
Abstract
Childhood abuse has been widely associated with mental health problems in adulthood and marital quality may be one possible mediator. We examine marital quality as a mediator linking childhood abuse to positive affect, negative affect, emotionally reactivity, and aggression. Using data from Midlife Development in the United States (MIDUS), results of structural equation modeling indicate that the indirect effects from childhood abuse to each of the mental health outcomes were significant. Marital quality may be a source of resilience among adults who were abused in childhood and could be a point of intervention for clinicians.
Marital Quality as a Mechanism Linking Childhood Abuse to Mental Health in Midlife Adults
Childhood abuse, defined by physical, emotional, and sexual abuse, is common within the United States and has been positively associated with mental, physical, and relational health problems across the life-course. A recent meta-analysis found roughly 24% of adults reported childhood physical abuse, 36.5% reported emotional abuse, and 20.1% of women and 8% of men report childhood sexual abuse (Stoltenborgh et al., 2015). Further, experiencing one form of childhood abuse dramatically increases the likelihood of experiencing another (Finkelhor et al., 2007). Childhood abuse has been linked to mental health problems in adulthood (DiLillo et al., 2007; Kong et al., 2018; Nelson et al., 2017) as well as physical health issues and early mortality (Lee & White, 2012; Widom et al., 2015). Due to the detrimental consequences, it is important to identify pathways and points of intervention to reduce health problems associated with childhood abuse.
Adult relationships with family members, friends, romantic partners, and general social support may mediate the association between childhood abuse and adult mental health (Kong, 2017). Intimate relationships are particularly important because of more frequent interactions and a greater level of interdependence compared to other interpersonal relationships. Marriage quality is consistently linked with mental health problems (Whisman & Baucom, 2012) and may serve as a mediator linking childhood abuse to adult mental health. Childhood abuse is an interpersonal act that causes physical and/or emotional harm, creating negative internal representations of relationships that can lead to relationship problems and psychopathology (Godbout et al., 2009). The extent to which adults have a quality intimate relationship may explain the association between childhood abuse and psychopathology (Author Citation). If adults abused in childhood can find an intimate partner offering support, nurturance, and companionship, they are likely to report fewer mental health problems, whereas adults in violent, strained, or conflictual intimate relationships are likely to experience mental health problems. Few studies, however, have considered relationship quality as a possible pathway by which childhood abuse is associated with adult mental health. The purpose of this study was to examine marital quality as a mechanism linking childhood abuse to mental health problems frequently associated with childhood abuse including aggression, emotional reactivity, positive affect, and negative affect in a sample of midlife adults.
Theoretical Background
The traumagenic model (Finkelhor & Browne, 1985) provides insight into the relationship between childhood abuse and adult mental health, and proffers there are four dynamics occurring during abuse: betrayal, traumatic sexualization, stigmatization, and powerlessness. Although the original model was proposed for survivors of sexual abuse, the dynamics also occur in emotional and physical abuse (DiLillo et al., 2009). The traumagenic model suggests abuse creates low self-worth, shame, guilt, mistrust, and distorts children’s view of relationships. These dynamics are often carried into adulthood and manifest in marriage. For example, abuse is frequently perpetrated by caregivers responsible for the child’s well-being, and this betrayal may lead to trust issues in marriage, because, like the parent-child relationship, marriages are interdependent relationships characterized by intimacy, closeness, trust, and mutual influence (DiLilio & Long, 1999; DiLillo et al., 2009). Traumatic sexualization may impact adults’ ability to have emotional and physical intimacy in relationships (DiLillo et al., 2007). Abused children often experience stigmatization, creating feelings of worthlessness and shame. This can result in detachment from partners, reassurance seeking, and conflict. Last of the traumagenic dynamics is powerlessness, where children are simultaneously dependent on caregivers for nurturance while also recognizing they are sources of pain, stress, and terror. In adulthood, powerlessness may impair decision making, identifying needs, and being open and honest with partners (DiLillo et al., 2009; DiLilio & Long, 1999; Finkelhor & Browne, 1985). Thus, the traumagenic dynamics may leave adults at risk for poorer quality relationships.
Decreased ability to form safe, secure relationships places adults at enhanced risk for poorer psychological adjustment. Underlying feelings of shame, guilt, worthlessness, and powerlessness are likely to potentiate a wide array of mental health problems (Dunlop et al., 2015; Kong et al., 2018). The extent to which adults report mental health problems may be partially explained by how safe and secure they feel in their marriage. For many, romantic relationships are a source of healing where a high-quality relationship attenuates the impact of traumagenic dynamics. Feeling comfort, companionship, support, and a sense they matter to their partner, provides a corrective experience that can attenuate mental health problems (Flett et al., 2016; Goff et al., 2006). Adults with a partner as a secure base have an interpersonal source of emotional regulation and experience greater positive effect and fewer negative affective symptoms (Thoits, 2011). Additionally, adults with a high-quality and secure relationship are better able to navigate conflict and strain. Walker and colleagues (2009) found childhood abuse was associated with greater emotional dysregulation during conflict, potentially leaving adults more vulnerable to aggressive behavior and intimate partner violence (IPV) whereas a secure relationship reduces the risk of violence (Spencer et al., 2020).
Childhood Abuse and Adult Mental and Relational Health
Mental health problems are common among adults who were abused in childhood. Abused children often feel powerless, worthless, shame, guilt, and unsupported and unimportant to caregivers (Finkelhor & Browne, 1985; Flett et al., 2016). These internalized beliefs often lead to mental health problems in adulthood. Additionally, childhood abuse can impair the ability to emotionally and physiologically self-regulate, a risk factor for long-term mental health problems (Coates & Messman-Moore, 2014). Consistent with these propositions, adults abused as children were found to have greater emotional reactivity and dysregulation (Dvir et al., 2014), less positive and more negative affect (Kong, 2017), somatic complaints (Zink et al., 2009), substance use (Dube et al., 2005), anger (Maldonado et al., 2015), and aggression (Chen et al., 2012). Using a nationally representative sample, Taillieu et al. (2016) found adults emotionally abused as children had an increased risk for developing numerous disorders including major depression, dysthymia, posttraumatic stress disorder, generalized anxiety disorder, social phobia, panic disorder, drug and alcohol dependence disorders, and personality disorders. Similarly, Afifi et al. (2017) found physical abuse was associated with increased odds of depression, suicide attempts, moderate to heavy drinking, and lifetime drug use.
A significant body of research found a negative association between childhood abuse and marital quality and indicators within marriage. Because abuse is an interpersonal betrayal that impairs psychosocial development, these capacities may not fully develop in childhood, resulting in effects seen in adult relationships. The association between childhood abuse and more negative and fewer positive interactions is consistently documented (Whisman, 2014). Specifically, abuse in childhood is associated with greater conflict (author citation), more volatile conflict resolution strategies (Knapp et al., 2017), poorer communication (Banford-Witting & Busby, 2019), and providing less emotional support to partners (author citation). Whisman (2014) found adults physically abused as children were perceived by their partner to engage in fewer positive and more negative interactions, and in turn perceived their partner to engage in more negative and fewer positive interactions. Childhood abuse is likely to negatively impact the overall quality of marriage through increasing the negative dimensions while decreasing the positive. The association between childhood abuse and lower quality relationships has been found for young adults (Riggs et al., 2011), newlyweds (DiLillo et al., 2009), midlife adults (Whisman, 2006), and older adults (Whisman, 2014).
Marital Quality and Adult Mental Health
Marital quality is an exceedingly complex concept (for reviews see Bradbury et al., 2000; Fincham & Rogge, 2010). Marital quality assessment strategies differ, as some argue there are too many domains to measure (Norton, 1983), some argue for the measurement of specific indicators of discrete domains (i.e., trust; DiLillo et al., 2009), while others advocate for implicit measures (Fincham & Rogge, 2010). Aspects frequently examined include communication, intimacy, emotional support, strain, conflict, and emotional distance (Bryant et al., 2016; Fletcher et al., 2000; Ledermann et al., 2010). Following this model, the current study conceptualizes marital quality as a multidimensional construct consisting of marital support, strain, and disagreement. This approach provides information researchers and clinicians can use to understand the intricacies of marriage in the context of childhood abuse and adult mental health (DiLillo et al., 2009). Global and implicit measures cannot provide nuanced information as clinically informative.
The relationship between marital quality and adult mental health has interested clinicians, researchers, and policy makers alike. Researchers have postulated that marriages are either a source of positive (e.g., joy) or negative (e.g., emotional reactivity) mental health. Approximately 30 years ago, Beach and colleagues proposed the marital discord model of depression (Beach et al., 1990), which posits marriages can be both sources of support (e.g., cohesion, support, and intimacy) and stress (e.g., discord, aggression, and relationship instability). Adults experiencing greater marital discord and stress, coupled with less support and intimacy, are at risk for developing depressive symptoms. Indeed, studies have found support for the marital discord model (e.g., Hollist et al., 2007; Miller et al., 2013). Despite an initial focus on depression, more contemporary research found empirical support for other mental health problems (Priest, 2013). For example, using a nationally representative sample, Whisman (2007) found marital problems were associated with enhanced likelihood of meeting criteria for mood, anxiety, and substance use disorders. In review, Whisman and Baucom (2012) noted both cross-sectional and longitudinal studies found associations between the quality of marriage and mental health problems. Supplementing these findings, the quality of marriage may also increase positive mental well-being (i.e., positive affect). Proulx et al. (2007) conducted a meta-analysis investigating the association between marriage and positive mental well-being and found marital quality was associated with greater mental well-being.
Adults who report a high-quality marriage are more likely to report less emotional dysregulation and impulsive behavior. In high-quality marriages, with greater support and less strain and disagreement, adults turn to partners for support, believe partners are well intentioned, and make fewer negative attributions about and are less emotionally reactive and aggressive toward their partners. This may be particularly important among adults abused in childhood, as they tend to be trustful of their partners (DiLilio & Long, 1999), but only if they develop a safe and secure relationship.
The Present Study
Research proposes childhood abuse is linked to mental health problems, and marriage may be one possible mechanism (author citation); however, researchers have yet to investigate this relationship. This omission misses an opportunity to advance our understanding of the process linking childhood abuse to adult mental health and could provide a point of intervention for clinicians working with individuals and couples with mental health problems. The current study examined the indirect effects from childhood abuse to positive affect, negative affect, aggression, and emotional reactivity. It is hypothesized that childhood abuse will be negatively associated with marital quality and positive affect and positively associated with negative affect, emotional reactivity, and aggression. Further, it is hypothesized that marital quality will be negatively associated with negative affect, emotional reactivity, and aggression, and positively associated with positive affect. Finally, it is expected that childhood abuse will be indirectly related to the mental health outcomes through marital quality.
Method
Sample
Descriptive Characteristics of the Analytic Sample.

Measures
Childhood abuse
Childhood abuse was measured using an adapted version of the Conflict Tactics Scale and measured emotional and physical abuse from parents, siblings, and others. Physical, severe physical, and emotional abuse items began with the stem, “When you were growing up, how often were any of the things mentioned above done to you by…”. Each item was asked about respondents’ mothers, fathers, brothers, sisters, and others and options ranged from 1 (Often) to 4 (Never). An example of emotional abuse was “insult or swore at you” and illustrative items capturing physical and severe physical abuse were “slapped you” and “kicked, bit or hit you with a fist.” Only maternal and paternal abuses were used in this study and were averaged across abuse type. In other words, emotional, physical, and severe physical abuses were an average of maternally and paternally perpetrated abuse. Scores ranged from 2 to 8 for each type of abuse. A higher mean score of maternal and paternal emotional abuse, physical abuse, and severe physical abuse indicates greater abuse. Childhood abuse was conceptualized as a latent variable with emotional abuse, physical abuse, and severe physical abuse as indicators.
Support
Perceptions of support from partner were assessed with six items from the MIDUS study. Items measured the frequency of common manifestations of emotional support, including “Does he or she really care about you” and “Can you open up to him or her if you need to talk about your worries.” Options ranged from 1 (A Lot) to 4 (Not at All). Items were coded and a mean score was computed. Higher scores are reflective of higher levels of support. Cronbach alpha = .89.
Strain
Relational strain was assessed with six items tapping how frequently requests from the spouse are strained. Options ranged from 1 (Often) to 4 (Never). Example items include, “Does he or she make too many demands of you” and “Does he or she make you feel tense.” Items were coded and a mean score was computed; higher scores reflect higher levels of strain. Cronbach alpha = .87.
Disagreement
Disagreement was measured by three questions asking participants how often the individual disagreed with her/his spouse on “money matters, such as how much to spend, save or invest,” and “household tasks, such as what needs doing and who does it.” Options ranged from 1 (A Lot) to 4 (Not at All). A mean score of the three items was computed. Higher scores were indicative of less disagreement. Cronbach alpha = .72.
Positive and negative affect
Positive and negative affect was measure using nine adjectives describing respondent’s mood: five items for negative affect and four items for positive affect. A stem of “During the past 30 days, how much of the time did you feel…” and the adjectives for negative affect were “afraid,” “jittery,” “irritable,” “ashamed,” and “upset” and the adjectives for positive affect were “enthusiastic,” “attentive,” “proud,” and “active.” Options for both the positive and negative affect scales ranged from 1 (All of the time) to 5 (None of the time). Items were reverse coded so higher scores indicated higher levels of positive and negative affect. The means of the items were used in analysis. Cronbach alpha = .82 for negative affect and .86 for positive affect.
Emotional Reactivity and Aggression
Aggression was measured using the aggression subscale of the multidimensional personality questionnaire, which consists of four items rated on a 4-point Likert type scale: 1 (True of you) to 4 (False). Items included, “Sometimes I seem to enjoy hurting someone by saying something mean” and “Sometimes I just like to hit someone.” The emotional reactivity subscale consists of three items rated on the same scale and included, “My mood often goes up and down” and “Minor setbacks sometimes irritate me too much.” For both scales, items were reversed coded and summed together, with higher scores reflective of greater emotional reactivity and aggression, respectfully. Cronbach alpha for the emotional reactivity sale was .75 and aggression was .66.
Covariates
Numerous covariates were used in the analysis. Sociodemographic variables included the dichotomous variables of race (White/racial minority), living with an alcoholic as a child (Yes/No), and gender (Male/Female). Education was entered in as an ordinal variable ranging from 1 (No Formal Schooling) to 12 (Doctorate). We also controlled for physical health using one item: “In general, would you say your physical health is excellent, very good, good, fair, or poor.” The physical health item was reverse coded where higher scores reflect better health.
Statistical Analysis
First, descriptive statistics, including correlations, means, and SDs, were generated in SPSS. Next, structural equation modeling (SEM) using Mplus (Muthen & Muthen, 1998) was used to test the indirect associations between childhood abuse with adult mental health outcomes through marital quality. A model was created with childhood abuse as the predictor, mental health problems, including emotional reactivity, aggression, positive affect, and negative affect as outcomes, and marital quality as a mediator. Both childhood abuse and marital quality were measured using latent variables, each with three indicators. Childhood abuse indicators included parental emotional abuse, physical abuse, and severe physical abuse, while marital quality indicators were support, strain, and disagreement. SEM uses several statistics to evaluate the fit of a model, including the chi-square statistic, comparative fit index (CFI), Tucker–Lewis index (TLI), and root mean square error of approximation (RMSEA). An adequate fitting model has CFI and TLI values greater than .90 and preferably greater than .95. A non-significant chi-square test indicates good fit; however, this statistic is sensitive to sample size as it becomes significant in larger samples despite other indictors of a good fitting model (Kline, 2015). RMSEA values below .08 are deemed adequate but are preferably below .06. The indirect (mediating) effects from childhood abuse to adult mental health through marital quality were tested using bias-corrected bootstrap confidence intervals (CI) based on 5000 bootstrap samples. Bootstrapping is the preferred method of examining mediation because it does not assume the indirect effects to be normally distributed, as they often are not (Hayes, 2009). Final model fit was acceptable (CFI = .974, TLI = .934, RMSEA = .045, SRMR = .021, χ2 (48) = 178.982, p < .001).
Results
Bivariate Associations
Correlations Among Study Variables and Covariates.

Note. * p < .05 ** p < .01 *** p < .001.
SEM
Results of the SEM model, including direct effects and latent variable factor loadings, can be seen in Figure 1. Regarding the factor loadings for the childhood abuse latent factor, emotional (ß = .76, p < .001), physical (ß = .92, p < .001), and severe physical abuse (ß = .68, p < .001) all loaded significantly. Likewise, the three indicators of marital quality, including support (ß = .71, p < .001), strain (ß = .89, p < .001), and disagreement (ß = .64, p < .001), also loaded significantly. Results of latent variable structural equation meditational model.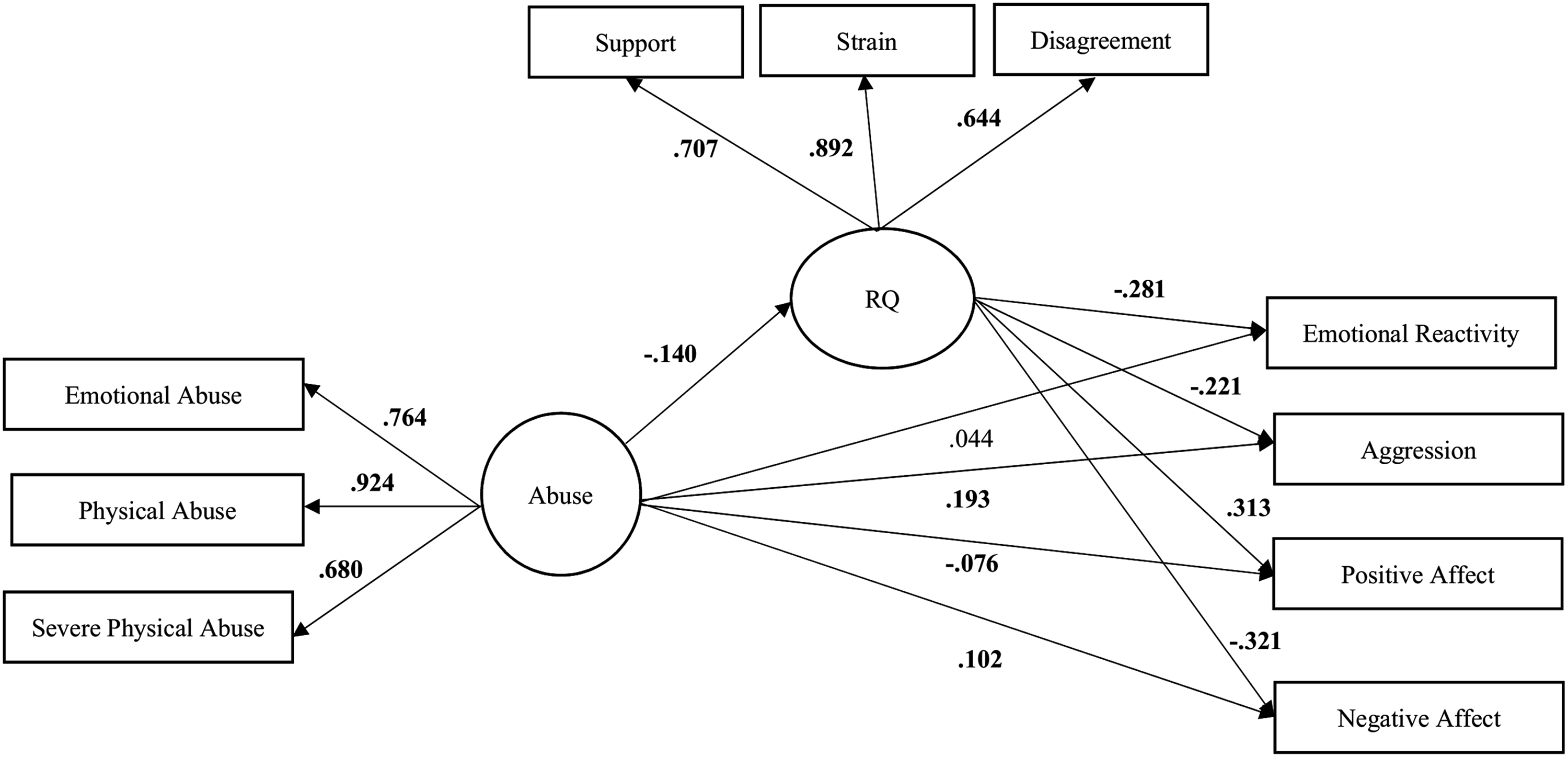
Direct Effects
In the full SEM model, childhood abuse was associated with poorer quality marriage (ß = −.14, p < .001) and higher levels of negative affect (ß = .10, p < .001) and aggression (ß = .19, p < .001). Furthermore, childhood abuse was negatively associated with positive affect (ß = −.08, p < .001). Childhood abuse was not, however, associated with emotional reactivity (ß = .04, p > .05). Marital quality was associated with each mental health outcome. Specifically, marital quality was inversely associated with lower levels of emotional reactivity (ß = −.28, p < .001), aggression (ß = −.22, p < .001), negative affect (ß = −.31, p < .001), and higher levels of positive affect (ß = .31, p < .001).
Indirect Effects
Bootstrapped Indirect Effects from Childhood Abuse to Mental Health Outcomes Through Marital Quality.
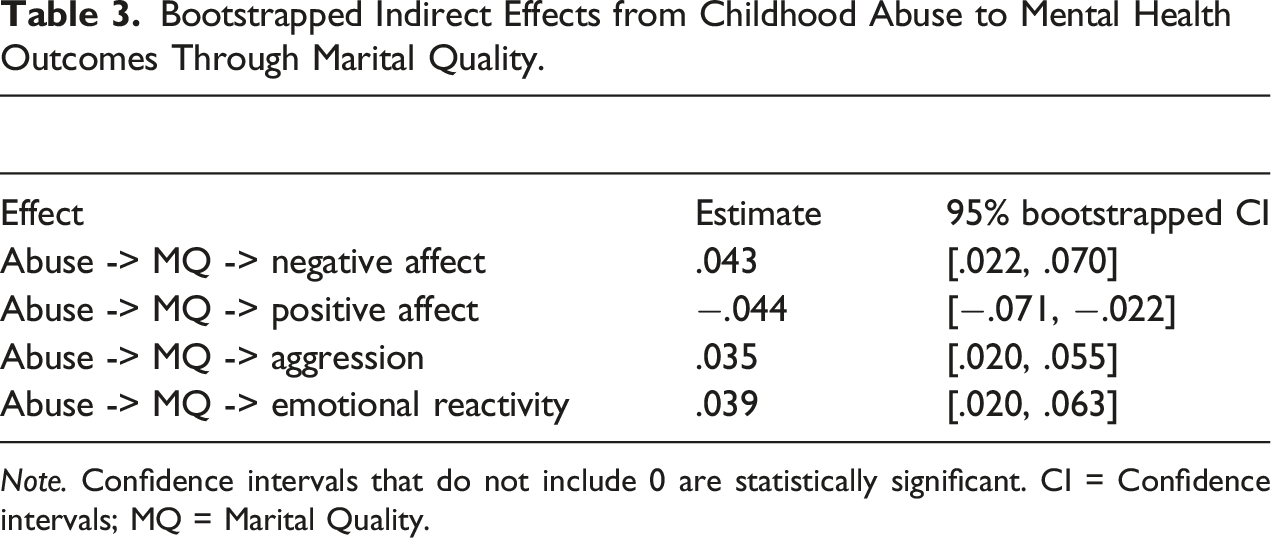
Note. Confidence intervals that do not include 0 are statistically significant. CI = Confidence intervals; MQ = Marital Quality.
Discussion
Childhood abuse has been consistently associated with mental health problems in adulthood. Prior research found adult interpersonal relationships may mediate the relationship between childhood abuse and mental health outcomes (author citation; Kong et al., 2018; Runtz & Schallow, 1997), and suggested marital quality may be a potential mechanism (Kendall-Tackett, 2002). The purpose of the current study was to examine marital quality as a potential mediator linking childhood abuse to numerous indicators of mental health functioning, including positive and negative affective symptoms, aggression, and emotional reactivity. These results provide preliminary evidence that marital quality is a possible mechanism linking childhood abuse to adult mental health functioning as we detected significant indirect effects to positive affect, negative affect, emotional reactivity, and aggression.
This study’s primary contribution was identifying that marriage quality was a mechanism linking childhood abuse to mental health outcomes in a large sample of midlife adults. Based on extent research, marital quality was expected to be a pathway linking childhood abuse to mental health outcomes, and this hypothesis was supported. Specifically, martial quality indirectly related childhood abuse to positive affect, negative affect, aggression, and emotional reactivity. Consistent with numerous studies, childhood abuse was associated with lower levels of marital quality (DiLillo et al., 2009; Dunlop et al., 2015; Whisman, 2006), which, in turn, was associated with each of the mental health problems (Whisman & Baucom, 2012).
Characteristics of high-quality marriages may provide a corrective experience compared to the traumagenic dynamics, including betrayal, powerlessness, traumatic sexualization, and stigmatization (Finkelhor & Browne, 1985). High-quality marriages, characterized by support, conflict resolution, and few negative interactions, can provide alternative experiences to adults abused as children. Marriages promoting self-esteem can ameliorate feelings of stigmatization, spousal support may override feelings of betrayal, and effectively resolving conflict can help adults feel empowered in their relationships. Consequently, marriages can have a diverse impact on mitigating negative symptoms as well as improving mental well-being (Beach et al., 1990; Whisman, 2007).
Thoits (2011) posited that higher quality marriages promote health though increasing health promotive behavior (e.g., dieting and exercise) and reducing health hindering behavior (e.g., alcohol use). She proposed high-quality marriages promote self-esteem and create a sense of belonging, companionship, acceptance, and emotional support (Thoits, 2011). Adults who were abused as children but forge a high-quality marriage, characterized by support, intimacy, and the ability to resolve conflict, may experience fewer mental health problems, and have greater positive affect, emotional regulation, and conflict resolution skills. This may be due to the psychosocial resources of the marital relationship (e.g., support) and increased self-esteem, which provides a secure base to talk about areas of disagreement and strain.
These findings suggest marital quality may mediate the abuse-mental health association, yet evidence of partial mediation for three of the four outcomes indicate there are other unmeasured variables affecting the relationship between childhood abuse and adult mental health. Prior research found familial and friend support are also mediators (Kong, 2017; Runtz & Schallow, 1997). For example, a recent study found childhood maltreatment was longitudinally associated with depressive and socially anxious symptoms through support from family, friends, and romantic partners, but did not account for individual factors (author citation). Kendall-Tackett (2002) suggested maladaptive coping strategies, cognitive schemas, and behavioral issues (e.g., sexual risk taking) also account for finding partial mediation. Future research may want to simultaneously examine interpersonal and intrapersonal pathways, providing insight into which paths have the strongest effect on adult mental health.
Limitations
Strengths of the study include the novelty of examining marital quality as a mediator linking childhood abuse to adult mental health, a large sample, and assessing a variety of mental health outcomes, yet this study is not without limitations. First, the study was cross-sectional, constraining our ability to make causal inferences. Second, the MIDUS data did not have an assessment of sexual abuse or neglect, so our assessment does not encapsulate the full experience of child maltreatment. Third, future research should not rely solely on survey methods because respondents with mental health problems may have biased perceptions of prior abuse. Prospective studies using substantiated cases of maltreatment (e.g., child protective services records) as well as observational methods can attenuate these limitations. The sample was also predominantly White, so extrapolations to racial minorities are significantly limited. Last, childhood abuse reports are retrospective and may be subject to reporting biases including not disclosing or recalling abuse.
Clinical Implications
Study findings have implications for clinicians. Marital quality was identified as a possible mechanism linking maltreatment to mental health outcomes. Although individual therapy could be effective and is sometimes required depending on the level of aggression within the relationship, we recommend couple therapy. Denton and Burwell (2006) found, compared to individual therapy, couple therapy demonstrated increases in both mental health functioning and marital quality. We suggest addressing disagreement, strain, and support in marriage may be particularly helpful. Partners may be caught in negative cycles of interaction (e.g., pursuer-distancer) leading to relational distress and higher levels of affective symptoms, emotional reactivity, and aggression. Replacing negative sequences of interaction (e.g., criticism and withdrawal) with more positive ones (e.g., intimacy and support) can allow couples to cope with stress, successfully navigate individual differences, and inject positive emotions into their marriage (Johnson, 2002). We recommend emotion-focused therapy for use where one or both partners have a history of abuse, as it has been found to be an effective treatment for such couples (Dalton et al., 2013), and may help address both marital problems and mental health issues.
Regarding aggression, results indicate addressing the couple relationship can improve aggression and other mental health problems, and that couple therapy can directly address such problems better than individual therapy. A thorough assessment of IPV is necessary so safety can be ensured. A meta-analysis found couple therapy for IPV shows promise (Karakurt et al., 2016); however, the authors cautioned to carefully assess each partner individually and again as a couple. Situational couple violence is characterized by mild to moderate levels of violence and can be worked on in the context of couple therapy. Alternatively, there is characterological violence and intimate terrorism that incorporates aspects of control and more consistent and severe relationship violence. In such cases, couple therapy is contra-indicated (Karakurt et al., 2016).
Conclusion
Results suggest marital quality may be one pathway by which childhood abuse is associated with adult mental health outcomes. Marital quality may be a point of intervention for clinicians and focusing on support, strain, and conflict may be a particularly important area of intervention. Adults who were abused as children are likely to view relationships negatively, leading to lower quality marriages; however, if adults develop high-quality marriages, they will likely report better mental health through fewer mental health problems such as emotional reactivity, aggression, and negative affect and greater positive aspects. Thus, a stronger marriage may have a dualistic impact on adult mental health.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: There was no direct funding associated with the publication of the current manuscript.