
Abstract
Introduction
In terms of transmission, impact, and potential for changing the attitudes and behaviors that underlie HIV/AIDS (human immunodeficiency virus/acquired immunodeficiency syndrome), adolescents are at the center of the global pandemic. Approximately 2 million adolescents between the ages of 10 and 19 years are living with HIV worldwide (UNICEF, 2016). However, in the United States, youth of color are at persistent risk for HIV infection. African American adolescents and young adults exhibit rates of HIV and STIs (sexually transmitted infections) that are significantly higher than their White, non-Hispanic peers (Centers for Disease Control and Prevention [CDC], 2012a). Although African American adolescents represent 15% of the U.S. adolescent population, they constitute 67% of reported HIV cases (CDC, 2014b). Also, the rate of new infections among young African American males aged 13 to 24 years is 11 times as high as that of young white males and 4 times as high as that of young Hispanic males (CDC, 2014a).
Overall, sexual risk behaviors are more prevalent in African American than White or Latino male adolescents. Among high school students, African American males have the highest rate of current sexual activity of all racial/ethnic groups (CDC, 2012b). The prevalence of having had sexual intercourse before age 13 years is higher among black males (21.1%) when compared with white males (5.2%; CDC, 2012b). African American male high school students (32.6%) were more likely than Hispanic and White students (20.3% and 13.3%, respectively) to report having four or more sexual partners by the end of 12th grade (CDC, 2012b). Increased rates of HIV/STI infection can be related to differences in the cumulative exposure to risk factors associated with condom use among adolescents, including family processes (Browning, Levanthanl, & Brooks-Gunn, 2005). Since adolescent sexual activity occurs within a broacher ecological context and is influenced by a myriad of factors at the individual, partner, peer, family, and community systems levels (Bronte-Tinkew, Moore, & Carrano, 2006; Hutchinson, 2007; E. K. Wilson & Koo, 2010); there has been a move toward understanding the role of parents on the sexual behaviors of their children.
Parental factors have been identified as potential influences on sexual attitudes and outcomes among adolescents including parental monitoring (V. Burns, 2008; Markham et al., 2003; Regnerus & Luchies, 2006; Rink, Tricker, & Harvey, 2007; Rose et al., 2005; Wight, Williamson, & Henderson, 2006), parent–child sexual risk communication (PCSRC; DiLorio, Pluhar, & Belcher, 2003; Hadley et al., 2009; Hutchinson & Montgomery, 2007; Kapungu et al., 2010; Udell & Donenberg, 2011; Udell, Donenberg, & Emerson, 2011; E. K. Wilson, Dalberth, & Koo, 2010; E. K. Wilson & Koo, 2010), and parent sexual socialization (DiLorio et al., 2003; Shtarkshall, Santelli, & Hirsch, 2007). Father involvement, relationship quality, and communication all have critical benefits for adolescents (Guilamo-Ramos et al., 2012; Harper & Fine, 2006; Hutchinson & Cederbaum, 2011; Julion, Breitenstein, & Waddell, 2012; Wong, Roubinov, Gonzales, Dumka, & Millsap, 2013); yet fathers are significantly underrepresented in studies of parental influences on adolescent sexual practices and risk behaviors (Bronte-Tinkew et al., 2006; Harris, Sutherland, & Hutchinson, 2013; Hutchinson & Cederbaum, 2011; Pingel et al., 2012; E. K. Wilson et al., 2010) and PCSRC (J. Burns & Caldwell, 2015; Dilorio, McCarty, Resnicow, Lehr, & Denzmore, 2007; Hutchinson & Cederbaum, 2011; Hutchinson & Montgomery, 2007; E. K. Wilson et al., 2010).
Despite the benefits of PCSRC for adolescents, sexual risk communication literature demonstrates that parents (both mothers and fathers) have fewer and less detailed conversations with their sons about sex (Dilorio et al., 2003; Kapungu et al., 2010; Udell & Donenberg, 2011; E. K. Wilson & Koo, 2010). A recent study by E. K. Wilson and Koo (2010) found that parents were more likely to believe sexual behavior to be less detrimental (i.e., psychological and physical effects) for sons than daughters. Examples of these types of gender differences have been found among other families across various ethnicities, including African American families (E. K. Wilson et al., 2010). Thus, there is a need for additional PCSRC research focusing specifically on sons.
Sixty percent of African American children reside in homes without their biological father in residence (compared with 40% Latino and 24% Whites, respectively; Carlson, McLanahan, & Brooks-Gunn, 2008). Although a significant number of African American fathers live in separate households from their children, the majority highly value being a father and desire to be consistently involved in their children’s lives (Cabrera, Ryan, Mitchell, Shannon, & Tamis-Lemonda, 2008; Julion, Gross, McLaughlin, & Fogg, 2007). Research has shown that higher levels of father involvement are associated to a number of improved child outcomes (Harper & Fine, 2006). For example, a longitudinal study conducted by Bronte-Tinkew and colleagues (2006) found that adolescents who have a father with an authoritative parenting style have a reduced risk of engagement in delinquency and substance abuse. Furthermore, the father–child relationship was more influential on risk behaviors of male than female adolescents (Bronte-Tinkew et al., 2006). Glenn, Demi, and Kimble (2008) examined family hardiness, fathers’ perceptions of adolescent self-efficacy to be abstinent and/or practice safe sex, and the influence of parental communication of adolescent sexual standards on adolescent sons among a sample of African American fathers (N = 70) from the South. In this study, the greater the son’s perception of the communication of sexual standards by his father, and the greater the father’s perceptions of his son’s self-efficacy were both significantly associated with enhanced self-efficacy for abstinence among the sons (Glenn et al., 2008). J. Burns and Caldwell (2015) examined characteristics of father–son relationships that best predict communication about sex among a sample of nonresident African American fathers and their adolescent sons. Their analysis found that fathers who do not live with their sons but who monitor their children are more likely to communicate with those sons about sexual health issues (J. Burns & Caldwell, 2015).
Several PCSRC programs for mothers and children have been developed and tested, while few programs have been developed and implemented specifically for father and sons (Dilorio et al., 2007). Dilorio and colleagues (2007) developed a HIV intervention program “R.E.A.L. MEN” for adolescent sons and their fathers. This intervention based on the social cognitive theory was developed for fathers and sons (ages 11-14 years). Outcomes for the intervention included delay of sexual intercourse, condom use among the sons that were sexually active, and increased PCSRC between fathers and sons (Dilorio et al., 2007). This study demonstrated positive effects of PCSRC on engagement in protective behaviors (e.g., enhanced rates of condom use, enhanced rates of abstinence, and delayed sexual debut) among the sons that participated in the study (Dilorio et al., 2007). However, sexual communication outcomes for the sons were not significant. This study has served as a foundation for subsequent research studies with African American fathers and sons (Caldwell, Bell, Brooks, Ward, & Jennings, 2011). Caldwell and colleagues (2011) developed a theory-based, culturally specific family intervention for African American fathers and sons (ages 8-12 years) that enhanced parenting attitudes and behaviors of nonresident African American fathers. The theoretical foundations for this study included the theory of reasoned action (TRA), social cognitive theory (SCT), and community-based participatory research (CBPR). The study also examined the effects of the intervention on father–son interactions, intentions to avoid violence, and aggressive behaviors among sons. The intervention “Fathers and Sons” was effective in influencing a number of protective factors for the sons, and it increased the fathers’ intentions to communicate with their sons about sex (Caldwell et al., 2011). All these studies suggest that more comprehensive research is needed to determine and assess the influences of parenting practices particularly PCSRC among African American fathers and its influence on adolescent male engagement in sexual risk behaviors.
To enhance the understanding of father involvement on the sexual behaviors of African American adolescent sons, the purpose of this study was to explore (1) PSCRC between African American fathers and adolescent sons and (2) the feasibility of implementing an HIV/STI intervention program for African American fathers and sons.
Theoretical Frameworks
Intervention programs based on solid theoretical frameworks and elicitation research with members of the study population are the most effective in changing HIV risk-associated sexual behavior (J. B. Jemmott, Jemmott, & Fong, 2010; L. S. Jemmott, Jemmott, Lanier, Thompson, & Baker, 2017; L. S. Jemmott, Jemmott, & O’Leary, 2007). The theory of planned behavior (TPB; Ajzen, 1991) and the parent-based extension of the TPB (PETPB) were the theoretical frameworks for this study (Hutchinson & Wood, 2007). TPB provides a framework for researchers to examine attitudes toward behavior and develop effective intervention programs. TPB posits that behavioral intentions are influenced by one’s attitude positive or negative toward performing the behavior (Ajzen, 2002), subjective norms about the behavior (the perception that those important to him approve/disapprove of the behavior), and control of one’s behavior (the degree to which carrying out the behavior is under the individual’s volitional control; Ajzen, 1985). According to Fishbein (1995), elicitation research based on TPB is used to identify (1) perceived outcomes, (2) relevant referent groups, (3) facilitators and barriers, (4) characteristics and qualities, and (5) alternatives to said action. PETPB exerts that Parent–Teen Sexual Risk Communication (PTSRC) is one of the most important influences of adolescent sexual risk behaviors (Hutchinson & Wood, 2007). In PETPB, the adolescents’ intentions remain the primary determinant of engaging in sexual acuity including unprotected sex or condom use. Also, sexual risk–related intentions are still primarily determined by the adolescent’s behavioral, normative, and control beliefs. In PETPB, parents’ intentions to engage in PTSRC are determined by their behavioral beliefs, normative beliefs, and control beliefs regarding the behaviors (Hutchinson & Wood, 2007). Thus, a family-based intervention program would be designed to alter adolescent sexual behavior by changing parenting beliefs and intentions regarding PTSRC (Hutchinson & Wood, 2007). The PETPB model also allows for exploration of community and social factors that might influence parents and adolescents, their beliefs and intentions, and adolescents’ sexual risk–related behaviors, such as cultural differences and nuances (Waldron, Hutchinson, Hewitt, Kahwa, & Hamilton, 2012). Based on experience in development of effective HIV/STI prevention programs using mixed method approaches (Baker et al., 2012; Brawner, Baker, Leader, et al., 2013; L. S. Jemmott, Jemmott, Hutchinson, Cederbaum, & O’Leary, 2008; L. S. Jemmott et al., 2017; Jones, Baker, Gelaude, King, & Jemmott, 2013), we conducted elicitation research based on TPB and PETPB to assess theoretical mediators of fathers/father figures as proximal influences of adolescent sexual behavior and to assess the feasibility of a father–son HIV/STI prevention program.
Method
Study Population and Recruitment
A convenience sample of African American fathers was recruited to participate in the study (see Table 1). Recruitment flyers were designed by the research team and were IRB approved. The barbershop owner of Philly Cuts barbershop used the flyers to recruit adult male clients for participation in the study. Interested participants called the number on the flyer to be screened for eligibility by a research team member. Fathers were eligible to participate if they (1) were the biological father/guardian, stepfather, or father figure (ex. grandfather, uncle, brother, family friend, mentor) of an African American adolescent male (between the ages of 11 and 17 years) who could participate with them, (2) lived in Philadelphia, Pennsylvania, and (3) were able to read, write, and speak English. Focus groups occurred 3 weeks after participants were recruited. The Institutional Review Boards of La Salle University and the University of Pennsylvania approved the study.
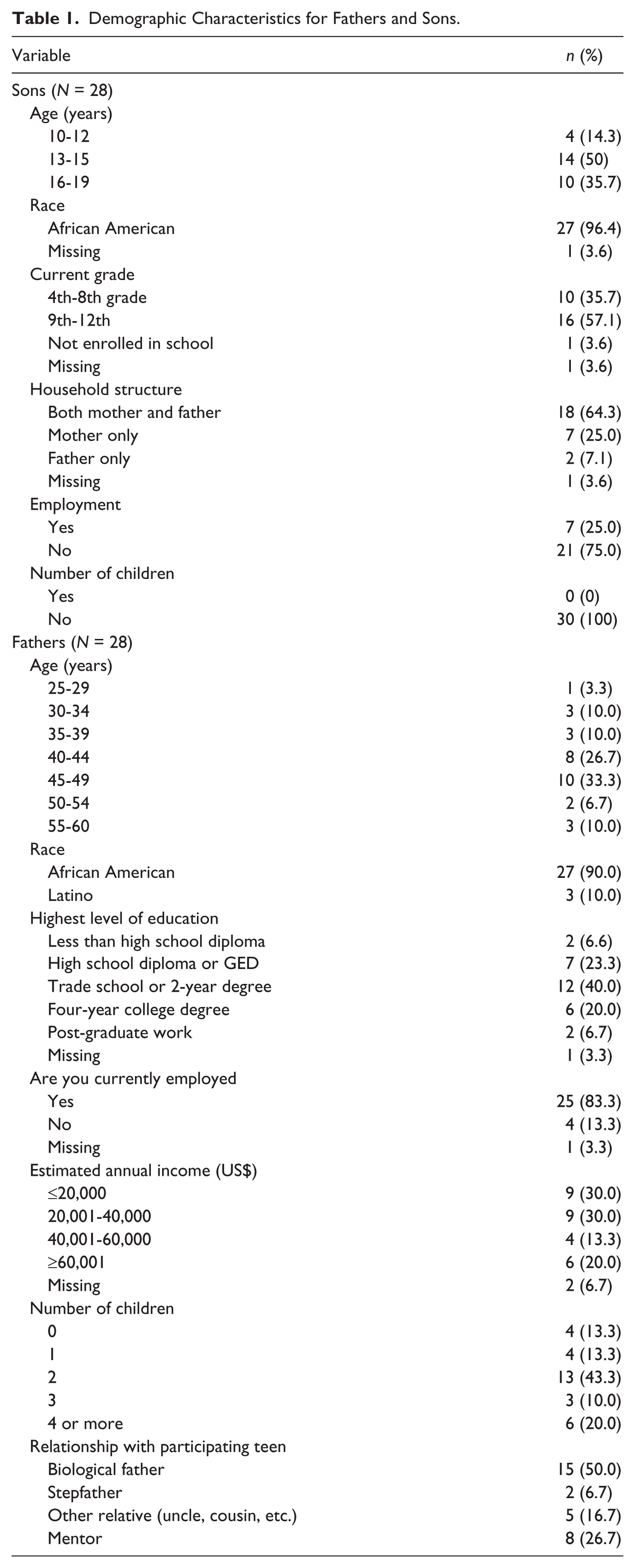
Demographic Characteristics for Fathers and Sons.
Focus Group Guides
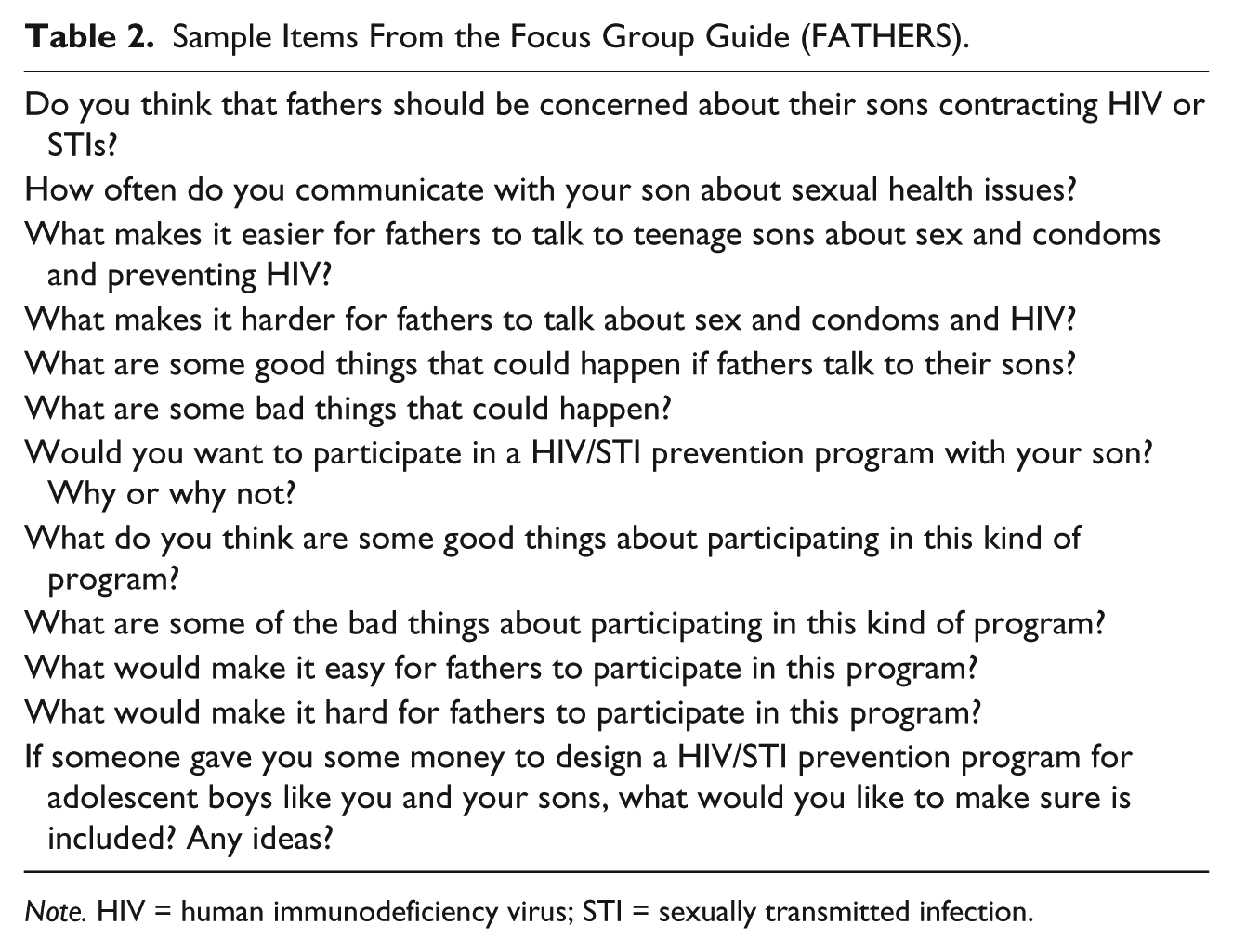
Semistructured focus group guides were developed to lead the conversations with fathers and sons. (Krueger & Casey, 2009) have noted the necessity of elicitation procedures prior to development of assessment instruments, including focus groups. Specifically, elicitation work is used to identify (1) perceived outcomes, (2) relevant referent groups, (3) facilitators and barriers, (4) characteristics and qualities, and (5) alternatives to said action (Fishbein, 1995). In the development of the focus group guides, tenets of both the TPB and PETPB were incorporated. The final scripts (see Tables 2 and 3 for selected questions from the focus group guides) incorporated questions related to attitudes and beliefs regarding PTSRC, HIV/STI knowledge, and preliminary information on the design of a culturally relevant, theory-based HIV/STI risk reduction intervention for African American fathers and sons. Sample questions included the following: “How often do you communicate with your son about sex?,” “Would you want to participate with your father in a program about sex?,” “What are some of the good things about fathers attending a program like this?,” and “What are the barriers to participating in a program like this with your father?”
Sample Items From the Focus Group Guide (FATHERS).
Note. HIV = human immunodeficiency virus; STI = sexually transmitted infection.
Sample Items From the Focus Group Guide (SONS).

Note. HIV = human immunodeficiency virus; STI = sexually transmitted infection.
Questionnaires
Fathers and sons completed an eight-page self-administered survey prior to the commencement of focus group sessions that included sociodemographic information, knowledge and attitudes about HIV/STIs, PCSRC, and sexual behaviors (adolescents only). Table 4 highlights the items developed based on TPB and PETPB to assess (1) fathers’ beliefs regarding PTSRC and (2) sons’ beliefs regarding receipt of PTSRC. Table 5 highlights items related to participation interest in a father/son HIV/STI prevention program. Ratings for these questions were on a 5-point Likert scale from very negative to very positive. The survey also includes questions about possible topics to be included in a father/son HIV/STI prevention program (refer to Tables 6 and 7). Ratings for these questions were on a 3-point Likert scale from very negative to very positive.
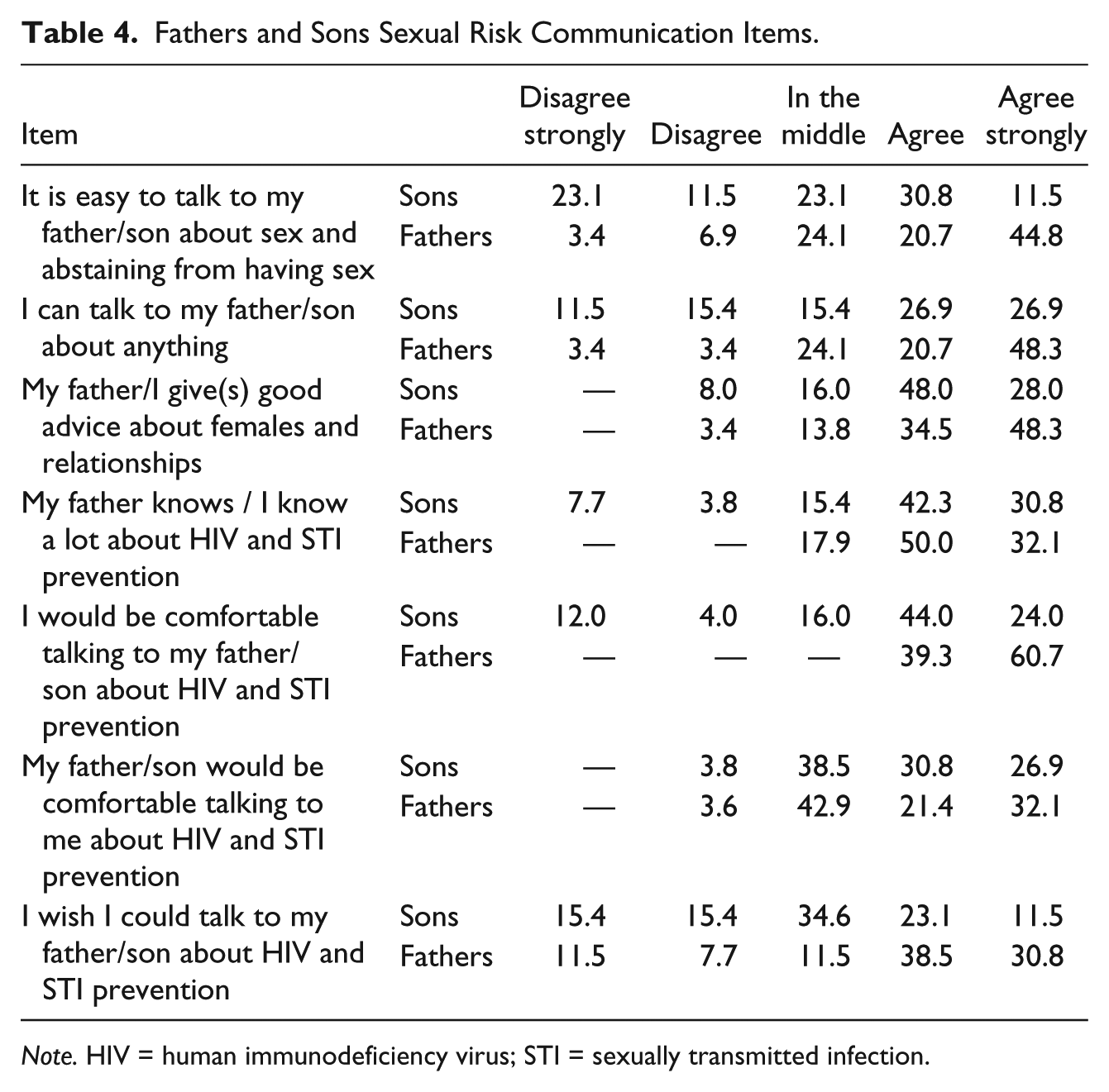
Fathers and Sons Sexual Risk Communication Items.
Note. HIV = human immunodeficiency virus; STI = sexually transmitted infection.
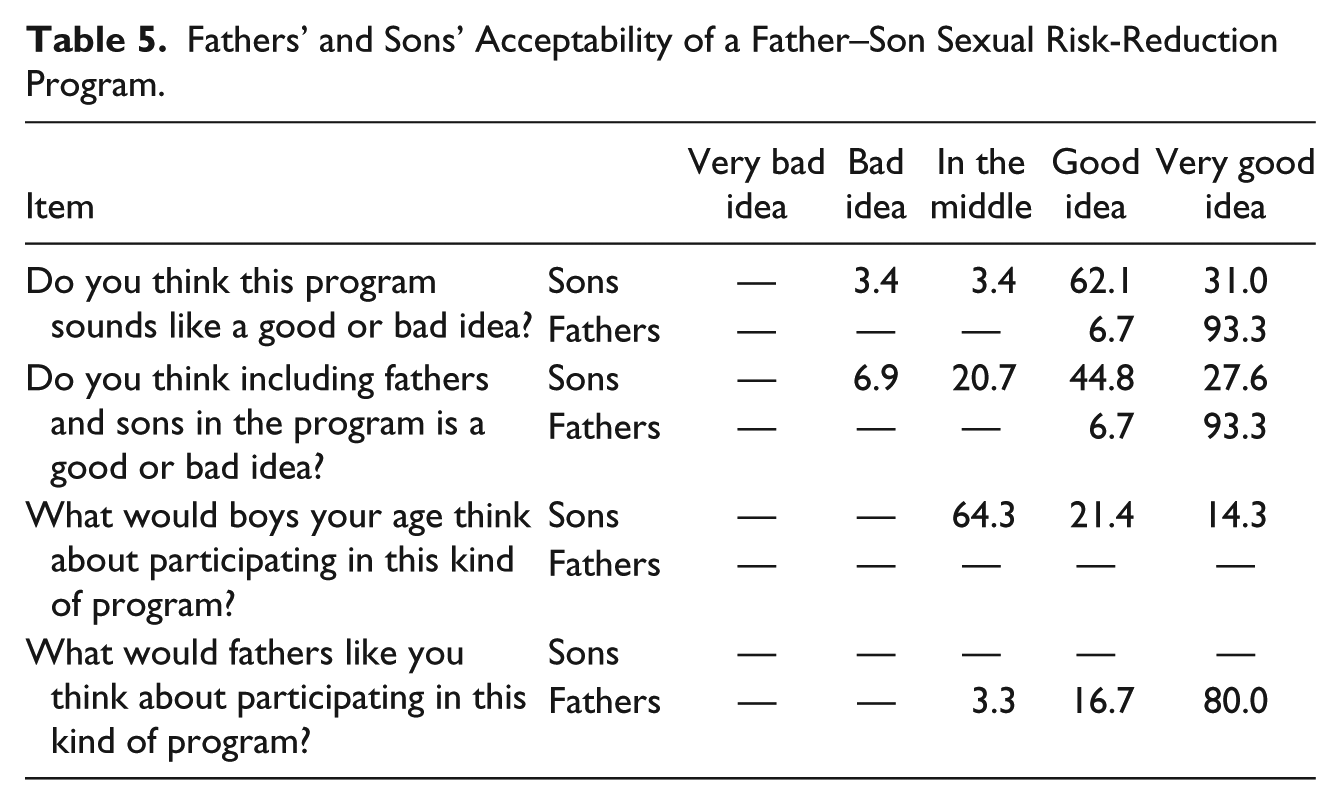
Fathers’ and Sons’ Acceptability of a Father–Son Sexual Risk-Reduction Program.
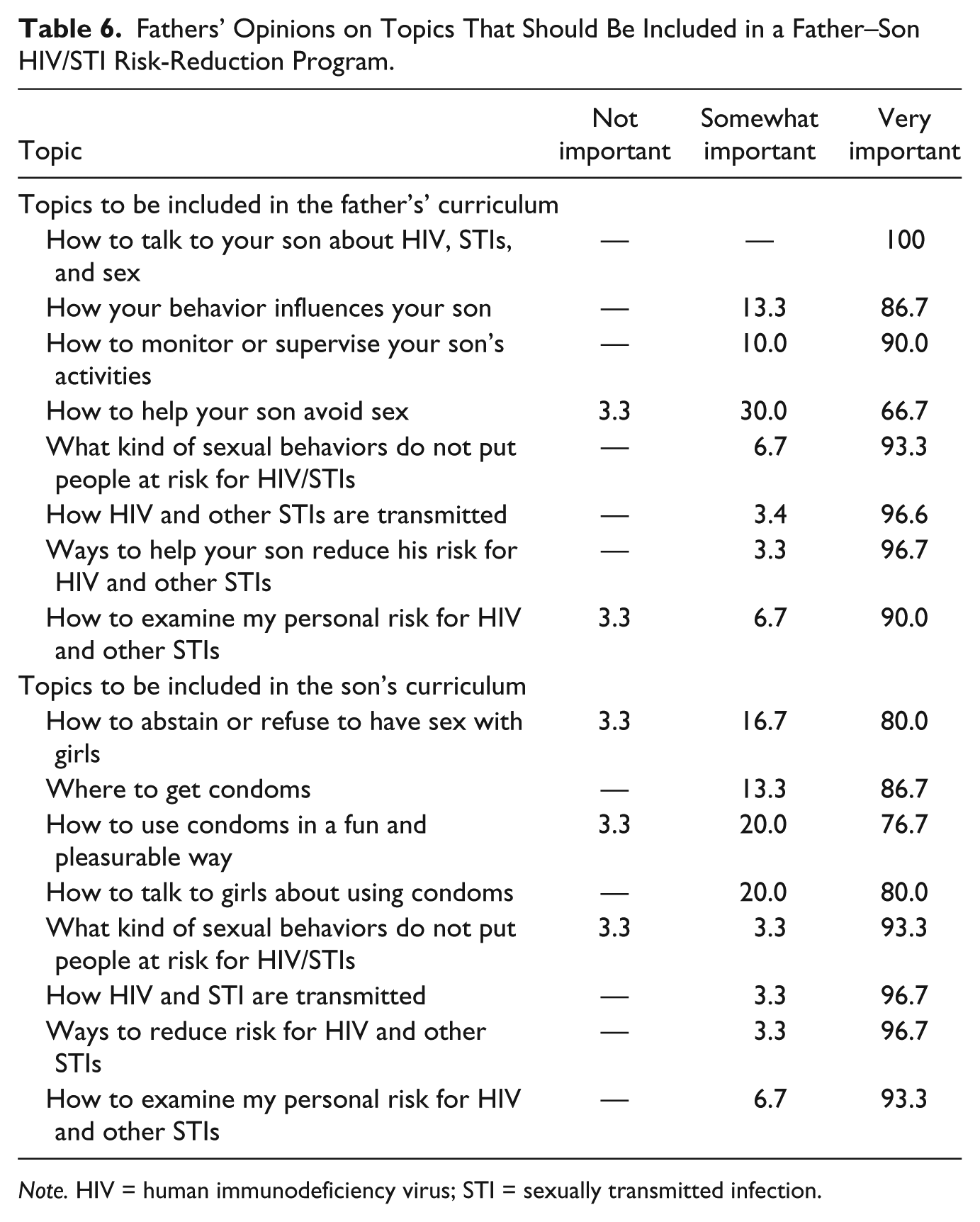
Fathers’ Opinions on Topics That Should Be Included in a Father–Son HIV/STI Risk-Reduction Program.
Note. HIV = human immunodeficiency virus; STI = sexually transmitted infection.
Sons’ Opinions on the Topics That Should Be Included in the Father–Son Sexual Risk-Reduction Program.

Note. HIV = human immunodeficiency virus; STI = sexually transmitted infection.
Procedure
Focus Groups
The Black barbershop has been deemed a culturally salient and effective setting for the delivery of health promotion programs for African American youth and men including HIV risk-reduction programs (Brawner, Baker, Stewart, et al., 2013; Hart et al., 2008; Holt et al., 2010; Linnan, D’Angelo, & Harrington, 2014; Luque, Ross, & Gwede, 2014; Releford, Frencher, Stanley, & Yancey, 2010; Victor et al., 2011; T. E. Wilson et al., 2014). In addition, barbers are highly regarded and trusted community leaders and may be effective behavioral change agents (Brawner, Baker, Stewart, et al., 2013). Based on this research and their teams’ own experience in developing health prevention programs in barbershops (Baker et al., 2012; Brawner, Baker, Stewart, et al., 2013; L. S. Jemmott et al., 2017), the co-investigative team members decided that the focus groups for this study would occur in a barbershop.
All focus groups were conducted at a local barbershop in West Philadelphia; 3 groups with fathers and 3 groups with adolescents. Father and son sessions were conducted simultaneously in the same barbershop but were separated for validity purposes so that fathers and sons would be more open and honest in the focus group sessions. On arrival to the barbershop, research assistants provided the adolescents (n = 30) and the fathers/father figures (n = 30) name tags and consent forms on their arrival to the sessions. Assent and verbal parent/guardian permission were obtained for the adolescents. Fathers provided written consent for their own participation. Two doctoral-level facilitators with expertise in advanced qualitative research methods moderated the focus groups. Prior to the interviews and focus groups, participants completed a self-administered questionnaire. The focus groups each ran for approximately 90 minutes. Four note takers (two per focus group) wrote detailed notes using the focus group scripts about the main ideas that were expressed during the sessions. Focus groups were also audio-recorded. Participants were assured that audio data would be destroyed after receipt of transcriptions. Fathers were compensated with $50.
Data Analysis
Data analysis involved analyzing both qualitative and quantitative data. Several research team meetings were held for concurrent review of all the data sources—audio recordings, transcripts, notes, and survey data. Research team members compared the audio recordings to the transcripts for content accuracy. Transcripts were also compared with notes to get a more complete understanding of the focus group sessions (Thurmond, 2001). Nvivo10 (QSR, 2014) was used to manage the data and for the coding process. A code book/list was generated after reading through each transcript in its entirety. We elected this approach in order to get a comprehensive view of each transcript and in an effort to obtain a complete code list. Once transcripts were coded, we used thematic content analysis to identify within- and across-group themes (Padgett, 2008). Broad themes were identified first then further analysis was done to identify subthemes. Thematic content analysis was conducted first by each focus group question and then across the entire transcript. Qualitative data saturation was reached once the same or common themes emerged across focus groups pertaining to our research questions. To increase reliability, four independent coders used the generated code list. When discrepancies in coding occurred, the research team met with the four coders to decide the final focus group themes within the focus group transcripts only. Survey data were entered in SPSS 22 (IBM Corp, 2013), and descriptive analyses were completed. There were no discrepancies within the analysis of the open-ended questions due to the nature of the line of questioning, thus open-ended responses from questionnaires were simply coded and tallied.
Results
Sample
Data reported below that includes percentages are from the questionnaires. A total of 30 father–son pairs participated in the study. Table 1 presents demographic characteristics for fathers and sons. The majority of fathers were African American (90%) and ranged in age between 25 and 60 years (mean age = 43.7 years). Most fathers had at least a high school diploma or GED. Approximately 83% of fathers were currently employed; 60% had an annual salary of less than or equal to $40,000. Most fathers reported having at least one child (86.7%). Half of fathers indicated being the participating adolescent male’s biological father. The other half of the sample was comprised of adult mentors (26.7%), other relatives (16.7%), and stepfathers (6.7%).
Of the 30 adolescent males, only 28 had available demographic data (2 sons did not complete the demographic portion of the questionnaire). Most of these youth were African American (96.4%) and ranged in age between 10 and 19 years (mean age = 14.7 years). More than half of teens were in high school (57.1%), and 25% were employed. Approximately 64% of sons reported living with both their mother and father. None of the teens reported having any children.
Below we present the broad themes as headings and subthemes are elaborated upon in the body of each section.
Father–Son Sexual Risk Communication
Fathers and sons sexual risk communication beliefs are found in Table 4. Approximately 75% of fathers and 66.7% of sons agreed/strongly agreed that they could talk to each another about anything (69% and 53.8%, respectively). About 73% of sons agreed/strongly agreed that their fathers knew a lot about HIV and STI prevention, whereas 82.1% of fathers agreed/strongly agreed that they knew a lot about HIV prevention. However, there was some discrepancy between fathers and sons with regard to their level of comfort in discussing these topics. For example, 65.5% of fathers agreed/strongly agreed that it would be easy to talk to their son about sex or abstaining from sex whereas less than half of sons (42.3%) agreed or strongly agreed that it would be easy for them to talk to their fathers about this issue. Similarly, all fathers (100%) agreed/strongly agreed being comfortable talking to their sons about preventing HIV and other STIs as compared with 68% of sons feeling comfortable talking to their fathers about these issues. More than half of fathers and sons agreed/strongly agreed that the other would be comfortable talking about preventing HIV and other STIs (53.5% and 57.7%, respectively). In addition, 69.3% of fathers agreed/strongly agreed that they wished that they could talk to their son about preventing HIV and other STIs. In contrast, 34.6% of sons were unsure about talking to their fathers about preventing HIV and other STIs.
“You Know What You Gotta Do”
In the focus groups, the general perception of PCSRC between fathers and sons diverged greatly. Fathers often felt they were engaging their sons in frequent, open conversations. One father stated, “It’s going to be the fathers that’s going to be leading our young men into these conversations.” Sons, on the other hand, felt the conversations with their fathers were brief, and uncomfortable. One father stated, “I talk to my son about sexual intercourse, about HIV, about all this. . . . I always tell him, ‘You know what you got to do,’” and another father stated, “I can’t say [this] for everybody but I’m open with my child, my son. I’m very open with him. We talk about everything.”
What is interesting to note is the apparent difference in perceptions from the fathers’ and sons’ perspectives. From the sons’ perspectives, sexual risk communication messages were either not initiated regarding sex or not clearly received. For example, when one son was asked about the conversations that were had about HIV, STI, and pregnancy prevention, he answered that the conversations were “short and sweet,” and “don’t get a girl pregnant and just check your condom.” This disconnect was possibly due to a degree of discomfort among the fathers in discussing sexual matters. One son indicated this possibility in saying, “My dad never even bought me a box of condoms or anything like that. My stepmother took me to the doctor; my dad is just not there yet.” Fathers and sons revealed that relationship quality had the potential to impede their sexual health conversations. Some of the sons admitted that they did not have a relationship with their fathers. Subsequently, they refused to engage their fathers when they did try to talk to them about sex. One father stated, “My son, as far as my son, he fears me. So he won’t talk about, well, he just started talking about sex to me and he told me why it don’t feel right talking to you, dad.” One son stated, “He’ll [his father] try to say something. He wants me to talk to him about sex. He wants that relationship but I’m not there yet. He tries to say stuff but I don’t add anything.” Despite lack of a close relationship between some fathers and sons, fathers still understood the influential role they played in enhancing sexual risk communication with their sons. A father stated,
One of the things we have to also do as the fathers, we have to make sure that our lines of communication are open with our sons. We have to make sure that our children, our boys feel comfortable bringing this to us because if they don’t feel comfortable we’re never going to know about it.
Program Interest: Father–Son HIV/STI Intervention
Fathers and sons reported favorable attitudes toward a father–son sexual risk-reduction intervention program (see Table 3). The majority of fathers and sons indicated that a sexual risk-reduction program for fathers and sons was a good/very good idea (100% and 93.1%, respectively). Additionally, all fathers and 72.4% of sons indicated that it was a good/very good idea to include both fathers and sons in the program. Nearly all fathers (96.7%) thought that other fathers would think that participating in this program was a good/very good idea. However, only 35.7% of sons thought their peers would want to participate in this kind of program.
“It May Help Start a Conversation”
In the focus groups, fathers and sons revealed that engaging in a sexual risk communication program aimed toward them would provide an opportunity to bond and enhance communication overall. One son said that he would want to participate in the program, “So I’d get to know things about my Dad. So he wouldn’t keep nothing away from me. We’d get to know each other.” Fathers’ hypothesized that their sons would “probably feel like the program would open them up,” and that it would be “good. It may help start a conversation.” One father indicated both a facilitator and barrier to a sexual risk reduction program in saying “I think the number one thing is engagement and reengagement with our kids.” While the opportunity to engage was an added benefit of the proposed program, the need to reengage their sons revealed a salient barrier. When asked about whether a son would want to participate in this program with his father, he said, “not necessarily. I would feel better not being with my Dad. I don’t want to talk to my Dad about those things [sex].” Fathers were invested in the possibility of a program that would help them communicate with their sons about sex while simultaneously providing an opportunity to enhance their existing relationships. One father shared,
You cannot delegate that to any other person, particularly if they’re not a man. Because there are certain things that men know, we walk in our shoes that no one else can speak to in addressing our sons. So first of all, and that’s in terms of, we have to set the example.
Program Content and Design of a Father/Son HIV/STI Intervention
Fathers
Fathers provided information regarding the content and design of the sexual risk-reduction program. With regard to the information that should be provided specifically for father, all men indicated that it was very important to include information on how to talk to your son about HIV, STIs, and sex. The majority of fathers also reported that it was very important to include information on how their behavior influences your son (86.7%), how to monitor or supervise your son’s activities (90%), how HIV and other STIs are transmitted (96.6%), the types of sexual behavior that do not put people at risk for HIV/STIs (93.3%), ways to help sons reduce their risk for HIV and other STIs (96.7%), and how to assess their own personal risk for HIV and other STIs (90%; see Table 4). Furthermore, 67% of fathers reported that it was very important that the program include information on helping sons avoid sex. Fathers also reported on the content that should be included specifically for sons. More than 90% of fathers reported that it was very important that the program include information on what kind of sexual behaviors do not put people at risk for HIV/STIs (93.3%), how HIV and STIs are transmitted (96.7%), ways to reduce risk for HIV and other STIs (96.7%), and what types of sexual behavior do not put people at risk for HIV/STIs (93.3%). Most fathers also indicated that it was very important to include information on how to abstain or refuse to have sex with girls (80%), where to get condoms (86.7%), how to use condoms in a fun and pleasurable way (76.7%), and how to talk to girls about using condoms (80%).
In the focus groups, fathers offered a wealth of suggestions for developing an engaging and comprehensive program. Fathers agreed that an intervention should be a joint program that they attend with their sons. For example, it was suggested that fathers share their sexual risk behaviors with their sons during the intervention. One father stated, “I would let my son know I got something because I didn’t use a condom in the past.” The fathers felt being honest about their behaviors would “make the messages real” and make them [the fathers] more relatable to their sons. Fathers also suggested using barbers and other African American men to serve as trainers to help them deliver the program content. One father stated, “I think one of the key elements in the program is first of all, we as men have the big responsibility of teaching our sons, our sons and the young boys in our lives how to be men.” All of the fathers agreed that they would need to be trained before being a part of the intervention in order to provide accurate health information to their sons. Additionally, they emphasized the importance of having a script to keep them on track during the program and that it shouldn’t include a lot of technical jargon.
With regard to program design, the fathers also agreed that follow-up sessions with program facilitators (e.g., themselves or barbers) should be designed for the sons in order for intervention messages to be reinforced. A father stated, “You can give us all information about HIV and STDs and all that different stuff but our delivery and how we deal with our sons is going to be very different.” Fathers expressed that the barbershop was an ideal location for a father–son intervention program. They believed the environment would be organic and comfortable for both the fathers and the sons participating in the intervention.
Sons
Sons also provided feedback on the content that should be included in the sexual risk-reduction program. Topics that the majority of sample reported as being very important for young males included: how to use condoms correctly (71.4%), where to get condoms (71.4%), what types of sexual behaviors do not put people at risk for HIV/STIs (81.5%), how HIV and STIs are transmitted (71.4%), ways to reduce risk for HIV and other STIs (85.7%), and how to assess personal risk for HIV and other STIs (71.4%). In contrast, less than half of sons reported that it was very important to include specific information on how to use condoms in a fun and pleasurable way and how to talk to girls about using condoms (39.3% and 42.9%, respectively).
In the focus groups, adolescents provided some very creative ideas for program content and delivery. In the focus groups, sons suggested that the program should be offered in the summer. Topics recommend to be included in the program were the following: (1) communication strategies with their fathers; (2) talking with fathers about future goals, such as college majors, long-, and short-term goals; (3) drugs; (4) sports; (5) school issues; (6) peer conflict; (7) violence; and (8) being a leader. Some of the sons stated that abstinence should not be an included topic for several reasons, including “a possible reason for fathers to not be proud of their sons,” “not being accepted by your friends,” and “girls frowning on boys for not being a man.” Sons who were abstinent expressed that their fathers may be ashamed about them not being sexually active yet. Another suggestion was that fathers and sons meet for 10 minutes at the end of each intervention session for a recap of what they learned.
Social Media Use in a Father/Son HIV/STI Intervention
“I’m on Twitter. I’m Usually on There and Instagram”
Both fathers and sons indicated that technology and media platforms were crucial to include as part of an intervention program. With regard to program design and materials, the adolescents suggested that technology including iPads be used so that adolescents could view pictures of STIs and retain program information. They also shared that the program should have an app and use a Twitter account to tweet HIV facts and statistics.
One father stated, “I’d say [you need] a virtual website where you can communicate like Facebook. . . . Because that’s the only way kids open up. More than face-to-face these days.” A son reaffirmed this statement saying, “I think you could have an app and people could get on there and have classes on diseases . . . they could hear it and promote it.” In addition, the sons also indicated the need to incorporate messages within the context of sports and popular activities as well as addressing what they felt were related concerns: education, violence, and drugs. One son stated, “Yeah, I would want it to be about sex, but more than that I want it to be about sports teams and boxing. Stuff that we would like to do.”
Discussion
Literature has strongly demonstrated that PCSRC among African American fathers and sons can positively influence sexual behaviors among adolescent African American males (Caldwell et al., 2004; Caldwell et al., 2014; Dilorio et al., 2007; Guilamo-Ramos et al., 2012; Harris et al., 2013; Hutchinson & Montgomery, 2007). In this study, father engagement was high, as all of the fathers wanted to be involved in their sons’ lives, help them make sound decisions, and to talk to them about serious topics, such as sex, HIV, STIs, and pregnancy. Similar to results found from other intervention studies with African American fathers and their children, we found that the quality of relationships between fathers and sons is significant for effective sexual risk communication (Caldwell et al., 2004; Caldwell, Rafferty, Reischl, De Loney, & Brooks, 2010; Cornelius, Cornelius, & White, 2013; Hutchinson & Cederbaum, 2011). Results highlighted that father–son intervention programs can serve as an opportunity to build open communication and stronger father–son relationships for (1) adolescents that have an existing positive relationship with their father and (2) for adolescents interested in improving their relationship with their father.
Results in this study demonstrated that fathers and sons were not in agreement about the frequency of communication and the breadth of sexual health topics discussed. Most of these fathers believed that they were providing consistent messages about HIV and safer sexual practices to their sons. Challenges in sexual communication received by sons were hindered by perceived discomfort of fathers facilitating sexual behavior discussions. Additionally, the sons’ focus groups revealed the promotion of abstinence was a concern for peer and father participation due to perceived culturally adapted masculine expectations. Focus group data supports that a structured HIV/STI intervention incorporated with tailored activities has the potential to (1) increase HIV/STI knowledge, (2) enhance PCSRC, and (3) provide sexual risk reduction skills to the sons. Sons expressed this in focus groups by not only naming HIV/STIs as topics for the intervention but other topics unrelated to sexual risk which could potentially serve as content for a control intervention condition in a randomized controlled trial. Furthermore, we found that social media platforms can also significantly support the need of both fathers and sons to have a variety of communication means to facilitate sexual risk discussions.
One major finding that highlights the distinctiveness of African American fathers and sons was a suggestion that a HIV/STI risk reduction program could help them cope together with emotional issues, violence prevention, and possibly repair strained father/son relationships. Many fathers reported that they are aware of the emotional health needs of their sons, such as anger and mental health issues, but are not sure how to facilitate a conversation to help their sons. On the other side, many sons expressed that they want to learn information to lead healthier lives, but they experience internal conflict if the messages are coming from a father/father figure that they do not have a close relationship with. Some of the sons in the study acknowledged that the state of their emotional relationship with their father could help or hinder their ability to hear any sexual health messages as well as other life messages. Both fathers and sons expressed that peer conflict and avoiding violence are concerns that a potential intervention program could address. Thus, a father–son intervention could prove to be valuable in providing education to support fathers in not only discussions about sex but also other health challenges faced by young, African American male adolescents (e.g., mental health, conflict/violence prevention).
Study Limitations and Strengths
There were definite limitations to this study. The study consisted of a small convenience sample (N = 60). Thus, the results are not generalizable to all African American fathers/father figures and adolescents. In addition, not separating the adolescent groups into smaller age ranges (e.g., 10-13 and 14-17 years) made focus group facilitation more complex. It is also possible that the older adolescents in the focus groups influenced the responses of the younger participants. This could also be the case with some of the focus groups with the fathers/father figures. Some of the fathers’ responses could have been influenced by some of the more outspoken fathers. In addition, self-reported data from the surveys could have influenced response bias and limited recall. Even though the study provided help for those with literacy issues, some men struggled with completing the survey and might have rushed or answered questions inaccurately to finish in a timely manner similar to other men in the study. However, using both questionnaires and focus groups was a particular strength of this study as it provided participants two chances to provide data on the topics discussed. In focus groups, all of the participants will not feel comfortable sharing information. Thus, some participants may have been more comfortable with answering questions from the surveys. The study results do support the development of a HIV/STI risk reduction program for African American father–son dyads depending on how the program is designed and the quality of the father–son relationship. Also, fathers and adolescents would both be willing to participate and recruit other participants.
Research Implications
Previous studies have demonstrated that fathers can be effectively involved in intervention research programs (Caldwell, Rafferty et al., 2010; Caldwell et al., 2011; Dilorio et al., 2007). This study highlights the need to further study the best way for fathers to communicate with their sons about sexual health issues. In particular, further studies could be conducted looking at a father’s ability to communicate with his son through various stages of the life cycle (ages 7-9, 10-13, 14-17, 18+ years). Further research could be conducted looking at possible differences in a father’s ability to communicate about sexual health issues based on a father’s education and income. In this study, we found that fathers and sons described the quality and quantity of their communication in divergent ways. Further research could examine and develop communication strategies for fathers and tools for sons to discuss sexual health issues and other important topics. Last, additional research examining if there are any differences of how fathers of different racial/ethnic backgrounds communicate about sexual health issues with their sons.
Conclusion
The results from this study also highlight the need for future research as well as the need for HIV/STI prevention programs geared to promote PCSRC practices among African American fathers and their children. In particular, African American fathers want to communicate with their sons about HIV/STIs but disconnects in fathers’ perceptions of messages delivered to their sons and the sons’ reality of what messages have been received; have the potential to serve as barriers to effective PCSRC. If PCSRC practices are not enhanced between fathers and sons, there’s a possibility that rates of HIV and STIs among adolescent African American males could remain the same or even increase. Father–son programs should focus on designing and testing a HIV/STI risk-reduction intervention that includes biological fathers and adult men that serve as father figures to young, African American males. A father/son HIV/STI risk reduction program could enhance the quality of the father–son relationship by helping African American fathers and sons to establish new levels of openness, honesty, and connection beyond what they are experiencing currently while simultaneously providing skills to their sons that would reduce their risk for HIV and STIs.
Footnotes
Acknowledgements
We would also like to acknowledge Mr. Darryl Thomas, the owner of Philly Cuts barbershop, and all of the barbers for supporting this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute of Child Health and Human Development grant (R01HD061061) awarded to Dr. Loretta Sweet Jemmott, the National Institute of Child Health and Human Development Diversity Research Supplement Award (5R01HD061061-03; PI: Jemmott) to Dr. Jillian Lucas Baker, and National Institute of Nursing Research Ruth L. Kirschstein NRSA Postdoctoral Fellowship (T32NR007100; PI: Sommers) to Dr. Yzette Lanier.