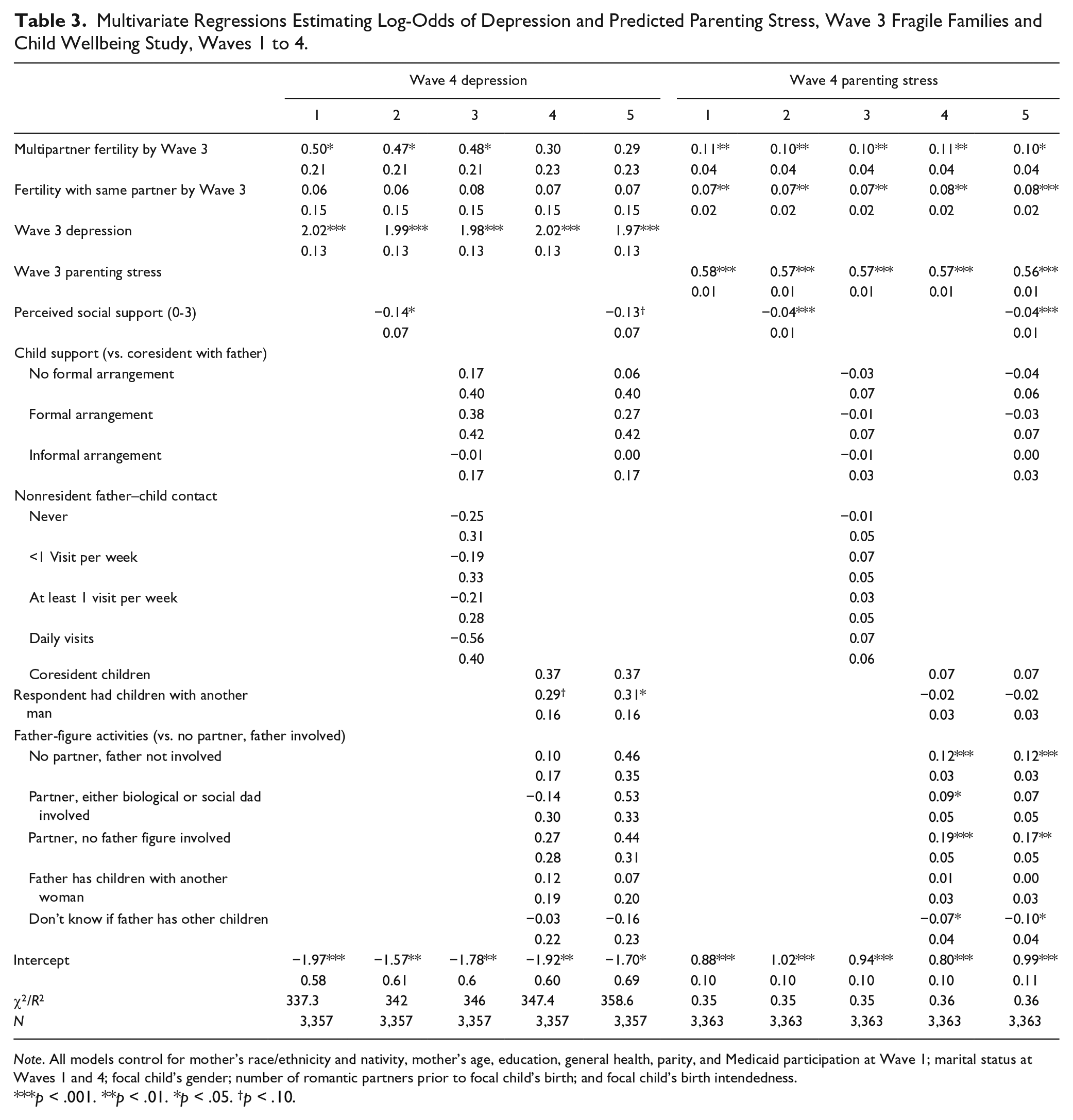
Note. All models control for mother’s race/ethnicity and nativity, mother’s age, education, general health, parity, and Medicaid participation at Wave 1; marital status at Waves 1 and 4; focal child’s gender; number of romantic partners prior to focal child’s birth; and focal child’s birth intendedness.
p < .001. **p < .01. *p < .05. †p < .10.
Also consistent with Wave 3, perceived kin support was negatively associated with the log-odds of depression and had a mild attenuating effect on the association of family complexity with the outcome. In contrast to Wave 3, however, father involvement did not explain the association between family complexity and the risk of maternal depression. Instead, accounting for indicators of boundary ambiguity, and particularly the presence of a partner’s other children in a household and a mother’s own prior multipartner fertility, diminished the magnitude of the effect of family complexity by 40%. This pattern of results held in the final model.
Unlike at Wave 3, family complexity was positively associated with parenting stress (Panel 2) at Wave 4. Having formed a complex family through multipartner fertility increased a mother’s predicted parenting score by .11 points (p < .01, one sixth of a standard deviation) compared with mothers who have had no additional children. Mothers who had another child with the focal child’s biological father also continued to have higher parenting stress (B = .07, p < .01), although at slightly diminished levels compared with Wave 3. At Wave 4, the magnitude of difference in the coefficients for women who had children with a new versus ongoing partner was marginally significant (p = .07), suggesting that longer term parenting stress was heightened in the context of complex family formation.
Among the explanatory mechanisms considered, access to perceived social support and father involvement had a mild attenuating effect on family complexity, reducing the magnitude of the coefficient by about 9% (B = .10 vs. B = .11 in the baseline model), but not diminishing statistical significance. Perceived access to social support and better relationship quality with the focal child’s biological father both independently reduced a mother’s predicted parenting stress score. Indicators of family ambiguity did not change the association between family complexity and parenting stress at Wave 4 compared with the baseline model. In the full model, accounting simultaneously for all explanatory mechanisms reduced the statistical significance of that association to p < .05, but did not further reduce the magnitude of the family complexity coefficient compared with the models that accounted for only perceived social support or father involvement. The magnitude of the coefficient associated with childbearing with an ongoing partner increased slightly in the full model compared with the baseline model, suggesting that mothers engaged in single-partner fertility since the focal child’s birth would have had greater parenting stress in the absence of protective factors like kin support and father involvement.
Discussion
Increasingly, multipartner fertility is a pathway to complex family formation. The research question posed here considered whether multipartner fertility and family complexity are associated with compromised maternal well-being on two dimensions: depression and parenting stress. Data were drawn from the Fragile Families Child and Wellbeing Study, a longitudinal study of mothers in large U.S. cities whose children represent a recent birth cohort in the United States. Mothers who had recently had a child with a new partner were compared with mothers who had additional children with an ongoing partner or who had no additional children since the birth of the Fragile Families focal child when the focal child was 3 and 5 years old.
Overall, mothers who had formed a complex family through multipartner fertility had an elevated risk of depression both in the short term (i.e., when they were still pregnant or had recently delivered a child) and in the longer term (i.e., approximately 2 years later). The results suggest that the risk of depression increases over time in a complex family, a finding consistent with the Double ABCX model of family stress theory (McCubbin & Patterson, 1983). However, that conclusion is not definitive, as the difference in the magnitude of coefficients associated with family complexity at Waves 3 and 4 was statistically nonsignificant. Mothers’ elevated parenting stress was slower to emerge in complex families. No association was present when the mother’s focal child was 3 years old, but 2 years later, family complexity was associated with a small but persistent positive effect on maternal stress. This pattern of mothers’ increasing parenting stress in complex families was in contrast to mothers engaged in new single-partner fertility, for whom parenting stress was high in the short term and diminished somewhat over the longer term. For family stress theory, these findings reinforce the value of long-range assessments of response to stressful events and highlight the need in considering contemporary family structure change to measure family process and involvement outside of household boundaries.
I considered three mediating mechanisms to explain the association between family complexity and maternal well-being: perceived kin support, father involvement, and boundary ambiguity. Collectively, the mechanisms were more effective in explaining variation in the likelihood of depression than in parenting stress scores. However, the factors that explained variation in depression changed over time, with father involvement having a stronger mediating effect in the short term (at Wave 3), and boundary ambiguity having a stronger effect in the long term (at Wave 4). This shift is consistent with McCubbin and Patterson’s notion that over time, new stressors are triggered in response to an initial stressor like childbearing, particularly where coping resources are insufficient. In this case, the salience of a former partner’s involvement for a mother’s mental health receded in the course of complex family formation, but another set of factors associated with family complexity—in particular, household composition—arose to take its place.
Why did the mediating mechanisms fail to explain more of the association between family complexity and parenting stress? The parenting stress construct may pertain more to the relationship between a mother and her children than to the more generalized sense of psychological distress that is captured by indicators of a depressive episode. For example, the statement “I feel trapped by my responsibilities as a parent” may prompt respondents to think about their concrete daily obligations to a child’s well-being, rather than to consider more abstract aspects of parenting like the effort required to effectively communicate with a child’s father about the child’s needs. Therefore, future research might consider how mother–child relationship quality and children’s development in complex families influences mothers’ perceptions of parenting stress. In particular, a growing body of literature has documented that repeated changes in family structure are associated with young children’s heightened aggressive and externalizing behavior and diminished prosocial behavior (Cavanagh & Huston, 2006; Osborne & McLanahan, 2007), factors that may add to parenting stress. A theoretical model that articulates the co-occurrence of parenting stress and children’s behavior problems in dynamic family structure systems would build on existing research to elucidate the interaction between family structure and family process from a life course perspective.
The current study has some limitations. First, the data are not nationally representative. Therefore, the findings may not characterize complex family formation and multipartner fertility in nonurban areas or among more affluent families. Second, the timing of multipartner fertility is unknown, so it is not possible to chart the sequence of childbearing and new coresidential unions, which might give some purchase on understanding the context of multipartner fertility. Third, the indicators of perceived social support are thin compared with the indicators of father involvement and boundary ambiguity that are available, and it is not possible to make direct conclusions about kin involvement with mothers or children. On the same lines, the analysis does not take into account that complex families may be embedded in multifamily households, a circumstance that may offset a lack of kin support outside of the household. Further research with alternative data sets may address these specific limitations. More broadly, studies using alternative designs to household-based studies can enrich the context in which we observe multipartner fertility and family complexity. For example, Seltzer (2011) highlights the importance of studies including families that bridge households to better understand the processes and relationships running simultaneously within and across households in complex family systems. Researchers also may focus on the relationships between multiple dyads in complex families, including the relationships between children and half-siblings and children and social parents, to better understand the nature and consequences of role ambiguity and resource distribution.
Despite these limitations, the preceding analysis presents evidence that family complexity is associated with mothers’ compromised mental health, and that the association endures beyond an initial period of adjustment to family growth. At least in part, poorer mental health is attributable to diminished access to social capital in the context of complicated or weakly defined expectations among family members. As multipartner fertility increasingly becomes an avenue to family complexity, future research should consider family process within and beyond the household to identify the evolving challenges to family functioning posed by family members’ shifting affinities and obligations.
Footnotes
Appendix
Descriptive Statistics for Control Variables Overall and by Complex Family Structure Status, Fragile Families and Child Wellbeing Study, Waves 1 to 4.
| Overall | Not complex | Complex | |
|---|---|---|---|
| Mother’s age at Wave 1 | 25.16 | 25.47 | 21.44* |
| Race/ethnicity | |||
| Non-Hispanic White | 0.22 | 0.23 | 0.11 |
| Non-Hispanic Black | 0.48 | 0.46 | 0.69* |
| Hispanic | 0.26 | 0.27 | 0.18* |
| Non-Hispanic other | 0.04 | 0.04 | 0.03 |
| Mother’s education at Wave 1 | |||
| Less than high school | 0.32 | 0.30 | 0.50* |
| High school diploma/GED | 0.31 | 0.31 | 0.32 |
| Some college for peer review | 0.25 | 0.26 | 0.17* |
| College degree or more | 0.12 | 0.13 | 0.00* |
| Mother used Medicaid at focal child’s birth | 0.62 | 0.61 | 0.80* |
| Focal child is male | 0.53 | 0.52 | 0.59* |
| Marital status with father at focal child’s birth | |||
| Married | 0.26 | 0.28 | 0.04* |
| Cohabiting | 0.37 | 0.38 | 0.21 |
| Romantic, nonresidential | 0.26 | 0.25 | 0.43* |
| No relationship | 0.11 | 0.09 | 0.32* |
| Marital status at Wave 3 | |||
| Married | 0.35 | 0.37 | 0.12* |
| Cohabiting | 0.30 | 0.30 | 0.36* |
| Single | 0.34 | 0.33 | 0.52* |
| Marital status at Wave 4 | |||
| Married | 0.37 | 0.39 | 0.14* |
| Cohabiting | 0.26 | 0.25 | 0.34* |
| Single | 0.37 | 0.35 | 0.52* |
| General health at Wave 1 (1 = poor, 5 = excellent) | 3.93 | 3.94 | 3.84 |
| Focal child’s birth was intended | 0.74 | 0.75 | 0.61* |
| Parity at Wave 1 (including focal child) | 2.06 | 2.06 | 2.11 |
| No. of prior romantic partners at Wave 1 | 2.17 | 2.22 | 1.56* |
| Intact household when mother was 15 years old | 0.43 | 0.45 | 0.28* |
| Mother is U.S. born | 0.85 | 0.85 | 0.94* |
| N | 3,366 | 3,102 | 264 |
Note. *p < .05
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.