
Abstract
Per minority stress theory, sexual and gender minorities are susceptible to bias-related social stressors that can internalize and increase their susceptibility to poor physical and mental health. Parents of transgender/gender-expansive (TGE) children may also encounter a number of stressors on account of their child’s gender experience. No known research had examined how these stressors align within a minority stress framework. This qualitative study examined and characterized minority stress phenomena in a clinically derived sample of English-speaking, cisgender parents of TGE children aged ≤11 years. Study findings included reports of distal and proximal forms of minority stress, with notable impact on health and well-being. Researchers highlight treatment implications and suggest studies continue to examine minority stress in parents of TGE children.
Transgender and gender-expansive (TGE) individuals have diverse gender identities or expressions that may not conform to culturally defined norms associated with their sex assigned at birth (Adelson, 2012). A growing number of TGE children and their families seek medical and mental health support in the United States (D. Chen et al., 2016; M. Chen, Fuqua, & Eugster, 2016) and abroad (Wood et al., 2013). This increase may result, in part, from several factors including a socially driven vulnerability to negative mental health outcomes, greater mass media awareness of transgender experiences, as well as increasing availability of gender-affirmative, nonpathology-oriented approaches to clinical care with TGE youth and their parents (Drescher, 2010; Edwards-Leeper, Leibowitz, & Sangganjanavanich, 2016; Hidalgo et al., 2013; Shires, Schnaar, Connolly, & Stroumsa, 2017). Several have noted that many parents of TGE children encounter a number of stressors associated with their child’s gender identity or experience (Brill & Pepper, 2008; Malpas, 2011) along what some have characterized as a “complicated and precarious [parenting] journey” (Ehrensaft, 2011; p. 169). These stressors resemble minority stress and may take a toll on the health of parents and, in turn, families. Parenthetically, it should be noted that the published literature has focused on parents who are cisgender (i.e., individuals whose affirmed gender corresponds with their sex assigned at birth; Simons, Leibowitz, & Hidalgo, 2014).
Minority stress theory posits that sexual minority (Meyer, 2003) individuals are subjected to “distal” and “proximal” stressors on account of their sexuality which, in turn, increase their vulnerability to negative mental and physical health outcomes. Distal stressors may include forms of discrimination and/or victimization that are codified through laws, policies, and cultural norms. Proximal stressors are experienced at the individual level and may include an individual’s perceived discrimination/hypervigilance, internalized homophobia or transphobia, or concealment of minority experience/identity. While minority stress theory was originally proposed to help explain disproportionate physical and mental health disparities in sexual minority adults (i.e., lesbian, gay, bisexual; Mays & Cochran, 2001; Meyer, 1995, 2003), in recent years, it has been adapted to reflect the minority stress experienced by TGE adults (i.e., gender minority stress). Gender minority stress posits that vulnerability to negative health outcomes among TGE individuals may be due to negative distal and proximal forces associated specifically with gender identity and/or expression (see Figure 1; Hendricks & Testa, 2012; Testa, Habarth, Peta, Balsam, & Bockting, 2015).

Gender minority stress and resilience factors.
The gender minority stress experiences of prepubertal children are understudied but national surveys suggest school-based harassment is not uncommon in gender minority youth in grades K-12. For example, experiences of discrimination and victimization on account of gender expression are reflected in a recent national survey assessing school climate among adolescent sexual and gender minority students. Indeed, 40% of students surveyed reported feeling unsafe at school and hearing negative remarks about transgender people, over half was verbally harassed, and 20% experienced physical harassment (Kosciw, Greytak, Giga, Villenas, & Danischewski, 2016). According to retrospective reports by adult respondents completing the National Transgender Discrimination Survey (James et al., 2016), 77% of respondents reported experiencing gender-related harassment in grades K-12. While the proportion of these discriminatory experiences that predate adolescence is unknown, it may be that some youth are referencing experiences dating back to early or middle childhood.
It is during early and middle childhood when a child’s parenting figures are primary agents in their children’s psychosocial and emotional development (Bronfenbrenner, 2005). Even in this early stage of development, parents of TGE children witness forms of social discrimination or other stressors directed toward their children on account of their gender identity/expression (Dierckx, Motmans, Mortelmans, & T’sjoen, 2016; Hill & Menvielle, 2009). In one case study, a mother of a 6-year-old transgender girl reported experiences of ridicule from family and peers, which contributed to self-blame (Johnson & Benson, 2014). Parents also report heightened negative outcomes among TGE youth, including suicidality and self-harming behavior (Aitken, VanderLaan, Wasserman, Stojanovski, & Zucker, 2016; Perez-Brumer, Day, Russell, & Hatzenbuehler, 2017). Other research noted that, in contrast to parents of TGE adolescents, those parenting prepubertal TGE children may be more likely to conceal their child’s gender experience from others out of fear of ridicule (Wren, 2002). Parents may also hold negative internalized beliefs about gender nonconformity—reinforced by messages from family members, peers, school policies—that make it difficult to affirm their children’s gender identity and/or expression (Wren, 2002). Perhaps also unique to the experiences of parents of TGE youth are the experiences of grief, loss, and coping strategies that some parents report subsequent to (or in anticipation of) the gender transition of their child (Norwood, 2013).
Results from a mixed-method study examining perspectives about the future among transgender youth (aged 7-18 years) and their parents indicated that parents most frequently worried about the physical and emotional safety of their children (Katz-Wise et al., 2017). Other studies note challenges including anxiety about their child’s possible “change of mind” regarding their identity (Sansfaçon, Robichaud, & Dumais-Michaud, 2015) and worries about their children’s societal treatment now and in the future (Kolbuck, Chen, Hidalgo, Chodzen, & Garofalo, 2017; Kuvalanka, Weiner, & Mahan, 2014; Rahilly, 2015). In one sample of parents, this anxiety, while falling within the normative range, was slightly higher than that of the average parent (Kuvalanka, Weiner, Munroe, Goldberg, & Gardner, 2017). However, it is less understood whether the negative experiences reported by parents of TGE children constitute a form of gender minority stress. While no known study has applied a minority stress paradigm to parents of TGE children specifically, results from a qualitative study of 14 Canadian parents suggest that minority stressors underlie emotional challenges they face, including stress, anxiety, and loneliness (Sansfaçon et al., 2015).
The practice literature has highlighted methods to address social stressors rooted in stigma, which may serve as barriers to a parent’s acceptance of their TGE child’s gender identity/expression. For example, parent–child attachment problems and marital conflict may arise when a parent’s method to protect their TGE child from social discrimination and other stressors is by limiting or discouraging their child’s authentic gender identity or expression. This formulation is the assumption of Malpas’ (2011) Multi-dimensional Family Approach (MDFA), the only known therapeutic model that highlights specific components and objectives in supporting parents of TGE children. The MDFA aims to ultimately support parents to realize that acceptance of their TGE child “is protection” through parent-focused treatment objectives including careful assessment of gender beliefs, psychoeducation, parental coaching, and dyadic therapy with parents (when discrepant support is present between parents).
The Current Study
We analyzed secondary data to examine gender minority stress experiences among a sample of parents of TGE prepubertal children who participated in focus groups of a larger study focused on how, if at all, emotional and behavioral problems of childhood are uniquely expressed by their TGE children . Our research questions explored the presence of distal and proximal forms of minority stress reported by the sample, and its toll on parents’ self-reported physical, emotional, and/or behavioral health.
Method
Participants
The sample consisted of parents of prepubertal TGE children who presented for care within a subspecialty gender clinic housed within a pediatric hospital located in the Midwestern United States. All participants identified as cisgender although there was no eligibility criterion based on gender or gender history. The study was approved by the hospital’s institutional review board, and parents provided written consent prior to participation. Full details regarding study recruitment and eligibility criteria are noted elsewhere (D. Chen, Hidalgo, & Garofalo, 2017).
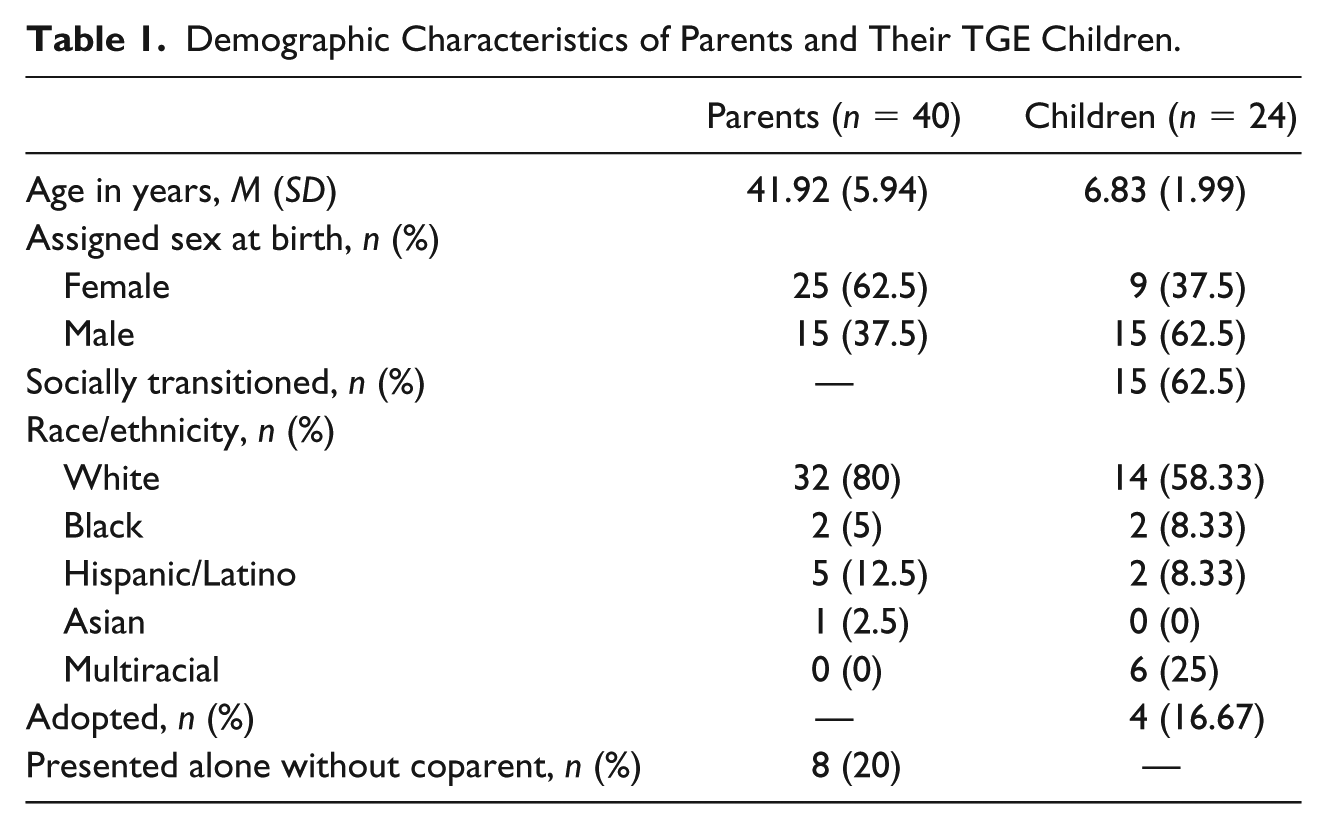
Researchers approached parents of 38 TGE children. Parents of two children were not interested, parents of four children did not respond to phone calls to determine eligibility, and parents of two children were unable to be scheduled. Thus, parents of 30 prepubertal TGE children were enrolled. A subset of these subjects participated in the current study, which consisted of a targeted focus group activity conducted from December 2015 to March 2016. The resulting sample was predominately European American and was composed of parents of 24 TGE children aged 4 to 11 years (see Table 1 for demographics; i.e., 40 parents; 8 participating alone and 16 participating as a dyad). Participants attended one of five scheduled focus groups. Their children varied by assigned sex at birth and degree of social gender transition, with the resulting characteristics: (a) seven gender-expansive boys (i.e., assigned males living as boys), (b) two gender-expansive girls (i.e., assigned females living as girls), (c) eight transgender girls (i.e., assigned males living as girls), and (d) seven transgender boys (i.e., assigned females living as boys).
Demographic Characteristics of Parents and Their TGE Children.
Targeted Focus Group Activity
Two licensed clinical psychologists with expertise in transgender health and qualitative data collection (Author 1, a Latino cisgender male, and Author 2, an Asian American cisgender female) conducted all focus groups, following a scripted protocol. Each focus group was conducted for 2 hours, involved 6-12 participants, and consisted of three segments: (a) discussion about unique experiences parenting a TGE child, (b) a targeted “free listing” activity asking parents’ opinions about common challenges that arise in TGE children and what has challenged them as a parent of a TGE child, and (c) discussion about programing to address challenges faced by TGE children and their parents.
The current study is based on data obtained from the second segment of the targeted focus group activity. In this segment, parents provided written responses regarding the personal challenges that arise in parenting a TGE child. The researchers chose to inquire about six specific problem areas often reported in the child/adolescent and family TGE literature (Dierckx et al., 2016; Malpas, 2011; Wahlig, 2015) and in the authors’ clinical practice experience: (a) anger, (b) sadness, (c) loneliness/isolation, (d) fear/worry/nervousness, (e) challenges managing stress, and (f) parenting conflicts with coparent. To elicit responses to each problem area, researchers employed “free listing,” a focus group activity intended to stimulate discussion about a particular domain (Bernard, 1995; Colucci, 2007). Parents commented on sheets of newsprint hung around the room, each titled with a different problem area. Comments were in response to the following probe: How, if at all, is this problem area related to your child’s gender nonconformity? Parents worked independently. Researchers assigned each participant a uniquely colored marker to match written data with each participant during analysis. Those presenting with a coparent were intentionally assigned to start at newsprint located across the room from one another. Participants rotated in a clockwise fashion in 3-minute intervals until every participant had completed all sheets. Researchers then provided the group with 5 minutes to review all sheets and add additional comments.
Qualitative Data Analysis
Researchers utilized a directed approach to content analysis (Hsieh & Shannon, 2005), the analytic steps of which are identical to those recently reported elsewhere (D. Chen et al., 2017). In brief, this analytic approach aims to expand understanding of an existing phenomenon to an understudied population where the phenomenon may be less understood (i.e., gender minority stress experiences applied to parents). This approach was consistent with a primary study aim: to explore how, if at all, parents of prepubertal TGE experience gender minority stress related to their children’s gender identity/expression. Researchers developed a qualitative coding framework informed by elements of the minority stress model, including proximal and distal factors, as well as psychosocial challenges parents linked to these factors. Resiliency factors, such as pride and community connection, have also been included in the gender minority stress model (Hendricks & Testa, 2012). However, the researchers chose to focus exclusively on stressors given that the data for this secondary analysis derived from short, parental responses to prompts about negative parenting experiences. This framework informed analysis by: (a) providing a guide to identify features of gender minority stress typically reported among TGE individuals and (b) providing a guide through which unique features germane to parents of TGE individuals could emerge.
Researchers employed a multiphasic, interrater coding process to establish reliability by combining pair and small group analysis with an external reviewer that possessed subject matter expertise (Miles & Huberman, 1994). The first two authors served as primary analysts. First, each analyst coded the focus group data independently per the coding framework. Once completed, to reduce independent rater bias, primary analysts met to establish consensus and resolve discrepancies. Once interrater consensus was established, and as an additional method of reducing bias, the coding pair established theoretical consistency by repeating the consensus-building process for data obtained in the first two focus groups with the external coder who provided feedback.
Using Dedoose (2015) software, researchers conducted comparative (i.e., cross-case) analyses according to differences by parent race/ethnicity, parent gender, by parent gender versus child sex, child’s gender expression or identity, or the degree to which (if any) the child had undergone a social gender transition (Miles & Huberman, 1994). True to the iterative nature of qualitative inquiry, researchers repeated each analytic phase until all available data were coded at least once and until novel codes no longer emerged from the data (i.e., saturation). No unresolved coding discrepancies emerged throughout the analysis.
Results
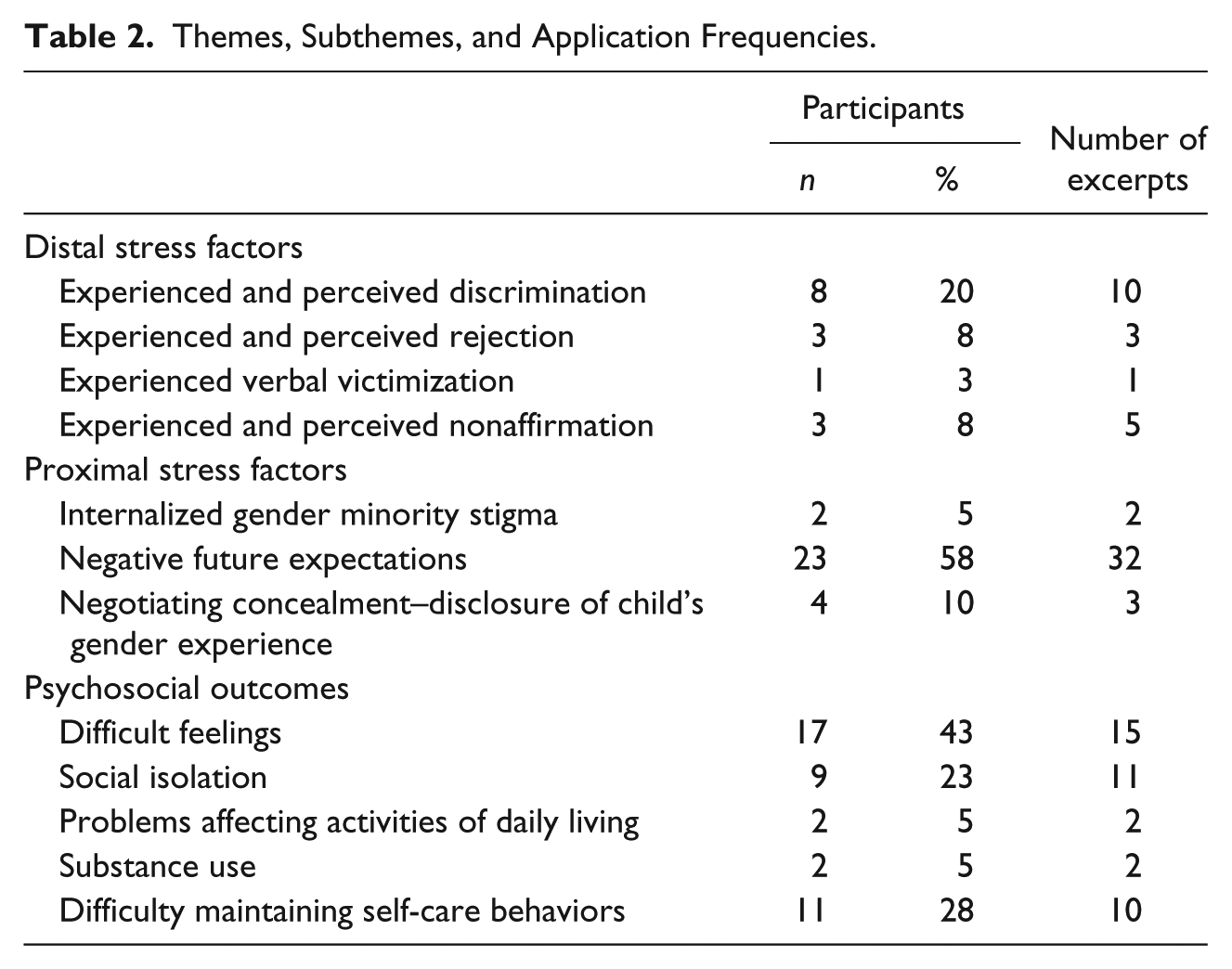
The analysis of free-listing data resulted in two major domains consistent with distal and proximal factors of minority stress, and a third domain in which parents linked experiences of stigmatization to their psychosocial health and well-being. In cross-case analyses, no observed differences were noted in prevalence or characterizations of the findings on account of parent race/ethnicity, gender, parent gender versus child sex, child’s gender expression or identity, or whether a child had undergone social gender transition (see Table 2 for themes, subthemes, and application frequencies).
Themes, Subthemes, and Application Frequencies.
The results are organized according to distal factors, proximal factors, and psychosocial health outcomes associated with gender minority stress (see Figure 2). Quotes are included to help characterize particular themes. Certain characteristic quotes may also include remarks from two participants. In most cases, these instances reflect when a participant contributed a free-text response to an item on the newsprint, and a separate participant who later encountered the same item wrote “I agree.” All participants have been assigned a pseudonym to assure their anonymity.
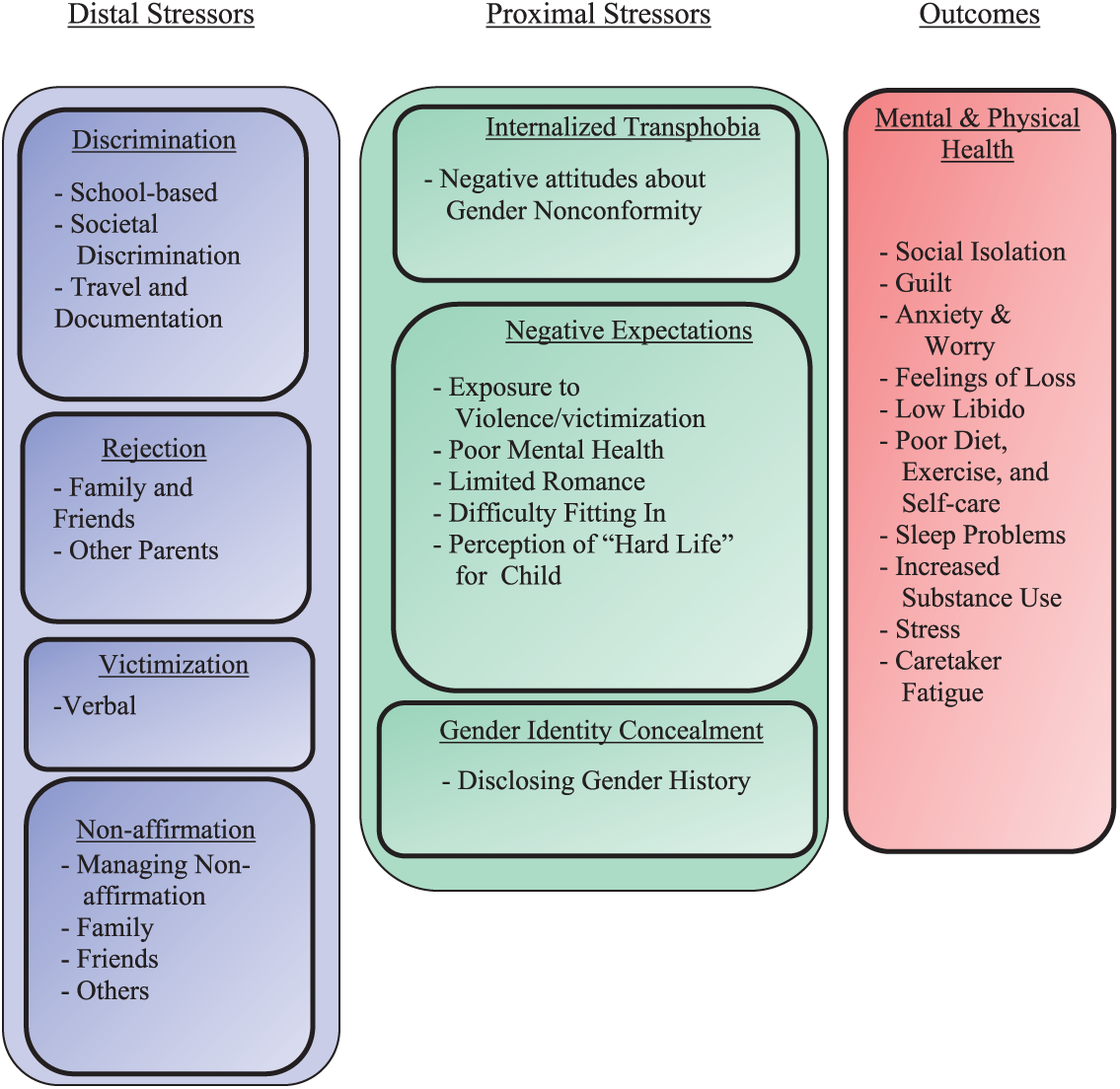
Forms of gender minority stress highlighted by parents of TGE prepubertal children.
Distal Stress: Experienced and Perceived Discrimination
Findings pertaining to distal factors of minority stress related to discrimination, rejection, victimization and nonaffirmation. These distal forms of minority stress emerged as either experienced and perceived, or solely experienced.
Parents reported three forms of this distal stress on account of their child’s gender identity/expression including peer discrimination, societal discrimination, and travel-related discrimination.
Perceived Peer Discrimination
Parents discussed peer discrimination as perceived (but not experienced), and predominately defined “peers” as other parents or unknown community members. Reports of this form of discrimination included perceptions of being scrutinized by peers, being watched when in settings with their child, and perceiving that peers are reticent to discuss their child when the parent is present. For example, one mother stated, “I’m guarded about talking with other parents and people because I don’t want to be the object of their curiosity” (Emily, mother of transgender boy). Other parents discussed an avoidant coping strategy to minimize this perceived discrimination altogether. For example, “I do find myself avoiding some social situations as I feel I’m being watched or I feel people being conscious of not talking about my child. Silence can be palpable” (Justina, mother of transgender boy; “Agree”—Ted, father of transgender boy).
Perceived Societal Discrimination
Parents unequivocally expressed that, when it comes to the experiences of prepubertal TGE children, society at large was ill-informed about their needs and the challenges faced by parents of these children. Nora, the mother of a gender-expansive boy shared, “Angry is a strong word, but [I’m] more frustrated at realizing that society is so gender biased. Where does my child fit?” (“Agreed”—Drew, father of transgender girl).
Experienced and Perceived Travel-Related Discrimination
When commenting further on her free-listed statement, a parent of a socially transitioned transgender girl remarked that new situations, especially those related to ticket-issue travel, in which identity documentation must be presented, can be stressful and result in experiences of discrimination (i.e., “[I’m ] Nervous for her in new situations. Travel [in which identity documentation must be presented].”—Shelby, mother of transgender girl).
Distal Stress: Experienced and Perceived Rejection
Parents reported three forms of either perceived or experienced rejection including rejection from family members, friends, or other parents.
Experienced Family Rejection
Parents described that extended family members from whom they experienced rejection were adults and not the child’s peers or adolescent family members. These forms of rejection were characterized as family members responding negatively such as refusing to learn more about their children’s gender experience, being “silent” or uninterested in this aspect of the parent’s experience, or criticizing or passing judgment on parenting practices. For example, “I have found that some family members rather not know and use the opportunity to criticize/judge” (Jasmine, mother of transgender boy).
Perceived Rejection by Friends
One participant attributed that her friends disengaged with her on account of their learning of her decision to support her child’s social gender transition. “[The] last 2 years [have been] pretty quiet regarding friends. They’re not checking in; they checked out” (Carly, mother of transgender boy).
Perceived Rejection From Other Parents
Parents reported feeling conspicuous and socially ostracized by other parents at times. In one notable case, this rejection occurred in gender-segregated activities in which the majority of participants were of a different sex assigned at birth (e.g., a gender-expansive boy joining a dance class designed for girls). “Our son [is] in ‘girls’ hip hop class; the other moms and girls kinda look at me; not a lot of convo” (Jackie, mother of gender-expansive boy).
Distal Stress: Experienced Verbal Victimization
The only form of victimization parents described was verbal in nature. This form of victimization included being referred to by others as a “bad” parent—“I do get angry occasionally when others tell me I’m being a bad parent” (Nick, father of gender-expansive boy).
Distal Stress: Experienced and Perceived Nonaffirmation
Parents reported three forms of either perceived or experienced nonaffirmation from others on account of their child’s gender identity/expression. These forms of nonaffirmation included others’ use of incorrect gender pronouns (i.e., “misgendering”), family-based nonaffirmation, and a general perception regarding future exchanges with nonaffirming individuals.
Experienced and Perceived Misgendering
Experiences of misgendering were reported exclusively by parents of children who had undergone social gender transition. Parents perceived that instances of misgendering were sometimes intentional and other times apparently inadvertent. One parent described “feeling hypervigilant about having to correct misgendering, etc.” (Shelby, mother of transgender girl).
Experienced Family-Based Nonaffirmation
Parents within extended family systems from which they had not experienced rejection on account of their child’s gender expression/identity described that these family members were still not fully supportive of their child’s gender experience. Parents described that family members would potentially obstruct affirming approaches parents chose to practice with their children. For example, “[I’m] nervous about how to get [maternal grandfather] on board, supportive, etc. Don’t want family to be an additional obstacle” (Wendy, mother of gender-expansive boy).
Anticipated Exchanges With Nonaffirming others
A final form of nonaffirmation was characterized as parents’ belief that experiencing nonaffirming reactions from others was inevitable. In light of this, parents worried about a range of ways in which they would respond in vivo to these situations. Two examples include, “[I’m] nervous about others’ reactions and my response to them.” (Betty, mother of gender-expansive boy) and “I worry that I will snap if someone insults my child. I worry that I might hit someone rather than walk away” (Steven, father of transgender boy).
Proximal Stress
Findings pertaining to proximal factors of minority stress in parents were related to internalized gender minority stigma, negative expectations about the future, and challenges with managing their child’s gender identity concealment–disclosure to others.
Internalized Gender Minority Stigma
Parents reported an internalization of stigmatizing societal attitudes related to gender-role behavior in their children. Specifically, parents of gender-expansive children (i.e., those who had not undergone social gender transition) reported being influenced by societal mores that admonish gender nonconformity in their children. For example, Juliette, the mother of a gender-expansive girl, stated “On several occasions I find myself getting upset with [child] when she isn’t or doesn’t want to conform to a ‘girl’ type.”
Negative Future Expectations
Parents reported an anticipation of negative future experiences tied to their child’s gender identity/expression. All parents who reported these experiences proposed them as negative events that their child would potentially face. The negative future expectations parents anticipated for their children included exposure to violence/victimization, poor mental health resulting from minority stress, limited romantic options, difficulty fitting in with others, and a general perception that their child’s life will be difficult. These themes are characterized by quotes below.
Exposure to violence/victimization: Fear of who will hurt my child physically/emotionally. (Gene, father of gender-expansive boy) Fear of public confrontations, harassment at public places. (Justin, father of gender-expansive boy)
Poor mental health due to minority stress experiences: [I fear my child will have] self-harm, suicide, [and] addiction. (Emily, mother of transgender boy) I’m sad and fearful for his future in terms of mental/physical abuse, risk for drug use, suicide . . . (Elliot, father of gender-expansive boy)
Limited romantic options: [I’m] sad that he might struggle finding a suitable partner. (Ted, father of transgender boy; “[I] Agree”—Steven, father of transgender boy)
Difficulty fitting in: [I] worry about him feeling like he belongs, has normal experiences, feels happy and safe. (Claudia, mother of transgender boy) [I] fear others making her feel less than. (Shelby, mother of transgender girl)
General perception of child’s “hard life”: [I feel] sadness when I think about how lonely/confused he may feel or when I think about the challenges he will face. Will he have a ‘hard’ ‘unhappy’ life? (Nora, mother of gender-expansive boy; “Agree”—Drew, father of transgender girl; “Yes, I’m concerned about this as well.”—Trevor, father of gender-expansive boy)
Negotiating Concealment–Disclosure of Child’s Gender Experience
Parents of both gender-expansive and transgender children reported being challenged by the degree to which they disclose aspects of their child’s gender identity or gender history with others. The parameters of disclosure included whether to (and how to) disclose their child’s gender history (i.e., their sex assigned at birth). For example, Steven, the parent of a transgender boy stated, “[I] don’t know what to say to those who assume off the bat that he is natal boy. Am I lying to them if I don’t say anything?”
Psychosocial Outcomes
Families did not report any problems with physical health on account of their children’s gender expression/gender identity; however, they reported various negative psychosocial health problems including difficult feelings (e.g., loss, guilt, anger, low libido, etc.) and social isolation. Parents attributed these problems to affecting activities of daily living (e.g., poor sleep, diet, and exercise), low energy, substance abuse, and difficulty maintaining self-care behaviors. For example: I feel guilty about not seeing the signs [of my child’s gender identity] earlier. (Lydia, mother of transgender girl) [I] feel sad to lose a son, and I feel guilty about that. (Betty, mother of gender-expansive boy) [I’m coping] through over indulgence in food/drink/drugs. (Steven, father of transgender boy) [I] have gained 9 lbs. in 6 [months]. [I] am binge eating junky [sic] food to sooth self. Very little self-care exercise. [This] affects my libido which affects my marriage. (Justina, mother of transgender male; “Agree”—Wendy, mother of gender-expansive boy) [I’m] not finding balance or time for myself and doing things for myself–exercise, hobbies, etc. (Wendy, mother of gender-expansive boy)
Discussion
In this study, researchers conducted a secondary analysis of focus group data about parenting experiences from parents of TGE prepubertal children gathered through “free listing,” a qualitative data collection method intended to stimulate discussion. The purpose of the current study was to examine experiences consistent with gender minority stress from parents of TGE prepubertal children. The study findings suggest that parents in the sample, who are involved in care at an affirmative, pediatric gender health clinic, may themselves be subject to gender minority stress experiences that impact their psychosocial well-being. Briefly discussed here are notable themes that emerged from these findings and some implications for clinical practice with parents of prepubertal TGE children.
Participants reported experiences consistent with distal and proximal forms of minority stress. Within the realm of distal stress factors, difficult interactions with family members characterized stressors related to rejection and nonaffirmation. While these two domains may be similar in name, they differed in important ways. Rejecting experiences were characterized as those in which family members were not at all willing to accept a child’s affirmed gender or the participant’s choice to affirm their child’s gender in any degree. In contrast, nonaffirming behaviors were often reported from family members who had, at the very least, not demonstrated complete apathy, disinterest or contempt for the parent’s affirming approach but did engage in behaviors such as misgendering the child or making statements to parents that imply the child’s gender expression is a problem behavior (e.g., “they’ll grow out of it”). This second group was similar to results from other studies in which family members were not supportive of the child’s gender transition or the parent’s affirmation of this decision (Kuvalanka et al., 2014; Sansfaçon et al., 2015). Most notably, mothers of prepubertal transgender girls at various phases of social gender transition (Kuvalanka et al., 2014) characterized family members as initially hesitant or resistant but ultimately accepting of the child’s gender transition.
The MDFA, as described previously, is a multimodal (e.g., parental coaching, education, and family therapy) model that aims to support parents in maintaining affirming and healthy attachments with their TGE children. Particularly relevant to our findings are the parental psychoeducational and coaching components of the MDFA model. Psychoeducation can be provided on topics related to gender development, research findings (and their limitations) on pediatric gender dysphoria and its course, and the critical role of parents in providing nurturance, affirmation, and advocacy. Parental coaching builds off of this knowledge with the aim to empower parents as resources and decision makers in issues affecting their child’s well-being. Parental psychoeducation and coaching are often integrated in clinical practice.
A clinician informed by the MDFA model may employ parental psychoeducation and coaching as they help parents build gender-affirming capacity in their family systems. For example, employing psychoeducation to distinguish rejection from nonaffirmation can be potentially helpful for parents who are aiming to identify family members that are more likely to engage in thoughtful discussion about their child’s gender development. Our findings suggest that the family members parents categorize as nonaffirming could be more amenable to affirming a child than family members they characterize as rejecting.
Also notable from the findings were various concerns participants voiced regarding the effect of situations in which their children experienced nonaffirming gestures (e.g., misgendering their child) or inappropriate comments from other adults while in their presence. Some parents feared the occurrence of these situations from strangers in public settings, and others feared that their reactions in these moments would be negative or ineffective and, in turn, adversely affect their child. Implicit in these concerns were parents’ attributions or perceptions that these negative situations arose/would arise from the ability of others to discern that their child was obviously of TGE experience.
Given how common this theme emerged in this sample, it is likely that parents with similar backgrounds will often present to therapists to discuss methods on managing negative reactions from others. No known literature has examined the methods parents of TGE children employ to manage these negative and inappropriate comments. However, the transracial adoption literature has examined such methods, particularly those employed by parents whose racial characteristics differ from those of their children. In a study of 245 parents of transracially (and transnationally) adopted children from China, parents were found to respond to challenging questions and comments by employing one of three strategies aimed at affirming their family identity: (a) educating/correcting the individual, (b) contradicting/challenging their comment or question, or (c) answering the question directly (Suter & Ballard, 2009). Other sources have also suggested additional strategies including responding with humor, or employing a privacy-guarding technique (“None of your business”; Partners, n.d.). A review of each specific response strategy and how it may be applied to parents of TGE youth is beyond the scope of this article. However, to illustrate one example, a parent employing an educational/corrective response to a comment that their transgender daughter “looks just like a real girl” might state as follows: “She is a real girl, and we all know that all real girls look different from each other.” Therapists can facilitate role plays of similar strategies with parents, which can ensure their self-efficacy and, in turn, also reduce concerns regarding their inability to manage such a situation.
The majority of findings on proximal stressors pertained to negative future expectations. However, parents discussed negative expectations regarding their children’s futures as opposed to any negative expectations regarding their own futures. While these findings are absent in minority stress literature, Katz-Wise et al. (2017) did report similar themes among parents of transgender youth. Parents reported concerns about their children facing challenges stemming from discrimination, potential safety concerns, and challenges in relationships, When considered together, these findings highlight the potential for foundational cognitive–behavioral approaches, such as cognitive restructuring, in specifically targeting a number of negative future expectations parents harbored on their children’s behalves (Beck, Rush, Shaw, & Emery, 1979). These negative future expectations included worries about victimization, limited romantic relationships, nonacceptance, and poor mental health. However, it is important when employing these approaches to critically consider the treatment assumption that the source of negativistic thinking stems from inaccurate, maladaptive cognitive patterns. In fact, among parents of TGE youth, these negative future expectations often arise in response to current events and social media reports of violence, suicidality, and social discrimination experiences tied to gender minority status. Parents/caregivers may benefit from time with a therapist, separate from their children, in which they can discuss their concerns for their child’s safety, and how to minimize the effects these concerns have on their own health and ability to affirm the child’s gender experience. The integration of mindfulness and acceptance strategies (Hayes & Lillis, 2014) may be particularly helpful in therapeutic work with parents of TGE children.
Limitations
Participants reported experiences of distal and proximal stress within this secondary analysis of focus group data from a larger study. However, the findings of this study must be considered within the context of its methodological limitations. Most notably, themes of parent minority stress may have emerged more readily in this sample since data emerged from a larger study aimed at examining how, if at all, emotional and behavioral problems of childhood are uniquely exhibited by their TGE children. Second, the authors’ framing of “problem” behavior may have inadvertently introduced a response bias where parents were deficit-focused and less inclined to recognize the valid or adaptive qualities of certain emotions or behaviors in their children (e.g., anger being a valid and appropriate response to social stigma). All participants were recruited from the same clinic, which was a gender-affirming multidisciplinary specialty program, representing a potential source of bias and thus limiting generalizability. For instance, parents not actively seeking care may not experience minority stress-like experiences to the degree our sample reported. Alternatively, parents may not seek support at a subspecialty care program for TGE youth due to experiencing other proximal stressors such as internalized stigma, guilt, or poor family support. The sample may also not reflect experiences of racial-minority parents, younger parents, and male-identified parents. Perceptions of social stigma, cultural norms related to gender-rearing and overall focus group participation may have varied with a sample more diverse in these areas. Another limitation is that the design of the larger study from where these data were gathered was primarily quantitative, thus limiting aspects of inquiry and the qualitative methodological approach. For instance, directed content analysis was conducted after all data were collected, which did not allow for additional themes to be explored, or credibility checking (i.e., “member checking”) of emerging themes with parents of TGE children during the data collection period. Furthermore, in the “free listing” method employed here, participants’ written responses may have been influenced by those of parents written before them. We attempted to reduce this limitation by requesting that, once all participants had interfaced with each sheet at least once, they review and comment on shared or divergent views expressed on the sheets.
Conclusion and Future Directions
Overall, the findings from this study indicate that there is a role for applying a minority stress paradigm to the formulation and treatment planning involved in gender affirmative family therapy with parents of prepubertal TGE children. A strength of the current study is obtaining narrative data from parents of prepubertal TGE children who identified many different examples of distal and proximal forms of stress and the ways in which these stressors affected their physical and mental wellness. In light of the stressors highlighted in this study, future research should also examine the degree to which parents report factors of resilience related to their parenting TGE children.
Footnotes
Acknowledgements
We thank Lisa Simons, Jennifer Leininger, Robert Garofalo, Scott Leibowitz, and Courtney Finlayson for their contribution to recruitment for this research. In addition, we thank the families who participated—we truly appreciate their time, effort, and thoughtfulness.
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Stanley Manne Research Institute’s Translational Research Pilot Study Fund at the Ann & Robert H. Lurie Children’s Hospital of Chicago and by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health (NIH) under Award Number R01HD082554.