
Abstract
Most measures of father involvement with children have been developed for use with middle-class fathers who reside with their children. The current study documents the development and initial validation of a new measure of decision-making responsibility for low-income fathers with a nonresident child. Focus groups conducted with 71 fathers revealed two dimensions of decision-making responsibility: making decisions with respect to direct care of the child and making decisions with respect to resources. Surveys were then collected from 542 nonresident fathers to validate a set of items measuring these two dimensions. The results of exploratory factor analysis and confirmatory factor analysis supported these factors. However, the results of convergent and predictive validity tests suggest that the resources factor does not add additional explanatory power above its association with the care factor. We suggest using only the seven care decision-making items in future studies.
There has been considerable interest among researchers and practitioners in the extent to which unmarried nonresident fathers assume responsibility for children. This interest is fueled by two societal changes in the United States: (a) a growing number of children born outside of marriage with their biological fathers residing outside the home who face significant challenges to active involvement in their children’s lives and (b) more mothers who are employed outside of the home and place increasing demands on fathers (including nonresident fathers) to become more involved in child care and child rearing. In addition, a growing body of research shows that positive father involvement is a protective factor and promotes child well-being (Flouri, 2005; Pleck, 2010). The present article examines low-income, nonresident fathers’ participation in one aspect of involvement with children: decision making regarding children. We specifically focus on the development of a new measure of nonresident fathers’ decision making, which we refer to as “decision-making responsibility.” We begin with a discussion of decision making as an element of parenting and how it has or has not been measured for nonresident fathers. Next, we described how we developed a new measure of decision making and how we tested for convergent and predictive validity.
Researchers have developed a number of measures of fathering (e.g., responsibility), but for the most part, they have been developed for use with fathers who reside with their children (for review, see Fagan & Kaufman, 2015). Consequently, current conceptualizations and measures of fathering are based on our understanding of how coresiding, mostly married, fathers engage in parenting. There is reason to expect, however, that there may be significant differences in the ways that fathers in nonresident family structures and coresident family structures engage in parenting (Hernandez & Coley, 2007). Our new measure of decision-making responsibility was developed for low-income fathers with at least one child with whom they do not reside. This measure is intended for use in low-income communities as well as for fatherhood programs that serve primarily never married, nonresident fathers.
Background
Early attempts to conceptualize father involvement were undertaken by Lamb, Pleck, Charnov, and Levine (1987) who suggested an organizational heuristic of types of father involvement, including three major constructs: engagement, accessibility, and responsibility. Engagement refers to fathers’ shared interactions with their children; accessibility is a father’s availability to a child whether he is directly engaged with that child; and responsibility refers to a father’s organizing and planning activities in relation to a child and provision of resources to that child (Lamb et al., 1987). Many researchers adopted this framework for conceptualizing father involvement and applied it to studies including nonresident fathers. Of the three types of involvement suggested by Lamb et al. (1987), researchers have typically studied paternal engagement and accessibility more extensively than responsibility, largely, perhaps, because engagement and accessibility were the simpler constructs to measure and overlapped the most with traditional notions of parenting. Responsibility may be understudied also because there is a lack of clarity about the meaning and relevance of this construct.
Pleck (2010) proposed a revised conceptualization of paternal involvement that includes positive engagement, warmth and responsiveness, control, indirect care, and process responsibility. Indirect care of children is a component of responsibility and is defined as participation in activities for the child (e.g., arranging for resources to be available for the child, promoting children’s community connections). Process responsibility refers to fathers’ use of personal agency such as taking initiative and monitoring what the child needs. Parke’s (1995) conceptual definition of responsibility was similar to Lamb et al.’s (1987) in that he referred to the managerial tasks of parenting, including organizing and arranging the child’s home environment, social contacts with playmates, and socializing agents outside of the family. On the other hand, Daly (2001) focused on the scheduling aspect of responsibility, that is, the arranging and planning of children’s time both in and outside of the home.
Although there is considerable disagreement about the meaning of responsibility, we agree with Stueve and Pleck (2003) who suggest that engagement and accessibility are primarily behavioral, while responsibility includes both cognitive and behavioral components. In addition, they suggest that responsibility encompasses both the organizing and managing of arrangements for the child and the performance of “infrastructure” tasks (things that are done for the child but not with the child). The measure developed for this study focuses on the organizing and managing aspect of responsibility, that is, fathers’ participation in decision making about children. Parents (fathers and mothers) must make many decisions for children in the process of organizing and managing their lives. These can range from deciding where children go to school, when to take them to the doctor, what foods to provide, and which friends they spend time with. The decisions that parents make for their children can have significant influence on children’s well-being. For example, parents’ decisions about use of out-of-home child care has implications for the quality of that care and ultimately influences child outcomes (Weber, 2011).
Decision making may be especially challenging for low-income, unmarried fathers who do not reside with their children. Mothers may exclude fathers from shared decision making because they are not available, or mothers may exclude fathers because shared decision making produces conflict between parents (Manning, Steward, & Smock, 2003). In addition, many low-income, nonresident fathers experience additional personal challenges. Waller and Swisher (2006) suggested that fathers with many personal challenges may passively withdraw from being involved with their children. Qualitative research with low-income, unmarried, nonresident fathers showed that mothers want their child’s father to be involved with the child, but only if the father does not have too many problems of his own and can provide for his children (Roy, Buckmiller, & McDowell, 2008). Lack of a legitimate means for securing a living wage has been found to be a significant correlate of low-income and minority fathers’ low-level involvement with children (Coley & Chase-Lansdale, 1999). However, Edin and Kefalas (2001) suggested that poverty alone is not a barrier to fathers’ family involvement; other factors include the father’s antisocial behavior, infidelity, pattern of intimate partner violence, and inability to stop using drugs and alcohol.
Current Study
This study reports the findings of a new measure of decision-making responsibility developed specifically for low-income, nonresident fathers. First, we describe the development of the measure based on a series of focus groups conducted with fathers in fatherhood programs. Second, we report the results of two quantitative studies based on two sets of data: an exploratory study examining the factor structure of the measure and a confirmatory factor analysis (CFA). The data are then combined to test for two types of construct validity: convergent and predictive. Tests of internal consistency of the measure are also presented.
Focus Group Study
Method
As a first step in the development of the responsibility measure, focus groups were conducted with low-income, nonresident fathers attending nine different fatherhood programs. Nonresidence was defined as not living in the same household with at least one of their children all or most of the time. Across the nine fatherhood programs, we recruited 71 fathers who completed one focus group session. Fathers were instructed to think about what it means to them to assume responsibility for one’s child. A content analysis of the narratives pertaining to responsibility was conducted. First, we examined broad themes within the 71 research participants’ narrative accounts. All nine transcripts were rigorously and systematically read several times by two readers to identify themes and categories. After discussion, a coding frame was determined and the transcripts were reread according to the new structure. Then, segments of the interview text were coded enabling an analysis of interview segments on a particular theme. After coding for broad themes (e.g., decision making), we coded for more specific decision-making themes.
The sample for the focus groups was composed of 71 biological fathers. Fathers ranged in level of educational achievement; nearly 20% reported having less than a high school diploma and around 45% of the sample reported having a high school diploma or GED. The majority were single and never married (n = 53), African American (n = 41), and reported an income of less than $10,000 before taxes and deductions (n = 38).
Results of Focus Groups
The content analysis revealed that fathers’ participation in making decisions about children is an important component of responsibility and that fathers made a variety of different types of caretaking decisions. Some fathers reported making decisions about what types of food the child eats, while others reported making decisions around the frequency or the type of discipline that was utilized when the child misbehaves. Other participants reported their involvement in making decisions with regard to physical care of the child. One father shared, “I have a thing with my daughter’s hair. I don’t like her hair to be messed up, so I have to find somebody to do her hair.” This analysis suggested the subtheme: fathers’ participation in making decisions with respect to caregiving.
The focus group data suggested that fathers participated in making decisions with respect to external resources too. Fathers frequently mentioned different types of decisions they had made about which school or day care the child would attend. One father concisely explained, “Changing schools . . . I make that decision.” Participants also discussed making decisions about when the child would visit the doctor. One father shared that since he is “the overprotective guy,” he often makes the decisions about when the child needs to visit the doctor. Although many participants shared anecdotes involving solo decision-making processes, some discussed collaborative decision making with the mother of the child. For instance, one father explained that both he and the mother of the child would collaboratively make decisions about their child’s school field trips and vacations. The second subtheme identified was: fathers’ participation in making decisions with respect to external resources.
Item Construction and Format
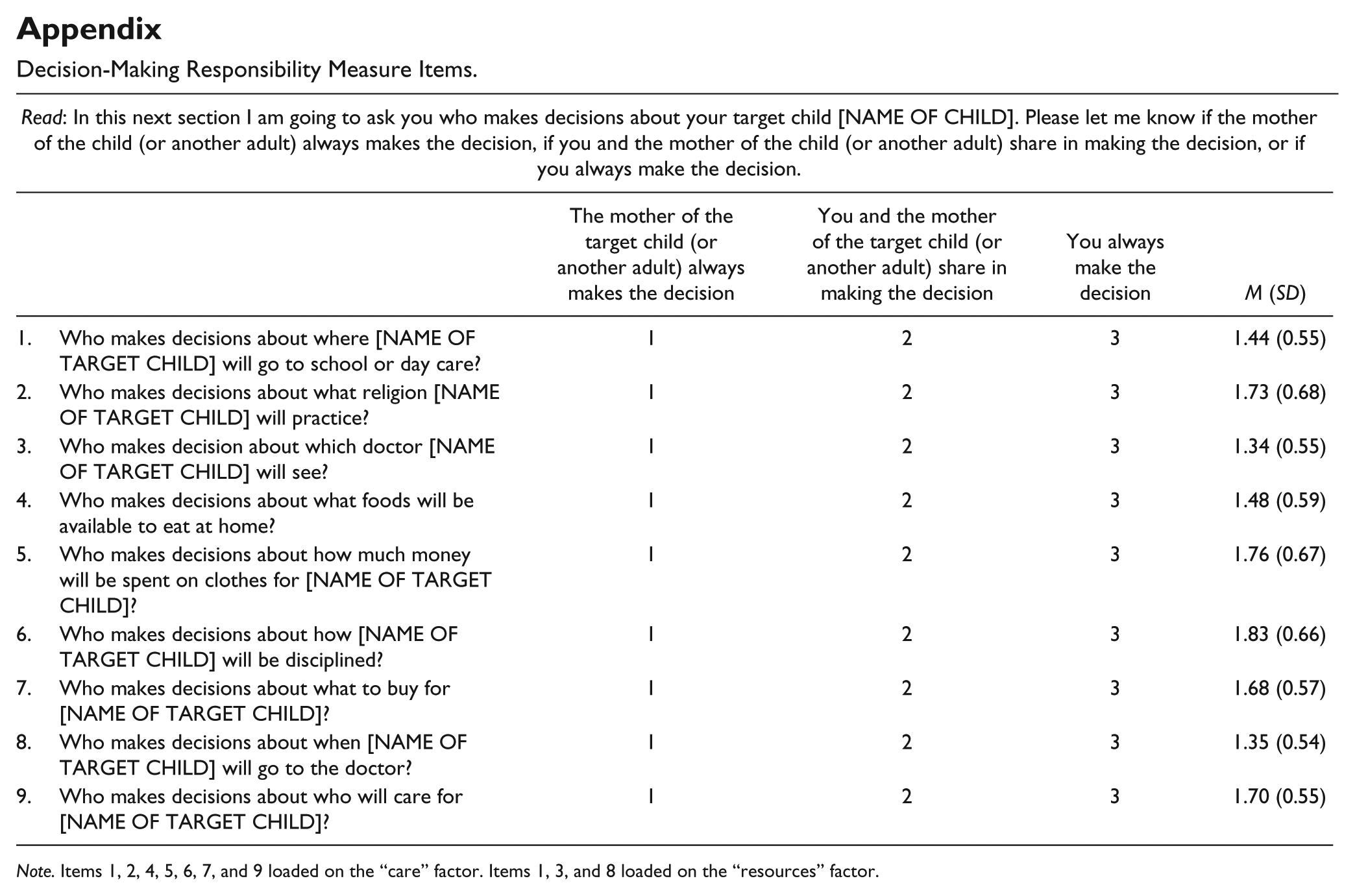
The next step in the development of the measure was to develop an item pool. Guided by the focus group data and researchers such as Daly (2001) who suggested that responsibility refers to arranging and planning both inside and outside of the home, we decided on items that pertained to both caring for children in the context of the home and to organizing resources outside of the home. We also decided to focus on decisions that would seem relevant to nonresident mothers and fathers and that may involve a significant amount of problem solving and negotiation between parents. For example, we selected items that pose significant challenges to parents in high-poverty communities, such as which school the child would attend or how the child would be disciplined (Boyd-Franklin & Franklin, 2001). The appendix shows the items developed for the decision-making responsibility measure.
Validation Study
Background
The validation aspect of our study examined the factor structure of the decision-making responsibility measure using exploratory factor analysis (EFA) and CFA. Within a single sample, the cases were randomly divided in half with the EFAs performed on one half of the sample and the CFAs on the other half. The data were then combined to test for two types of construct validity: convergent and predictive.
To test for convergent validity, we examined the relationship of our new decision-making responsibility measure with the following measures: father involvement (Hernandez & Coley, 2007), number of nights spent with the child, and father’s contact with the child. The Hernandez and Coley (2007) measure, called father involvement, is a multicomponent instrument based on the three major constructs of Lamb et al. (1987): engagement, accessibility, and responsibility. The measure was validated with a low-income sample of fathers participating in Welfare, Children, and Families: A Three-City Study. About half of the fathers participating in this study were nonresidential, 45% were African American, and the average education level was less than a high school diploma. We also examined convergent validity with a measure of father’s nights spent with the child because studies find that fathers’ proximity to children when they spend nights together is highly correlated with amount of involvement (including responsibility; Levine, Kaufman, Hammar, & Fagan, 2015). Validated measures are not generally available for nights spent with child because this construct is normally assessed using a single item. We also tested convergent validity with a measure of contact with the child: a single item asking fathers how often they have face-to-face contact with the child. Again, measures of contact were not validated instruments but are highly correlated with fathers’ responsibility for children, particularly among nonresident fathers.
To test predictive validity, we examined the relationship of our new decision-making responsibility measure with the following constructs: father–child closeness, parenting self-efficacy, fathers’ role salience, and parenting satisfaction. The more the father is able to enact his role in the responsibility dimension, the greater the salience the role will have, the more satisfied he will be in the role, the greater his sense of parenting self-efficacy, and the greater the likelihood of a close father–child relationship (Rane & McBride, 2000). These measures were also selected because of their relevance to unmarried, nonresident fathers’ attachment bonds with their children. Attachment theory emphasizes the father’s sense of closeness to the child and his sensitivity to children’s emotional development (Bell & Ainsworth, 1972). Fathers who are more highly involved and responsible for their children are likely to have closer relationships with them. Pianta’s (1992) Child-Parent Relationship Scale (CPRS) was used to assess closeness. The CPRS has been validated in a number of studies with mothers and fathers and has been shown to be highly correlated with observations of parental supportive presence, sensitivity, and positive caregiving (Driscoll & Pianta, 2011).
Attachment theory also suggests that the thoughts and feelings that fathers (and mothers) have toward their children are linked to the quality of parenting, and more specifically, to parenting behaviors that promote children’s secure attachments to them (Bell & Ainsworth, 1972). Fathers who are more involved in making decisions for their children are likely to have higher levels of parenting self-efficacy, satisfaction with parenting, and role salience. We used the Network of Relationships Questionnaire to assess satisfaction with parenting (Furman & Buhrmester, 2009). The Network of Relationships Questionnaire was developed for use with youth, but it has been adapted for adults. The children’s version has been validated in several articles (see Furman & Buhrmester, 2009).
Fathers’ role salience refers to “the probability of evoking a given identity [father identity] across or within situations of interaction” (Stryker, 1991, p. 23). Bruce and Fox (1999) suggest that a father’s commitment to the parenting role determines the salience of his role identity in the identity hierarchy. We used an adapted version of father role salience (Bruce & Fox, 1999) because it has been subjected to correlation analysis to assess scale validity. The validity study included a sample of low-income African American fathers with low levels of education attainment. Bruce and Fox (1999) report that the scale appears to have good validity as it correlates well with the fathers’ opinions regarding the obligations of the father role, a lack of ambivalence in taking on the father role, and satisfaction with being a father.
Fathers’ parenting self-efficacy is broadly defined as parents’ appraisals of their competence in the parenting role (Coleman & Karraker, 2003). Studies of mothers show that parenting self-efficacy is an important determinant of competent parenting behavior and healthy child outcomes (Jones & Prinz, 2005). We used a measure that recently was developed to assess the parenting self-efficacy of low-income, nonresidential fathers in the current study. Consequently, there is no validity information available for this measure.
The current study included the following statistical controls in the convergent and predictive validity models: father’s unemployment, income, highest level of educational attainment, race/ethnicity, father’s age, target child’s age, father’s face-to-face contact with the child, nights spent with the child, and coparenting. Pleck (2010) suggests that unemployment and joblessness account for the diminished family role of the father in disadvantaged communities. Research has also shown that fathers who have higher levels of education are more likely to be involved with their children and to exhibit positive parenting behaviors than less educated fathers (Cook, Jones, Dick, & Singh, 2005). We controlled for race/ethnicity because previous studies have shown father involvement with children is greater for African American fathers than for other racial/ethnic groups (Sanderson & Thompson, 2002). We controlled for father’s age because previous studies suggest that older fathers may possess more resources that enable involvement with their children (Cooksey & Craig, 1998). We controlled for child age, as research shows that fathers spend less time with very young children than with older children (Pleck, 2010). Fathers’ involvement and responsibility is also likely to diminish when they have adolescents who are striving to achieve independence from their parents (Shumow & Lomax, 2002). We include child age squared because of the possible curvilinear relationship with decision-making responsibility. Finally, we controlled for coparenting (maternal gatekeeping) because fathers’ decision-making responsibility is likely to be influenced by the constraints that mothers place on fathers’ involvement with the child (Carlson, McLanahan, & Brooks-Gunn, 2008).
Procedures
For the validation aspect of the study, fathers were recruited from six northeastern and one southern U.S. city. Recruitment took place across 14 different fatherhood programs (n = 220 fathers) and various other nonprogram sites in high-poverty neighborhoods (n = 322 fathers) between January 2015 and June 2015. Fathers recruited from the community were approached in various neighborhood locations including grocery stores, barber shops, and churches. In order to qualify for participation in the study, fathers were required to (a) be at least 18 years of age; (b) have at least one nonresidential, biological child between the ages of 1 month and 18 years; and (c) not reside with their youngest child (target child). Nonresidence was defined as not living in the same household all or most of time. We omitted 11 fathers who indicated that they are nonresident but also said they spent every night with the target child in the past month. Twenty-six trained graduate and undergraduate students individually administered the quantitative questionnaire in these fatherhood programs and community settings. Each student read the survey forms aloud to the participating father and filled in his responses. All students received at least 3 hours of training on administering the questionnaire, obtaining informed consent, and answering participants’ questions.
Respondents completed an extensive interview regarding their involvement with one target biological child younger than the age of 18 years. In order to obtain data about children across the developmental spectrum, we attempted to target equal numbers of infants (ages 0.1-1), toddlers/preschoolers (ages 1.1-5), children in middle childhood (ages 5.1-12), and adolescents (ages 12.1-18). This was accomplished by tracking the ages of the child throughout the study. The Decision-Making Responsibility Scale was one of 17 other scales administered to the sample of 542 biological fathers. The interview included other central constructs related to parenting such as father engagement with “target” child, quality of parent–child relationship, and frequency of father–child contact.
Participant Characteristics
We created two subsamples from the overall sample of 542 fathers by randomly dividing it into two groups. The sample size for the EFA was 273 and CFA was 269 (Brown, 2015). Slightly more than 50% of participants (n = 142) in the EFA sample reported their highest level of education to be a high school diploma or GED, and 19% (n = 52) had less than a high school degree (see Table 1). More than a third of participants had one biological child (41.8%), yet, on average, fathers had slightly more than two children (2.18). Most participants were single and never married (78.8%) and African American men (70.2%).
Participant Characteristics.
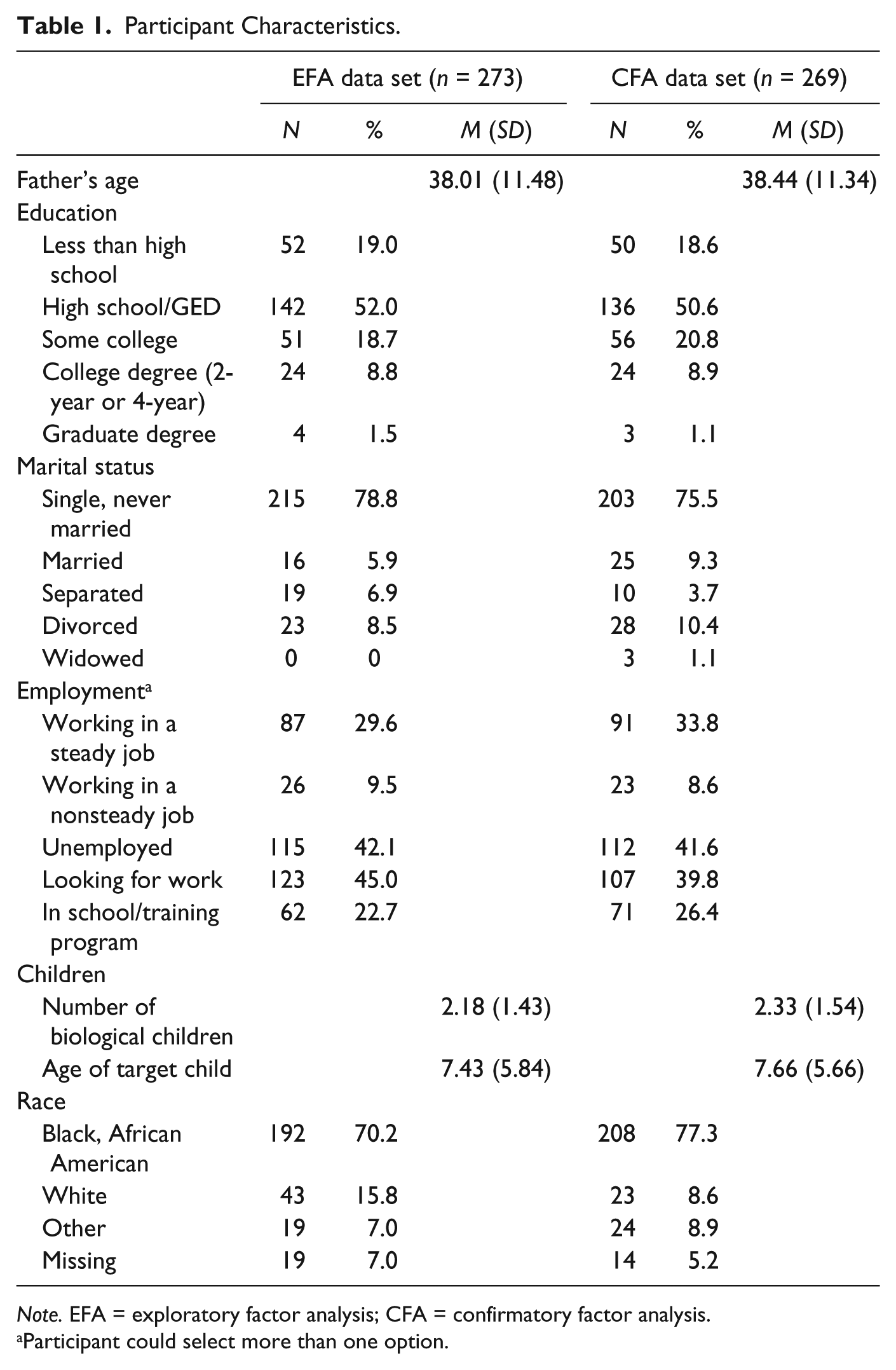
Note. EFA = exploratory factor analysis; CFA = confirmatory factor analysis.
Participant could select more than one option.
All 269 participants in the second sample were biological fathers and ranged in ages 18 to 72 with a median age of 38.44. A little more than three quarters of the sample reported their marital status as single and never married (75.5%). While most participants had a high school diploma or GED (50.6%), nearly 19% had not completed high school or obtained a GED. A smaller percentage (8.9%) had a 2-year or 4-year college degree. A little more than 40% had one biological child (40.5%), and almost 34% identified their employment status as currently unemployed.
Measures
As previously mentioned, the Decision-Making Responsibility Scale was developed from the focus group study with 71 noncustodial fathers. This nine-item scale contains a 3-point response option format: (1) the mother of the child (or another adult) always makes the decision, (2) you and the mother of the child (or another adult) share in making the decision, and (3) you always make this decision. Sample items include “Who makes decisions about which doctor the ‘target child’ will see?” and “Who makes decisions about how the ‘target child’ will be disciplined?” (A full inventory and descriptive statistics for each item are in the appendix.)
For the purpose of conducting the convergence validation study, we used the Father Involvement Scale (Hernandez & Coley, 2007), a measure of father’s nights spent with the target child, and a measure of father–child in-person contact. The Father Involvement Scale includes a total of five items, three of which were measured on a 4-point Likert-type scale ranging from none (1) to a lot (4). Sample items include “How much responsibility does [father] take for raising child?” and “How much does [father’s help] with financial and material support of the child help [mother]?” This measure also included one item: “How many hours per week does [the father] take care of the child?” The final item, “How often do you see or visit with child?” was measured on a 6-point scale, ranging from never (1) to father lives with child (6). Each item was standardized and then all items were added together to construct a composite measure of father involvement (α = .80).
Nights spent with the target child were obtained for the past 30 days. Fathers were first asked to provide information about all of their children including their age, with whom they reside, and the name of the child’s mother. Fathers were then asked to fill out a calendar indicating which specific dates, of the 30 days preceding the interview, the father had spent the night in the same residence as each child. This retrospective time diary allowed us to compile data for the total number of nights spent with each individual child and a composite of the total number of nights spent with any child (i.e., target child). To assess the frequency of father–child contact, participants were asked: “In the past month how often did you have face-to-face, in person contact with your target child on average?” Response options ranged from: every day or nearly every day (1) to not all (7).
Four measures were used to assess predictive validity of the responsibility scale: CPRS (Pianta, 1992), Satisfaction Scale (Furman & Buhrmester, 1985), Self-Perceived Competence Scale, and Father Role Salience (Fox & Bruce, 2001). The CPRS (short form) contains two subscales: a measure of closeness and a measure of conflict. This measure has been validated for children between the ages of 3 and 12 years. Each of the 15 items are rated on a 5-point scale from definitely does not apply (1) to definitely applies (5). Items include “I share an affectionate, warm relationship with my child” and “My child and I always seem to be struggling with each other.” Only the closeness subscale was used in this study (α = .89).
The Network Relationships Inventory–Relationship Qualities Version includes a three-item measure of parenting satisfaction (Furman & Buhrmester, 2009). Each item is ranked on a corresponding 5-point scale. Items include “How satisfied are you with your relationship with your target child?” and “How happy are you with the way things are between you and your target child?” The alpha reliability for the three items is .74.
The researchers adapted the seven-item father role salience measure (Fox & Bruce, 2001) to produce a 12-item measure of the degree of commitment the father derives from being in the fathering role. Participants were asked to report the degree to which they believe the item to be representative of their feelings. Sample items include “I enjoy going places my target child will enjoy” and “I prefer the company of adults to spending time with my target child.” Each item was rated on a 3-point scale from not very true of me (1) to very true of me (3). The alpha reliability for the 12 items is .65.
Finally, the Parenting Self-Efficacy Scale was developed by the authors of this article from the focus group study with 71 noncustodial fathers as a measure of how competent fathers feel in their role as a parent. This seven-item measure asks participants to rate how strongly they agree with statements such as “I am good at helping my child when he or she is upset or distressed.” Responses were rated on a 5-point Likert-type scale from strongly disagree (1) to strongly agree (5). The alpha reliability for the seven items is .92.
In regard to control variables, education was measured on a 6-point ordinal scale, with the following categories: less than high school, high school diploma or GED, some college, 2-year degree, 4-year degree, and graduate degree. Unemployment was assessed as a dummy variable (1 = unemployed, 0 = employed). Race/ethnicity was assessed through four mutually exclusive dummy variables: Black, non-Hispanic (reference group); White, non-Hispanic; Hispanic; and Other, non-Hispanic. Age of target child (squared) and father were incorporated as continuous variables. We assessed mother–father coparenting using three items measuring maternal gatekeeping specifically developed for this study. A sample item is “The mother of my child makes it hard for me to spend time with my child.” Response options ranged from: strongly disagree (1) to strongly agree (5). These items were added together to construct a measure of gatekeeping (α = .85).
Analysis Plan
All models were fit using Mplus 7.31 with full information maximum likelihood used to handle missing data. The amount of missing data for the Decision-Making Responsibility Scale ranged from 5 (0.9%) for the item about decisions regarding what to buy for children to 54 (10%) for decisions about what religion children will practice. We initially conducted an EFA to determine the number of factors and obtain an initial sense of the factor structures. In factor analyses, it is important to make the appropriate distributional assumptions about the factor indicators. We therefore explored whether to specify the indicators as continuous or ordered categories. Since the indicators themselves suggest a continuous distribution, the continuous specification may fit the data better. However, since the indicators have only three response categories, it may be that specifying the indicators as categorical more appropriately captures the nature of the indicators. Given the responses are skewed along the three categories, when specifying the model as continuous, we used the maximum likelihood estimation with robust standard errors (MLR) estimator rather than the typical ML estimator since MLR is robust to nonnormal data. For EFA, we used the Mplus default of oblique Geomin (OB) rotation (correlated factors) because it was developed to allow for complex factors and provide an interpretable pattern matrix.
Following the determination of the number of factors and the appropriate distribution to specify (continuous or categorical), a CFA was conducted. This included any cross-loadings that appeared in the EFA. We considered unstandardized loadings greater than .30 to be indicative of a cross-loading. Both conceptual and statistical criterion (chi-square difference test, Δχ2) were used to determine whether these cross-loadings should be retained.
Model fit is also important to examine in both EFA and CFA analyses. Model fit indices used included the root mean square error of approximation (RMSEA; <.06 for good model fit), the confirmatory fit index (CFI; >.95 for good model fit), and standardized root mean square residual (SRMR; <.08 for good model fit; Hu & Bentler, 1999). Again, the sample was randomly divided in two (one for EFA and the other for CFA) so as to avoid capitalizing on chance sample-specific characteristics (Brown, 2015).
Convergent and predictive validity were then examined using the full sample. To determine the relative contribution of both factors, several models were fit. First, a model that only considered controls was estimated. Then, including all controls, the following iterations of the model were fit: (a) a model containing both care and resource factors; (b) a model where the care and resource factors were combined into a single factor (i.e., all items loading on the same factor); (c) a model containing only the care factor, and (d) a model containing only the resource factor. Fitting these four models aided in determining the degree to which each factor displayed some unique relationship with the convergent and predictive validity constructs.
Results
Exploratory Factor Analysis
Table 2 contains parameter estimates and model fit information for EFA results. When specifying factors as continuous (with MLR estimator), the one- and two-factor solutions both had eigenvalues above 1.00. For the two-factor solution, all indicators that had been predicted to load on care decision making (care factor) and resource decision making (resources factor) loaded above .30 (evidence for the hypothesized relationship between items and the responsibility dimensions). In addition, there was one indicator from the care dimension that loaded onto the resources dimension (“care,” loading = .302) and one item from the resources dimension that loaded onto the care dimension (“school,” loading = .344). We therefore examined possible cross-loadings in the CFA model. The two-factor model fit the data acceptably (RMSEA = .073, CFI = .955, SRMR = .034).
Standardized Parameter Estimates (Standard Errors) for EFA of Care and Resource Responsibility (n = 273).
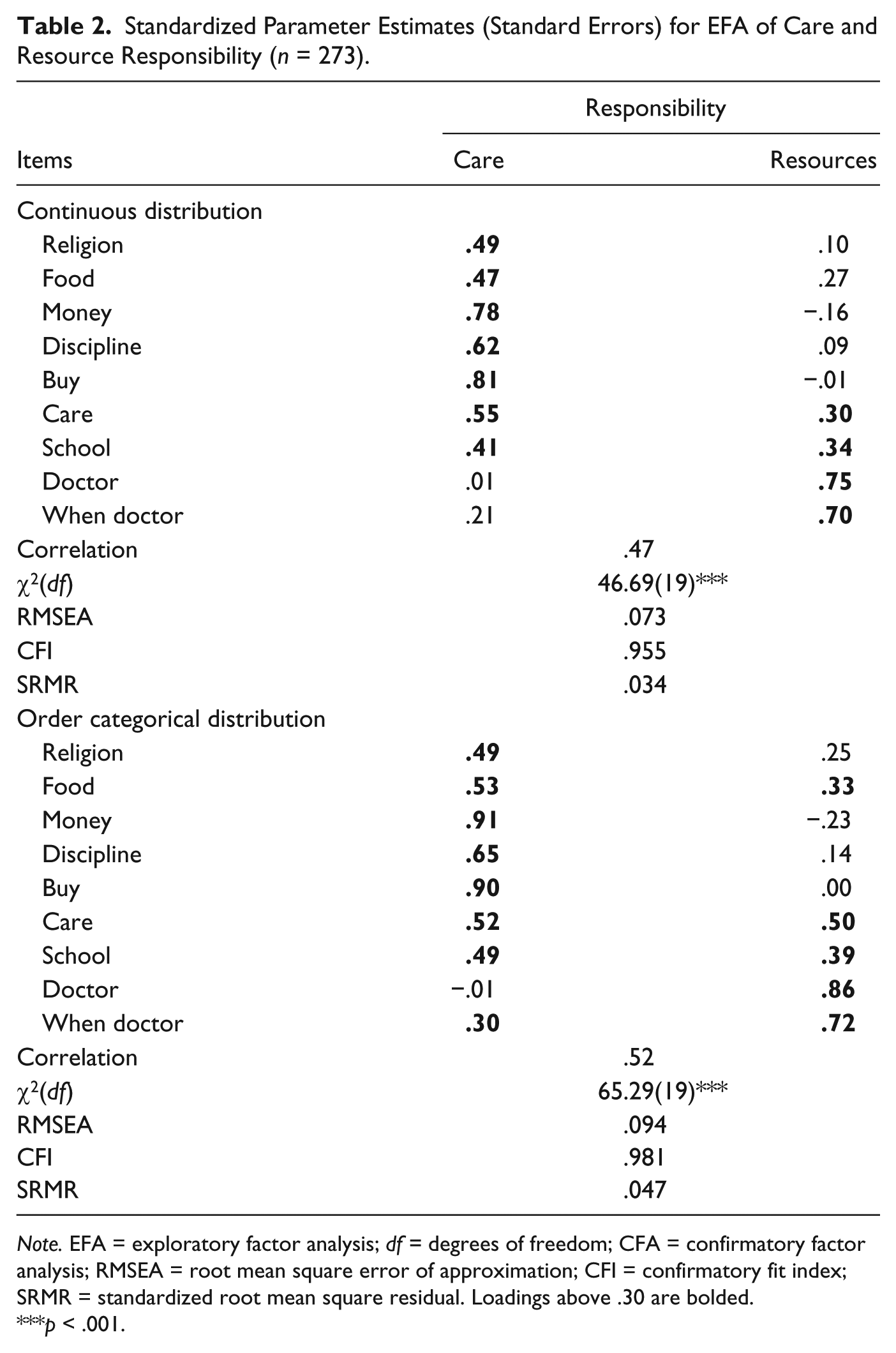
Note. EFA = exploratory factor analysis; df = degrees of freedom; CFA = confirmatory factor analysis; RMSEA = root mean square error of approximation; CFI = confirmatory fit index; SRMR = standardized root mean square residual. Loadings above .30 are bolded.
p < .001.
When specifying factors as categorical, both the one- and two-factor solutions had eigenvalues above 1 (5.468 and 1.010). The two-factor solution fit the data acceptably (RMSEA = .094, CFI = .981, SRMR = .047), although the RMSEA indicated poor model fit. In the two-factor solution, all indicators predicted to load on care and resource responsibility loaded above .30. There was also evidence of cross-loadings for the items “school,” “care,” “deciding when to go to the doctor,” and “food.”
The continuous and categorical models both provided similar solutions. However, the RMSEA and CFI indicated good model fit for the continuous specification, whereas the RMSEA for the categorical specification indicated a poor model fit. Also, the continuous model had a simpler and more interpretable structure (fewer cross-loadings). That is, the conceptual separation between the two factors was greater. Furthermore, when specifying a CFA with categorical indicators versus continuous, more parameters are needed for estimation which further complicates the model. It was therefore determined that the model with items specified as continuous would be used for the CFA.
Confirmatory Factor Analysis
Table 3 contains details of the CFA that included the cross-loadings for the items “care” and “school.” The model fit the data well (RMSEA = .052, CFI = .966, SRMR = .038) with all loadings being above .30 except the loading of “care” on the resources factor (λ = .17). To determine whether to retain the cross-loading for this item a Δχ2 test (with the Satorra–Bentler correction factor) was used. Although the p value indicated a significantly worse fit (p = .038) change in other fit indices indicated little decrement in model fit (ΔRMSEA = .003, ΔCFI = −.006, ΔSRMR = .002). Due to these minor changes in model fit and the small loading, it was determined to accept the more parsimonious model and eliminate this cross-loading.
Standardized Parameter Estimates (Standard Errors) for CFA of Care and Resource Responsibility With “Care” and “School” Items Cross-Loading (n = 268).
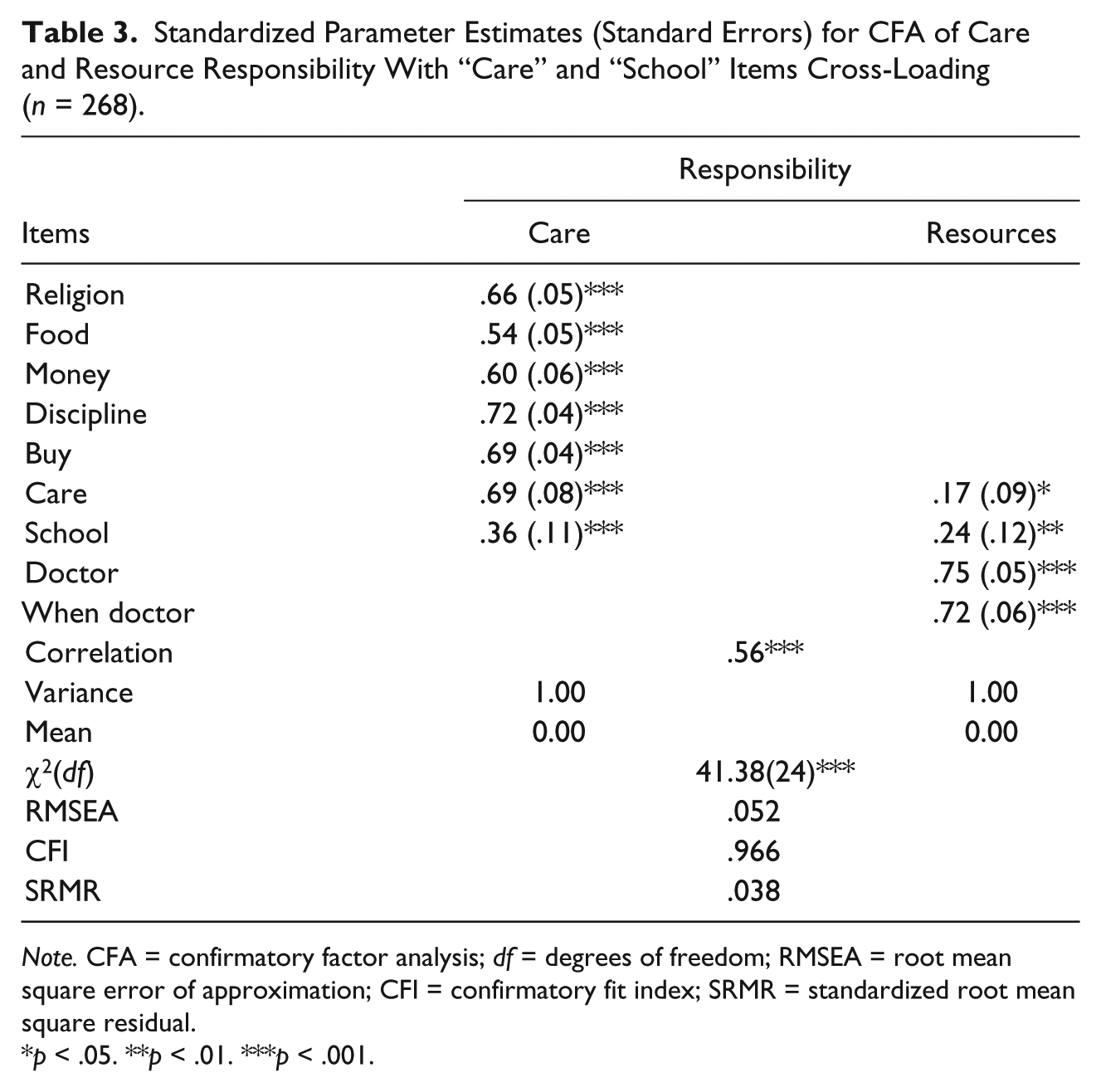
Note. CFA = confirmatory factor analysis; df = degrees of freedom; RMSEA = root mean square error of approximation; CFI = confirmatory fit index; SRMR = standardized root mean square residual.
p < .05. **p < .01. ***p < .001.
When examining the cross-loading of the “school” item on the care factor, the Δχ2 test was highly significant (p < .001) and other model fit indices indicated a much worse fitting model such that the RMSEA and CFI both indicated inadequate model fit (RMSEA = .069, CFI = .934, SRMR = .053). We therefore determined to include this cross-loading. Table 4 contains parameter estimates of this final CFA model.
Final CFA Model: Standardized Parameter Estimates (Standard Errors) for CFA of Care and Resource Responsibility With the “School” Item Cross-Loading (n = 268).
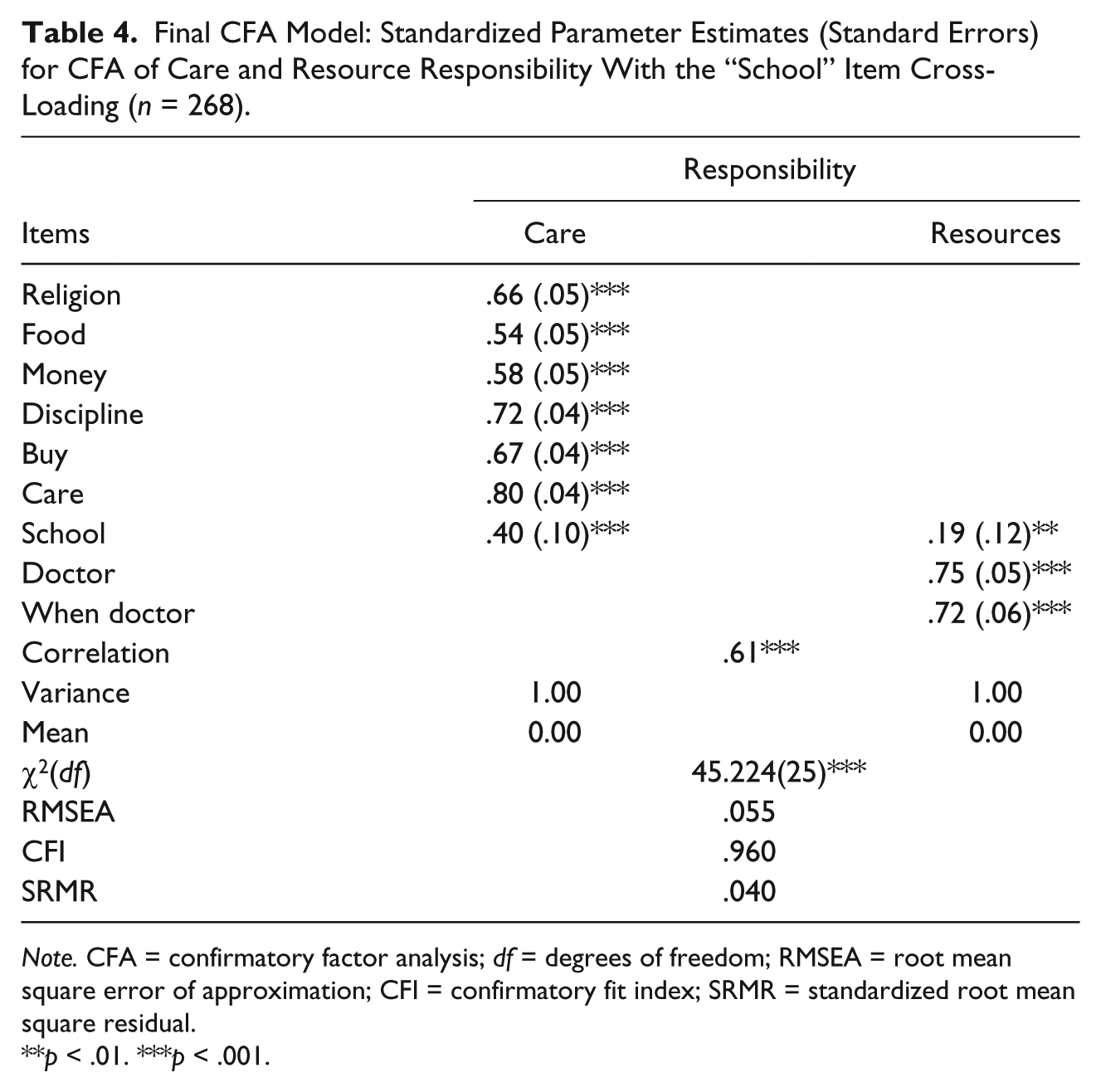
Note. CFA = confirmatory factor analysis; df = degrees of freedom; RMSEA = root mean square error of approximation; CFI = confirmatory fit index; SRMR = standardized root mean square residual.
p < .01. ***p < .001.
We also examined the reliability of the scales using Cronbach’s alpha. Although there are known issues with Cronbach’s alpha (see Dyer, 2015), it does provide a baseline level of reliability (i.e., given measurement error is removed, reliability for scales will be higher in the CFA context). Cronbach’s alpha for the care factor was .83 and for the resources factor, it was .70 indicating good reliability for both scales.
Convergent Validity
All convergent and predictive validity models control for father’s employment, income, race (White, Black, Other), education, age, and child’s age. Predictive validity models also included controls for convergent validity constructs (involvement, nights per month, and face-to-face contact). First, a model with controls only was fit. Then, including all controls, the following iterations of the model were fit: (a) a model containing both care and resource factors; (b) a model where the care and resource factors were combined into a single factor (i.e., all items loading on the same factor); (c) a model containing only the care factor; (d) a model containing only the resource factor. Fitting these four models aided in determining the degree to which each factor has some unique relationship with the convergent and predictive validity constructs. All models fit the data well with RMSEA ranging from .00 to .047, CFI ranged from .913 to 1.000, and SRMR ranged from .017 to .063.
See Table 5 for convergent and predictive validity models. Results were similar across the three convergent validity constructs (involvement, nights per month, face-to-face contact). In each case when both factors were included, only the care factor significantly predicted the convergent validity construct. In the “care only” models (i.e., the resource factor was not in the model), the care factor predicted as much variance in the convergent validity construct as when both care and resource constructs were included. The care factor, by itself, also predicted as much variance as when both care and resource factors were combined into a single factor (except for face-to-face contact where the “care only” model predicted 1% less of the variance vs. the combined factor model). When only the resource factor was included, it predicted less variance than the care factor did by itself and less variance than the combined factor.
Convergent and Predictive Validity Results (N = 542).
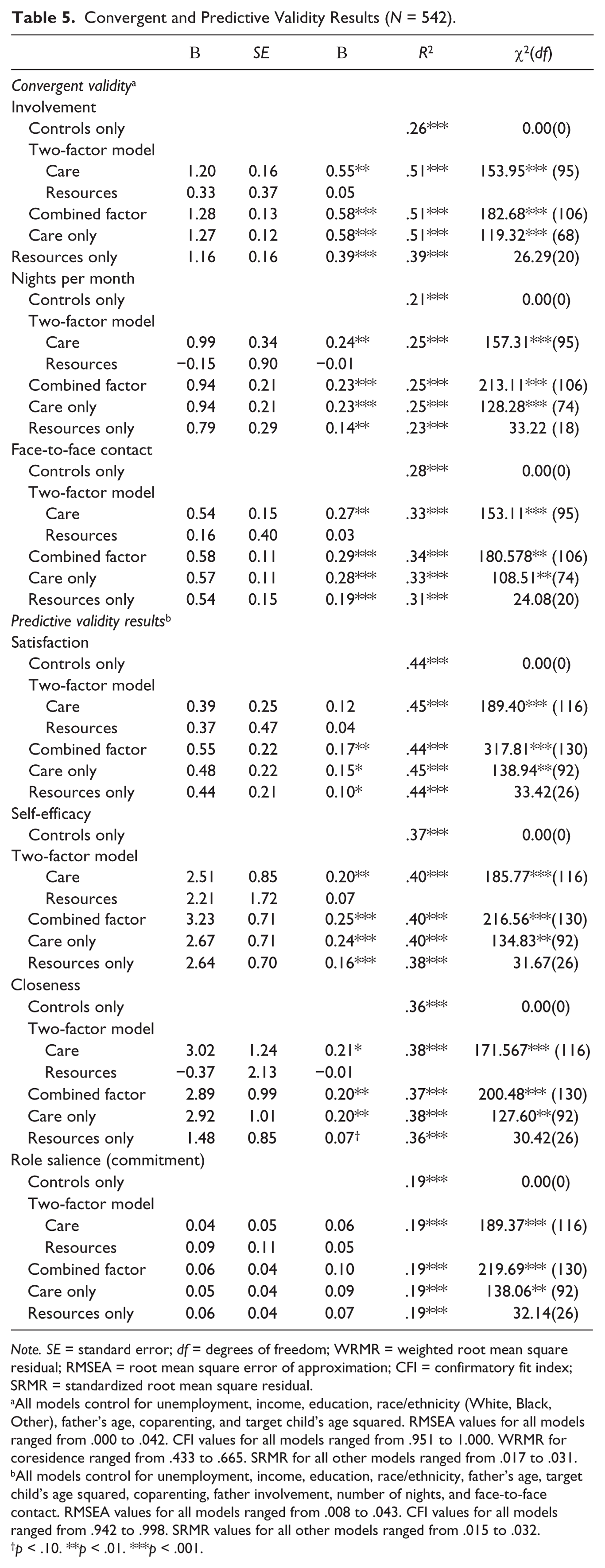
Note. SE = standard error; df = degrees of freedom; WRMR = weighted root mean square residual; RMSEA = root mean square error of approximation; CFI = confirmatory fit index; SRMR = standardized root mean square residual.
All models control for unemployment, income, education, race/ethnicity (White, Black, Other), father’s age, coparenting, and target child’s age squared. RMSEA values for all models ranged from .000 to .042. CFI values for all models ranged from .951 to 1.000. WRMR for coresidence ranged from .433 to .665. SRMR for all other models ranged from .017 to .031. bAll models control for unemployment, income, education, race/ethnicity, father’s age, target child’s age squared, coparenting, father involvement, number of nights, and face-to-face contact. RMSEA values for all models ranged from .008 to .043. CFI values for all models ranged from .942 to .998. SRMR values for all other models ranged from .015 to .032.
p < .10. **p < .01. ***p < .001.
Regarding the amount of variance predicted, models that included the combined factor or only the care factor (models that predicted the most variance) predicted between 4% and 25% more variance than the model with controls only.
Predictive Validity
For self-efficacy and closeness, when both care and resources are included in the model, the care factor is significantly related to the outcome, whereas the resource factor is not. Furthermore, when included by itself the resource factor predicted less variance than in any of the other models except the “control only” models. Also, when comparing the “care only” model to the model that combines both care and resources into the same factor, the “care only” model predicts at least as much, if not more, variance than the combined factor.
For satisfaction, in the two-factor model, neither care nor resources significantly predicted the outcome. However, the combined factor did significantly predict the outcome as did the care only, and resources only model. The most variance was explained in the two-factor model and the care model (45% of the variance) though this was only 1% more than the controls only model. In the role salience models, neither care nor resources in any combination predicted the outcome.
Regarding the amount of variance predicted, the “combined factors” model and the “care only” model predicted between 1% and 3% more variance above the model with controls only (excepting the role salience model which did not predict any additional variance). We also fit all predictive validity models that excluded convergent validity items as controls (i.e., involvement, nights per month, and face-to-face contact). This was important since it is expected that there are parts of the variance in the convergent validity items that are likely valid parts of decision making (i.e., they should have conceptual overlap). Thus, when we controlled for them, we were likely removing some of the variance that validly belongs to the decision-making scale. In models where these convergent validity items were removed the amount of additional variance explained by the combined decision-making models and care only models was between 17% and 19%. In these models, the resource factor still did not predict any unique variance.
Discussion
Practitioners and policy makers have noted a lack of validated and relevant measures available for fatherhood programs serving primarily low-income, unmarried, nonresident fathers (Osborne et al., 2014). This study contributes to the fathering field by developing and validating a new measure of fathers’ responsibility for children. Furthermore, responsibility has been the least well conceptualized construct of fathering in the model of father involvement developed by Lamb et al. (1987). Although there is currently one validated measure of father involvement available for low-income, nonresidential fathers (Hernandez & Coley, 2007), this measure includes only one item regarding fathers’ responsibility, and it does not address decision making.
The first goal of this project was to obtain fathers’ own perceptions of what is meant by taking responsibility for children. Although fathers in our focus groups provided a variety of opinions about what it means to take responsibility for children, we consistently heard fathers refer to making decisions about children as an important component of this construct. These findings are consistent with the theoretical work of researchers such as Stueve and Pleck (2003) who suggest that responsibility encompasses both the organizing and managing of arrangements for the child. Organizing and managing children’s lives is a multifaceted construct, and making decisions on behalf of children is one component of this construct. Making decisions may be particularly important to nonresident fathers because they often struggle to become involved in this aspect of parenting (Roy et al., 2008). Our qualitative results supported our efforts to develop and test a quantitative measure of decision making with a sample of low-income, nonresident fathers.
Our exploratory study of the new quantitative measure (EFA) and the verification of its factor structure (CFA) resulted in the identification of two unique factors, which we referred to as care and resource decision making. Tests of convergent validity showed the care factor alone or the combined care and resource factors proved to be better predictors than the resource factor alone. A similar pattern was found when testing for predictive validity. It is not surprising that the resources factor did not predict much, if anything, above the care factor, given the narrow conceptual range of the resources items (they focused almost exclusively on decisions about medical care). Medical care decisions are relatively infrequent. Even fathers who are highly involved in medical decisions likely only engage with it every few months. It is therefore unlikely to have any substantial impact on the validity constructs.
It was noteworthy that our decision-making responsibility measure was not significantly related to fathers’ role salience in the predictive validity analyses. One possible reason for this finding is that the role salience measure had low reliability. The measure of role salience used in this study (Fox & Bruce, 2001) has not been tested previously with this population. Another possible explanation is that fathers responded to the role salience items in a socially desirable manner. That is, fathers may have indicated that the fathering role is important to them because it is uncomfortable to admit that being a father is not as salient to them as other roles.
A potential criticism of the new decision-making responsibility measure is that it is actually a measure of coparenting. For example, the midpoint response category for the decision-making items in this study was “mother and father share making decisions.” Importantly, the current measure only examines how much responsibility the father assumes rather than being a measure of the separate construct coparenting. Coparenting includes dimensions such as gatekeeping, alliance, and undermining. These are not a part of the current measure and may function independent of it. (We controlled for gatekeeping in the current study.) A father may have a good coparenting relationship with the mother of the child but assume no responsibility. Or the father may have a very poor coparenting relationship with the mother but assume a great deal of responsibility. What we assume here is that, independent of the coparenting relationships, the father’s decision making will have an impact. It will be important for future research to develop measures of coparenting for nonresident fathers and examine its interplay with responsibility.
Several limitations of this study should be noted. The majority of participants in this study were African American. Thus, the results may be more applicable to African American fathers than to other racial/ethnic groups. Another limitation is that this measure does not address all aspects of fathers’ responsibility for children (e.g., monitoring what the child needs). Future studies may explore developing measures of arranging children’s time. Additional studies are also needed to determine the predictive validity of this measure in relation to child outcomes. Despite these limitations, this new measure should help to fill a significant gap—it provides a validated measure of decision-making responsibility for low-income, nonresident fathers.
In conclusion, although we identified a two-factor solution for decision-making responsibility, the results of our convergent and predictive validity tests suggest that the resources factor does not appear to add additional explanatory power above its association with the care factor. Thus, the resource items could potentially be dropped for a shortened scale. Moreover, these findings seem to suggest the importance of assessing low-income, nonresident fathers’ participation in decision making about direct care for children because it is closely tied to fathers’ parenting attitudes and quality of father–child relationships. We suggest using only the seven care decision-making items in future studies. Fatherhood programs may find this short validated measure of decision-making responsibility useful for evaluating the impact of their program on fathers and children.
Footnotes
Appendix
Decision-Making Responsibility Measure Items.
| Read: In this next section I am going to ask you who makes decisions about your target child [NAME OF CHILD]. Please let me know if the mother of the child (or another adult) always makes the decision, if you and the mother of the child (or another adult) share in making the decision, or if you always make the decision. | ||||
|---|---|---|---|---|
| The mother of the target child (or another adult) always makes the decision | You and the mother of the target child (or another adult) share in making the decision | You always make the decision | M (SD) | |
| 1. Who makes decisions about where [NAME OF TARGET CHILD] will go to school or day care? | 1 | 2 | 3 | 1.44 (0.55) |
| 2. Who makes decisions about what religion [NAME OF TARGET CHILD] will practice? | 1 | 2 | 3 | 1.73 (0.68) |
| 3. Who makes decision about which doctor [NAME OF TARGET CHILD] will see? | 1 | 2 | 3 | 1.34 (0.55) |
| 4. Who makes decisions about what foods will be available to eat at home? | 1 | 2 | 3 | 1.48 (0.59) |
| 5. Who makes decisions about how much money will be spent on clothes for [NAME OF TARGET CHILD]? | 1 | 2 | 3 | 1.76 (0.67) |
| 6. Who makes decisions about how [NAME OF TARGET CHILD] will be disciplined? | 1 | 2 | 3 | 1.83 (0.66) |
| 7. Who makes decisions about what to buy for [NAME OF TARGET CHILD]? | 1 | 2 | 3 | 1.68 (0.57) |
| 8. Who makes decisions about when [NAME OF TARGET CHILD] will go to the doctor? | 1 | 2 | 3 | 1.35 (0.54) |
| 9. Who makes decisions about who will care for [NAME OF TARGET CHILD]? | 1 | 2 | 3 | 1.70 (0.55) |
Note. Items 1, 2, 4, 5, 6, 7, and 9 loaded on the “care” factor. Items 1, 3, and 8 loaded on the “resources” factor.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the Department of Health and Human Services, Administration for Children and Families (Office of Planning, Research, and Evaluation), Grant #90PR0006.