
Abstract
Due to linguistic and cultural adjustments to a new country, first-generation immigrant’s caregiving challenges have been well-documented. However, little is known of U.S.-born, U.S.-educated, English-speaking later-generation caregivers’ (2nd, 2.5, and 3rd-generation) attitudes and needs regarding caregiving. Given this context, we interviewed 40 later-generation Chinese-American caregivers in Seattle and Houston. Caregivers had a mean age of 59 years, were married, college-educated, and working females with children. The later the caregiver’s generation, the higher their acculturation, but their sense of filial responsibility remained high across generations. While Seattle caregivers wish to live in a high-quality, long-term care facility, Houston caregivers prefer to live with their adult children for their future care. Findings emphasize the importance of understanding the caregivers’ ethnically and generationally specific caregiving attitudes and preferences for geographically specific services. Collaborating with existing local organizations, it is critical to ensure that the provision of services meets local Chinese-American caregivers’ needs and preferences.
Introduction
Due to an increase in the aging population internationally and in the ease of world travel, many Western countries, including the United States (U.S.), have been receiving older immigrant populations (Lin et al., 2015). One of the major reasons for such immigration among older adults is a reliance on family members for care. Consequently, there have been a burgeoning number of caregiver studies among diverse racial/ethnic and cultural groups (Connell & Gibson, 1997; Dilworth-Anderson et al., 2002). The literature reviews on Asian caregivers in the U.S. have been published for decades now, and they consistently suggest both commonalities and differences among disparate populations by geographic location (Kong, 2007; Miyawaki, 2015; Mokuau & Tomioka, 2010; Sun et al., 2012).
First-generation immigrants and their caregivers tend to face caregiving challenges due to linguistic barriers, and differences in health care systems and caregiving expectations between their home and host countries (Angel et al., 2014; Crist & Speaks, 2011; Kong et al., 2010). You may face different filial practices, especially if you come from a collectivist culture such as many Asian and Hispanic countries to an individualist culture such as the U.S. (Anngela-Cole & Hilton, 2009; Funk et al., 2012; Hsueh et al., 2008, ). As such, the caregiving literature to date has focused primarily on 1st-generation immigrant caregivers and their caregiving challenges, and there is much less information about the caregiving attitudes and needs of U.S.-born, U.S.-educated, English-speaking 2nd-, 2.5- and 3rd-generation caregivers. Given the fact that many Asian caregivers actually belong to these later generations, it is essential to understand their caregiving views and preferences (Anngela-Cole & Hilton, 2009; Kobayashi & Funk, 2010) so that we can better serve their needs. These later-generation Asian caregivers have grown up as Americans and have assimilated to American individualistic culture, and, thus, the level of filial responsibility may differ from that of 1st-generation counterparts (Funk et al., 2013; Hsueh et al., 2008). The purpose of the study was to explore the caregiving attitudes and needs of later-generation Chinese-American caregivers. Two research questions guided this study: (a) Do the levels of acculturation and filial responsibility among later-generation Chinese-American caregivers differ across generations and by geographic locations? and (b) Do the caregiver’s attitudes and needs differ among later-generation Chinese-American caregivers across generations and by geographic locations? Chinese-Americans were selected as an exploratory study sample because they are the largest Asian sub-ethnic group with multiple generations living in the U.S. (Hoeffel et al., 2012). We used a mixed-method approach because we first needed to find out if there are differences in their acculturation and filial responsibility levels across different generations (quantitatively measured by survey), and we explored any potential impacts on their caregiving attitudes and needs by their acculturation and filial responsibility levels in depth (qualitatively explored by interview). Then we will be able to provide the necessary services that are beneficial and unique to the later generations of caregivers.
Literature Review
Confucianism, originating in China, teaches family members their social role and obligation, lifetime interdependence, and loyalty, and emphasizes the maintenance of family harmony (Weng & Nguyen, 2011). Filial responsibility has been strong in Chinese culture, and, as such, the filial responsibility of respect and obedience to elders is taught at a young age and its practice is expected. In traditional Chinese culture, adult children are expected to care for their aging parents, contribute financially, and provide emotional support (Weng & Nguyen, 2011).
Jones and colleagues (2002) and Jones et al. (2003) found that the vast majority of these caregivers immigrated to the U.S. for a better life compared to their home country. After settling down themselves, many invited their parents to the U.S. to perform their caregiving as their filial responsibility, especially after the 1965 Immigration Act, which allowed new Chinese immigration based on its family reunification emphasis (Wong, 2006). A challenge of this is that their caregiving cultural values were nurtured on the conditions and expectations of their home country, however, the practice was implemented in the U.S.: a transition between Asian and Western cultures. In some cases, caregivers had to face personal sacrifices such as quitting their paid jobs in order to meet their caregiving needs. But they are willing to place their commitment to their parents’ care as the highest priority in their lives (Jones et al., 2003). Tang (2011) found that despite these challenges, caregivers had better health and more positive feelings toward caregiving when they were involved in caregiving roles because they are fulfilling their filial responsibilities. Holland et al. (2010) found that caregivers were less depressed and had greater self-efficacy with more positive caregiving experience and that they had the ability to respond well to challenging behaviors of care recipients. Caregivers felt psychological rewards (Zhan, 2004) or satisfying psychological well-being (Jones et al., 2001) by caring for their parents and performing their filial piety, and, thus, could cope with their stressful situations.
Levy and colleagues (2000) reported somewhat different dimensions of caregiver experiences: the more interaction caregivers have, the higher the caregiver burden, because they needed to keep their traditional caregiving practices and values and their family ties salient in the U.S., but they couldn’t have as big social networks as they could have had in their home country. These caregivers are 1st-generation immigrant caregivers who have been educated, have developed the filial values of their country of origin, and have brought their parents/parents-in-law to the U.S. in their late lives (Miyawaki, 2015). But it has been more than 50 years since these 1st-generation immigrants have settled in the U.S. and their 2nd-, 2.5-, and 3rd-generations are facing their caregiving issues for their own aging parents. However, we do not have knowledge about the experience of later-generation Chinese-American caregivers.
To fill this knowledge gap, I aimed to explore the later-generation Chinese-American’s caregiving attitudes and needs based on their acculturation and filial responsibility levels. Gordon’s assimilation theory (1964) was used as the theoretical framework. Gordon’s theory states that the longer the immigrants reside in the host society, the greater they assimilate to the host society, and, thus, the immigrant and majority groups share more similarities. He proposed seven stages in this theory, and this study focused on stage one: cultural/behavioral assimilation (acculturation). These elements were also compared in two different geographic locations. Two metropolitan cities, Seattle, Washington, and Houston, Texas, were chosen because Chinese-Americans are the largest Asian sub-ethnic group in Seattle and the third largest in Houston (U.S. Census Bureau, 2016). The numbers of Chinese population are similar in both cities (Seattle: 30,233; Houston: 34,088), however, their sizes are different (4.5% of Seattle population; 1.5% of Houston), and, thus, their visibilities within the cities may differ (U.S. Census Bureau, 2016). Moreover, Chinese residents in Seattle have over 160 years of immigration history (populated since 1850s) (Chin & Chin, 2013) versus the Houston Chinese-Americans who have a little shy of 50-year history (since 1970s) (Chen & von der Mehden, 1982). Thus, it was anticipated that their acculturation and filial responsibility levels, caregiving attitudes, and needs differ.
Growing racial/ethnic diversity of caregivers is a reality, and their generational differences in caregiving attitudes and needs are expected to differ as well, especially with the intersection of acculturation and filial responsibility. Therefore, it is crucial to explore this issue and the results of this study can contribute to knowledge base within the field of caregiving study as well as provide practice implications for health care providers and senior care industry.
Methods
The purpose of this study was to explore the caregiving attitudes and needs of later-generation Chinese-American caregivers in two U.S. cities accounting for the acculturation and filial responsibility levels based on their immigration history. The study aims were to quantitatively measure the 2nd-, 2.5-, and 3rd-generation Chinese-American caregivers’ acculturation and filial responsibility levels and to qualitatively explore in depth their caregiving attitudes and needs, using a content analysis, and compare them between Seattle and Houston.
Sample, Recruitment, and Data Collection
Inclusion criteria were caregivers who (a) are currently caregivers; (b) are either 2nd-, 2.5- or 3rd-generation immigrants; (c) care for their parent/parent-in-law/aunt/uncle/grand-parent/other relatives; (d) help with Activities of Daily Living (ADLs; e.g., bathing, feeding, and walking) and/or Instrumental Activities of Daily Living (IADLs; e.g., cooking, medication management, and shopping); (e) have cared for longer than six months; and (f) have lived in Seattle or Houston during the caregiving. In this study, first-generation immigrants mean that they were born outside of the U.S. and came to live in the U.S. at a later time of their lives. The 2nd-generation caregivers are defined as those who were either U.S.-born or immigrated to the U.S. prior to age 14 years with both foreign-born parents. 2.5-generation caregivers are U.S.-born and have one U.S.-born and one foreign-born parent. The 3rd-generation caregivers are U.S-born with both U.S.-born parents.
As for recruitment strategies, because in Seattle there are many Chinese-ethnic-specific senior residential facilities/care homes in addition to Chinese churches and community organizations, the Principal Investigator (PI) first approached these organizations. They advertised the study in their email newsletter, and their key personnel introduced the PI to potential participants. Snowball sampling with English/Chinese study fliers were utilized, asking interested individuals to contact the PI by phone or email. Twenty-three potential participants expressed interest, of which 22 were determined to be eligible; however, a final participant count ended with 19 because we were able to obtain enough data by interviewing the first 19 caregivers. The interviews were held at either caregivers’ homes or community centers, were conducted in English, and lasted on average 66 minutes (ranged from 38 to 110 minutes).
In contrast with Seattle, the greater Houston area has only one Pan Asian senior social service agency. The PI contacted the key personnel in this agency and placed both English and Chinese study fliers in the agency. Through this agency, the PI then contacted several Chinese-American churches in the area and hosted a recruitment table on several Sundays. Potential study participants were asked to sign up with their contact information, based on a brief eligibility conversation at the recruitment table. Nineteen potential participants signed up during the recruitment table and nine additional participants were recruited by word of mouth. After eligibility check, 21 caregivers remained eligible. All the interviews were conducted at the participants’ church and were on average 50 minutes (ranged from 31 to 80 minutes).
During the initial contact, participants’ eligibility was verified in person, by phone, or by email. The PI then scheduled an interview at a mutually agreed upon location. Upon a written consent from all participants, each caregiver’s demographic information, and acculturation and filial responsibility surveys were filled out. The PI conducted all the interviews in English, and upon participants’ consent, interviews were digitally recorded. Participants were compensated $20 and $25, given different waves of data collection and funding sources. The study was approved by the institutional review boards of the PI’s universities.
Measures and Data Analysis
Twenty-one multiple choice items of the Suinn-Lew Asian Self-Identity Scale (SL-ASIA) were used to measure the later-generation Chinese-American caregivers’ levels of acculturation (Suinn, 1994). The SL-ASIA, the most frequently used scale (Miller & Speight, 2006), is known to successfully measure the acculturation level of Asians of all ages (Ownbey & Horridge, 1998) (α = .79) (Suinn et al., 1995). It is a self-report scale, and it assesses sample’s language capability, identity, friendship choices, ethnic associations, food preferences, and generation. The acculturation score is an average of the sum of the 21 items and dividing the sum by 21. The score ranges from 1 (low acculturation level) to 5 (high acculturation level).
A 12-item scale, Filial Values Index (FVI), was used to measure the caregivers’ filial values. The FVI consists of three dimensions measuring the levels of filial responsibility (α = .79), care (α = .90) and respect (α = .93) for parents by adult children. Questions to determine the level of filial responsibility are (a) adult children should protect their families’ reputations; (b) taking care of aging parents is part of an adult child’s moral responsibility; (c) we need to take care of our parents because they gave birth to us; and (d) taking care of my aging parents is part of my faith. This scale has been successfully tested with Chinese-American caregivers (Jones et al., 2011). The filial responsibility score is an average of the sum of these statements and divided by four for each caregiver. The scores range from 1 (completely disagree) to 9 (completely agree to question statement).
Interview questions were pilot-tested with one 2nd- and one 3rd-generation caregiver who were not included in the final sample. As a result, some clarifying modifications were made. The final version of the interview guide included 17 questions within five topics: (a) caregiving; (b) culture; (c) acculturation; (d) intervention, program development, and policy changes; and (e) recommendations for future caregivers.
All the recorded interviews were professionally transcribed verbatim. Notes were used to keep track of the PI’s general impressions and participants’ facial/verbal expression. The analysis involved an ongoing process of comparing between and within transcripts and notes. A codebook was developed using a combination of the aforementioned five content categories and sub-categories identified using content analysis (Elo & Kyngäs, 2007; Hsieh & Shannon, 2005). Content analysis was used because we wanted to classify and identify similar themes and meanings from the interviews (Moretti et al., 2011). Content analysis was appropriate for this study because it can be used to examine any kind of communication materials (Abrahamson, 1983), and it identifies and represents explicit or implicit communication (Hsieh & Shannon, 2005). First, five themes from the interview questions were identified and coded. Second, passages with similar content were grouped during axial coding, and subthemes were developed reflecting more situational perspectives, such as a sense of filial responsibility within the cultural values theme. These subthemes included similarities and differences between and within participants and generations, and were repeatedly redefined. To enhance analytic rigor and to reduce interpretation biases (Lincoln & Guba 1985), the PI received written and oral feedback on the interview guide, and the study results from four faculty with expertise in qualitative and caregiving research (for Seattle study), and minimal changes, such as replacing terms, were made to the guide. To promote trustworthiness, a second coder (a senior faculty) performed an independent audit of the transcripts and reviewed all the theme and subtheme codes that the PI recorded; as a result, no changes were made. To validate accuracy of data interpretation, member checking (Turner & Coen, 2008) was also conducted. For the Houston study, all the codings were performed by the PI and PI’s assistant, and we used Atlas.ti version 7 to analyze the data.
Results
Participants’ Characteristics
Table 1 shows the characteristics of Seattle and Houston Chinese-American caregivers. Seattle caregivers (Mean age=61.2 years; age range 49–73 years) were slightly older than Houston caregivers (Mean age=56.5 years; age range 35–72 years). This fact supported that more Houston caregivers have children under 18 years old (76%) compared to their Seattle counterparts (63%). The vast majority were employed and highly educated across generation in both locations.
Characteristics of Chinese-American Caregivers by Generation in Seattle and Houston.
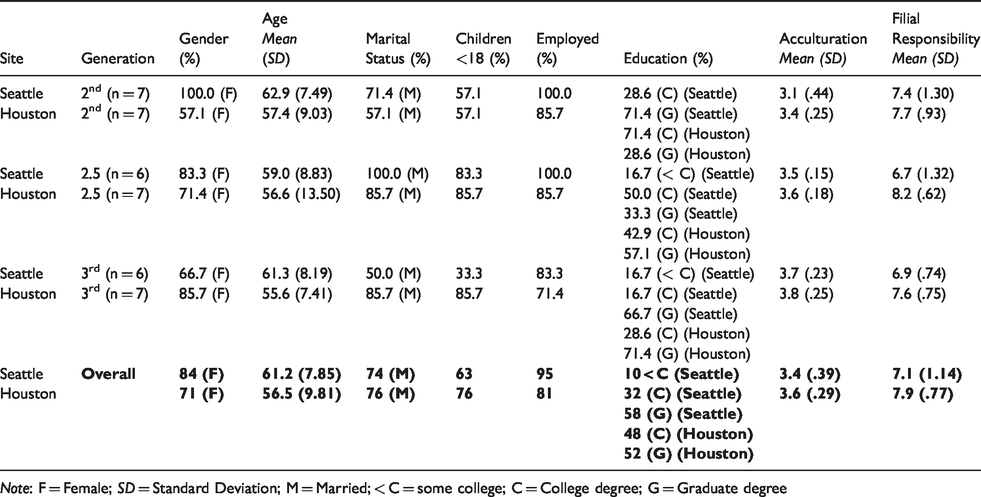
Note: F = Female; SD = Standard Deviation; M = Married; < C = some college; C = College degree; G = Graduate degree
The acculturation scores revealed that the later the caregivers’ generation, the higher the acculturation level for both caregiver groups. For the Seattle sample, a statistically marginal difference between generations was found (p = .068). Multiple comparisons using the Tukey test showed that the 3rd-generation caregivers’ acculturation level was marginally higher than the 2nd-generation counterparts (p = .068). For the Houston sample, there was a statistically significant difference among three generations (p = .0002). Comparisons resulted that both the 2.5- and the 3rd-generation caregivers’ acculturation levels were statistically significantly higher than the 2nd-generation counterparts (p = .022; p = .0002 respectively), but there were no statistically significant differences between the 2.5- and 3rd-generations. In terms of filial responsibility levels, there was not a significant difference between generations for both geographic locations. However, both Seattle and Houston caregivers showed high levels of filial responsibility (Seattle: Mean = 7.1, SD = 1.14; Houston: Mean = 7.9, SD = .77). No statistically significant acculturation difference was found geographically, but a significant filial responsibility difference was found geographically (p = .018), expressing higher responsibility levels among 2.5-generation Houston caregivers (p = .05).
Caregiving Attitudes and Needs
Out of five interview question topics, content analysis identified four themes that stood out from the interviews: caregiving challenges and support systems, cultural values, acculturation issues, and caregivers’ own future care. Considering the line of specific interview questions, theme 1: Caregiving challenges and support systems, can be a byproduct from the questions. However, the rest of the themes, especially theme 4: Caregivers’ own future care, emerged most inductively because as all the caregivers went through question topics, many ended up talking about concerns about their own future care, realizing that their own children (more later generation) may not have the same level of filial responsibility as their level due to the higher level of acculturation to the U.S. lifestyle and U.S. caregiving practices. Table 2 presents the summary of themes and subthemes that were emerged from the analysis.
Themes and Subthemes.

Theme 1: Caregiving challenges and support systems
Caregivers expressed several caregiving challenges, however, rather than physical, emotional aspects of caregiving were the most striking and frequently expressed challenges.
Both Seattle and Houston caregivers rarely used formal outside assistance. Their care recipients were not receptive to bringing in/hiring help: “Parents don’t want to have help because they think they can do it themselves” (2nd-generation daughters, Seattle and Houston; 3rd-generation daughter, Houston); and “Professional caregivers would come to her, but she’d say ‘Go away, I don’t want you’” (2nd-generation daughter, Seattle) or “She [Mother] would have made them [caregivers] mad and they wouldn’t have stayed anyway” (2nd-generation daughter, Houston). Moreover, Houston caregivers had never thought about hiring a professional caregiver or placing their loved ones into an institution. Rather, caregivers preferred to move their loved one into their own homes, “We would move her into our house. We would not put her in [to an institution]” (2.5-generation son, Houston).
Theme 2: Cultural values.
Houston caregivers showed a strong sense of filial responsibility as well, and their sense was emphasized by the Asian/Chinese cultural values such as respect for elders. In Asian families, the parents command so much respect…You still feel a very, very strong Asian culture, Chinese culture that you would respect your parents (2.5-generation son, Houston) I feel like it is somewhat my obligation as well as my duty … and realize that this is a privilege to be able to take care of your most ther. (3rd-generation daughter, Houston)
Theme 3.: Acculturation issues
I think our sibling’s level of responsibility is all about the same, but my mother expects a lot more. So it definitely is a generational (gap): a 1st generation versus 2nd-generational gap. (2nd-generation daughter, Seattle) She [Mother] is an American-born…I think we understand each other better [than if she was foreign-born]…also culture, too because she’s basically an American. (3rd-generation daughter, Houston)
Theme 4: Caregivers’ own future care
Caregivers’ preference for their own future residence was an emerging theme. Many care recipients refused to accept outside help and, therefore, only few caregivers used paid professionals when they were unable to provide care by themselves. In terms of their own care, however, the caregivers would accept in-home caregivers as long as they do their job.
As for institutionalization, all accepted the idea of moving into a long-term care facility in the future, because they did not want to impose their own care upon their children and other relatives. Despite the fact that there are Chinese-specific care homes available locally, Seattle caregivers would choose to live in mainstream facilities because of their acculturation level and linguistic disconnect with the Chinese language: I don’t necessarily would choose [sic] [name of Chinese facility] because the residents speak Chinese. (2nd-generation daughter, Seattle) Because my communication skills aren’t there, so I think there’s a big disconnect there. (3rd-generation nephew, Seattle)
Discussion
This study first examined the levels of acculturation and filial responsibility of later-generation Chinese-American caregivers quantitatively (survey), and followed it up by exploring their caregiving attitudes and needs in relationship to their immigrant generations qualitatively (interview) in two U.S. cities. Quantitative results of the caregiver’s acculturation levels were well supported by the results of the qualitative interviews; however, caregiver’s filial responsibility levels had mixed results because, overall, qualitative interviews revealed a strong sense of caregiver’s filial responsibility level regardless of caregiver’s generation in both cities. The 3rd-generation caregivers showed the highest acculturation level in both cities, which is supported by Gordon’s assimilation theory: the later the immigrant generation, the greater the similarities between the immigrant and majority groups. This progression was expressed in many ways in the interviews, such as generational differences in caregiving patterns and fewer conflicts between 2.5- and 3rd-generation caregivers compared to 2nd-generation counterparts. This appears to be because the parents of 2.5- and 3rd-generation caregivers were already acculturated as the parents themselves are U.S.-born 2nd-generation. However, no statistically significant differences were found in caregivers’ filial responsibility levels across generations regardless of geographic locations. Rather, the scores of all generations were relatively high maintaining a strong sense of filial responsibility despite their higher level of acculturation. This pattern was also expressed in the interviews: caregivers’ caregiving commitment to their loved ones remained high regardless of generations and geographic locations, which was supported by few previous studies on the concept of familism in multiple generations of Asian and Hispanic American caregivers (Miyawaki, 2017; Rudolph et al., 2011). Further, Houston caregivers’ filial responsibility scores were higher compared to Seattle caregivers. This may be because the majority of Houston caregivers were churchgoers, and their Christian beliefs of respecting elders as this sentiment was often expressed in their interviews, may have influenced a higher level of filial responsibility compared to their Seattle counterparts who did not indicate any Christian affiliations during their interviews.
As seen in the themes of the cultural values and acculturation, more 2nd- and 2.5-generation caregivers experienced caregiving conflicts with 1st-generation immigrant parents in caregiving expectations, which is a very similar pattern that has been found in many previous studies among 1st-generation caregiver and care recipient relationships (Dilworth-Anderson et al., 2002). Some 1st-generation parents could not speak English or drive, and thus caregivers’ caregiving duties started during their teens. The 1st-generation parents held higher caregiving expectations than their children’s generation, causing some disconnects between the two generations. In contrast, 3rd-generation caregivers did not have to face the language and driving issues because their parents were U.S.-born English-speakers and drove cars (Miyawaki, 2017). However, this generational difference was not reflected in the caregivers’ decision to use outside help, indicating cultural maintenance and resistance to the idea of institutionalization. When conflicts in their caregiving expectations occurred, regardless of generation, all children obeyed their parents. This hierarchical attitude and its continuity are congruent with Wong’s account (2006) of Chinese people’s maintenance of tradition.
Knowledge of Chinese-American immigrant history is useful to understand these caregiving views. Since the opening of mass immigration in 1965, there has always been a continuous flow of Chinese newcomers and, thus, Chinese-Americans may have a good chance to maintain their home culture influenced by new 1st-generation immigrants (Miyawaki, 2017). This pattern can also be found among Hispanic-American caregivers as they continue to preserve their cultural beliefs and practice (Flores et al., 2009). The vast majority of caregivers in this study did not use institutional care demonstrating ongoing commitment to care. Moreover, nearly all the Houston caregivers expressed their plans of taking their parents into their homes rather than placing them into long-term care facilities; reflecting the traditional cultural caregiving style and their strong sense of filial responsibility. This attitude may be supported by the ethnic retention model of Portes and Zhou’s segmented assimilation theory (1993), retaining ethnic culture while assimilating to mainstream culture.
Previous studies identified current Chinese-American caregivers’ concerns about their own future care (Funk et al., 2011; Hsueh et al, 2008). This is because their U.S.-born children have assimilated to the mainstream culture and acquired beliefs and values that are different from those of current caregivers. As a result, these caregivers may not be able to expect the same level of filial care from their own children. Although later-generation caregivers in this study had not placed their loved ones in institutions, they were open to living in a high quality residential facility in their old age. This attitude points to the different acculturation levels of later-generation Chinese-Americans. However, some Houston caregivers expressed their preference of co-residing with their children as their choice instead. There appears to be more family cohesion among Houston caregivers as their family unites in relation to their residential locations and sharing of caregiving duties.
Implications for Practice and Future Research
The current studies were conducted in Seattle, Washington, and Houston, Texas, where diverse populations with multiple generations co-exist, making it possible to recruit Chinese-American samples. In Seattle, there are well-established Chinese community centers, churches, senior service agencies, in-home caregiver services, and care homes. In Houston, there are a large number of newly arrived Chinese immigrants, but the number of ethnic-specific organizations is very limited. The reason of the differences could be the Seattle Chinese-American’s over 160 year-long immigration history and their visibility in the Seattle community (4.5%) versus 50 years of Houston Chinese-American history and their visibility (1.5%) despite the similar numbers of Chinese-Americans in each city. Thus, the needs of Houston Chinese-Americans have not been studied as much as those in Seattle. Because new Chinese immigrants need ethnic-specific traditional care with linguistic assistance, it is important for these ethnic-specific agencies to provide services to meet the newcomers’ needs. For Houston, there is an urgent need to build ethnic-specific facilities because caregivers expressed their wishes for long-term care facilities with an Asian environment for their loved ones. However, in order for these agencies to maintain their businesses, they also need to provide services that reflect the needs of later-generation Chinese-Americans. Seattle’s later-generation caregivers feel disconnected from Chinese ethnic-specific facilities because their activities are offered in Chinese language only. While providing linguistically/culturally sensitive services to newcomers, these agencies must also address the needs of bicultural, more acculturated Chinese-Americans. For example, the wish for Chinese/Asian food at the mainstream long-term care facilities was mentioned among both Seattle and Houston caregivers. Since many later-generation caregivers did not mind moving into long-term care facilities, offering familiar food could be an attraction to potential residents.
Future research is needed with larger, more socially and economically diverse Chinese-American caregivers. Because the 2.5-generation has a unique background: one foreign-born and one US-born parent, we need to explore their caregiving experiences further in relation to culture and acculturation. Depending on the influence of either parent more toward foreign or U.S., their cultural values on filial responsibility may result in different experiences. Studies with later-generation caregivers’ perception of institutionalization and expectations of types of care by gender is also needed.
Limitations of the Study
This study used small, purposive samples of 19 caregivers from ethnic-specific social service agencies in Seattle, and 21 from Chinese church-related samples in Houston. Having strong ties with their ethnic communities may skew the results. Likewise, given the smaller sample size, the results may not be generalized more broadly to the larger geographic areas. All the caregivers were healthy, highly educated individuals regardless of generation and gender, and, thus, they may not represent the majority of Chinese-American caregivers. Nonetheless, this research provides a contextually rich initial understanding of the views of later-generation Chinese-American caregivers to inform future research.
Conclusion
Later-generation Chinese-American caregivers appeared to show high acculturation as well as strong filial responsibility levels while continuing their caregiving with traditional caregiving attitudes. Thus, ethnic Chinese-American caregivers’ cultural values seemed to remain the same across generations. For their own future care, it looks that Seattle caregivers chose mainstream facilities whereas some Houston caregivers preferred living with their children. These findings emphasize the importance of available local services as well as available services within the facilities. There has been a continuous flow of Chinese newcomers: they are the third largest immigrant group in the U.S. in 2017, following Mexican and Asian Indians (Zong & Batalova, 2017). It is essential to establish and maintain Chinese-specific service organizations where new immigrants can receive linguistically and culturally specific help. However, it is also important to ensure that appropriate services and supports are offered to consider later-generation caregivers’ culture such as English language, but Chinese food. There may be a need for ethnic-specific services such as a Chinese caregiver registry and Chinese food within the existing mainstream local residential facilities. It is critical that provision of services is in accord with the needs and preferences of local caregivers and their loved ones to prevent social isolation and to facilitate healthier and more productive lives among aging Chinese-Americans.
Footnotes
Acknowledgments
I sincerely express my appreciation to Dr. Nancy Hooyman, who reviewed the qualitative coding and manuscript reading for the Seattle caregiver study. I am grateful to my colleagues, Drs. Susan P. Robbins and Danielle Parrish for their advice for the Houston caregiver study, as well as Dr. Iris Chi for her thorough and rigorous reviews of the manuscript. I also appreciate Drs. Nai-Wei Chen and Paul Swank for statistical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The author received the School of Social Work Doctoral Award for Dissertation Support from the University of Washington, as well as from a Eunice Kennedy Shriver National Institute of Child Health and Human Development research infrastructure grant, R24 HD042828, to the Center for Studies in Demography & Ecology at the University of Washington for the Seattle caregiver study. The Seattle study was also in part funded by the T32 Women’s Health Postdoctoral Fellowship, National Institutes of Health (NIH), through Grant AG027677. The Houston caregiver study was funded by the Okura Mental Health Scholarship, sponsored by the Council on Social Work Education. The findings of this project are those of the author and do not necessarily represent the official views of the “NIH.”