
Abstract
This article explores the motivations for unregulated child care use within Canada. Using focus group data from 109 mothers, we analyze unregulated child care use within a policy context in which regulated child care is only available for 20% of preschool children. The key drivers for unregulated care were framed by participants as benefits: trust in a known caregiver with similar values, offered in a home-like environment. Importantly, one driver that was not seen as beneficial was the lack of affordable and accessible, regulated child care. Sometimes used as a last resort amid regulated child care shortages, unregulated care became the driver of how mothers organized their time. Within the constraints of a limited regulatory child care environment, we argue that Mathieu’s (2016) concept of demotherization is beyond the grasp of the majority of Canadian mothers.
Introduction
A striking trend, known as the child care transition, has been observed in Organisation for Economic Co-operation and Development (OECD) countries in recent years: the majority of preschool children now spend a significant amount of time in nonparental child care. United Nations International Children’s Emergency Fund (UNICEF, 2008) flagged this trend as a critical policy issue, declaring that the extent to which the child care transition presents “an advance or a setback—both for today’s children and tomorrow’s world—will depend on the wisdom of the [policy] response” (p. 7). Within the international context, Canada, among OECD countries, is an interesting case study. Canada has a high rate of maternal employment: over 70% of mothers with preschool children are employed (Ferns & Friendly, 2014). However, mothers’ labor force participation is not matched by a corresponding level of regulated child care spaces. In 2014, there was a regulated child care space for just over one in five children aged 0 to 5 years in the majority of Canadian provinces (Friendly et al., 2018). Within this context, nearly two thirds of employed parents with preschool children in Canada are dependent on unregulated child care (Beaujot, Du, & Ravanera, 2013). Despite the prevalence of unregulated care, there is little known about the drivers of unregulated care use for families of preschool children. Several scholars have identified that a lack of research on unregulated child care constitutes a substantial gap in the academic literature (Bryson, Purdon, Brewer, Sibieta, & Butt, 2012; Ferns & Friendly, 2015; Pasolli, 2015).
The system of child care in Canada has been described as a “laggard” on the international scene (Jenson, 2004), and is characterized as a piecemeal, “patchwork” of services offered primarily through the nonprofit and for-profit private sector (Mahon, Anttonen, Bergqvist, Brennan, & Hobson, 2012). In UNICEF’s (2008) analysis of early childhood education and care, Canada met only 1 of 10 benchmarks that assessed child care quality, access, and financing. Outside of Quebec, the only province in Canada with a universal child care system, there is minimal public expenditure on child care, only 0.25% of the GDP (Friendly & Prentice, 2009). This is a low rate of investment in the early years by comparison with other high-income countries (Thevenon, 2011). Of the funding that is provided for child care, the vast majority has been invested in the demand-side through offering parental subsidies, particularly to low-income families, while limited funding has gone into the supply-side of providing child care (Mahon, 2005). Consequently, over 80% of the operating costs associated with child care are covered by parent-paid fees (Friendly et al., 2018; Friendly & Prentice, 2009). In Alberta, child care subsidies are available for low-to-middle income families (Government of Alberta, 2017b).
Unregulated home-based group care is legal throughout Canada, provided it does not exceed the provincially determined maximum number of children; however, “there are no health, safety or training requirements or provision for public oversight in unregulated care; [and] any attention by local or provincial public officials is on a complaint basis” (Childcare Resource and Research Unit, 2013). In the Province of Alberta, home-based group child care, called family day homes, can be regulated or unregulated; while the legal status of a particular day home is determined by the province, parents may not always know or distinguish between these types. Alberta’s Child Care Licensing Act allows family day homes to “provide child care to a maximum of six children aged 0 to 12 years old in the private residences of the providers” (Government of Alberta, 2013). Agencies exist within the province to recruit, monitor, and support family day home providers (Government of Alberta, 2017a). The Province of Alberta also provides kin care payments for low- and middle-income families of preschool and school-aged children, enabling families to pay their relatives to care for their kids (Government of Alberta, 2017b).
Within the context of regulated child care shortages, the key aim of this article is to explore the experiences and motivations of unregulated care use in the Western Canadian Province of Alberta. We consider the extent to which this child care environment contributes to demotherization, as explained below.
Theoretical Framework
In this article, we use Mathieu’s (2016) concept of demotherization to consider the extent to which unregulated child care provides mothers with meaningful options to share 24/7 social reproductive work with other carers. Mathieu (2016) defines demotherization as “the extent to which mothers can offload caregiving responsibilities onto other family members, the state, or the market” (p. 585), thereby providing them with opportunities for labor force attachment. How care is provided, and who takes responsibility for it (i.e., state, market, or family), will influence the extent to which demotherization occurs.
Mathieu offers a typology of four types of maternalism, exploring the public policies that encourage these kinds of maternalisms. Traditional maternalism is based on the assumption that mothers are both able and willing to care for their children and offers little-to-no policies to support the combination of earning and caring. Implicit maternalism occurs when mothers are offered money to care for children; maternity leave is one such example. In this type, mothers’ care of children is recognized and provision is made for it. State-funded dematernalism removes the caring responsibilities from the family by offering state-funded child care services or policies that demotherize responsibility of care. “Daddy quotas” for paternity leave would thus also be part of state-funded maternalism. The distinguishing factor in this kind of maternalism is that the state actively provides policy frameworks to take the burden of care off mothers. Familialized dematernalism is a type of dematernalism in which the family, rather than the state, holds primary responsibility in providing child care. It differs from traditional maternalism in that the care work is shared by fathers, grandparents, or possibly nannies, for those families who can afford it. Using Mathieu’s typology, our analysis was attentive to the ways in which the child care policy context in Alberta provided opportunities and constraints for mothers’ choices in child care, and the nexus between earning and caring.
Literature Review
Defining Unregulated Child Care
The literature on unregulated care does not provide a precise definition of unregulated care, and features a variety of terms and conceptualizations. Wheelock and Jones (2002, p. 444) note the lack of a standard definition and prefer to use the term “complementary care.” Other researchers delineate informal and formal care without consistent reference to the level of regulation provided for the care types within these categories (Brady & Perales, 2016; Bryson et al., 2012; Qu & Wise, 2004). Following this delineation, researchers agree that informal care includes care offered by grandparents, other relatives, friends, and neighbors. Bryson et al. (2012, p. 14) and Qu and Wise (2004) argue that nanny care is informal care. However, like Brady and Perales (2016, p. 340), and consistent with Loeb’s (2016) concept of “lightly regulated” child care, we consider nanny care formal because it is (weakly) regulated and is paid for by parents. For employment purposes, the Government of Alberta (2016) considers nannies domestic employees; while employment standards specify a minimum wage and employee entitlements, there are no standards, oversight, or monitoring specific to the provision of child care. Home-based group care, called day homes in Alberta, is categorized as either regulated or unregulated, depending on its licensing status (Friendly et al., 2018).
In light of a lack of standardization of unregulated care in the literature, we define unregulated care as any nonparental child care arrangement that occurs without government oversight, licensing, standards, and monitoring with respect to the care setting, the care/group size, and the qualifications and qualities of the caregivers. Unregulated care may be formal (such as care provided in an unregulated day home or by a privately employed nanny) or informal (such as care provided by grandparents, other relatives, or friends). Although it may seem nonsensical to classify unregulated day homes as formal, we suggest that these types of care settings are sufficiently different than informal care to warrant classification as formal. Because day homes entail searching, procuring, and paying a child care provider who is not typically a relative or friend, it is a formal arrangement, whether regulated or not. Unregulated care may be provided for payment (e.g., care offered by a regular babysitter for wages), under a reciprocal arrangement (e.g., care by a friend offered on the basis of a “trade” or in-kind payment), or for free (e.g., grandparent care offered free of charge).
Unregulated Care Use
Analysis of the 2006 Canadian General Social Survey shows that, with the exception of Quebec, the nonparental care of Canadian children aged 0 to 4 years is divided between regulated child care (37.5% includes center-based care and care in licensed day homes), nonrelative care (36% unregulated), and care by relatives (26.5% unregulated; Beaujot et al., 2013). Taken together, the majority of children in nonparental child care are in unregulated care (62.5%). For the Prairie provinces—of which Alberta is one—Statistics Canada (Sinha, 2014) data indicate the use of child care arrangements as 31% home daycare, 23% daycare center, and 43% private care (the highest rate of private care among all Canadian provinces).
Studies in other national contexts show the prevalence of unregulated child care in various Western countries. In the United States, National Center for Education Statistics data indicate that more than half of the 0- to 2-year-olds are in unregulated child care settings (Loeb, 2016). In Australia, Brady and Perales (2016) report that 25% of employed families with children aged 0 to 6 years use only unregulated care. In short, unregulated care use in Canada and some other English-speaking nations is substantial and merits scholarly attention.
Motivations for Unregulated Child Care Use
The current literature highlights two key motivations for unregulated care use: caregiver trustworthiness and flexibility (Bryson et al., 2012; Morrissey, 2008, 2009; Skinner, 2003, 2005; Wheelock & Jones, 2002). Unregulated care provided by kin is trusted because it is generally performed by family or close friends who hold similar values, and is generally provided in home environments (Brady & Perales, 2016; Bryson et al., 2012; LeBihan & Martin, 2004; Reschke & Walker, 2005; Stoll, Alexander, & Nicpon, 2015). Importantly, grandmother care is the most prevalent form of unregulated care. Zamarro’s (2011) examination of child care in Europe, using data from the Survey of Health, Aging and Retirement, showed that grandmothers, specifically, were the primary caregivers for European children. In 2002, Wheelock and Jones found that grandparents provided regular care for 52% of their U.K. sample. In the United States, Posadas and Vidal-Fernández (2012) report that grandparents provide child care for 20% of preschool children with employed mothers. Wheelock and Jones’s (2002) study concludes that, in the absence of parental care, “grandparents are the next best thing” (p. 454).
Flexibility is also seen as a key advantage of unregulated care because unregulated caregivers often have the capacity to offer care outside of standard working hours (Brady & Perales, 2016; LeBihan & Martin, 2004; Loeb, 2016; Reschke & Walker, 2005; Wheelock & Jones, 2002). Grandparent care is particularly favored, because in addition to being trustworthy, it can be used to support parents’ nonstandard hours of work, unpredictable schedules, and times of child illness (Reschke & Walker, 2005).
In addition to unregulated care, research in the United States and Australian contexts shows that some parents use multiple care arrangements to meet their child care needs (Brady & Perales, 2016; Folk & Yi, 1994; Morrissey, 2008; Neilsen-Hewett, Sweller, Taylor, Harrison, & Bowes, 2014). Multiple care arrangements, or child care packages, often use combinations of regulated and unregulated care for practical benefit, where unregulated care can fill in the care needs where unregulated care is unavailable, or to manage logistics such as transport. Bryson et al. (2012), reporting on unregulated child care in the U.K. context, note that “most packages combine group-based formal child care with grandparental care” (p. 6). In addition, parents also package regulated and unregulated care to balance the “home-like environment” of unregulated care with the enrichment and socialization benefits of regulated care. Importantly, concerns about multiple care arrangements have been identified, including unstable care arrangements, and health or behavior risks in children (Chen, 2013; Morrissey, 2013; Pilarz & Hill, 2014).
Bryson et al. (2012) point out that families who use unregulated care “are not a homogeneous group” (p. 5) and that there is no single model of use. Both as a single care arrangement and as a critical component in establishing multiple care arrangements, families often rely on unregulated child care. Informal, unregulated care types, based on social networks, are used to increase the hours of nonparental care; “glue” together complex jigsaws of care; offer safety nets in times of crisis; and play a connecting role during employment transitions (Skinner, 2003, 2005; Stoll et al., 2015).
In sum, there are documented gaps in our understanding of unregulated care (Bryson et al., 2012; Ferns & Friendly, 2015; Pasolli, 2015). Researchers attribute these gaps to a scholarly focus on regulated, formal child care (Brady & Perales, 2016); the problematic nature of understanding how parents “choose” child care arrangements (Bryson et al., 2012); and the “intrinsically private nature” of unregulated child care (Ferns & Friendly, 2015). In the Canadian context, Perlman, White, Friendly, and Ferns (2014) expound a basic research agenda for unregulated care, including a call for more research into parents’ perspectives on unregulated child care. In the present study, we explore unregulated child care in the Province of Alberta, describing parents’ experiences and demonstrating how these experiences are shaped by policy contexts that entail both opportunity and constraints. Using a gender lens, our study prioritizes the perspectives of mothers, fulfilling calls for a shift in research and analysis “from families to mothers when examining the effect of social policies on the gendered division of social reproductive work” (Mathieu, 2016, p. 585).
Methodology
The analysis for this study is situated within a larger research program on child care policy (Breitkreuz, Collins, Cook, Gokiert, Sakaluk, & Hurava, 2013). The key aim of the broader study was to explore the child care experiences of families with preschool children in Alberta within a context in which fewer than 20% of children in the province younger than 5 years had access to a regulated child care space (Childcare Resource and Research Unit, 2013). Between 2012 and 2017, we conducted 15 focus groups in six urban and rural locations across the Province of Alberta. Participants were eligible if they currently had a preschool child, were using or seeking nonparental child care, and were employed or had been employed within the past 6 months. Importantly, we did not specify any particular kind of child care use: rather, we recruited parents who were seeking or using any child care. In the focus groups, we used a basic interview guide to ask questions about what and how child care arrangements were made, the reasons why particular types of child care were used, and parental strategies to integrate paid work and child care. We talked to parents using all kinds of child care: center-based care, day homes, grandparents, nannies, babysitters, friends, neighbors, et cetera, to attempt to capture the full range of experiences with child care as it was used in day-to-day life. As we collected the data and conducted the first phase of open coding of the data from the focus groups, we noticed high usage rates of multiple forms of unregulated child care. Further coding and deeper analysis led to the identification of a key topic, drivers of unregulated care, and this subject served as the basis for this article.
Data Collection
We used focus group methods as they are an effective way to gather a significant amount of data on a particular issue for which not much is known, providing the opportunity to identify key themes on the phenomenon of interest (Morgan, 1997). Benefits of focus groups include their success in creating an environment that encourages participant contribution (Frey & Fontana, 1991) and in capturing “the multivocality of participants’ attitudes, experiences, and beliefs” (Madriz, 2000, p. 836). Focus groups were approximately 90 minutes long, with an average of six to eight participants per focus group. Focus groups were facilitated by experienced facilitators—the authors and/or a trained PhD student. Focus groups were audio recorded with participant consent, and transcribed verbatim by professional transcriptionists.
Data Analysis
We used interpretive description (Thorne, 2008) to analyze and interpret the focus group data. Interpretive description is a pragmatic qualitative methodology that is useful for advancing disciplinary knowledge and providing knowledge with practice implications. Like other qualitative approaches, interpretive description starts with a thick description of the data. It moves beyond this description, however, to answer the “so what” of the data as well (Thorne, 2008). In this study, we wanted to get an in-depth understanding of the participant experiences with unregulated care to understand the extent to which unregulated care facilitated demotherization for women.
To analyze the data, we carefully and systematically reviewed transcripts, consulting the detailed field notes prepared following each focus group. Transcripts were reviewed, coded, recoded, and organized (Morse, Barret, Mayan, Olson & Spiers, 2002) using the NVivo 11 qualitative research software to identify key concepts. Based on the literature, we developed a working matrix of care types and their level of formality and regulation (see Table 1); this matrix guided the coding process to identify unregulated care types and participant contributions and discussion related to them. Second, we analyzed the data thematically using the constant–comparative method (Strauss & Corbin, 1998), breaking down the data into discrete units as organized by the original codes, and organizing them into categories. We grouped data into a number of broad themes, including the motivations for using unregulated care. Based on multiple iterations and the comparisons between categories, we developed subthemes to capture parents’ experiences of and motivations for unregulated child care usage (Braun & Clark, 2006). Using these subthemes, we compiled descriptive summaries and representative direct quotations for each subtheme.
Child Care Types: Classification and Use (N = 109).

More than one type of child care was used by many parents and all of the specific types identified on the demographic questionnaires were included in this table.
Participant Demographics
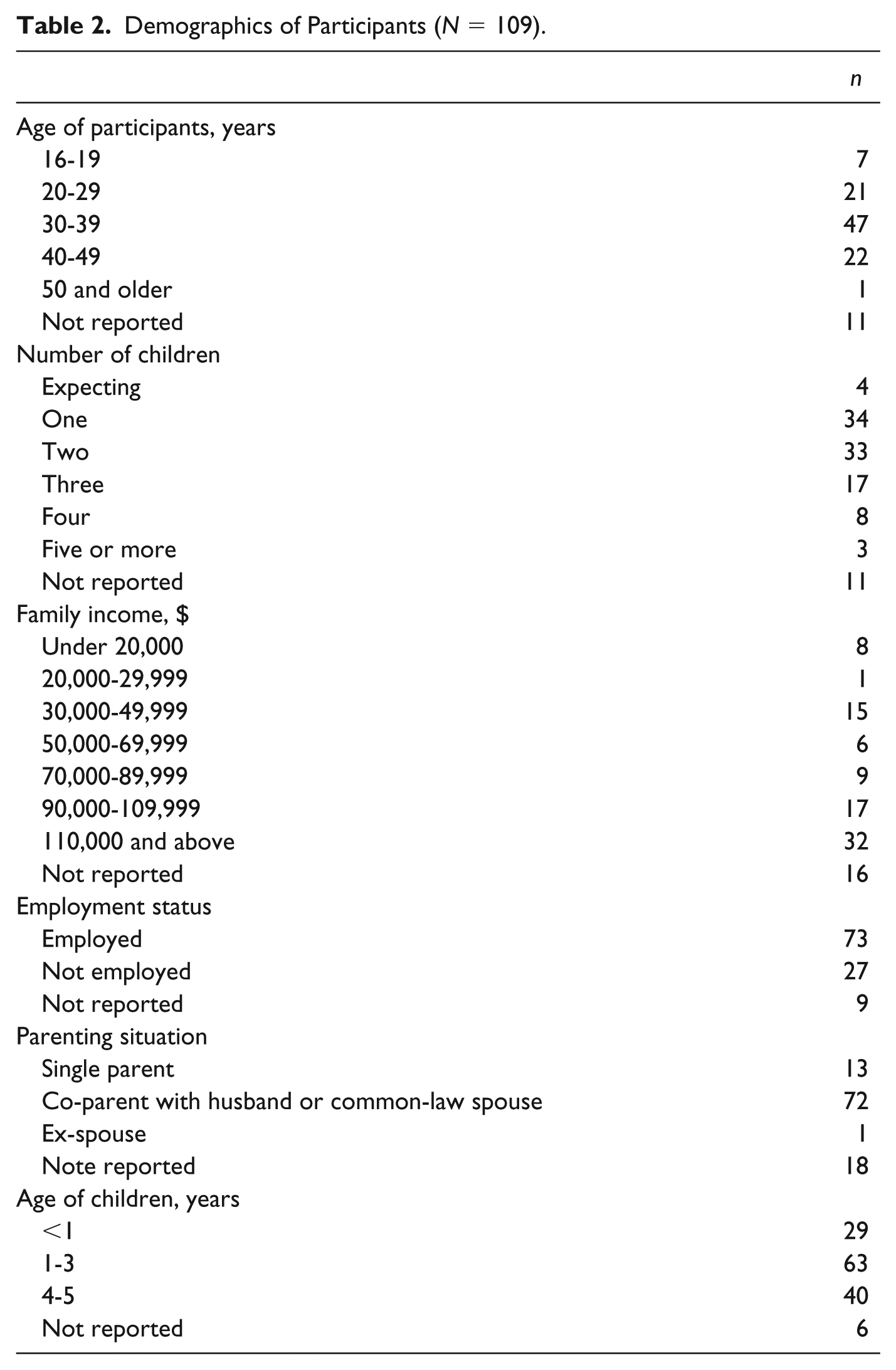
Our study included 109 mothers. 1 Approximately 30% of participants reported family incomes greater than the median income in Alberta, which was $100,750 in 2014 (Statistics Canada, 2016). Two thirds of the participants were employed. The majority (61%) of participants had one or two children, and all participants had at least one preschool-aged child. Detailed demographic characteristics of the study participants are presented in Table 2.
Demographics of Participants (N = 109).
Findings
Table 1 presents the specific types of child care used by participants in our study, indicating the level of formality and the level of regulation for each type. For the purposes of this article, we have adopted Brady and Perales’s (2016) categorization, as detailed in the literature review, to represent the formality of each arrangement.
The findings demonstrate that mothers in our study used a wide variety of child care options. Of the 99 participants who voluntarily completed the demographic questionnaire, 2 the most common type of child care was grandparent care (used by 38% of participants), followed by parent-turn-taking (32%), daycare (22%), and friend and neighbor care (21%). With the exception of daycare, these care types are informal and unregulated, lacking the public oversight, standards, supervision, and support of regulated care (Ferns & Friendly, 2015). Day homes were used by 19% of participants; however, as part of this study, we were unable to confirm whether day homes used by participants were regulated or unregulated. For the purposes of thematic analysis, and in the presentation of results below, we have only included focus group data on day homes where participants explicitly mentioned that the day home their family used was unregulated (sometimes described as “private” or “unregistered”).
Grandparent Plus
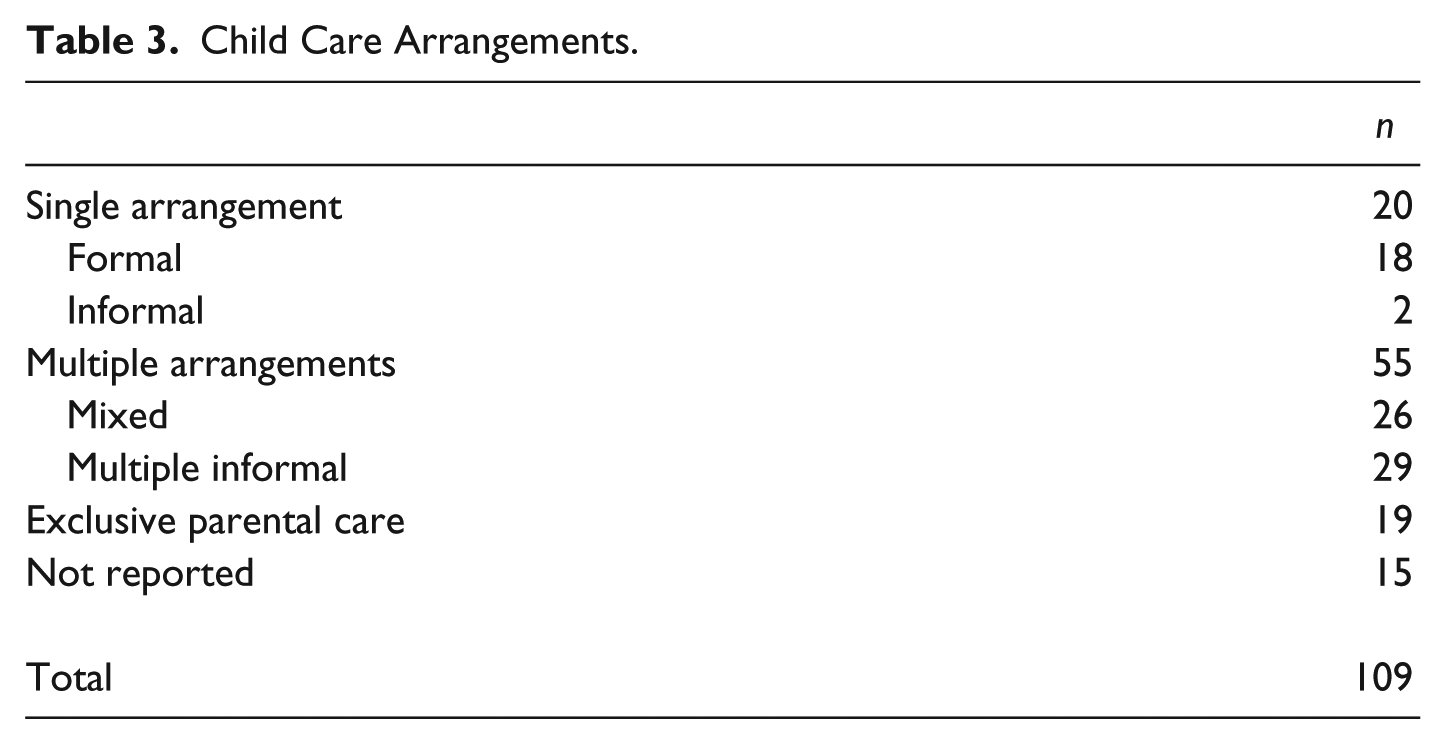
Consistent with existing research, participants who used informal, unregulated care tended to use multiple care types (Brady & Perales, 2016; Folk & Yi, 1994; Morrissey, 2008; Neilsen-Hewett et al., 2014). Table 3 presents the breakdown of child care arrangements according to single arrangement, multiple arrangements, and exclusive parental care. Notably, the majority of parents who used nonparental care used multiple arrangements (55 of 90). Brady and Perales (2016) refer to these arrangements as child care packages; they discuss child care packages as formal only, informal only, and mixed. Importantly, mixed child care as defined by Brady and Perales entails formal plus informal child care. In our study, the ways that child care was used did not break down that cleanly: rather, a range of combinations were used, including multiple forms of informal child care. Most commonly, participants described care packages that we conceptualize as “grandparent plus”: grandparent care plus friend care, grandparent care plus other extended family care, and grandparent care plus parent-turn-taking. Other child care packages referenced by participants in our focus groups included family care and babysitter care, babysitter care and friend care, and additional combinations of formal and informal care. Because of this range of child care combinations described by parents, child care packages here refers to a greater, and less tidy, range of categories than described in previous literature.
Child Care Arrangements.
Overall, mothers described the practice of using unregulated care as a kind of care map with many intersections, multiple directions, and multiple players. The drivers for using unregulated care, as discussed by mothers in our focus groups, were primarily synonymous with the benefits of using unregulated care, with one important exception: many of the participants in our study who used unregulated care indicated that they were unable to find available and affordable regulated care, and unregulated care, particularly care by grandmas, became the default.
Unregulated Care in Practice: “It’s a Little Bit All Over the Map.”
Many participants’ stories of unregulated child care paint a picture of arrangement complexity. Almost one third of participants in our study who used unregulated care used more than one unregulated child care type, nearly a quarter of our sample used a combination of formal and informal child care, and still others used formal child care with multiple types of informal child care. Here, we discuss the situations in which at least one type of unregulated care was used.
Sonja,
3
who worked part-time in a health profession, described the variety of care arrangements used for her preschooler: I worked three days a week and we had family and friends taking care of our 2-year-old. So, it was a combination of my sister would take her usually once a week, my mother-in-law would take her another day, and my mom would take her a different day. But, those days were different most weeks. So, usually every month we would figure out who was gonna do each day, that week. And, every now and then we would have to get friends to watch if there was a gap. (FG15)
Courtney’s child care arrangement—including grandparent care, parent-turn-taking, and friend care—for the youngest of her three children also reflects this complexity: Our youngest is 4 years old and [ . . . ] she’s in preschool 2 days a week and then one day she’s with her grandparents. And most of my time I’m in school and I work from home. So, I just try to work around that schedule of child care. And my husband does shift work, so we try to coordinate, like I work when he’s available, around his shift. And sometimes I go in to an office to work for a different job and my friend then, comes over for a few hours. Our life changes every 2 weeks, so we try to make [child care] as consistent as possible but it’s . . . yeah . . . it’s a little bit all over the map. (FG15)
As a final example of multiple, informal, unregulated child care arrangements, Anjum, who was completing graduate studies and working on a casual basis as a teacher, relied on multiple informal child care arrangements to supplement child care needs around a preschool program: I was doing playschool two mornings a week and then I had an afternoon community program once a week for about 2 hours, 2½ hours, and then we have different babysitters that come and go, and then sometimes when I had meetings I would lean on a friend and drop off . . . (FG16)
For some families, even the use of a single unregulated child care arrangement had an overhead of coordination and contingency planning. Debra, who took turns caring for her preschool-aged child with her partner, considered their situation less-than-satisfactory: And, then, our baby, our little guy, is just being juggled right now. My husband works shifts, so he works six days on and three days off, and half of those days are start in the afternoons, and so then he has mornings off to look after him, and so I go to work early in the morning and then come home at noon and he leaves for work, and some days I bring my child to work, and some days I don’t go to work you know? . . . it’s not working very well. (FG2)
In short, child care arrangements were messy, complicated, and often unsatisfactory. Why then, did mothers use these arrangements? We detail the drivers of unregulated child care below.
Motivations for Unregulated Care Use
Trust: “It’s Family. And I Trust Them For the Most Part.”
When mothers in our study discussed the reasons they used unregulated child care, over one third of their discussions centered on the high trust they had in their unregulated child care providers, particularly grandparents and other family members.
Participants described a high level of trust and confidence in family caregivers. Brodie reflected, “With your family you’re confident. You’ve seen them raise whoever, but with somebody outside, you don’t know them that deep and personally to trust them with your own little guys, right” (FG12)? Similarly, Lizzy, whose mother cared for her preschool-aged children, echoed this trust: “The best thing for me is that it’s family. And I trust them. For the most part. They come to me, so I don’t even have to drive them anywhere, which is, like, super delightful” (FG15).
In some instances, participants attributed higher trust to unregulated caregivers based on prior negative experiences with, or skepticism about, other care types. Mothers found family care as protective against the anxiety associated with other care types. For example, Illona expressed concern with having her preschooler in the care of anyone but family: I’m protective, I’m paranoid about things happening. I feel comfortable with my mom and dad or family watching them, and a few close friends, but other than that, I just, I don’t know. I always imagine the worst things are going to happen . . . (FG6)
Angela’s trust in grandparent care was reinforced by anecdotes about nanny care: “I hear horror stories about nannies and people buying Nanny Cams and so I trust my mom and dad and they’re . . . it’s family. Well, and if your kids are getting a licking, it’s with love” (FG12).
For some families, the decision to use an unregulated care provider—even one they trusted—was accompanied by a sense of risk. Nikki, who relied on a babysitter to care for her child, described the tension involved for her in using unregulated care: . . . the lady across the street had a long-time friend that she used to work with who was her babysitter. So, we interviewed her and we liked her, but I was still a little nervous because, you know, this is not regulated. Really, it’s just a friend watching her child. (FG9)
Even though this child care provider was recommended by a trusted source, Nikki, like some other mothers, suggested that she would prefer regulated care. Trust in unregulated care, for some, had its limitations.
Values: “A Stand-in Me.”
Across unregulated child care types, participants expressed a desire to have their values affirmed by the caregiver and cited this as a reason for deciding to use unregulated care. Mothers who used grandparent care felt congruent values facilitated and reinforced this decision. As Amber commented: I knew that having my mom watch my daughter would mean that the relationship we have is that her values and mine are very much the same, our approach to discipline is very much the same and I knew that my daughter would be comfortable and safe with her, right? So, it was kind of a no-brainer when she said, “Yeah, I’ll do it.” It was easy. (FG9)
Kazia reflected, “For us, the best thing I find in the child care is just having grandparents that affirm the same values that we are teaching at home. And so that was a top priority for me” (FG15). Based on shared values, one expectant mother in our study planned to use her mother for child care: What I would look for in childcare is somebody that’s a stand-in me. I can’t be here right now, but I still want you to do what I would want you to do and be how I would want you to be. [ . . . ] But if you’re going to grandma’s house, hopefully it’s similar family values to what you already have so that, you know, it’s easy. (FG9)
Mothers who used nonfamily unregulated care types also referred to values as a support for their choice. Melissa, whose daughter was cared for in an unregulated day home, shared: When we picked [our caregiver], we just had aligned values. We could see that things were aligned in the way that she does her day and, you know, the importance of naps and healthy eating and being outside. Just those things that are important to me, is what she does. (FG5)
Care Environment: “It Mimics What We Do in Our Own Home.”
For mothers in our study, another driver to use unregulated child care was the opportunity to have their children cared for at home, or in a home-like setting. This driver applied to the decision to use informal unregulated carers, such as grandparents, friends, neighbors, or babysitters, as well as to formal unregulated carers, such as unregulated day home caregivers.
Mothers mentioned convenience, environmental consistency (in relation to space, toys, and food), and routine consistency (such as napping) as benefits to care provided at home or in a home-like environment. Jessika worked part-time as a nurse; her older children had been cared for in a daycare setting, but she used a number of different babysitters to care for her preschoolers: “I just love them being at home, too, and not having to get them bundled up and taking them out, and I’ve done that for a season so this is like, that aspect feels refreshing” (FG16). Melissa valued the home-like environment—which she perceived in the structure and food provided—of the unregulated day home her daughter attended: With my daughter’s caregiver, she was a kindergarten teacher at one point so she understands children very well and how, I mean, she has a structure that really mimics the structure we’ve always had in our home and she feeds them homemade food which is something . . . it just mimics what we often do in our own home. (FG5).
Mothers valued the perceived consistency of in-home or home-like care offered by unregulated caregivers.
Lack of Availability and Affordability of Preferred Care: “Put the Grandmas Into it.”
Participants’ stories of how they arrived at using unregulated care share a common theme: unregulated care is often a “last resort” when other options are either not available or are not affordable. Jessika described how her family came to use a combination of different babysitters for her preschool-aged children: . . . with our fourth [child] we found a young girl to come in to our home, and that was a choice. A day home—we couldn’t find spots that would take a 1-year-old, and had a spot for 4-year-old, so we had options of like splitting them up between two day homes and that seemed, at the time we were like, “Yeah we could do that,” and then it seemed absolutely ridiculous to try to do that, and get to work on time, and not be crazy. So then we just looked in to finding an option with someone coming to our home and so we looked in to nannies.com, then put an ad on Kijiji and got some random people, and then just really through Facebook was how we found our first girl that did three days a week . . . (FG16)
For Rachel, who worked shifts, the child care her family required and at a cost they could afford, was not readily available: I was doing 12-hour shifts initially with childcare. It was a cost thing. [ . . . ] I had to be at work by 7[am], so to get to a place that would be willing to take them by 6. That was hard to find a place that would take them that early. It was a combination of there really wasn’t what I needed available and it was more cost effective to not pay. So, that’s when we kind of put the grandmas into it. We’ve been able to ride that train for a while. Sometimes the quality of care is like, “You fed them marshmallows? Ok. How much . . . ?” I’m not complaining it’s been good overall. (FG15)
In particular, the decision to use an unregulated day home was arrived at by a number of mothers in our study after they had explored, and exhausted, other options. Dance teacher Tania’s story illustrates this point: I was having trouble, and I wanted a day home for 1 day a week so that I could get everything done on 1 day, I would teach, volunteer, teach. One person, right? And nobody would take you. It’s just, they’re like, “No we want full-time,” and I went to the day home place or the daycare, and they’re like, “Well, between us and the agencies, you need to find somebody to fill the other four days, otherwise you don’t get a spot.” And it’s like, “Well, nobody’s going to want the four days that I don’t want.” So, luckily there’s a mom that comes here all the time and she has an unregistered day home and she took my kids. (FG13)
Similarly, Wendy noted, “It is a private day home, so she’s not through an agency, but, [ . . . ] you try anywhere on the list to find a day home and it’s next to impossible” (FG9).
Many mothers weighed the cost of other forms of child care before deciding to use unregulated care. Carol, whose daughter was cared for by both grandmothers, shared: Cost was a factor, ‘cause we’re very lucky to have family take care of our daughter and I went back to work before my daughter was one—like she was about 9 months old—so, I was quite apprehensive to find other kinds of childcare. And, actually, to find childcare for a kid under 1 is very difficult and very expensive. We thankfully have pushy mothers who recommended themselves, kind of told us that they would prefer that we use them instead of finding other kinds of childcare. (FG15).
In sum, a lack of available, affordable, and flexible options led some mothers to choose unregulated care, even when they recognized that the care quality might be compromised.
Discussion
This study contributes to fulfilling a research gap about the motivations and experiences of families who use unregulated child care within what has been dubbed the “child care crisis” (Davies, 2012), “the child care deficit” (Purdy, 1998), and the patchwork of care. In this study, we explored and problematized the use of unregulated child care to consider how a lack of regulated child care in the Province of Alberta affects the potential for demotherization for mothers of preschool children. We show that in the midst of substantial regulated child care shortages, mothers draw on unregulated care, often from grandparents, to patch together their child care needs. A key contribution of this study is its exploration of child care use by families in their day-to-day lived realities. Importantly, we did not attempt to slot child care use into preexisting categories, but rather allowed the participants to explain in detail the ways that they met their child care needs.
Without exception, mothers in our focus groups expressed a desire for quality child care environments for their children. Quality child care environments were equated with child care that mothers could trust. Consistent with other studies (Bryson et al., 2012; LeBihan & Martin, 2004; Reschke & Walker, 2005; Stoll et al., 2015; Wheelock & Jones, 2002), our analysis shows that unregulated care was trusted because it was generally provided by family (grandparents) or close friends who held similar values. Motivations for using unregulated care were, by and large, framed by our participants as the benefits of unregulated care.
Importantly, one driver for unregulated child care use that was not seen as a benefit was the lack of accessible, affordable, regulated child care. In addition to choosing unregulated kin care due to the trust and flexibility associated with it, our study shows that in many cases, unregulated care offered by a range of sources became a default choice: regulated care was not amid the array of options considered because mothers were unable to find regulated child care that was accessible, affordable, and flexible enough to meet their needs. The various motivations for using unregulated child care thus paint a more nuanced picture of child care choice: this depiction suggests that the constraints to finding affordable, accessible, and quality regulated child care may be more of a motivation for using unregulated care than previously found. Although not explicitly stated by mothers in our study, analysis shows that unregulated care became the driver of how mothers organized their time. In other words, child care was not arranged around the employment needs of mothers; rather, employment opportunities were arranged around the availability of child care. This finding has substantial implications for understanding the employment decisions of mothers, and warrants further research attention.
In popular child care discourse, parental choice is assumed to guide the child care and employment decisions of mothers with preschool children. Fagan (2001) argues that the language of preference is somewhat problematic because preferences are “expressed from the vantage point of current circumstances, needs and the range of perceived feasible alternatives, and would be expected to change in different circumstances” (p. 244). Likewise, Ellingsæter and Gulbrandsen (2007) highlight the difficulty of explicating preference because of the powerful influence of the social context in which preferences are formed and expressed. Rather than preference, they suggest enhancing “understanding of the social preconditions of preferences; the circumstances shaping and changing preferences and choices” (Ellingsæter & Gulbrandsen, 2007, p. 656). They propose that opportunity structures—the social, economic, and political context, social norms and specific choices available to persons within any given society—are a critical precondition for preferences. As maternal employment and/or child care opportunities increase, so do more accepting attitudes about nonparental child care (Ellingsæter & Gulbrandsen, 2007; Himmelweit & Sigala, 2004).
Canadian research on child care preferences for employed mothers shows that the kind of care used may not reflect the type mothers want (Beaujot et al., 2013; Beaujot, Ravanera, & Du, 2010; Bibby, 2004; OECD, 2004). Using data from the Canadian General Social Survey, Beaujot et al. (2010) found that 20% of parents in their sample who were using nonparental child care would prefer to use another type. Parents using “care in someone else’s home by a nonrelative,” followed by “own home care by a relative” were the most dissatisfied (Beaujot et al., 2010). Although participants in our study indicated that they were generally satisfied with unregulated care, particularly kin care, because it was trusted and in a home environment, participants also acknowledged that some of the care was not ideal. Particularly when family members offer care, it may be that parents are more tolerant of less than ideal circumstances, because the care is provided by a known entity, offered by caregivers they trust. That does not mean, however, that with a greater range of options they might not prefer another type if it was available.
Notably, Beaujot et al. (2013) found that in Quebec, the vast majority of parents (73%) of children aged 0 to 4 years used nonparental child care, whereas in the rest of Canada fewer than half (41%) of parents did. These findings suggests that having access to regulated child care affects the usage rates of nonparental child care and raises questions about the effects of a lack of regulated child care spaces among Canadian families outside of Quebec. In a similar vein, Brady and Perales (2016), examining child care in Australia, question whether parental choice in relation to child care arrangements is genuine, or simply a “coping strategy” (p. 340) put in place to manage a number of variables and constraints. More understanding is needed to tease out how preference, choice, and constraint shape the use of unregulated child care in current policy environments.
We show that mothers in the current child care policy climate in the Province of Alberta, like many other sites in Western societies, have limited state solutions to meet their child care needs; within this context, they turn to family, friends, and others to meet these needs. Our current child care policy framework suggests a predominant focus on traditional maternalism with some elements of implicit maternalism (e.g., maternity leave provision), and some elements of familialized dematernalism (e.g., kin care payments). Using unregulated care to fill the void of regulated child care further entrenches the ideological climate of traditional maternalism that reinforces the notion that it is mothers, and mothers alone, who should bear the primary responsibility for child care provision. Until this ideology and subsequent policy framework change, demotherization will not be achieved.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by The Alberta Centre for Child, Family and Community Research, and the Killam Research Fund, University of Alberta.