
Abstract
Poverty and poor health disproportionately affect older adults serving as primary caregivers to their grandchildren. In underserved, rural regions, where grandparent caregivers may be especially vulnerable, grandparent caregivers may find support in cultural traditions. As part of a mixed methods study investigating stress among grandparent caregivers, the role religion and spirituality play in coping was explored using a survey complemented by semi-structured interviews with 26 rural grandparent caregivers. Findings suggest religion and spirituality facilitate coping by (a) providing a sense of purpose and perspective; (b) fostering peace and perseverance; and (c) promoting stability and social cohesion. This study describes how cultural assets aid grandparent caregivers’ coping and may inform supportive policies and practices for grandfamilies.
Introduction
Approximately 2.6 million older adults serve as the primary caregiver for one or more grandchildren (U.S. Census Bureau, 2017). Grandparent caregivers are a vulnerable population experiencing a higher poverty rate than the national average. Nearly one in five grandparents raising grandchildren live below the poverty level (U.S. Census Bureau, 2016), compared to a national poverty rate of 12.3% (U.S. Census Bureau, 2018). Further exacerbating the vulnerability of grandparent caregivers, disability affects approximately one-fourth of grandparent caregivers (U.S. Census Bureau, 2017). Many grandparent caregivers also live in areas lacking adequate healthcare-related goods and services. In communities with few healthcare-related resources, including those in Appalachian Kentucky, grandparent caregivers may delay or forgo personal care (Hayslip et al., 2017). Faced with many challenges, grandparent caregivers often report increased levels of stress as well as poorer self-perceived health (Trail Ross et al., 2015). Intensifying high prevalence of poverty, chronic disease, and disability, grandparent-headed households tend to receive fewer resources than nonparental homes/foster families (Strom & Strom, 2011). We sought to understand how these grandparents cope with multiple challenges. Although we had not intended to focus on religion and spirituality among grandparent caregivers, the voices of our participants made it clear that faith comprised a key coping strategy.
Religion and Spirituality as Culturally Supported Coping Strategies
Religious coping is a multifaceted construct that includes the use of spiritual beliefs, individual behaviors, social rituals, and practices to address hardship (Harrison et al., 2001). Existing research describes two forms of religious coping. Positive religious coping, which older adults more often use (Koenig et., 1998), reflects feelings of connection with God and spiritual connection with others. Negative religious coping involves expressions of spiritual discontentment such as feeling punished by God and blaming God (Koenig et., 1998).
Previous research describes a variety of mechanisms through which religion and spirituality support coping. Among family caregivers (Brémault-Phillips et al., 2016) and older adults (Koenig, 2015; Krause, 1988) religious participation facilitates stress management and provides a sense of purpose. Religious participation also helps caregivers develop a sense of peace (Dilworth-Anderson et al., 2007; Paiva et al., 2015). Extensive research among older African American caregivers has shown that faith and its expressions help manage stress (Pickard et al., 2018). Likewise, research conducted among South African grandmother caregivers revealed that prayers for strength, guidance and life necessities help grandmothers achieve a sense of purpose and hope (Dolbin-Macnab et al., 2015). Spirituality can also be an effective coping strategy (Simpson et al., 2017) associated with greater well-being among grandparent caregivers (Wilmoth et al., 2018).
Religiosity and spirituality in the Appalachian Kentucky setting
Across Kentucky, most adults (63%) describe religion as “very important in their life,” with 39% of adults praying at least daily and 63% of adults attending religious services at least weekly (Pew Research Center, 2018a). Given the importance of religion to residents of rural Kentucky, it is vital to examine the role religion plays in helping grandparent caregivers manage stress.
Within Appalachian communities, religious participation and social support align through Appalachian cultural traditions of strong extended family ties (Katz et al., 2007). These ties are fostered by specific “family churches” or religious congregations. Such church affiliations solidify social ties and provide a sense of order and space (Gerard et al., 2006; Hatcher, 2018; Zimmerman et al., 1990). Within rural Appalachian communities, “mountain churches” often develop special practices and structures that closely corresponds to the particular situations and circumstances of their members (Zimmerman et al., 1990). While the existing literature frequently characterizes rural populations as more religious, we currently lack research on the use of religious coping strategies within rural communities. To fill this gap in the research, we examined caregiving grandparents’ individual and communal forms of religious and spiritual practice through two approaches: questionnaires and in-depth interviews. Guided by immersion, the PI, an anthropologist, developed a mixed methods approach. Combining questionnaires that allowed us to investigate standard outcomes (social support) with in-depth interviews enabled a multifaceted and immersive perspective (Gilgun, 2012).
Theoretical Framework
To guide our exploration of how religious and spiritual coping support grandparent caregivers, we draw on a social ecological perspective, which emphasizes that individual functioning is influenced by a dynamic interdependence of situational social, cultural, environmental, and personal factors (Stokols, 1996). This perspective acknowledges multiple levels of influence. Micro-level influences encompass the interactions among friends, family, coworkers, and community members, and meso-level influences include the interrelations among micro-level influences. Macro-level influences involve cultural values, beliefs, and policy imperatives at the local, state, or national level (McLeroy et al., 1988).
Acknowledging multiple levels of influence, social ecological frameworks enhance the understanding of the range of influences on stress and coping (Elliott et al., 2006; Ungar, 2011). For example, micro-level influences may provide examples of socially normative coping responses, but these responses are embedded in and reliant upon the available community resources. How one copes and the expectations of one’s coping are further influenced by the broader cultural landscape (McLeroy et al., 1988; Ungar, 2011). Thus, a social ecological understanding of coping acknowledges the constraints and opportunities of the systems within which a caregiver is embedded. In the context of this study, a social ecological perspective directs attention to certain unique benefits and challenges of rural Appalachian life, and life in rural Eastern Kentucky more specifically. The Appalachian region is well known for its low socioeconomic status (Billings, 1974), with a median household income 20% lower than the rest of the United States (Appalachian Regional Commission, 2016). Appalachian residents experience some of the highest rates of heart disease, diabetes, cancer, stroke, injury, COPD, and suicide in the country (Appalachian Regional Commission, 2017b), as well as limited access to health-related resources (Hayslip et al., 2017). Amid conditions of scarcity, Appalachian communities maintain strong cultural traditions of religious beliefs and active involvement in church communities (Zimmerman et al., 1990). “Mountain churches” in rural Appalachia tend to reinforce real and fictive kin relationships and provide strong emotional and instrumental support to members of their congregations. For example, research in other Appalachian communities demonstrates that some churches provide childcare for grandchildren (Hatcher, 2018) and assistance to grandparents in accessing governmental aid (Gerard et al., 2006). In summary, a social ecological perspective supports an expectation that the perceived benefits and activities associated with religious or spiritual coping are contextual, specific to the unique social circumstances, and responsive of the social environment surrounding grandparent caregivers’ coping efforts.
Method
Setting
The Appalachian region of the southeastern United States covers 205,000 square miles and is home to more than 25 million people (Appalachian Regional Commission, 2017b). This study took place in two rural counties in central Appalachian Kentucky. Table 1 highlights socioeconomic conditions in the sample counties compared with state and national counterparts.
Socioeconomic Characteristics: Sample County A, Sample County B, Kentucky, United States.
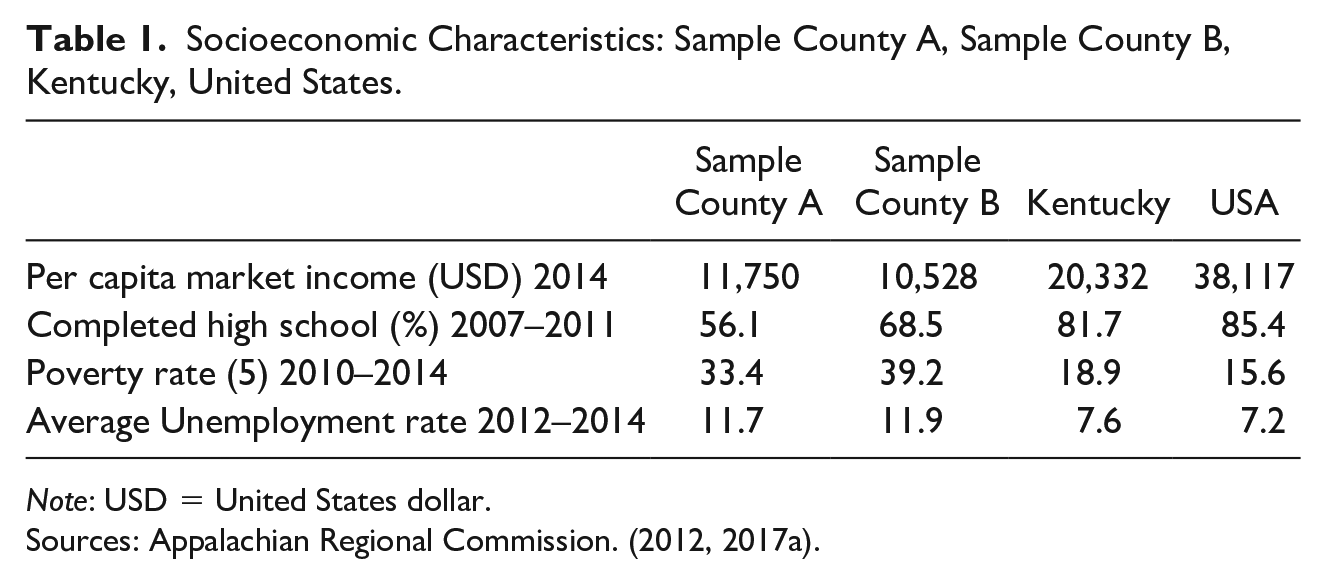
Note: USD = United States dollar.
In Kentucky, grandparents rearing their grandchildren is very common, and often occurs in conditions of extreme scarcity. Fifty-seven percent of co-resident grandparents in Kentucky have formal responsibility for their grandchildren, significantly higher than national rates (Murphey et al., 2012). These childrearing constellations frequently take place in challenging environments. In Appalachian Kentucky, the poverty rate (25.4%) is nearly twice the national percentage (15.6%) (Appalachian Regional Commission, 2017a). Despite the increased prevalence and vulnerability of grandparent-headed households in rural areas (Hayslip & Kaminski, 2005), researchers have not extensively examined rural grandparents’ caregiving and coping experiences. Many Appalachian cultural traditions, including religious practices and spirituality, offer grandparents support when facing these challenges. In this article, we first characterize the basic demographic, health, and psychosocial characteristics of 26 grandparent caregivers living in Appalachia. Grounded in a community-based participatory research approach (CBPR) (Wallerstein & Duran, 2006), we then highlight the voices of Appalachian caregiving grandparents. Consistent with the existing literature on Appalachian religious traditions (Houck, 2012), these grandparents describe how religious and spiritual coping support their lives as grandparent caregivers.
Design
Using a CBPR approach and mixed-methods, we conducted the “Grandfamilies in Gardens” study. The project focused on obtaining contextual insights and implementing an intervention to decrease food insecurity among grandfamilies in Appalachian Kentucky (Israel et al., 1998; Israel et al. 2001; Minkler & Wallerstein, 2008). The University of Kentucky Institutional Review Board approved the protocol, with grandparents and grandchildren providing informed consent and assent, respectively. We used mixed methods to understand contextual circumstances of the grandparents, complementing questionnaires with in-depth interviews. Consistent with principles of cultural-variant community-based participatory research (CV-CBPR), we adopted a strengths-focused lens and used culturally sensitive practices throughout the project (Henderson et al., 2017).
Sampling Strategy
Grandparents eligible for the study met the following criteria: (a) being 65 years or older; (b) serving as the primary caregiver of one or more grandchildren between the ages of 5 years and 18 years old, and (c) living with one or more grandchild(ren) for at least the past year. We collaborated with Family Resource Centers (which provide medical and social case-management services to students in public schools) and other social service organizations. We also collaborated with the local Cooperative Extension Service, which sponsors a grandparents’ coalition/support group. After attending meetings or contacting organizational leaders, we described our project, and sought the contact information for potentially eligible individuals. The local project manager then contacted individuals to confirm eligibility, determine interest, and, when indicated, coordinate grandfamily participation. Snowball sampling enhanced recruitment.
Data Collection
Data collection included four interviews with one self-designated grandparent from each family. During initial interviews, researchers used established questionnaires to collect data on demographic characteristics, health status, health behavior, and family interactions. Grandparents’ stress and enjoyment associated with caregiving was assessed using a modified version of the Parenting Stress Scale (Berry & Jones, 1995) (α=.79) in which “grandparent” replaced “parent.” Grandparents responded using a five-point scale, with higher scores indicating greater agreement. Modified versions of the Short-Form 36 (SF-36) Health Survey and scoring manual, in which distances in “blocks” were converted to “yards” to reflect the rural setting, were used to assess grandparents’ physical and mental health (Ware et al., 1994). Higher scores reflected better physical and mental health. Among adults ages 65–74 in the US population, average physical health score is M= 43.65, SD=11.02, and average mental health score is M=52, SD=9.53. To measure grandparents’ level of depression, we used the nine-item Patient Health Questionnaire-9 (α=.80), which includes nine questions rated using a four-point scale, with higher scores indicating deeper depression (Martin et al., 2006), and scores above 5 suggesting depressive disorder (Lamers et al., 2008).
Grandparents’ access to four types of social support: affectionate support, emotional/informational support, tangible support, and positive social interaction, was assessed with the 18-item Medical Outcomes Study Social Support Survey (α=.93 to.98) (Sherbourne & Stewart, 1991) in which indications of how often someone was available to offer support on a five-point scale, were averaged, with higher scores indicating greater access to support. Two questions assessed grandparents’ religiosity and spirituality: “How often do you attend church or other religious meetings?” and “How often do you spend time in private religious activities, such as prayer, meditation or Bible study?” Participants answered using a six-point Likert scale that ranged from “1=never” to “6=more than once per week.” Finally, grandparents rated their perceived financial status by identifying with one of three statements: (a) “I have more than I need to live well,” (b) “I have just about enough to get by,” and (c) “I sometimes struggle to make ends meet” (Keller et al., 2018). Final interviews included open-ended questions about grandparents’ stress experience and coping mechanisms, as seen in Table 2. Grandparents received an honorarium of $50.00 for participating in each 1–2-hour interview.
Stress and Coping Interview Guide.

Data analysis
Descriptive statistics were used to analyze key sociodemographic data including grandparent age, marital status (single or partnered), highest level of education completed, perceived financial status, and the number of co-resident grandchildren. For the qualitative interviews, audio recordings were transcribed and analyzed by three independent coders using conventional content analysis (Hsieh & Shannon, 2005). The researchers recorded themes with analytic memos and developed a draft codebook, which was subjected to numerous revisions. To ensure coding validity, the three coders co-coded initial transcripts until the inter-coder reliability reached or exceeded an acceptable level (0.75) (Campbell et al., 2013). Throughout the process, the PI and coders met regularly to discuss themes, resolve discrepancies in coding, and refine the codebook. Collaboratively and iteratively developing the common codebook enhanced rigor by ensuring researchers applied codes with consistent meaning. From patterns emerging among the codes, themes were identified that illustrated the role of religious and spiritual coping among grandparent caregivers.
Several strengths of the data collection and analysis increase confidence in the credibility of the findings. First, our research team has partnered with communities throughout Eastern Kentucky to conduct community-engaged research for more than 15 years. Additionally, our team has helped build capacity within communities across Eastern Kentucky by providing research skills training and employment. Our strong track record of CBPR projects characterized by immersion in these communities has facilitated recruitment and engendered trust in our research team. Such trust encouraged participants to express themselves freely. Likewise, community partnerships afforded us insight into participants’ experiences and the meaning participants assigned to their circumstances. Throughout this in-depth study, we practiced immersion by gathering multiple sources of data including survey items focused on spirituality and religiosity, as well as open-ended questions about stress and coping strategies (Gilgun, 2012; Schoenberg et al., 2011). Finally, upon completion of our initial 10 transcripts, we employed member checking to assess and enhance validity of our data. Specifically, we presented our initial findings to participants and to our project managers, lifelong members of the local communities (Lincoln & Guba, 1985). Immersion also guided our data analysis. As we examined multiple dimensions of participants’ religious and spiritual coping, we identified connections among themes and subthemes and attempted to contextualize these within the rural Appalachian culture (Gilgun, 2012).
Results and Findings
Survey results
As shown in Table 3, participants included 26 grandparents (25 women), approximately half of whom (46%) were unmarried. Grandparents’ mean age was 67.7 years, and all participants self-identified as European American/White, consistent with the local population (Pollard & Jacobsen, 2017). The average year of education completed was 10th grade. Approximately two grandchildren under the age of 18 lived with each grandparent (M= 1.86; SD= 1.12), and more than half of grandparents (66%) had formal custody of their grandchildren.
Participants’ Demographic and Health Characteristics.

As shown in Table 4, respondents attended public religious activities between a few times a month and a few times a year (M= 3.74, SD=1.88), and reported taking part in private religious practice more than two times per week (4.0, S.D. 1.78).
Participants’ Psychosocial Characteristics.
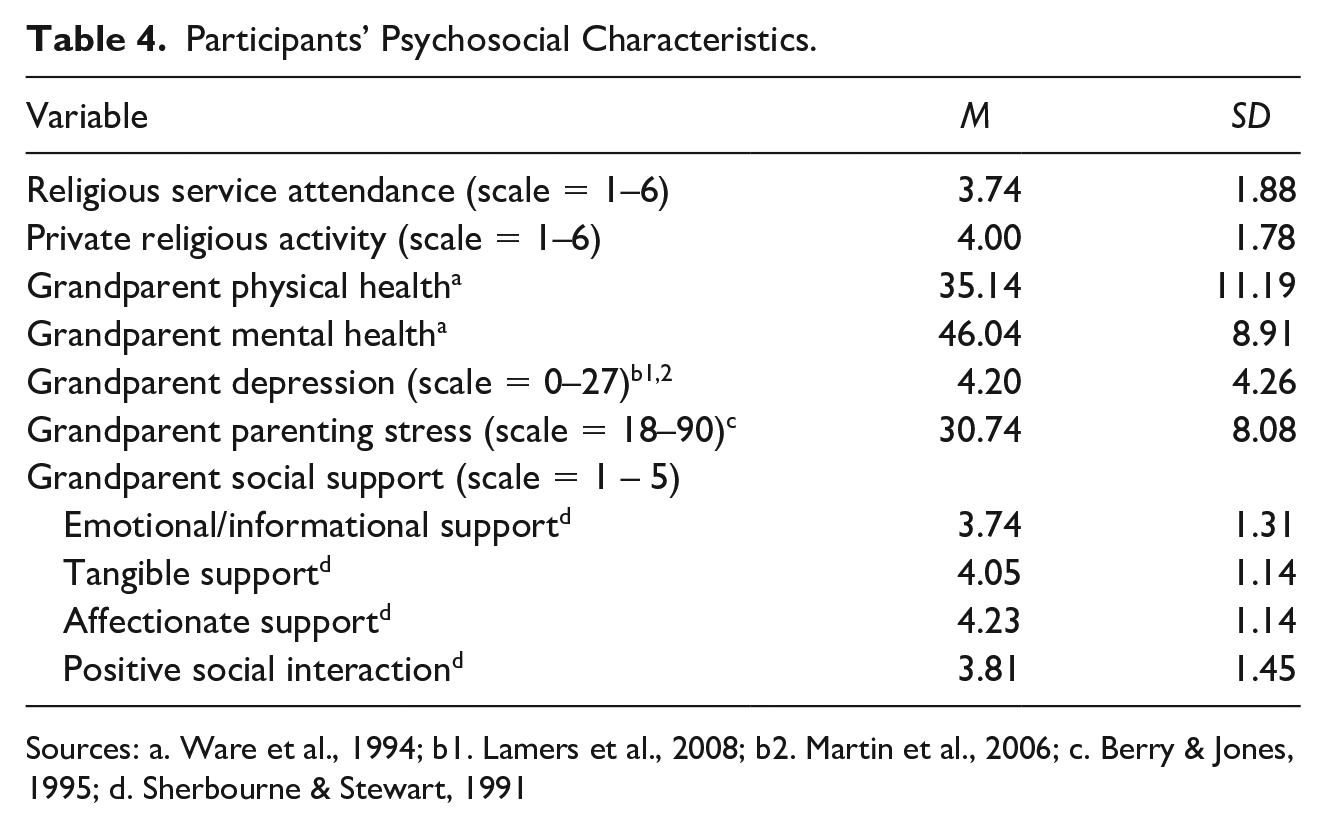
Sources: a. Ware et al., 1994; b1. Lamers et al., 2008; b2. Martin et al., 2006; c. Berry & Jones, 1995; d. Sherbourne & Stewart, 1991
Grandparents reported greatest access to affectionate support (M= 4.23, SD= 1.14) and tangible support (M=4.05, SD= 1.14). Emotional/informational support (M=3.74, SD= 1.31) and positive social interaction (M=3.81, SD=1.45) were also accessible to grandparent caregivers.
Findings from In-depth Interviews
Seeking to understand grandparent caregivers’ experiences, researchers practiced immersion by examining multiple perspectives and multiple dimensions of data (Gilgun, 2012). Consistent with the social ecological theory, grandparents’ behaviors, including coping mechanisms, reflected social, cultural, environmental, and personal influences (Elliott et al., 2006; Ungar, 2011). Grandparents revealed how religion and spirituality influenced their thoughts, feelings, and interactions with family and community members. Key themes emerged indicating that religion and spirituality aid grandparents’ coping by the following: (a) providing a sense of purpose and perspective (n=7; 27%), (b) fostering peace and perseverance (n=7; 27%), and (c) promoting stability and social cohesion (n=6; 24%).
Providing a Sense of Purpose and Perspective
Regular private and public religious activity provided a sense of purpose that enabled grandparents to cope with painful, traumatic experiences and difficult situations. Describing his experience rearing three grandchildren due to their father’s substance abuse, one grandfather noted, “God kept us alive for a reason…. Our children need to be taken care of.” His wife also explained, “We could have let these kids go but we had to intervene.” In addition to offering that rearing grandchildren was an assignment from God, grandparents discussed God’s assistance enabling them to accomplish this purpose. As a grandmother rearing two adolescent boys due to their mother’s death and father’s abandonment expressed: I tell them all the time, God has given me good health and blessed me with good health, because He knew I had to take care of these children. Somebody had to see after them. I’m always thankful.
Grandparent caregivers explained how religious activity provided social interactions that fostered appreciation and awareness. Describing how he dealt with a nearly constant state of financial concern, one grandfather revealed how attending church increased his awareness of other people’s struggles by diverting attention from his own problems: You get up, go to church, help people who need help, and you get home and wonder if you’ll make next month’s bills, but they’re always paid, you always make it. So that makes me feel good to help other people and sit down and still make it.
Religious and spiritual orientations, nurtured by regular private and public religious activities, provided a sense of perspective that enabled grandparents to reconcile the mistakes of the parent generation. As a grandmother who had been rearing her and her ex-husband’s grandchildren due to parental drug abuse described, “I think God’s plan is for us to make those mistakes. Because without making mistakes, you never learn.”
Fostering Peace and Perseverance
Key informant interviews enhanced our understanding of grandparent caregivers’ access to affectionate support and social interactions by revealing how conversations at church nurtured grandparents’ sense of peace and perspective. While describing how faith helped him buffer stress, one grandfather, who had been caring for his daughter’s children since they were born, explained: “You get up and go to church and listen to the people who talk, prayer requests and everything, it gives you the peace of mind.”
Religious practice and spirituality fostered a combined philosophical and theological orientation that reinforced grandparents’ recognition of God’s sovereignty, nurtured their sense of peace, and enabled their perseverance through trials. As expressed by one grandmother who had suffered the loss of multiple family members and now was rearing two adolescent grandsons: the God of the day is the God of the night, so He’s taken care of me, through the good times and the bad times. Last year, when my husband died, one Friday, the next Friday my brother died. I tell you what, I don’t think…. I haven’t even had time to really stop to think about it. . .but sometimes I say, well, I could sit and dwell on it, but it wouldn’t do me no good…. I’ve lost my daughter, my husband, and my only brother. And I’m standing on two feet – I’m good, I’m good. I’m good. I’m just glad I can take care of my children.
This philosophical, theological orientation, reinforced by regular private and public religious practice, enhanced grandparent caregivers’ awareness of affectionate support and helped grandparents frame daily circumstances as gifts from God. “It’s a big job to keep up with two girls, washing, taking care of their clothes, waiting on them hand and foot. Yep. But it’s the Lord’s blessing. I give Him all the credit,” noted one great-grandmother. Another grandmother rearing three grandchildren explained how certainty of God’s sovereignty gave her peace and hope for the future: I always say, and I say this every night before I go to bed. God is not going to put more on me than I can handle. And God is not going to put more on me tomorrow than what He’s got on me now. That’s something I go by. And I pray every night that He keeps us safe and I know He’s going to.
Private religious service, including conversations with God, helped grandparents manage stress: “It makes you feel at peace to talk to the Lord,” declared one grandfather. Grandparents mentioned that prayer helped them manage one of the greatest sources of stress: their grandchildren’s future. Grandparents prayed specifically for God’s assistance as illustrated in the words of a grandmother who had begun rearing grandchildren due to the parents’ substance abuse. “I worry about them, I worry about their future because it is so uncertain…. A lot of the things depend on their choices, so I hope and pray they make the right choices.” Another grandmother, who was rearing a difficult grandson, echoed similar sentiments by describing how constant prayer and talking with her grandson helped her manage worry and accept uncertainty: Yes. I worry about one thing, my grandkids. I raise them the best I can. I have one of them who has a temper and an attitude. I raise them the best I can, always pray for him. He’s got his daddy’s attitude, his daddy’s personality running through his veins. Every day we talk to him and encourage him to keep his friends, that’s all I can do.
Promoting Stability and Social Cohesion
Complementing the quantitative survey results, key informant interviews revealed how participation in church activities countered the stress and uncertainty of rearing grandchildren. Regular public religious and spiritual participation provided opportunities to connect with others and with a comfortable past. This connection made life more predictable and manageable for grandparent caregivers. When asked if rearing grandchildren had changed what he looked forward to, one grandfather noted, “No, not really. The only thing we’ve done more than anything else is go to church. We love going to church.” An 86-year-old great grandmother echoed this sentiment when asked if life had changed after her granddaughter moved in, “No, not really. I’ve always been a church-goer and I’ve always tried to keep my children in church.”
Regularly connecting with lifelong friends and traditions at church helped grandparents maintain their sense of self and enhanced grandparent caregivers’ access to affectionate and emotional support. “We’re close, we’re like family in our church. We grew up together,” explained one grandmother. Some churches also fostered comradery and emotional support among grandparent caregivers by hosting programs tailored to grandparent caregivers’ interests and needs. One grandmother described how membership in a religiously sponsored grandmothers’ group made her aware of how common her circumstances were and helped her focus on the positive aspects of rearing grandchildren: I did not know, until Sister Mary Kay (Catholic spiritual leader who leads the grandparenting group), there was that many grandparents raising their grandchildren and when I look at them, I think, “Man, I am blessed.” Because I didn’t lose my children to drugs, and the biggest part of grandparents raising grandchildren, it is where the parents lost them and they went to their grandparents. I’m glad that it didn’t get my children, because most of them come from drug families. Gosh, I am blessed. When I see them with 2, 4, 6 kids…. I am so blessed.
In addition to providing emotional support, public religious and spiritual activities enhanced the stability of grandparents’ lives by fostering access to informational and tangible support. For example, church-affiliated clubs helped grandparents cope with the disappointment of restricted freedom by providing opportunities for respite and fun with other grandparents experiencing similar circumstances. One grandfather explained: “We planned on getting up and going places and this makes it hard to do things…. It keeps us home more, not traveling and going to different places. We’d have to bring the grandkids with us.” After noting that rearing grandchildren limited her spontaneity and ability to travel to visit friends and family, one grandmother explained how the grandmothers’ group helped her cope with these restrictions: That’s the main reason why I joined a granny club, for grannies raising grandchildren…. We go there once a month and we go there for two hours but they feed us, and they give us a gift card and take us to Natural Bridge (State Resort Park) to go swimming, sometimes to eat. It’s been exciting for that. Jimmy will say, you don’t need to go to that and I say, yes, I do. I need to have some time off.
Church affiliation also increased grandparents’ access to material goods, as one grandmother mentioned: “sometimes we will go there [the church-affiliated clothing store] and they’ll let us go there and get what we need.” Familiarity and comfort with their church community helped grandparents overcome barriers to accessing needed supports.
Discussion
This study is among the first to describe coping among the growing population of extremely vulnerable rural grandparent caregivers. Such insights are critical since (a) nearly one in five rural residents is older than 65 years of age (Pew Research Center, 2018b); (b) Appalachian residents account for approximately 8% of the US population (Appalachian Regional Commission, 2018); (c) grandparent caregivers are more prevalent in Appalachia compared to other regions of the US; and (d) Appalachian grandparent caregivers likely represent an extreme version of what other grandparent caregivers are experiencing due to low socioeconomic status, sparse community resources, and geographic isolation of Appalachian communities.
Guided by immersion and the socioecological model, the present study acknowledges the influence of cultural nuances on grandparent caregivers’ perceptions of and approaches to managing stress (Gilgun, 2012; Letiecq et al., 2008), and complements previous qualitative research into grandparents’ experience of the caregiver role (Landry-Meyer & Newman, 2004).
The quantitative data demonstrated Appalachian grandparents’ high degree of religiosity and spirituality, as well as their access to abundant social support. Most study participants engaged in private religious practice more than twice a week, and reported high levels of affectionate support tangible support, positive social interaction, and emotional and information support. The in-depth interviews revealed not only that religion and spirituality provided a sense of purpose, perspective, and peace, which helped grandparent caregivers persevere, but also that religious practices promoted stability and strengthened grandparents’ social cohesion. The qualitative data also reinforced and specified the influence of socioecological factors in shaping grandparent caregivers’ use of religiously- and spiritually focused coping strategies. For example, Appalachian grandparent caregivers in our study prayed for grandchildren, the parent generation, and God’s assistance. These requests mirror prayers for resolution, change of perspective, intervention, and assistance documented among African-American grandparent caregivers in the Southern United States (Harris, 2013). Here we discuss how our findings corroborate and enhance existing research into the lives of grandparent caregivers. We also outline implications for future research, practice, and policy.
Appalachian grandparent caregivers maintained an overwhelmingly positive approach to religious coping. Previous research indicates that older adults tend to use positive religious coping strategies, which emphasize connection with God and others (Koenig et., 1998). Consistent with these findings, none of the participants in this study described feeling punished by or disappointed in God. This lack of negativity associated with religion or spirituality was surprising given the contrast between conservative religious values described by existing research on Appalachian religious traditions (Hutson et al., 2018) and the problematic circumstances (substance use disorders, incarceration, and parental neglect) leading to grandparents providing care. While piety is emphasized among mountain churches, grace and the Holy Spirit are also important foci, possibly explaining participants’ lack of negativity (Leppman, 2005; McCauley, 1995).
Second, familiarity with the church community helped grandparent caregivers overcome barriers to needed support. Consistent with the findings of this study, existing research has documented a connection between religious participation and social support among older adults (Horning et al., 2011) as well as among various caregiver populations (Cless et al., 2018; Heo, 2014). Among grandparent caregivers in Appalachia, religious participation and social support come together in culturally patterned ways such that attending church allowed grandparents to maintain continuity not only with their own history and traditions but also with lifelong members of their church “family.”
Implications for Practice and Policy
Our findings suggest numerous opportunities for practitioners, policymakers, faith leaders, and social service administrators to leverage cultural traditions in Appalachian communities. The current study documented that participation in religiously affiliated grandparent support groups provided tangible support (food and outings for grandparents), emotional support, comradery, and respite from childcare responsibilities. Appalachian churches may also provide childcare and positive experiences for grandchildren (Hatcher, 2018). Some religious organizations also provide informational and tangible support by helping grandparents access governmental aid. When churches support grandparent caregivers, grandparents’ well-being improves (Gerard et al., 2006). Acknowledging the great solace grandparents find in religious practice by attending church, faith organizations may consider expanding ritual and social programming for grandparents. Potential programs could include events to foster a sense of purpose among grandparents through social action projects, classes and leisure events. For example, intergenerational scripture studies may promote connectivity and learning while reinforcing values. Community leaders, local service providers and spiritual leaders should also seek opportunities to locate programming for grandparents in religious and spiritual settings since grandparent caregivers’ familiarity and comfort in these environments may facilitate grandparents’ access to needed supports.
In July of 2018, the Supporting Grandparents Raising Grandchildren Act was signed into law, which created the Advisory Council to Support Grandparents Raising Grandchildren to “identify, promote, coordinate, and publicly disseminate information and resources to help older relatives meet the needs of the children in their care and maintain their own health and emotional well-being” (Congress, 2018). As organizations expand programs, research should document and disseminate findings so that the advisory council’s reports reflect culturally relevant best practices and gaps in services.
Study Limitations
While this investigation provides insight into connections between cultural assets including traditions of religion and spirituality, and grandparent caregivers’ stress management, several limitations must be considered. First, our findings may not be generalizable to all grandparent caregivers. Though most grandparent caregivers are younger than 65 years of age (Ellis & Simmons, 2014), our eligibility criteria required grandparents to be at least 65 years old to participate in the study. For this reason, we may not have accounted for the full range of grandparent perspectives. Furthermore, predominantly grandmothers participated in this study, so the important contributions of grandfathers (Fuller-Thomson & Minkler, 2001) have not been fully explored. For these reasons, future research among rural grandparent caregivers should focus on investigating the stress experience and coping strategies of younger grandparent caregivers and of grandfather caregivers. Second, the racially homogenous population, though consistent with local demographics, is distinct from much of the United States. Third, caregiving experiences among grandparents in Appalachia may not be identical to all other grandparent caregiving, thus limiting generalizability.
Despite these limitations, there is much to be gained from these in-depth insights given the prevalence of grandparent caregivers in Appalachia and the extreme disparity Appalachian grandparent caregivers experience. Though specific coping strategies used by grandparents vary, religious and spiritual practices remain a cornerstone of some Appalachian grandparent caregivers’ coping response.
Footnotes
Acknowledgements
We express appreciation to the following individuals for their considerable efforts on behalf of this project: Shuang Bi, Aaron Guest, Rachel Swanson, and Lily Weddle. Special appreciation goes to Project Managers Glenn Kincaid and Barbara Bowling.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by The Retirement Research Foundation [#2014-211: Schoenberg]; Igniting Research Collaborations [Keller & Schoenberg]; and the University of Kentucky Center for Clinical Translational Sciences [Keller]. The CCTS is funded by the National Center for Advancing Translational Sciences, National Institutes of Health, through grant number UL1TR001998. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Retirement Research Foundation or the NIH.
Ethical Approval
University of Kentucky Institutional Review Board protocol/human subjects approval number: IRB #15-0108-P3H