
Abstract
Little work has considered the relationship between parental dissatisfaction and health and well-being among older adults. This study investigates whether parental dissatisfaction is linked to four health and well-being outcomes and whether the proposed associations are partly mediated by self-esteem and feeling useless in a 2014 sample of 432 community-dwelling older Chinese parents aged 60 to 79 years. Results from logistic and ordinary least squares regression modeling show that parental dissatisfaction is significantly associated with the four outcomes (physical health, mental health, depression, and life satisfaction), net of age, gender, and financial hardship. Findings from mediation analyses reveal that these associations are attributable to self-esteem and feeling useless both independently and jointly (with varying effects on different outcomes). Parental satisfaction contributes to healthy aging in China. It is important to develop interventions that enhance self-esteem and reduce feeling useless among older adults who are dissatisfied with their parental roles.
Although research on parent–adult child ties across the life course is increasing in both number and significance as populations age, much of the existing research focuses on how variables such as frequency of contact, living arrangement, and intergenerational transfers may affect parental health and well-being in old age (e.g., Kirchengast & Haslinger, 2008; Silverstein, Cong, & Li, 2006). Parental dissatisfaction in later life has received little scholarly attention in the health and aging literature, not to mention the possible psychological mechanisms through which parental dissatisfaction may affect older parents’ health and well-being. Recent studies, however, point to the importance of exploring these areas of research (Reczek & Zhang, 2016; Thoits, 2011; Uchino, Bowen, Carlisle, & Birmingham, 2012). Drawing on relevant aspects of symbolic interactionism perspective, the life course perspective, and the stress process model, the current study examines the associations between parental dissatisfaction and four health and well-being outcomes and explores the underlying psychological pathways in a sample of older parents in China.
The symbolic interactionism perspective and the life course framework are of particular relevance for deriving hypotheses about how and why parental dissatisfaction matters in later life. Social roles, according to the symbolic interactionism perspective, are positions or statuses in the social structure regulated by a set of normative rights and obligations, which give identity, guidance, purpose, and a sense of meaning to life through role involvements (e.g., Berkman, 2000; Thoits, 2011). Individuals assume multiple roles in life domains such as family, work, friendship, and the community throughout the life course and act in ways consistent with the behavioral expectations required by each role when interacting with others (Orth, Maes, & Schmitt, 2015). The life course perspective (e.g., Mayer, 2009) emphasizes that development and aging are lifelong processes and that the lives of parents and children are linked across the life course. In accordance with the two perspectives, the parental role represents “a life-long trajectory of shifting demands and responsibilities” (Milkie, Bierman, & Schieman, 2008, p. 87). Among all social roles an individual could possess throughout the life course, the parental role is found to be a prominent source of identity and ranked at the top of most parents’ identity salience hierarchies, even higher than their worker role (Thoits, 1992). Unlike most other social roles that have specified durations and clear boundaries, the parental role never ends and continues its reach into later life. The parental role might become even more important relative to other roles as individuals transition into old age where negative changes in social roles occur frequently (Pudrovska, 2009). The decision to have a child, made earlier in life, therefore has lifelong consequences for a wide range of parental psychological outcomes and life circumstances (Nelson, Kushlev, & Lyubomirsky, 2014), given that the parent–child relationship may provide a unique enduring social tie throughout the life course (e.g., Umberson, 1992).
Furthermore, since the quality of experience in a role is more important to health than role occupancy per se (Barnett & Hyde, 2001), parental satisfaction, conceptualized as “an individual social-psychological construct that taps individual feelings of satisfaction with one’s relationships with one’s children” (Rogers & White, 1998, p. 297), becomes particularly relevant to older parents’ health and well-being. According to Sabatelli and Waldron (1995, p. 975), the parent–adult child interactions and “parents’ satisfaction with their child, children, or stepchildren, or parents’ perceptions of the burdens and rewards derived from being a parent” should be the focal measurement of parenthood.
The direct evidence in the literature on the relationship between parental dissatisfaction and health and well-being in later life, however, is limited to two U.S. studies that examine the same outcome using the same measurement. The older study, conducted by Umberson (1992), found that parentally dissatisfied individuals had elevated levels of psychological distress (measured by an 11-item version of the Center for Epidemiological Studies Depression Scale), using cross-sectional data from a 1986 U.S. national survey of parents of offspring aged 16 years and older. The more recent study (Reczek & Zhang, 2016) reached the same conclusion, analyzing longitudinal data from the first four waves of the Americans’ Changing Lives panel study (1986-2001).
Moreover, only a handful of studies investigated the impact of strained and conflicted parent–adult child relationships on health and well-being in old age. Among them are four U.S. studies (Koropeckyj-Cox, 2002; Milkie et al., 2008; Milkie, Norris, & Bierman, 2011; Ward, 2008) consistently showing that poor relationship with adult children was associated with greater depression in older parents. The fifth and the only non-U.S. study was conducted by Zunzunegui, Béland, Sanchez, and Otero (2009) using a random sample of community-dwelling people older than 65 years, living in Madrid, Spain, in 1993, who were followed up for 15 years. Their findings showed that in the fully adjusted model, having a poor relationship with at least one child increased mortality by 30%, whereas elderly persons in this sample who felt their role in their children’s lives was important had a lower mortality risk than those who felt they played a small role.
In sum, the few studies reviewed here, directly or indirectly addressing parental dissatisfaction and health in later life, were all conducted in the Western world and focused mainly on depression as an outcome (except for the Spanish study that examined mortality). There is virtually no research examining whether these results are applicable to other health outcomes or replicable in non-Western cultures, such as China, where the experience of later-life parenthood is arguably quite different.
If parental dissatisfaction affects parental health and well-being in later adulthood, why and how does this occur? Pearlin and colleagues’ stress process model (Pearlin, 1989; Pearlin, Lieberman, Menaghan, & Mullan, 1981), which has been extended to the family level (Milkie et al., 2008), can be drawn on to help speculate the mechanisms through which parental dissatisfaction may harm health and well-being for older parents. According to Pearlin (1983), strains emanated from the enactment of major social roles, such as worker and parent, representing a particular source of chronic stress given the centrality of these roles. In the context of the family, chronic strains could arise from interpersonal conflicts within the parent–adult child role set, as they interact with each other in a continuing relationship throughout their shared life. Such chronic strains erode positive concepts of self, such as self-esteem and mastery, and often manifest in the form of psychological distress that ultimately increases the risk of poor physical health outcomes.
In stressful times, resources are typically drawn on in reaction to stress. Self-esteem and feeling useful, among others, are such psychological resources (Pearlin et al., 1981) that can be used to buffer against the deleterious health and well-being consequences due to exposure to stressors. These positive psychological resources, however, can be depleted eventually by continuing and powerful stressors, as per the resource deterioration model proposed by Ensel and Lin (1991). Therefore, we expect that parental dissatisfaction (a chronic stressor) reduces or weakens self-esteem and decreases a sense of usefulness (a psychological asset), which subsequently results in poor parental health and well-being outcomes.
The impact of psychological resources on health and well-being outcomes has been well corroborated by evidence showing that high levels of positive psychological resources are related to positive health outcomes. For example, higher self-esteem has been linked to good physical health (Orth, Robins, & Widaman, 2012), lower risk of depression (Sowislo & Orth, 2013), and higher levels of satisfaction with life (Zhang & Leung, 2002) across a wide range of age groups. It has also been shown that greater self-esteem prospectively predicts lower risk of having the onset of difficulty in performing activities of daily living among older Chinese adults (Yang & Wen, 2015). Similarly, higher levels of feeling useless have been linked to higher risk of the onset of activities of daily living disability, poorer physical health, and higher risk of mortality in later life (Gruenewald, Karlamangla, Greendale, Singer, & Seeman, 2007; Gruenewald, Karlamangla, Greendale, Singer, & Seeman, 2009; Okamoto & Tanaka, 2004).
In addition, the influence of lower levels of self-esteem or higher levels of feeling useless on health and well-being may be more evident in later life given that self-esteem begins to decrease in old age (e.g., Orth et al., 2015), and older people generally see themselves as less useful than middle-aged individuals (Mutran & Burke, 1979). As such, any disruptions in psychological resources resulting from parental dissatisfaction may be particularly detrimental for parental health and well-being. Likewise, empirically establishing self-esteem and feeling useless as two psychological pathways linking parental satisfaction to health and well-being would inform researchers, practitioners, and policymakers to design and implement more effective interventions (e.g., Gruenewald & Seeman, 2010; Thoits, 2011). It is thus logical and significant to think that self-esteem and feeling useless may underlie the link between parental dissatisfaction and parental health and well-being in later life, which we trace in this study through a Chinese case.
China can be a fruitful setting to examine these associations for several reasons. First, China has the largest older population in the world, with more than 110 million people aged 65 years or older in 2010, and it is projected to have more than 240 million in 2030 and 370 million in 2050, according to projections (United Nations, 2015). Second, family support from adult children remains a primary source of support for the elderly in China, where social welfare and health insurance systems are quite limited and still being developed. Third, traditionally in Chinese culture, filial piety—the virtue of respect for, taking care of, and obeying one’s parents—has shaped the expectations and behaviors of Chinese families for thousands of years as a central value of family life (Ikels, 2004). Under the regulation and guidance of filial piety beliefs, older Chinese adults may have different expectations for the parental role in later life as well as for the interactions with and support from adult children when compared with older adults in other cultural contexts. This is because cultural norms (e.g., definitions of acceptable and unacceptable behaviors) can affect capabilities and subjective role quality by way of affecting role practices (Barnett & Hyde, 2001) and also because social integration and support may be conditioned on cultural context (Thoits, 2011). Hence, it may be particularly detrimental for older Chinese adults if they are dissatisfied with their parental role.
The present study uses data from a sample of older Chinese parents to test whether parental dissatisfaction in later life is associated with parents’ health and well-being and if so whether this link is attributable to lower levels of self-esteem and/or higher levels of feeling uselss. Figure 1 presents the conceptual model that guides our empirical analyses. Specifically, we hypothesize the following:
A conceptual path model of the association among parental dissatisfaction, self-esteem, feeling useless, and health and well-being outcomes.
Method
Data
The data were collected between June and August 2014 employing face-to-face interviews with a sample of 432 older parents residing in Linxi County, a traditionally agricultural county located in the Inner Mongolia Autonomous Region of northern China. Linxi County had a total population of 240,906 as of 2013, of which 75% were agricultural population and 94% were Han Chinese. People from 10 ethnic groups including the Mongols accounted for 6% of Linxi population. Linxi County has been one of the 592 counties labeled “below poverty level” in China since 1992 due to the meager average disposable income of its residents. According to the documents from Linxi County government, 24% of its agricultural population and 28% of its nonagricultural population live below the poverty level as of 2012. The average disposable annual income of its urban and rural residents is ¥18,209 ($2,785) and ¥6,771 ($1,036), respectively, in 2013, significantly lower than the national average of ¥26,955 ($4,123) and ¥8,896 ($1,361), respectively. Data collection conducted from administrative regions at this level and of comparable socioeconomic standing is very rare.
The sample was drawn from 45 neighborhoods within seven community centers of the two subdistricts of the county seat and a township (the equivalent of a subdistrict). The selection criteria included participants who were, at the time of the survey, 60 to 79 years old, apparently cognitively capable of answering questions, from different households (if a couple in the same household were both qualified, we only interviewed one of them), and who had at least one living child. The project received approval from the University of Utah’s Institutional Review Board.
Procedures
The source of the sample was the electronic resident roster kept in the computer system of each community center, which records detailed demographic information of all household members in each household within all neighborhoods under its governance. At each participating community center, a community staff contacted eligible respondents and scheduled the interviews for those who were willing to participate. Interviews were conducted mostly at community centers, without the presence of persons other than the respondent and the interviewer, by the first author and three trained interviewers. Informed consent was obtained from each participant prior to the start of an interview. The duration of each interview varied from 1.5 hours to 2.5 hours. Participants received ¥50 ($7.60) on completion of the interview. Only a small number of missing values (<4% for all the questions) were found in the data cleaning process. These missing values were imputed by reviewing the completed instruments and interviewers’ notes first, and then if necessary simple imputation procedures, such as using sample mode and mean to substitute for the missing values, were employed.
Of the 464 eligible respondents contacted, 432 completed the face-to-face interview, yielding a response rate of 93%. The high response rate is largely attributable to the study being conducted with strong collaboration and support from local governing subdistricts and community centers. Being contacted by and interviewed in the community center greatly enhanced the credibility of the survey and therefore promoted awareness and involvement among local residents.
It is worth noting that although we employed a convenience sampling method to reach participants, the sex and education composition of the sample is roughly comparable to that of the national level. According to the 2010 Census (National Bureau of Statistics, 2012, Forms 3-1b and 4-1b), of Chinese aged 60 to 79 years living in townships, 50.54% were female (52.19% in Inner Mongolia) and 17.12% had no formal education compared with 55.32% and 20.83% in this sample, respectively.
Measures
Dependent Variables
We examined four dependent variables in this study. Physical health was assessed using a single-item measure asking respondents, “How do you rate your health on a 5-point scale ranging from 1 (excellent) to 5 (poor) these days?” The validity of this global single-item indicator in independently predicting morbidity and mortality has been well established (e.g., Manora, Matthewsb, & Powerb, 2001; Schnittker & Bacak, 2014). We collapsed the five response options into a dichotomous response (1 = fair or poor; 0 = excellent, very good, or good) to deal with its highly negatively skewed distribution. Mental health was tapped with a single question that asks, “How do you rate your overall mental health on a 5-point scale ranging from 1 (excellent) to 5 (poor) these days?” This self-rated single-item measure has been increasingly used as a stand-alone indicator of mental health in health research (Ahmad, Jhajj, Stewart, Burghardt, & Bierman, 2014). As a global indicator, it has been reported to be significantly associated with psychological symptoms and mental disorders (e.g., Fleishman & Zuvekas, 2007). Like physical health, responses to this question were dichotomized into two options (1 = fair or poor; 0 = excellent, very good, or good) to deal with its highly negatively skewed distribution.
Depression was screened using a five-item version of the Geriatric Depression Scale (GDS-5) that asks respondents to answer “yes” or “no” to five questions (see Table A in the appendix). The maximum point total is 5. Respondents with a total score of 0 or 1 are considered “normal,” while those who scored 2 or higher are categorized as “depressed” (α = .67). GDS-5 was shown as effective as the 15-item GDS for screening of depression in older adults (e.g., Nguyen, Inderjeeth, Tang, Barnabas, & Merriam, 2006) yet avoiding response fatigue that was encountered while using the long and comprehensive form of the GDS assessments. Life satisfaction was measured by the widely used Satisfaction With Life Scale (Diener, Emmons, Larsen, & Griffin, 1985), rated on a 7-point scale of 1 (strongly disagree) to 7 (strongly agree) for each item (see Table B in the appendix). The points are aggregated across items with higher scores representing higher life satisfaction (α = .81).
Key Independent Variable
Parental dissatisfaction is the key independent variable based on a question used in previous research (e.g., Mitchell, 2010; Reczek & Zhang, 2016). Before asking this question, interviewers read the following sentences to each interviewee: “Next, we’ll move into the Relationship and Exchange With Children section. Questions in this section are to ask your relationship with your children.” Then, the interviewers paused for a second and asked the first section question: “All in all, on a scale of 1 to 6 with 1 being not at all satisfied and 6 being extremely satisfied, how satisfied are you with being a parent?”
Responses to this question were highly skewed, with the majority of responses falling into category of very or extremely satisfied (n = 280, 64.81%) and the rest containing less satisfactory options such as not at all satisfied to somewhat satisfied. Subject to the social desirability bias, people tend to report what is socially acceptable or expected rather than their real sentiments. In addition, dissonance theory (Secord & Backman, 1974) argues that parents report high satisfaction in the parental role despite the presence of deleterious relationships with children, responding to an attitude adjustment consistent with their earlier decision to have children. As such, we dichotomized the measure of parental dissatisfaction into very/extremely satisfied (5 and 6) = 0 and somewhat dissatisfied (1-4) = 1 to deal with its highly skewed distribution.
Mediating Variables
Self-esteem was assessed with eight items from Rosenberg Self-Esteem Scale (Rosenberg, 1979) (see Table C in the appendix); a frequently used and well-validated measure of global self-esteem (Sowislo & Orth, 2013). Responses were measured using a 4-point scale ranging from 1 (strongly agree) to 4 (strongly disagree). Five items were reverse-coded before aggregation to make the higher the score the higher the level of self-esteem (α = .80). Feeling useless was assessed by a single probe, “Do you feel the older you get, the more useless you are?” Response options range from 1 (never) to 5 (always), with intermediate labels to denote intermediate levels of feeling useless. To be consistent with the original Chinese wording of this question, we did not reverse the scores, though. A higher score thus represents a higher level of feeling useless.
Three sociodemographic variables were controlled, including age (in number of years), gender (1 = female and 0 = male), and financial hardship (1 = having difficulty paying monthly bills and 0 = no).
Analysis
We performed logistic regression modeling for physical health, mental health, and depression while ordinary least squares linear regression analysis for life satisfaction. For each outcome, Model 1 examined the main effect of parental dissatisfaction. Model 2 added self-esteem (Mediator 1) to Model 1 to test whether the link would be explained by parental differences in levels of self-esteem. Model 3 added feeling useless (Mediator 2) to Model 1 to test whether the relationship would be explained by parental differences in levels of feeling useless. Model 4 added both self-esteem and feeling useless to Model 1 to explore whether the explanatory power of each mediator would coexist. Covariates were controlled for in each model. All analyses at this stage were performed using Stata/MP 13.1.
In addition, mediation analyses were conducted. For the three binary outcomes (i.e., physical health, mental health, and depression), coefficients across logit models fitted to the same sample were compared using the Stata command khb as recommended by Breen, Karlson, and Holm (2018), which controls for the rescaling or attenuation bias that arises in cross-model comparisons in nonlinear models (Kohler, Karlson, & Holm, 2011). The analysis was structured in three steps. First, we decomposed the effect of parental dissatisfaction on the three binary outcomes using self-esteem and feeling useless, respectively (Figure 1, Paths a and b). Second, we added both self-esteem and feeling useless to the decomposition and evaluated the mediating effect of both mediators (Figure 1, Path c) simultaneously. Third, we added three covariates—age, gender, and financial hardship—to the decomposition to control for possibly confounding variables. To assess whether medication is statistically significant, the test statistic developed in Karlson, Holm, and Breen (2012) was used to obtain the value of Z scores.
For the nonbinary outcome of life satisfaction, mediation analysis was performed employing the Hayes PROCESS macro (Hayes, 2013) in IBM SPSS Statistics 24 via the following three steps. First, self-esteem was analyzed using simple mediation analysis to determine whether the indirect effect was significant (Figure 1, Path a). Second, feeling useless was analyzed going through the same procedure (Figure 1, Path b). Third, both mediators were retained in the multiple mediation models to simultaneously examine whether any individual variable still significantly mediated the observed association while also evaluating the other mediator (Figure 1, Path c). We reported bootstrap estimates based on 10,000 bootstrap samples because bootstrap confidence intervals “yield inferences that are more likely to be accurate than when the normal theory approach is used” (Hayes, 2013, p. 105). The 95% bias-corrected (BC) confidence intervals (CI) were used to infer significance: Significant mediation effects are supported when the 95% BC CI for the point estimate does not include zero (Hayes, 2013).
Results
Respondents’ Characteristics
The sample is composed of 432 older people with a mean age of 66.24 years (range = 60-79 years; SD =5.00). The majority of the respondents are women (55.32%), are Han Chinese (96%), have experienced financial hardship (68.98%) in terms of having difficulty paying monthly bills in the past year, and report having poor physical health (63.89%). Fewer than half of the sample reported being dissatisfied as a parent (35.19%), having poor mental health (47.92%), or being depressed (34.95%). The mean score of life satisfaction for the participants is 26.79 (range = 8-35; SD=4.93). With regard to self-esteem and feeling useless, the sample has a mean score of 22.38 (range = 14-32; SD = 2.78) for the former and 2.58 (range = 1-5; SD = 1.23) for the latter.
Bivariate correlations of study measures indicated that all correlation coefficients are less than .55, and the highest correlation is observed between self-esteem and depression (r = .54, p < .001). Variance inflation factors diagnostics (ranging from 1.06 to 1.33) did not reveal alarming multicollinearity.
Parental Dissatisfaction, Self-Esteem, Feeling Useless, and Health and Well-Being Outcomes
Tables 1 to 4 display the results from logistic and ordinary least squares regression testing the relationship between parental dissatisfaction, two mediators, and each of the four outcomes, net of age, gender, and financial hardship. Results of Models 1 reveal that parentally dissatisfied older adults experienced worse health and well-being outcomes compared with those who reported being a satisfied parent. Models 2 present that, in general, higher levels of self-esteem are linked to lower possibility of having poor physical health, mental health, and depression, and to higher levels of life satisfaction. Models 3 show that higher levels of feeling useless are associated with higher likelihood of having poor physical health, mental health, being depressed and with lower levels of life satisfaction. Models 4 present the full models where the key independent variable, the two mediators, and covariates are all included. Results show that the two mediators together partially mediate each parental dissatisfaction–outcome link, respectively.
Odds Ratios From Logistic Regression of Ill Physical Health (N = 432).
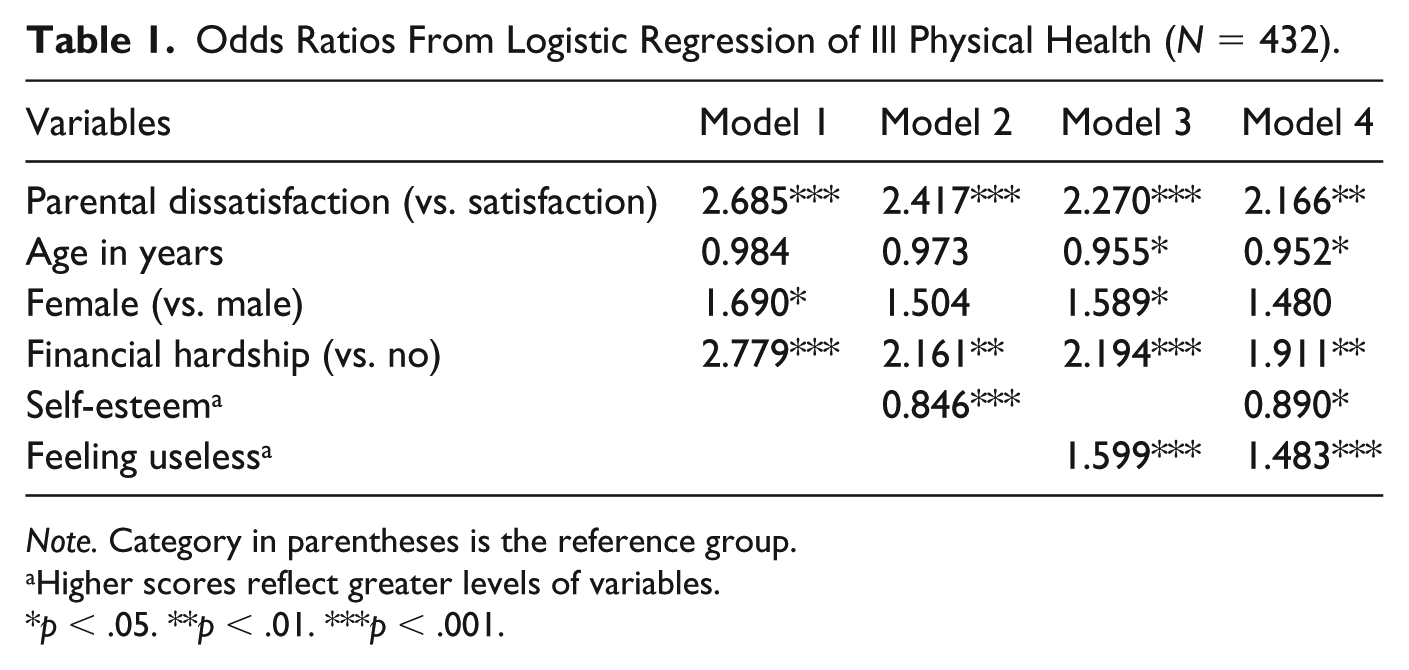
Note. Category in parentheses is the reference group.
Higher scores reflect greater levels of variables.
p < .05. **p < .01. ***p < .001.
Odds Ratios From Logistic Regression of Ill Mental Health (N = 432).
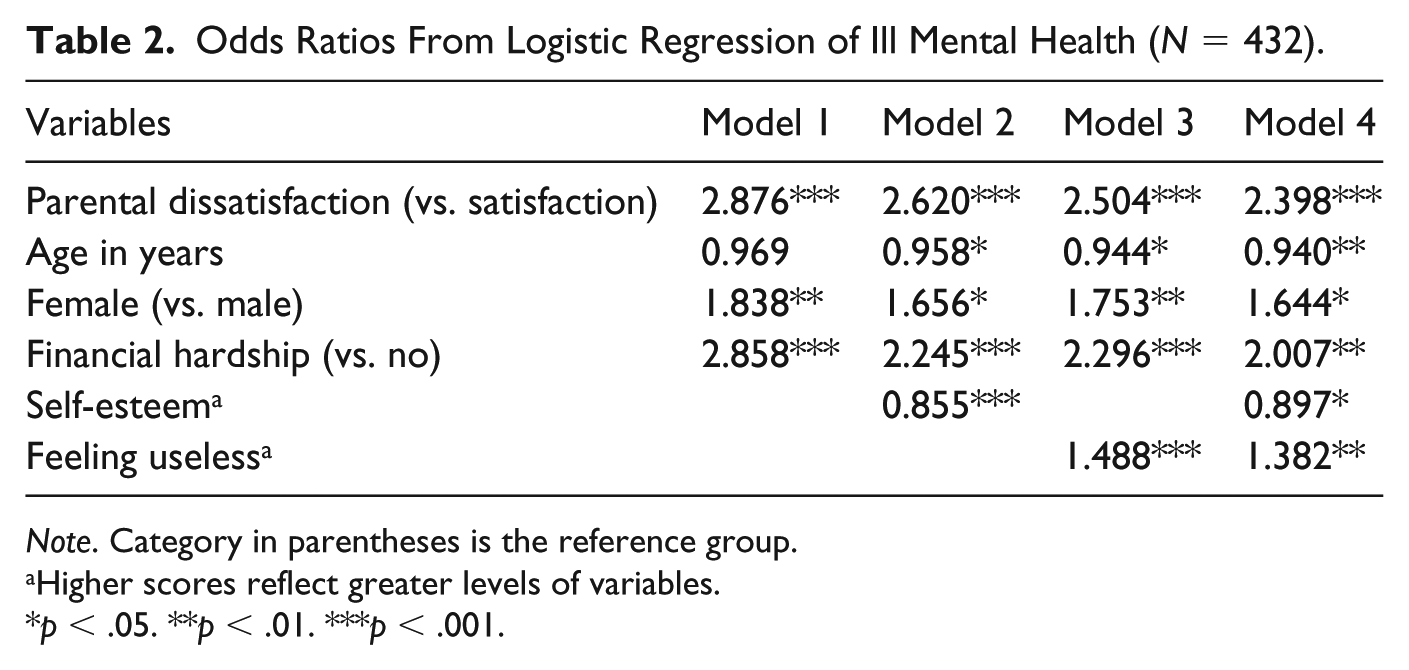
Note. Category in parentheses is the reference group.
Higher scores reflect greater levels of variables.
p < .05. **p < .01. ***p < .001.
Odds Ratios From Logistic Regression of Depression (N = 432).
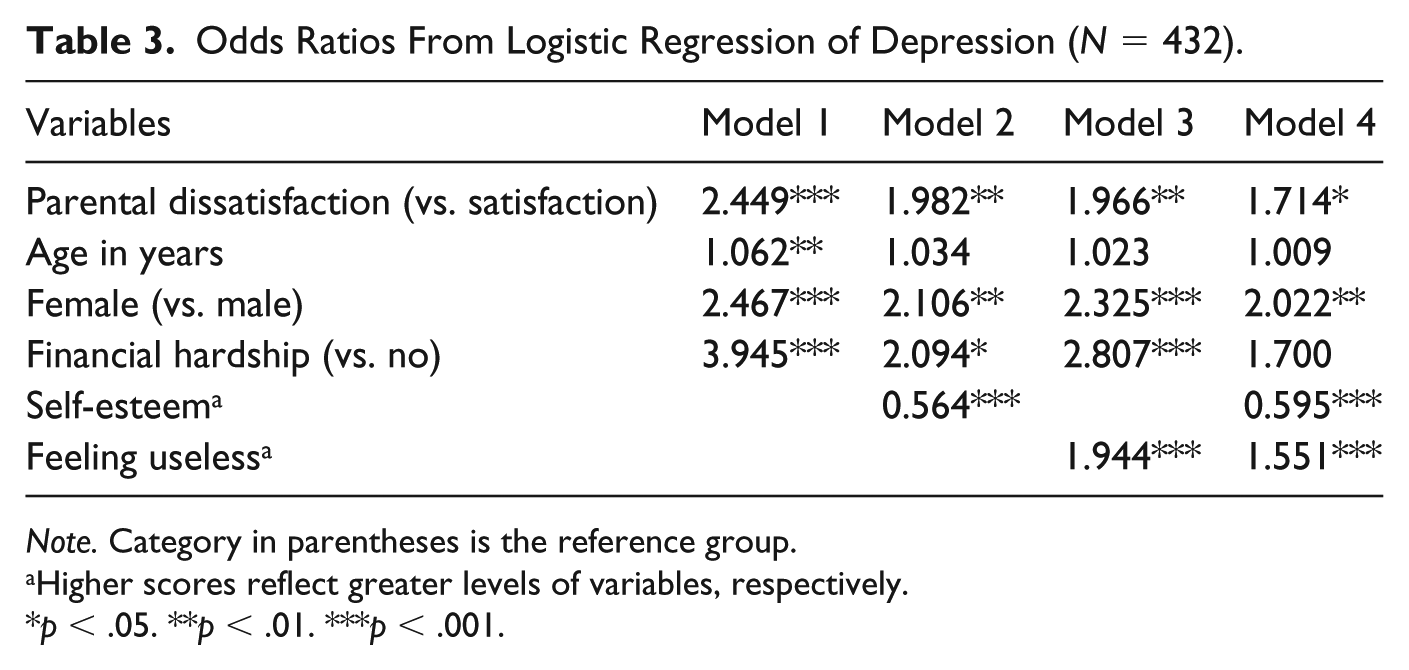
Note. Category in parentheses is the reference group.
Higher scores reflect greater levels of variables, respectively.
p < .05. **p < .01. ***p < .001.
Coefficients From OLS Regression of Life Satisfaction (N = 432).
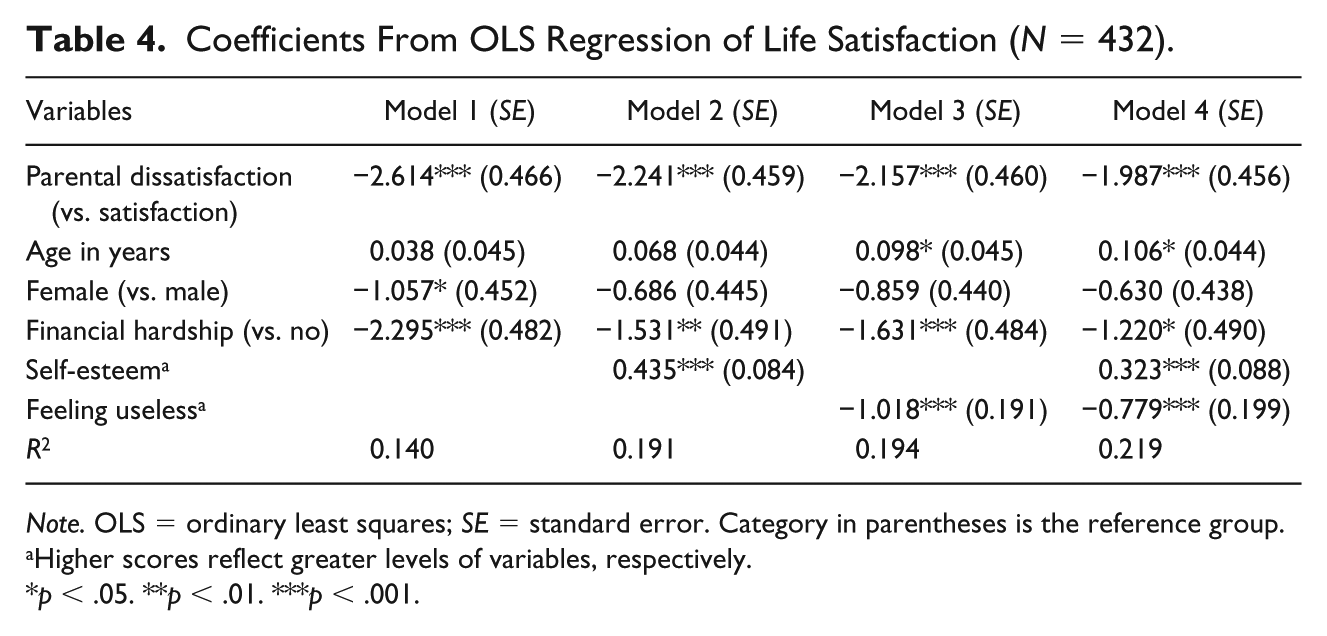
Note. OLS = ordinary least squares; SE = standard error. Category in parentheses is the reference group.
Higher scores reflect greater levels of variables, respectively.
p < .05. **p < .01. ***p < .001.
Evidence of Mediation: Self-Esteem and Feeling Useless as Mediators
Tables 5 and 6 report the results of a decomposition of parental dissatisfaction on each of the three binary outcomes (i.e., physical health, mental health, and depression), with self-esteem and feeling useless serving as the mediator, respectively. The test statistic of Z scores indicates that all effects are statistically significant (Karlson et al., 2012). In Table 5, take the example of the effect of parental dissatisfaction on physical health with self-esteem being the mediator, the total effect of 1.107 was decomposed into a direct part, 0.897, and an indirect part, 0.211. In Table 6, for instance, the total effect of 1.146 for parental dissatisfaction on mental health with feeling useless being the mediator was decomposed into a direct part, 0.950, and an indirect part, 0.196.
Decomposition of Total Effect of Parental Dissatisfaction on Ill Physical Health, Ill Mental Health, and Depression Into Direct Effect and Indirect Effect via Self-Esteem(N = 432).

Decomposition of Total Effect of Parental Dissatisfaction on Ill Physical Health, Ill Mental Health, and Depression Into Direct Effect and Indirect Effect via Feeling Useless (N = 432).
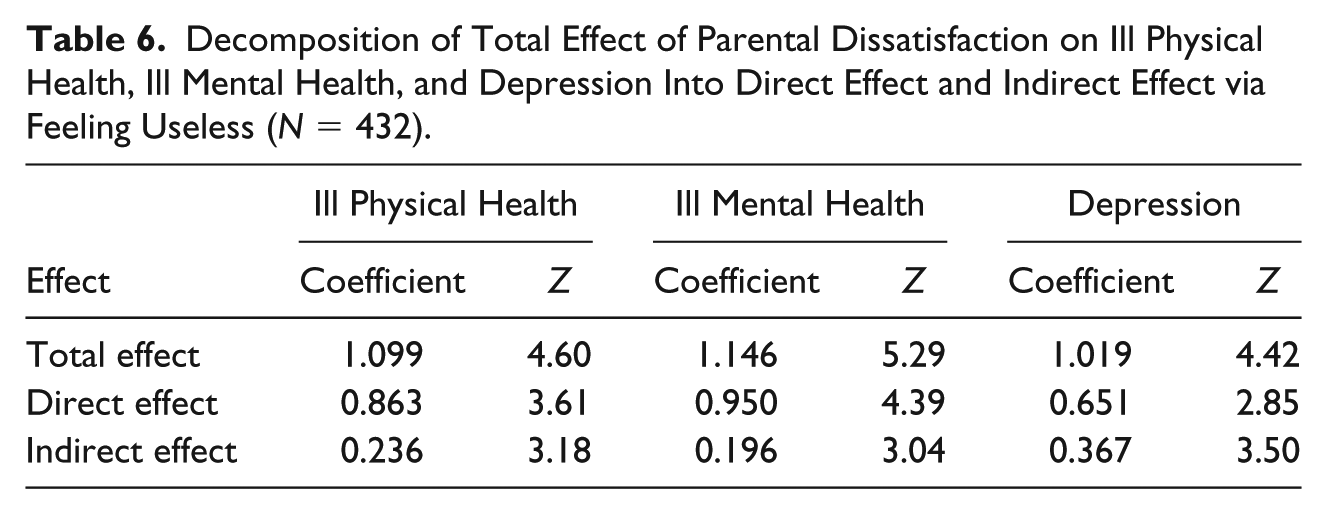
Table 7 shows the results of a decomposition of parental dissatisfaction on each of the three binary outcomes, with self-esteem and feeling useless as mediators while holding constant three covariates’ possible influence on the results. The indirect effect due to both self-esteem and feeling useless are broken down into its respective components. The effects are still statistically significant, suggesting that the results are unaffected by the effects of the covariates. However, it seems that feeling useless has a stronger mediating effect than self-esteem for physical health and mental health. In contrast, self-esteem exhibits a larger mediating effect than feeling useless for the effect of parental dissatisfaction on depression.
Decomposition of Total Effect of Parental Dissatisfaction on Ill Physical Health, Ill Mental Health, and Depression Into Direct Effect and Indirect Effect via Self-Esteem and Feeling Useless(N = 432).

Note. All models are controlled for age, gender, and financial hardship.
Table 8 presents the results of mediation analyses for the effect of parental dissatisfaction on the nonbinary outcome life satisfaction through self-esteem and feeling useless, individually and simultaneously. Since none of the 95% BC CI reported for the indirect effects includes zero, the findings are supportive of mediation by self-esteem and feeling useless independently and jointly on the relationship between parental dissatisfaction and life satisfaction. For instance, simple mediation analysis using PROCESS macro shows that the indirect effect of parental dissatisfaction on life satisfaction via self-esteem is significant. Likewise, results for multiple mediation analysis are displayed in Figure1, Path c of Table 8, showing that the indirect effect of parental dissatisfaction on life satisfaction via self-esteem and feeling useless is significant.
Mediation Effect of Parental Dissatisfaction on Life Satisfaction via Self-Esteem and Feeling Useless, Individually and Simultaneously (10,000 Bootstrap Samples).
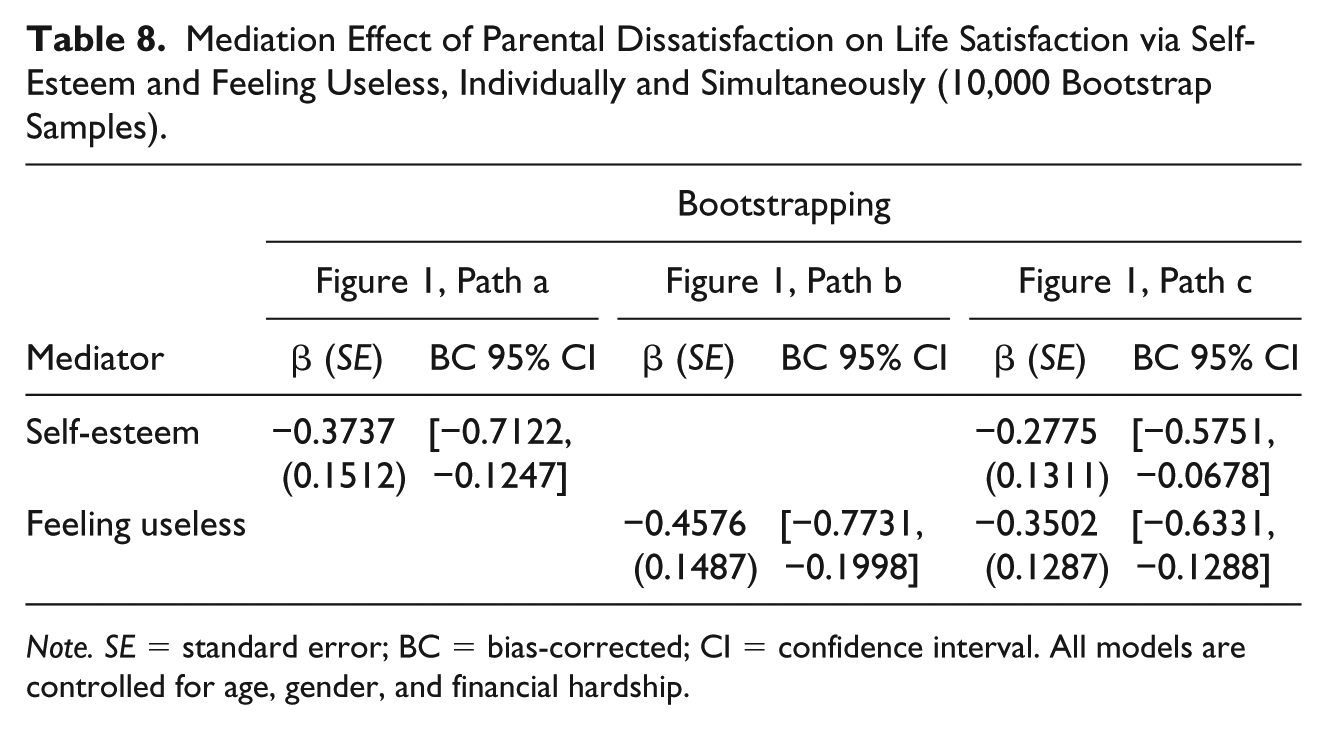
Note. SE = standard error; BC = bias-corrected; CI = confidence interval. All models are controlled for age, gender, and financial hardship.
Discussion
Using a sample of 432 older Chinese parents aged 60 to 79 years, the current study examines whether parental dissatisfaction is associated with multiple health and well-being outcomes and explores the role of two psychological constructs—self-esteem and feeling useless—in explaining these links. Overall, our results suggest that parental dissatisfaction is a significant risk factor for poor health and well-being, supporting our first hypothesis. Consistent with our second hypothesis, self-esteem and feeling useless are found to serve as not only individual pathways but also parallel mechanisms responsible for the association between parental dissatisfaction and the four outcomes. Results regarding depression are consistent with the two U.S. studies (Reczek & Zhang, 2016; Umberson, 1992), confirming that parental dissatisfaction is significantly linked to later life parental depression across cultural contexts. That said, future research is needed to test the effect of parental dissatisfaction on physical health, mental health, and life satisfaction in other cultures. Findings also indicate that the mediating effects by both mediators vary on different outcomes, with feeling useless exercising a stronger effect on physical health and mental health while self-esteem exhibiting a larger effect on depression. These results echo research that shows self-esteem is a risk factor for depression at all phases of the adult life span (e.g., Orth, Robins, Trzesniewski, Maes, & Schmitt, 2009) and studies that reveal the linkage between feeling useless and physical health and mortality (e.g., Gruenewald et al., 2009), respectively.
These findings lend support for the resource deterioration model within the stress process framework (Ensel & Lin, 1991). Parental dissatisfaction as a chronic stressor has a negative impact on self-esteem and feeling useful, indicating that positive resources deteriorate when older adults are dissatisfied with their parental role. These diminished resources are the mechanisms through which stressors exert their detrimental effects on health and well-being. That said, the detrimental effect is not eliminated altogether. A portion of the parental dissatisfaction effect on health and well-being remains net of these mediating effects suggesting either a direct effect of parental dissatisfaction on health and well-being exits or some other important mediating factors omitted from the analysis.
Several limitations in this study should be considered. First, the measure of parental dissatisfaction is based on a single item, whereas a multi-item scale including other questions on parental satisfaction should be considered in future studies. That said, evidence from Western studies has shown that single item of positive affect measures such as happiness or satisfaction are often sufficient (e.g., Scarpello & Campbell, 1983; Wanous, Reichers, & Hudy, 1997). Although little is known as to what degree the single item of parental satisfaction is sufficient to capture the construct in the Chinese settings, a previous study by the authors (Yang & Wen, 2016) found that this single item of parental dissatisfaction was significantly associated with several conceputally relevant constructs such as getting along with offspring; offspring meeting parental expectations in terms of providing emotional, practical, and financial support; and offspring being filial, supporting this single item’s construct validity. Second, no causal inferences can be made due to the cross-sectional nature of the survey design, and reverse causality and the bidirectionality of the relationships are also likely. Parental dissatisfaction could be an outcome of life stressors such as poor physical and mental health. It is also possible that the relationship between parental dissatisfaction and psychological mechanisms is reciprocal. Future research using longitudinal data is warranted to further examine these research questions, but without randomized trials, causality will remain elusive. Third, as previously mentioned, although our sample is similar to Chinese aged 60 to 79 years living in townships in terms of sex and education composition revealed in the 2010 Census, future studies with nationally representative data are still needed to test whether the findings would be replicated for the purpose of generalizability. Finally, neither age nor gender difference is detected in this study in the parental dissatisfaction and health and well-being linkages. Given the importance of age and gender differences in later life outcomes, future research should examine this possibility with other data.
Despite these limitations, the current study contributes to the literature in two important ways. First, this study reports that parental dissatisfaction is significantly linked to four health and well-being outcomes among older Chinese parents, providing novel evidence to fill in a gap in the health and aging literature. Another major contribution of this study is the demonstration of two individual pathways and the simultaneous coexistence of the two psychological mechanisms linking parental dissatisfaction to poor health and well-being outcomes among older adults, addressing important questions pointed out in earlier and recent work (Reczek & Zhang, 2016; Sabatelli & Waldron, 1995; Thoits, 2011; Uchino et al., 2012). Nonetheless, our findings have important implications for intervention. Evidence has shown that meaningful and appropriate social roles interventions (e.g., Retired Senior Volunteers, Park Maintenance Corp, Foster Grandparent Program, Older Mentors for Newer Workers) conducted in developed countries are found to be effective in improving health and well-being for older people who carry out the role (Heaven et al., 2013). Older adults in Mainland China, where volunteering opportunities are rare, might also benefit from such interventions by taking some aforementioned modifiable social roles.
In conclusion, this study adds to our understanding of the parental role and parental health and well-being dynamics in later life by identifying the associations between parental dissatisfaction and multiple parental health and well-being outcomes, and by providing evidence of the existence of individual and multiple psychological mechanisms underlying each individual association and to explain why this is so. Our findings also suggest that self-esteem and social role intervention projects could be valuable in screening and targeting parentally dissatisfied older adults to enhance their health and well-being.
Footnotes
Appendix
Eight Items From the Self-Esteem Scale.

| At times, I think I am no good at all. I feel that I have a number of good qualities. I am able to do things as well as most other people. I feel I do not have much to be proud of. I feel that I’m a person of worth, at least on an equal plane with others. I wish I could have more respect for myself. All in all, I am inclined to feel that I am a failure. I take a positive attitude toward myself. |
Source. Rosenbery (1965).
Acknowledgements
We are grateful to Shujun Tian, Xia Sun, Wen Li, and Yang Yang for their valuable assistance with data collection. We thank Michael F. Timberlake and Sonia L. Salari for their helpful comments on the original draft. We also wish to acknowledge the careful and constructive review by the annoymous reviewer.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data collection was supported by the University of Utah Center on Aging 2014 Pilot Grant.