
Abstract
Background:
Internet gaming disorder (IGD) has become a growing mental health problem, especially among young people. eHealth literacy, the ability to find, understand, and assess health information from electronic platforms and apply acquired knowledge to address health problems, may play a crucial role in improving mental health and promoting help-seeking behaviors.
Objective:
This study aimed to test the role of eHealth literacy in IGD symptoms and help-seeking intentions for IGD and the mediating role of illness representations in these relationships.
Methods:
A cross-sectional survey was conducted online using a convenience sample of university students in Hong Kong (N = 370). Data were collected using the Brief Illness Perception Questionnaire, 9 diagnostic criteria proposed in the DSM-5, the Mental Help Seeking Intention Scale, and the eHEALS tool.
Results:
Among participants, 28.9% met criteria for probable IGD, yet only 10.8% self-declared as having IGD. Male students (β = 0.123, P = .018) and those with higher education levels (β = 0.120, P = .021) exhibited elevated IGD symptoms, while higher education (β = 0.128, P = .014) and fewer gaming hours (β = 0.135, P = .009) predicted stronger help-seeking intentions. eHealth literacy was negatively associated with IGD symptoms (β = −0.110, P = .034) and positively correlated with perceptions of treatment control (β = 0.106, P = .040). Path analysis revealed that eHealth literacy indirectly enhanced help-seeking intentions through increased treatment control beliefs (β = 0.031; 95% CI, 0.003-0.074).
Conclusion:
Findings highlight eHealth literacy’s protective role against IGD and its indirect effect on help-seeking through treatment control beliefs. Interventions targeting eHealth literacy and perceived treatment efficacy may reduce IGD risk and promote help-seeking.
Introduction
With the widespread use of the Internet, gaming has become a popular online activity. In Hong Kong, a study reported that 83% of young people play Internet games. 1 Internet gaming can be addictive. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), listed Internet gaming disorder (IGD) as a condition for further study, and the World Health Organization formally recognized gaming disorder as a diagnosis in The International Classification of Diseases, 11th Revision (ICD-11), with similar diagnostic criteria.2,3 It is defined as persistent and recurrent excessive use of the Internet to play video games, resulting in considerable impairment or distress over a period of one year. 3 IGD includes symptoms of (a) preoccupation, (b) withdrawal, (c) tolerance, (d) unsuccessful attempts to control, (e) loss of other interests, (f) continued excessive use despite psychosocial problems, (g) deceiving others regarding online gaming, (h) using games for escape, and (i) functional impairment. 3 IGD may lead to or co-occur with depression, anxiety, attention deficit hyperactivity disorder (ADHD), poor sleep quality, academic failure, and interpersonal difficulties.4-10 The prevalence of IGD in young people is particularly high. For instance, a study on IGD among young adults (aged 18-25) reported a rate of 26% in the United States, 21.1% in China, and 15.4% in Singapore. 11 Studies in Chinese college students reported prevalence ranging from 4% to 25.7%.9,12-15
Help-Seeking Intention for IGD
Evidence has shown that IGD is treatable with effective interventions, including cognitive-behavioral therapy, motivational interviewing, family-based approaches, and combined pharmacological-psychological therapy. 16 This implies that people need to raise their awareness of IGD and seek professional help to treat it. Seeking appropriate help is widely acknowhese findings emphasize the impledged as a protective factor against the development of mental disorders among various age groups, especially young individuals.17,18 Professional help-seeking intention refers to the intention to consult mental health professionals for their IGD. Based on the Stages of Change model, 19 help-seeking intention aligns with a stage of preparation and serves as an important predictor for actual help-seeking behavior. A study reported that the prevalence of intention to seek professional help for IGD among Chinese college students was 35.4%. 20 No related studies have been conducted in Hong Kong.
eHealth Literacy
eHealth literacy is defined as “the ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to addressing or solving a health problem.” 21 (p1) It may be a protective factor against IGD and a facilitator of help-seeking for IGD because these skills empower individuals to recognize problematic gaming patterns, comprehend their potential negative consequences, and identify effective strategies and resources for management and recovery. eHealth literacy may be linked to better psychological well-being by enabling a process where individuals can effectively seek, interpret, and apply online health information to reduce uncertainty, foster self-efficacy, and initiate appropriate coping or help-seeking behaviors. Previous studies have reported negative correlations between eHealth literacy and depression, insomnia, and post-traumatic disorder, which supports this proposed pathway.22,23 Additionally, regarding the role of eHealth literacy in help-seeking behavior, previous studies found that individuals with higher levels of eHealth literacy were significantly associated with a more positive attitude toward seeking mental health services, greater self-efficacy in seeking professional help, and more adaptive health-related behaviors.24-27 These findings emphasize the importance of eHealth literacy in managing mental health, particularly in promoting acceptance and engagement with mental health services. However, no study has tested the role of eHealth literacy in the context of IGD. Specifically, no studies have explored the relationship between eHealth literacy and IGD or help-seeking intentions for IGD. eHealth literacy remains a vital but underexamined issue in the area of IGD, not only to understand the levels and roles of eHealth literacy in this newly defined mental disorder by the World Health Organization but to develop appropriate interventions and promote service utilization for IGD.
Illness Representations
Illness representations reflect individuals’ perceptions of a health condition and its treatment, which can impact how they react to the potential threat it poses. Based on the Common-Sense Model of Illness (CSM),28,29 people form mental representations of their illness by integrating “lay” information learned from knowledge, previous social communication, the external social environment, and the current experience of the illness. Illness representations include cognitive and emotional representations. The cognitive representations consist of consequences (the effect of the illness on individuals’ life), timeline (whether the illness is acute, chronic, or cyclical), control (the extent to which the illness can be controlled), identity (labeling the illness and recognizing its symptoms), illness comprehension (overall understanding of the illness), and cause (perceived cause of the illness). 30 Emotional representations (the emotions induced by the illness) explain individuals’ emotional responses, especially negative ones such as worry and anger. These representations shape individuals’ coping strategies in parallel processes and influence their behavioral responses to the illness. Several studies have tested the role of illness representations in different mental health disorders and related help-seeking. 31 However, only 2 studies have been conducted in the context of IGD. One study reported significant correlations between some dimensions of illness representations regarding IGD (ie, consequence, timeline, personal control, treatment control, and concern) and symptoms of IGD in Chinese college students. 32 The other study found that consequences, timeline, and treatment control were the main predictors of professional help-seeking intention for IGD among undergraduates in China. 20
eHealth literacy may affect illness representations. 33 High eHealth literacy may enhance Internet gamers’ capacity to understand, evaluate, and act on online health information about IGD and develop accurate perceptions of their own risk of IGD. People with high eHealth literacy may have more positive attitudes and perceived resources for IGD treatment (eg, high treatment control). Such perceptions of IGD and IGD treatment may in turn reduce IGD symptoms and enhance help-seeking intentions for IGD. No studies were identified on whether eHealth literacy would affect illness representations of IGD or IGD and help-seeking via illness representations.
Purpose
While the existing literature establishes the global significance of IGD and the potential importance of eHealth literacy, several critical gaps remain, particularly within the Hong Kong context. First, although prior research has linked eHealth literacy to general mental well-being, its specific role as a protective factor against IGD has not been empirically tested. Second, the potential mechanisms linking digital health competencies to help-seeking behaviors for IGD are entirely unexplored. Furthermore, there is a distinct lack of data on help-seeking intentions and their correlates among Hong Kong college students. This population is of particular interest due to Hong Kong’s unique sociocultural environment—a highly digitalized, high-pressure academic setting where gaming is prevalent, yet mental health stigma may be a significant barrier to care. 34 This study aimed to test the roles of eHealth literacy in IGD and help-seeking intentions for IGD and the potential mediating role of illness representation of IGD in these relationships. Based on the above literature, 3 hypotheses are proposed: (1) Individuals with higher eHealth literacy would show fewer IGD symptoms; (2) individuals with higher eHealth literacy would be more likely to seek professional help to treat IGD; (3) eHealth literacy would reduce IGD symptoms and promote professional help-seeking via illness representation of IGD.
Methods
Study Design
We conducted a cross-sectional, observational survey over an eight-week period from September 1 to October 30, 2024. A non-probability convenience sampling method was used to recruit participants from the student populations of 2 major public universities in Hong Kong. Recruitment materials stated the study’s focus on “internet gaming and student well-being” to minimize selection bias from overtly seeking individuals with gaming problems. Potential participants were recruited via university mass e-mails. Interested and eligible participants finished the online self-administered questionnaires via Qualtrics. The inclusion criteria for participants were as follows: (1) being a university student in Hong Kong, (2) having played Internet games in the past year, and (3) providing informed consent for this survey. All Hong Kong college students can speak English and therefore the questionnaire was in English. The survey took about 10 minutes to complete. No incentive was provided for the participants. A total of 1500 students were invited to participate via university-wide e-mail lists. Of these, 520 clicked on the survey link (initial response rate: 34.7%). Seventy-two participants were excluded for not meeting the inclusion criterion of having played Internet games in the past year. A further 78 participants were excluded due to incomplete responses (completion rate <90%). The final analytical sample comprised 370 participants, representing 71.2% of those who started the survey and 24.7% of those initially invited.
Measures
eHealth Literacy
eHealth literacy was measured by the eHealth Literacy Scale (eHEALS), which is the most widely used measurement tool in this field. 35 It consists of the following 8 items (rated on a 5-point Likert scale, where 1 = strongly disagree and 5 = strongly agree): (1) I know how to find helpful resources on the Internet; (2) I know how to use the Internet to answer my questions about health; (3) I know what health resources are available on the Internet; (4) I know where to find helpful health resources on the Internet; (5) I know how to use the health information I find on the Internet to help me; (6) I have the skills I need to evaluate the health resources I find on the Internet; (7) I can tell high-quality from low-quality health resources on the Internet; and (8) I feel confident in using information from the Internet to make health decisions. The scale had good reliability (α = 0.89) in the current sample.
Illness Representations of IGD
Participants’ cognitive and emotional perceptions of IGD were examined through the 8 dimensions of the Brief Illness Perception Questionnaire (B-IPQ), 36 which consists of (1) consequences (“How much impact will this problem have on your life?”), (2) timeline (“How long do you think the problem will last?”), (3) personal control (“To what extent do you feel you can control the problem?”), (4) treatment control (“To what extent do you think treatment can help you with the problem?”), (5) identity (“How severe do you think the symptoms caused by this problem would be?”), (6) illness concern (“how concerned are you about this problem?”), and (7) comprehension (“How much do you think you understand about online game addiction?”). Each of these dimensions was rated from 0 (no effect at all) to 10 (severely affects my life). 30 It is important to note that in this study, the items assessed the perceptions under the hypothetical situation that the participants had IGD, and such hypothetical assessments have been used in a previous study. 20 Good psychometric properties have been reported for use with Chinese college students with IGD. 32 The scale had good reliability (α = 0.76) in the current sample.
Probable IGD and Self-Declared IGD
Probable IGD was assessed using the 9 diagnostic criteria proposed in the DSM-5, 3 which are preoccupation, tolerance, withdrawal, unsuccessful attempts to limit gaming, deception or lies about gaming, loss of interest in other activities, use despite harm, use for escape or relief of negative mood, and causing harms. In the questionnaire, participants indicated whether they had experienced these symptoms in the last 12 months (0 = No, 1 = Yes) and the scores were obtained by summing the participant’s answers, with higher scores indicating more severe IGD symptoms. Those who scored ≥5 were classified as having probable IGD.20,37 This scoring is consistent with the diagnostic criteria of the DSM-5. The tool has been used in other IGD studies.20,38-41 The scale had good reliability (α = 0.74) in the current sample. After completing the questionnaires to screen for probable IGD, the participants’ self-declared IGD status was assessed by asking, “When you think about your experience related to Internet gaming, do you think that you are addicted to Internet gaming?” (No = 0, Yes = 1).
Help-Seeking Intention for IGD
The participants were asked to indicate their intentions to seek help for IGD using the professional help-seeking subscale of the Mental Help Seeking Intention Scale (MHSIS). The scale is an adapted version from Ajzen’s Theory of Planned Behavior and was standardized by Hammer and Spiker. 42 It is designed to measure respondents’ intention to seek professional help if they had a mental health concern and it included a 3-item scale: (1) I intend to seek mental health service, (2) I will try to seek mental health service, and (3) I plan to seek mental health service, with responses ranging from strongly disagree (1) to strongly agree (6). The intention score was calculated by adding up the scores from all 3 items and then dividing the total by 3 to get the average. A higher score indicates a greater intention to seek help, and the scale has been used in previous studies on mental help-seeking intentions. 43 The scale had good reliability (α = 0.93) in the current sample.
Data Analysis
Descriptive analysis was conducted using mean (standard deviation [SD]) for continuous variables and frequency (%) for categorical variables. Linear regression analysis was performed to examine the association of background variables on IGD symptoms and help-seeking intention. Correlation analyses examined relationships between eHealth literacy, IGD symptoms, help-seeking, and each IPQ item.
Structural equation modeling (path analysis) was then applied to test the proposed model. Model fit was assessed with the following indices: (1) Comparative Fit Index (CFI) ≥0.95, (2) Tucker-Lewis Index (TLI) ≥0.95, and (3) Root Mean Square Error of Approximation (RMSEA) ≤0.07. 44 The significance of the mediation effects was assessed using bootstrapping analysis. The coefficients, along with their 95% confidence intervals (CI), were estimated through bootstrapping with 5000 resamples. SPSS 26 and AMOS (IBM Corp., Armonk, NY, USA) were used for data analyses.
Ethical Considerations
Ethics approval was obtained from the Survey and Behavioral Research Ethics Committee of the Chinese University of Hong Kong (#023-24). Informed consent was obtained from every participant at the beginning of data collection.
Results
Background Variables
Of the 370 participants, most were undergraduate students (66.5%) and female (64.1%). The mean of weekly Internet gaming hours was 7.9 (SD = 8.5). The number of participants with probable IGD was 107 (28.9%) based on the DSM-5, while 40 participants (10.8%) subjectively perceived having IGD (Table 1).
Participants’ Background Characteristics, IGD Status, Help-Seeking Intentions (N = 370).
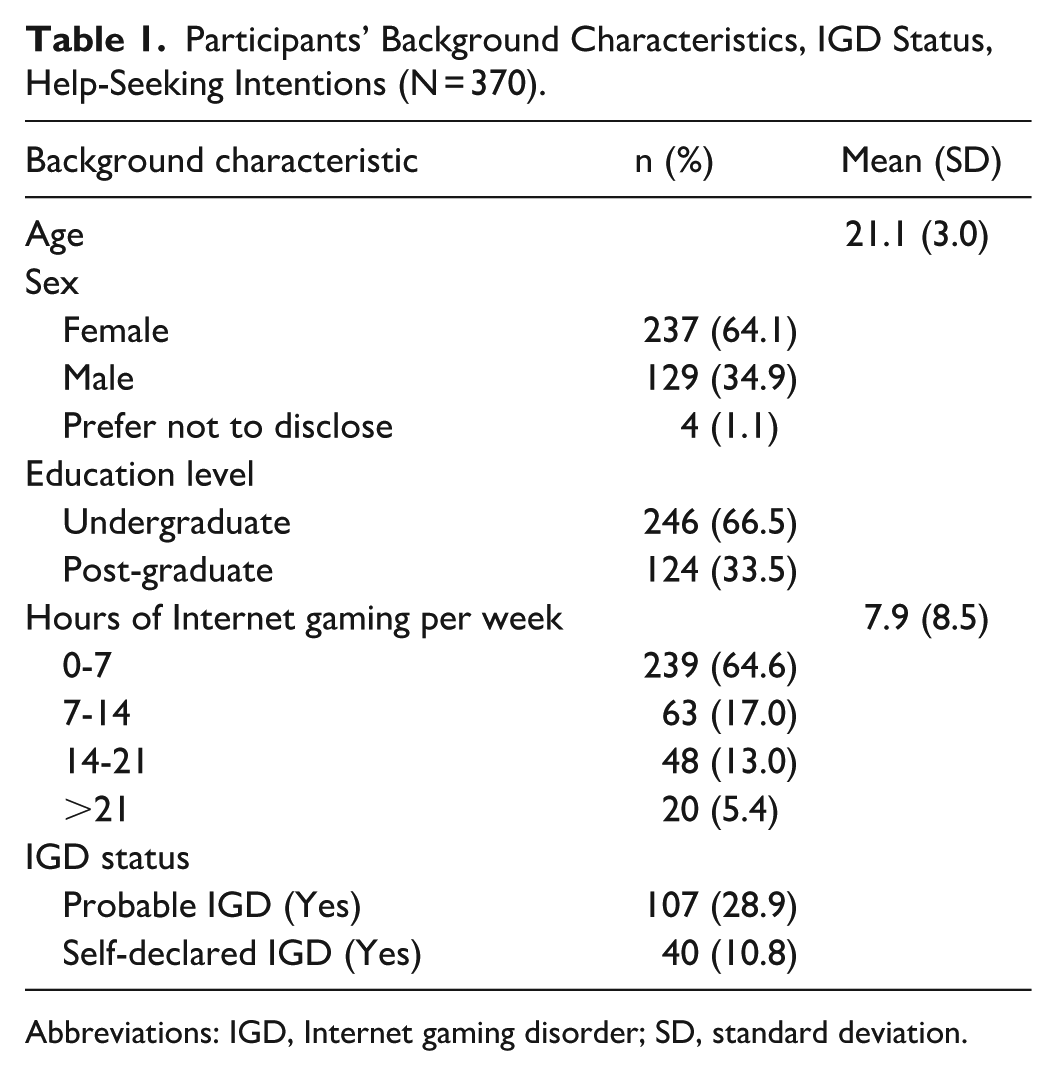
Abbreviations: IGD, Internet gaming disorder; SD, standard deviation.
Role of Background Variables on IGD and Help-Seeking Intention
Individuals who were male (β = 0.123, P = .02) and those with higher education levels (specifically, post-graduate students compared with undergraduate students) (β = 0.120, P = .02) exhibited higher levels of IGD symptoms. Additionally, those who self-declared as having IGD (β = 0.463, P < .001) were significantly more likely to report IGD symptoms. Furthermore, spending more hours on Internet gaming per week (β = −0.135, P = .009) was associated with lower levels of help-seeking intentions (Table 2).
Role of Background Variables on IGD and Help Seeking (N = 370).
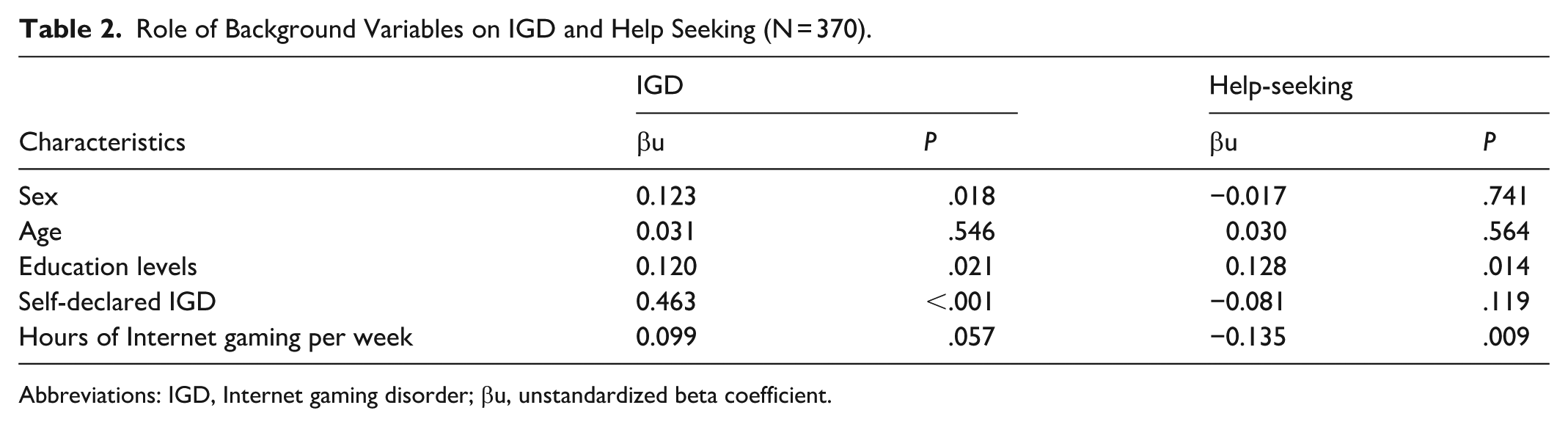
Abbreviations: IGD, Internet gaming disorder; βu, unstandardized beta coefficient.
Correlations Between eHealth Literacy, IGD, Help-Seeking, and Each IPQ Item
eHealth literacy had a significant negative correlation with IGD (r = −0.110, P < .05) and a positive correlation with treatment control (r = 0.106, P < .05). IGD exhibited a significant negative correlation with personal control (r = −0.162, P < .01) and positive correlations with consequence (r = 0.183, P < .01), timeline (r = 0.200, P < .01), identity (r = 0.174, P < .01), concern (r = 0.112, P < .05), and emotional response (r = 0.208, P < .01). Help-seeking intention was positively associated with consequence (r = 0.148, P < .01), treatment control (r = 0.295, P < .01), identity (r = 0.188, P < .01), concern (r = 0.193, P < .01), and emotional response (r = 0.157, P < .01) (Table 3).
Correlations Between eHealth Literacy, IGD Scale, Help-Seeking, and Each IPQ Item (N = 370).
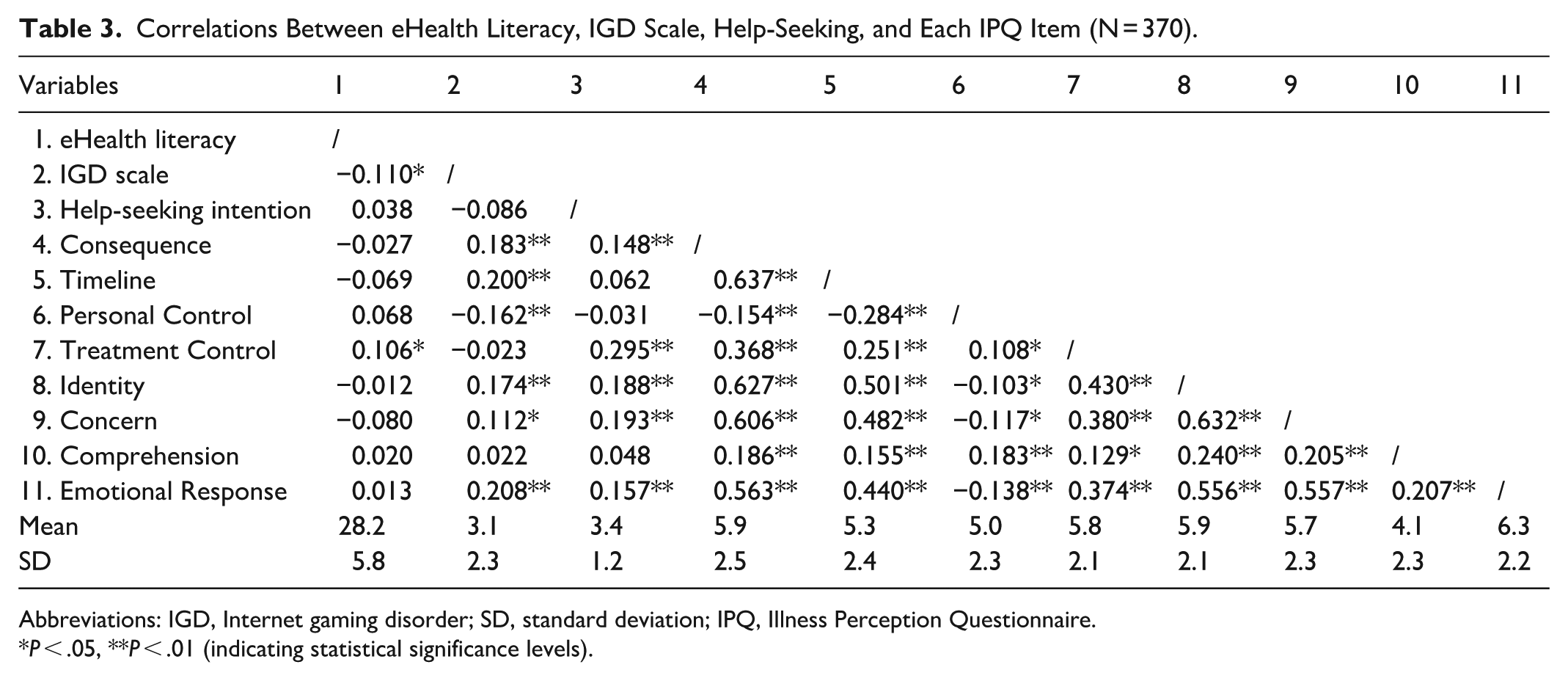
Abbreviations: IGD, Internet gaming disorder; SD, standard deviation; IPQ, Illness Perception Questionnaire.
P < .05, **P < .01 (indicating statistical significance levels).
Path Analysis
The model yielded a good fit to the data: χ2 = 0.047, P = .83, CFI = 0.999, TLI = 0.999, and RMSEA < 0.001; 90% CI, 0.000-0.083 (Figure 1; Table 4). The path analysis showed that eHealth literacy exhibited a positive association with treatment control (β = 0.106, P = .04) and a negative association with IGD (β = −0.110, P = .03). However, the relationship between eHealth literacy and help-seeking intention was nonsignificant (β = 0.007, P = .90). Treatment control was significantly associated with help-seeking intention (β = 0.293, P < .001). For indirect effects, eHealth literacy exerted an indirect influence on help-seeking intention through treatment control (β = 0.031; 95% CI, 0.003-0.074). Thus, a complete (full) mediation effect was demonstrated.
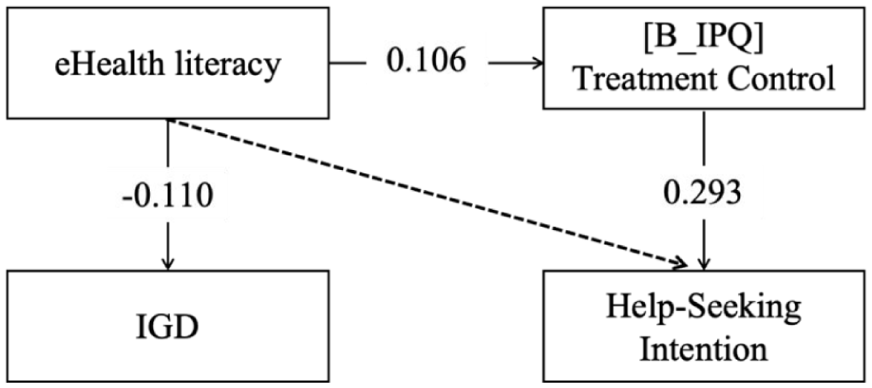
Proposed model.
Path Coefficients (N = 370).
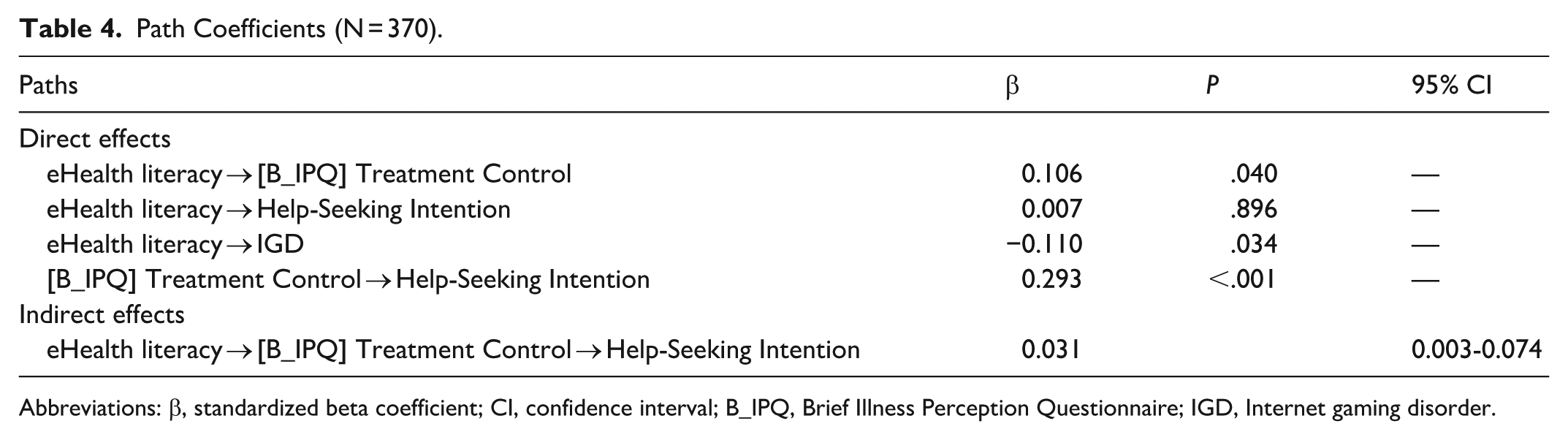
Abbreviations: β, standardized beta coefficient; CI, confidence interval; B_IPQ, Brief Illness Perception Questionnaire; IGD, Internet gaming disorder.
Discussion
This is the first study to test the role of eHealth literacy in IGD symptoms and professional help-seeking for IGD and the mediating role of illness perceptions. The results in our sample of college students in Hong Kong partially support our hypotheses.
First, we found that eHealth literacy was negatively associated with IGD symptoms. This finding is consistent with our hypothesis and previous studies on other mental health problems, such as anxiety and depression.22,23 It extends the relevance of eHealth literature theory to a novel domain: the realm of IGD as a recently classified mental health disorder and an emerging mental health challenges in the digital age. The results suggest that individuals with higher eHealth literacy skills may be better equipped to prevent, manage, and potentially mitigate symptoms of IGD. This implies that the ability to navigate online health information, evaluate resources effectively, and make informed decisions regarding one’s mental well-being could play a protective role against the development or exacerbation of problematic gaming behaviors. However, the modest magnitude of the standardized coefficients underscores that eHealth literacy is one of many contributing factors to IGD, which is a complex condition influenced by a confluence of individual (eg, personality, genetics), social (eg, peer influence), and environmental (eg, game design) factors. The small effect size is consistent with the notion that no single psychosocial variable is likely to exert a large, isolated influence on such a multifaceted disorder. Therefore, while our findings identify a statistically significant and theoretically plausible protective pathway, they should be interpreted as evidence of a small, incremental contribution of digital health competencies within a broader biopsychosocial model of IGD.
Furthermore, eHealth literacy may have implications for help-seeking. We found that eHealth literacy did not directly affect help-seeking intention but was indirectly associated with it via increased perceptions of treatment control for IGD. This finding suggests that eHealth literacy could affect how people perceive the treatment efficacy for IGD. Previous studies in other mental health problems also found that eHealth literacy was positively associated with positive attitudes toward seeking mental health services24,25 and self-efficacy in seeking professional help. 26 In turn, positive attitudes toward treatment (ie, perceived treatment efficacy for IGD in our study) could encourage and empower individuals to take charge of their mental health and seek appropriate assistance when needed. This highlights the importance of cognitive attitudes toward IGD treatment and the psychological processes in affecting professional help-seeking. Future research could delve deeper into the specific aspects of eHealth literacy that contribute to perceptions of treatment control and help-seeking intention for IGD. Exploring how different dimensions of eHealth literacy, such as information evaluation skills and digital health self-efficacy, might interact with treatment control beliefs could provide valuable insights into the underlying mechanisms driving help-seeking behaviors in the context of digital mental health support.
Compared with college students in some other cultures, our sample had a relatively lower level of eHealth literacy (eg, a mean of 30.2 in China; 31.9 in the United States)25,45 but higher than that in a Japanese survey (23.6). 46 These comparisons suggest that there may be cultural or regional differences in the levels of eHealth literacy. These differences may be influenced by a variety of sociocultural factors, such as attitudes toward technology, digital literacy, health information sources, technological access, and health care system differences. Efforts to address disparities in eHealth literacy in different regions and populations and identify the related factors are warranted.
This study has several limitations. First, the study used a cross-sectional study design, which cannot establish causal relationships among the variables. Further studies could use longitudinal methods to identify how changes in eHealth literacy levels may precede or follow changes in IGD symptoms and subsequent help-seeking behaviors. Experimental studies are also needed to test whether improving eHealth literacy would increase the intention to reduce IGD symptoms and to seek professional help for IGD. Second, our convenience sampling in Hong Kong college students might have induced sample bias and limited the generalizability of the findings. Third, the use of self-reported measures, while standard, introduces the risk of reporting bias. Especially for the IGD status, the proportion of probable IGD measured by the screening tool (28.9%) was much higher than that of self-declared IGD (10.8%). This discrepancy may be due to stigma and “shame” culture, lack of awareness of IGD symptoms, and social desirability bias. It highlights the limitations of self-diagnosis and reinforces the necessity of using standardized screening tools in both research and clinical settings to identify at-risk individuals who may not yet seek help. Future initiatives should focus on developing culturally sensitive measures and providing psychoeducation to improve symptom recognition. Finally, we adapted the illness perception scale and help-seeking scale into the context of IGD without formal validation. Moreover, we assessed the participants’ intention in a hypothetical context of having IGD. Thus, future studies should well validate these scales and confirm these findings in the sample of patients with IGD.
Conclusion
These findings contribute to the growing body of literature on eHealth literacy and IGD, highlighting the multifaceted impact of digital health competencies on young people’s IGD symptoms and attitudes toward seeking help for IGD. By elucidating the indirect pathways through which eHealth literacy influences help-seeking intention, this study underscores the potential of integrating eHealth literacy interventions in university health promotion frameworks to promote proactive help-seeking behaviors and prevent IGD symptoms among Internet gamers.
Particular intervention efforts and attention should be paid to males and those with higher education levels to prevent the development of IGD. Those with lower education levels who spend more hours on Internet gaming may have lower intentions for help-seeking and could benefit from targeted interventions and support strategies aimed at addressing their specific needs and challenges.
Due to deep-seated cultural stigma surrounding mental health issues in Hong Kong and resource constraints within university counseling centers, future efforts should focus on embedding eHealth literacy seamlessly into the academic curriculum, utilizing peer educators to reduce stigma, and securing top-down administrative endorsement to legitimize and fund these essential health initiatives.
Footnotes
Ethical Considerations
The study procedures were carried out in accordance with the Declaration of Helsinki. The Institutional Review Board of the Chinese University of Hong Kong approved the study (Ref.#023-24). All subjects were informed about the study, and all provided informed consent.
Author Contributions
XY: Conceptualization, writing, data analysis, data collection; QW: Writing, data analysis; LZ: Review.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Health and Medical Research Fund of Hong Kong #20210481 and #08230058.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.