
Abstract
This research note analyzes the relationship between language use and children’s Body Mass Index (BMI) growth in the United Kingdom. Making use of the Millennium Cohort Study (MCS), we assess whether the main language spoken in the household explains BMI divergences between immigrants’ and natives’ children. We provide evidence that the integration process hampers BMI growth and therefore exerts a small protective effect: male children living in English-speaking households gain weight slower than those with less integrated parents. However, the protective effect applies only to sons from higher social origins.
Introduction
Childhood obesity has been on the rise all over the world during the past 30 years (NCD-RisC 2017) with important implications for health inequalities. The Body Mass Index (BMI), defined as the weight in kilograms divided by the square of the height in meters, is a universal anthropometric indicator for classifying overweight and obesity (World Health Organization 1995). Higher BMI levels during childhood increase the probability of becoming an overweight or obese adult, which in turn is associated with cardiovascular diseases, type-2 diabetes, muscular and skeletal pathologies, and tumors (Guo et al. 2002). Additionally, being overweight may influence self-esteem and social skills, as people in this condition are often discriminated against in schools and, subsequently, at work (Puhl and Heuer 2009).
In the United Kingdom, around a third of children aged two to 15 years old are overweight or obese (National Health Service 2017). Although childhood obesity seems to have reached a plateau in Britain, BMI levels and trajectories are strongly influenced by social origins (Stamatakis, Wardle, and Cole 2010). In addition to socio-economic and biological factors (Della Bella and Lucchini 2015), studies find that parents’ migration status is a significant factor (Johnson, Wright, and Cameron 2012; Sardadvar 2015): in both the United States and the United Kingdom, children of ethnic minorities are more likely to suffer from this condition (Brophy et al. 2009; Zilanawala et al. 2015). For this reason, children of migrants are at an increased risk of experiencing physical and mental health issues associated with overweight and obesity in their adult life.
A plausible explanation of this difference may lie in the downsides of the integration process. Although integration is usually associated with positive labor outcomes such as higher earnings and better employment chances (Chiswick 1978; Fellini and Guetto 2018), adverse effects on health have been observed. Several studies show that in many places, immigrants abandon healthier eating habits and beneficial traditional diets in favor of processed and energy-dense food easily available in the destination country (Gorman, Novoa, and Kimbro 2016). This practice, in addition to lower levels of physical activity and stress caused by having to integrate into a new country, might explain immigrants’ progressive convergence, over the life course, toward natives’ obesity rates (Riosmena et al. 2015). Analogously, a higher incidence of obesity may be reported among second- and third-generation immigrants when compared to their first-generation counterparts and to natives. In fact, the assimilation of obesity-related behaviors by parents could translate into unhealthy eating habits and sedentary lifestyles for the whole family, which are in turn associated with higher BMI in children.
Extant evidence seems in line with this hypothesis. The incidence of overweight and obesity among children of Latino and Asian immigrants in the United States increases with the length of residence and the ability to use natives’ language (Gordon-Larsen et al. 2003; Bates et al. 2008; Park et al. 2009). Similarly, Allen et al. (2007) find that first-generation adolescents from both Mexico and Asia have healthier diets than their American counterparts but that this advantage erodes, and is even reversed, when looking at second- and third-generation immigrants.
Crucially, however, the integration process varies depending on children’s gender and parental socio-economic status. Available evidence in the United States indicates that the harmful effects of integration are most evident among males, since less integrated parents across ethnic groups tend to be more permissive and indulgent to boys when it comes to eating habits (Van Hook and Baker 2010). Concurrently, some studies underline the importance of considering how immigrant families’ socio-economic status can mediate some negative health implications of integration: for instance, in the United States, more affluent immigrant families seem able to buffer their children from host country unhealthy habits (Van Hook and Stamper Balistreri 2007; Martin, Van Hook, and Quiros 2015).
Yet depending on the context, the adaptation process might also be beneficial and protective: immigrants could start adopting healthier eating habits or simply receive information on salubrious practices through health promotion programs or through their children (Morales and Hanson 2005; Esteban-Gonzalo et al. 2015). However, since most studies to date tend to be adult- and US-centered (Van Hook and Stamper Balistreri 2007; Van Hook and Baker 2010; Martin, Van Hook, and Quiros 2015), we still lack an examination of children’s BMI trajectories in other countries.
Research Questions and Hypotheses
This study’s primary goal is to analyze the BMI growth curves of immigrants’ and natives’ children in the United Kingdom from early childhood to adolescence, for boys and girls, respectively. We examine whether these patterns of growth are different, what effect language spoken at home has on the BMI trajectories, and how language interacts with parental socio-economic status. Although the focus on language does not capture the many nuances that characterize the integration process (e.g., beliefs, attitudes, and behaviors), the single-element approach has the advantage of offering analytical insights on the possible mechanisms through which language itself operates (Zane and Mak 2003; Abraído-Lanza et al. 2006).
Three sets of hypotheses guide our work. First, since it is widely acknowledged that children of immigrants are at a higher risk of overweight and obesity than their native counterparts (Labree et al. 2011), we expect that children of immigrants tend to gain BMI more rapidly than do children of natives (H1).
Second, we surmise two contrasting hypotheses regarding the effect of language use. On the one hand, in line with some evidence gathered in the United States (Van Hook and Baker 2010), we might expect that children of immigrant parents who are more integrated to the UK context gain BMI more quickly than do the children of natives and less-integrated parents (H2a). This expectation implies that the adaptation process impinges negatively on the health habits of immigrants’ children over time. On the other hand, and in line with some evidence gathered in Europe (Esteban-Gonzalo et al. 2015), it is also possible that integration has a protective effect because parents and children acquire information on the beneficial aspects of healthy behaviors for counteracting BMI gain over time. Thereby, we might expect that children of immigrant parents who are more integrated to the UK context gain BMI more slowly than do the children of less integrated parents and have BMI gain rates more similar to those of the children of natives (H2b).
Finally, we concentrate on the role of parental socio-economic status as a possible moderator of the integration process and test whether the size and direction of the effect depend on the mother’s educational level. In line with previous contributions (Martin, Van Hook, and Quiros 2015), we suppose that children of immigrant parents who are more integrated in the UK context and come from a more advantaged socio-economic background gain BMI more slowly than do the children of less integrated parents and similarly integrated parents with lower socio-economic status (H3).
Data and Methods
The data used in the analysis come from the Millennium Cohort Study (MCS), a nationally representative longitudinal survey following the lives of around 19,000 children born in the United Kingdom between September 2000 and January 2002. The sample has a probability design and is clustered at the electoral ward level. Disadvantaged residential areas and areas with a high proportion of ethnic minority groups are overrepresented to better identify the effects of disadvantage and ethnic diversity on children’s outcomes.
Six sweeps have been conducted hitherto: the first wave (MCS1) was carried out when the children were around nine months old, and data collection was subsequently repeated around the age of three, five, seven, 11, and 14 years old. Although time-invariant information on parental and household background at child’s birth was retrieved from sweep 1, our analysis is based on child anthropometrics from sweeps 2 to 6. Data were collected through home interviews with the main caregiver, usually the mother. The final unbalanced sample consists of around 13,558 cases.
Variables
The main outcome of interest for our analysis is BMI. BMI scores are calculated using the height and weight measurements collected by interviewers using a set of Tanita scales (Calderwood et al. 2014). Prior research on child obesity identifies BMI as a suitable obesity index for children (Poskitt 2007; Van Hook and Stamper Balistreri 2007), since height and weight are easy to obtain with a reasonable degree of accuracy. Raw BMI scores are considered instead of BMI z-scores. We used the raw BMI score as a dependent variable because compared to its z-score, it is better suited to analyze BMI changes over time, as within-child variability depends on the child’s initial obesity level (Cole et al. 2005). In line with previous research (Gordon-Larsen et al. 2003; Van Hook and Stamper Balistreri 2007), we distinguish between children of natives and children of immigrants. The latter group corresponds to children who have at least one foreign-born parent. The survey provides very limited information about each household member’s language use and ability. Thus, we measure language use through a variable reporting the language most frequently spoken at home, distinguishing between households of natives, non-natives speaking English, and non-natives speaking a different language. 1
We included several socio-economic and demographic characteristics at the time of the first interview (2001), which may be associated with children’s BMI growth (Boone-Heinonen et al. 2016): sex, age, type of family (both natural parents, single mother), mother working status and education level (low, medium, and high), and household annual income quartiles. To account for the biological component (Della Bella and Lucchini 2015), we control for the mother’s BMI before childbirth. To address ethnic differences in BMI, we consider the cohort member (CM) ethnic group. The categories are defined by mothers’ reports of children race/ethnicity and are based on the 11 ethnic categories defined in the UK census. The classification used for the analysis is obtained by aggregating such categories into four groups: white, Asian, black, and mixed. Descriptive statistics of the variables included in the models are reported in Supplemental Tables S1, S2, and S3 (available in the online version of this article).
Empirical Strategy
We estimated growth curve models of children’s BMI. Given the employment of longitudinal data, the units are observed at multiple points in time with data on height and weight collected repeatedly across surveys since sweep 2. In general, growth curve models allow us to identify how outcomes for person j at period i are determined as a function of the sample mean (β), a residual component specific to each individual and constant across periods (φ i ) and a component specific to each subject at each time period (∊ ij ) (Macmillan and Furstenberg 2016).

The models simultaneously estimate effects for Level-1 units (the multiple observations for each child across age) and Level-2 units (the children). The Level-1 model fits BMI as a function of age across the time observations for each child. Starting from the baseline model in equation (1), we add covariates to the part of the model predicting the intercept (i.e., the initial BMI and/or the predicted change in BMI over time). To test whether child BMI growth patterns vary with parental migration status (H1), we estimate the following model:

where
Second, we test whether language spoken at home exerts a detrimental (H2a) or protective (H2b) effect on boys’ BMI growth. The specification of the model is as follows:

Finally, to test H3, we include an interaction term between language spoken at home and parental socio-economic status (i.e., mother’s educational level 2 ) to assess whether the magnitude and direction of the language use coefficient vary accordingly:

Results
BMI Growth Curves and Language Use
The hypothesis of heterogeneity in BMI growth patterns between children of immigrants and natives is corroborated by the estimates presented in Table 1 (see Supplemental Table S4 for the full model, available in the online version of this article). The growth trajectories identified by the models are coherent with those estimated by Stuart and Panico (2016), who studied socio-economic patterns in childhood obesity trajectories using the same data source. We observe that the BMI of children of immigrants rises at a faster rate with respect to the BMI of their native counterparts, starting from early childhood and continuing more intensively during preadolescence and adolescence. Parental migration status has a positive and significant effect on children’s BMI at subsequent time points (model 1). Children of immigrants report slightly higher BMI from the age of five on, but the magnitude of the divergence between the two groups increases over time. The results from the full sample are more noticeable when estimating the growth curves only on the male subsample. Table 1 reports BMI trajectories separately for male and females. To help interpret these findings, we generated predicted values of children’s BMI over time. The significant discrepancy in the two groups’ BMI increases when considering boys only (model 2): at the age of 14, the predicted BMI of children of immigrants is 0.9 percent and 1.96 percent higher than that of their native counterparts in the full sample and among males, respectively. On the contrary, no statistically significant difference is reported between the growth curves of the two groups in the female subsample (model 3). Therefore, it turns out that parental migration status plays a role in defining growth trajectories exclusively among boys.
Growth Curve Models of Body Mass Index (BMI).
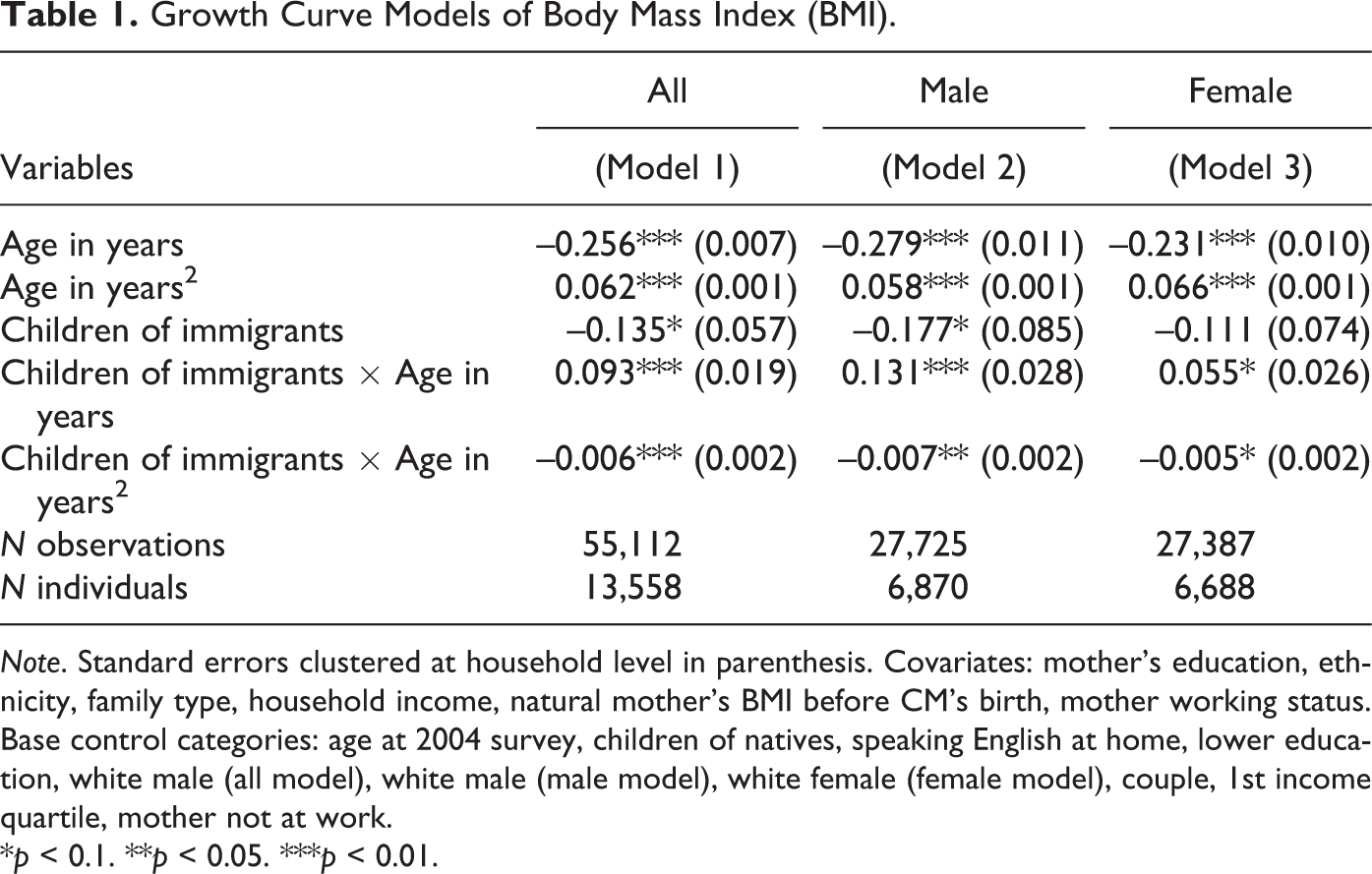
Note. Standard errors clustered at household level in parenthesis. Covariates: mother’s education, ethnicity, family type, household income, natural mother’s BMI before CM's birth, mother working status. Base control categories: age at 2004 survey, children of natives, speaking English at home, lower education, white male (all model), white male (male model), white female (female model), couple, 1st income quartile, mother not at work.
*p < 0.1. **p < 0.05. ***p < 0.01.
Figure 1 presents the growth curves based on equation (3), therefore examining the role of language use on children’s BMI growth. The estimations confirm that the BMI levels of children of immigrants converge toward those of children of natives when the family speaks English as the main language. The predicted BMI of children aged 14 and living in households speaking English is the same as that of natives, while the BMI of those speaking other languages is 2.64 percent larger. These findings support hypothesis H2b: in contrast to H2a and the evidence gathered in the United States, speaking English in Britain is not associated with BMI growth.
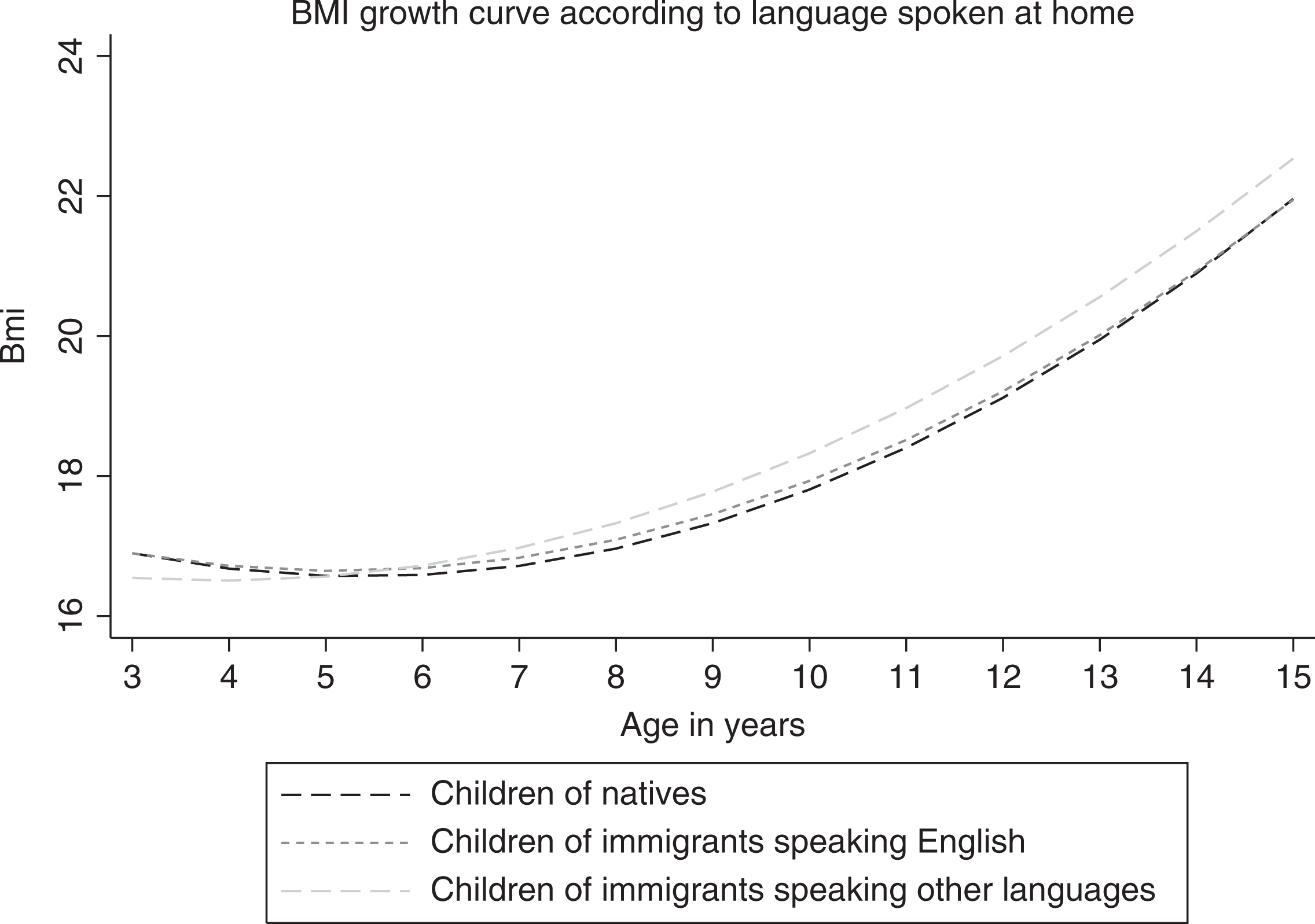
BMI growth curve according to language spoken at home.
Finally, the last model indicates that these patterns vary across socio-economic status and corroborates previous findings on the mediatory role of families’ resources on the integration process (Van Hook and Stamper Balistreri 2007; Martin, Van Hook, and Quiros, 2015). Figure 2 illustrates how growth curves of the sons of immigrants differ when considering the interaction between language use and mother’s educational level. The BMI of children of immigrants speaking English with high-educated mothers tends to grow significantly less compared to all other children of immigrants. This finding implies that language skills exert a protective effect only for children of immigrants with higher socio-economic background, who tend to converge toward the trajectories of children of natives. On the contrary, children’s BMI in English-speaking families with lower educational resources grow similarly as the BMI of children of immigrants speaking another language.
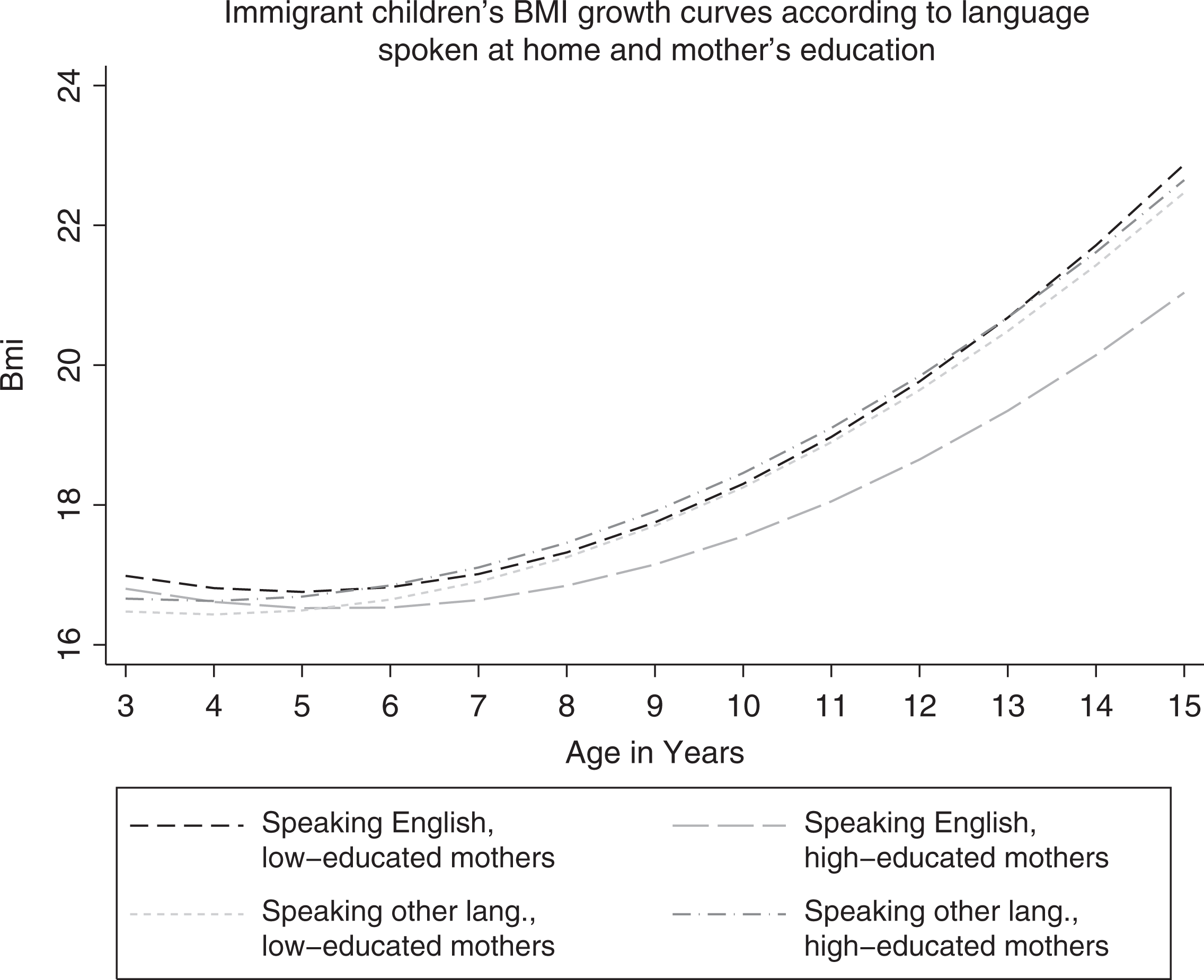
Immigrant children’s BMI growth curves according to language spoken at home and mother’s education.
Discussion
Understanding the determinants of children’s obesity and how their trajectories change over time is of extreme importance for the implementation of effective public policies. Childhood obesity is a critical condition that impinges negatively on future health chances by increasing the risk of several diseases and tumors (Guo et al. 2002; Puhl and Heuer 2009). Despite the fact that much has been done to prevent obesity among children, inequality still depends on their social origins. Apart from the well-known relation between the familial socio-economic gradient and children’s obesity level, parental migration status is a relevant force at play. Research has shown that BMI growth patterns of immigrant adults and their children are shaped by the degree of integration into the destination country. Yet the social determinants of children’s BMI development over time are still understudied, especially in a European context (e.g., Van Hook and Baker 2010). In this light, our research note provides a first attempt in this direction by focusing on the UK context.
Three main conclusions are in order. First, in line with the existing literature (Labree et al. 2011), our findings indicate that children of immigrants gain BMI faster than children of natives. However, once we distinguish our results by gender, we find the effect to be significant only among boys. This result replicates that of Van Hook and Baker (2010), who find that in the United States, boys, but not girls, of immigrant families gain weight more rapidly than natives. Although in the first wave their BMI is similar to that of their native counterparts, by the age of 14, this relation is overturned. Later waves will shed light on the evolution of the trend, suggesting that differences in BMI growth curves amplify during late adolescence. The gender difference we see, however, may be due to several causes and deserves serious investigation. As a tentative interpretation, one may follow Van Hook and Baker’s (2010) line of reasoning, suggesting that due to immigrant families’ beliefs on gender roles, boys enjoy more freedom than girls, and parents tend to be more permissive with the former when it comes to food consumption.
Second, our findings contradict most of the US literature on the harmful health effect of integration. The effect of language spoken at home indicates that the BMI growth of the sons of immigrants is hampered in English-speaking households. This result gives further support to the findings of Esteban-Gonzalo et al. (2015), who identified a protective effect of length of stay on immigrant adolescents’ weight and eating habits in Madrid. Possibly, immigrant parents who become acquainted with the UK context have easier access to information on healthy behaviors and salubrious food. Speaking English or simply more knowledge of the UK context might improve communication with primary school teachers or medical professionals that suggest best food practices (Katz et al. 2011; Steele et al. 2011); concurrently, parents could more easily read commercial food ingredient labels and limit the presence of energy-dense meals or junk food (Vahabi and Damba 2013). In any case, integration appears to be a desirable outcome for preventing BMI growth among children of ethnic minorities and for reducing health inequalities between immigrants’ and natives’ children.
Finally, in line with other studies (Martin, Van Hook, and Quiros 2015), we highlight that integration is not a homogenous process for all immigrant children but differs depending on their socio-economic background. Crucially, the interaction between language spoken at home and maternal education shows that the protective effect holds only for children with tertiary-educated mothers. Understandably, cultural resources may ease the adaptation process and facilitate the acquisition of health literacy and values that drive food choices and compliance to dietary advice (Abel 2008; Oncini and Guetto 2017, 2018).
In a policy perspective, it may be suggested that stronger efforts should be made to inform newly arrived immigrants, and especially their preadolescent sons, about best practices on good nutrition and physical activity. For instance, portion information on packaging could be translated in other languages, whereas energy-dense food products could contain easily recognizable warnings on the negative effect for health and BMI growth. Similarly, interventions within and beyond schools could better target those most in need of advice and jointly involve families and children in health promotion programs (Wills, Danesi, and Kapetanaki 2016; Oncini 2017).
Some limitations of this contribution should nevertheless be addressed. First, language spoken at home may not directly reflect each household member’s language proficiency. More specific information on reading and writing skills, attendance of language courses, and language use outside domestic surroundings would provide a more comprehensive and accurate measure of parental language ability and use, although this information is not available in the data.
Second, the use of language as a main independent variable is problematic itself, since it is a one-dimensional indicator of the complex and debated integration process. This measure is questionable in many ways, since it does not allow us to disentangle different facets of the phenomenon, such as cultural maintenance and acquisition, and says nothing about the mechanisms underlying the relation between integration and health (Doucerain, Segalowitz, and Ryder 2016). For instance, this approach impedes the evaluation of the mediatory role that language skills might have in accessing information on best health practices. Future research could certainly benefit from the collection of measures reflecting different dimensions of the integration process (Abraído-Lanza et al. 2006) as well as specific variables associated with health behaviors, such as food consumption and type of cuisine, the frequency of contacts with health specialists, and parent’s beliefs on gender roles.
Third, although the use of longitudinal data is helpful for describing BMI patterns of growth, here we do not make use of time-variant information that might unveil causal mechanisms behind trajectory changes. 3 Ideally, one would like to have time-variant information on family eating practices so as to capture more precisely how integration, food consumption, and BMI trajectories interrelate.
Finally, the sample size does not allow us to assess whether the relation between language and BMI trajectories differs across ethnic groups or nationalities. Consequently, we cannot fully ascertain to what extent language use’s overall protective effect is solely driven by the characteristics of the host country or by the composition of the immigrant population in the United Kingdom.
We conclude with a suggestion for future research developments. Comparative studies, or at least studies in countries and continents beyond North America and Europe, are needed to test how BMI growth curves vary depending on parents’ background as well as on the cultural and institutional characteristics of the context. Cross-country variations in the quality of available food, in public expenditure for health campaigns, or in fiscal measures against energy-dense products might unveil how different factors affect the integration process and help develop more effective policies against childhood obesity.
Supplemental Material
Supplemental Material, MRX798336_Supplemental_Material - Language Use and Children’s BMI Growth among Second-Generation Immigrants in the United Kingdom
Supplemental Material, MRX798336_Supplemental_Material for Language Use and Children’s BMI Growth among Second-Generation Immigrants in the United Kingdom by Sara Giunti and Filippo Oncini in International Migration Review
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.