
Abstract
In this descriptive study, we analyzed survey data regarding communication, instruction, and assessment strategies school personnel in K-12 settings reported using during the COVID-19 pandemic for students with emotional and behavioral disorders (EBD). Results indicate, whether instructional continuity was mandated or not, support personnel serving students with EBD reported using a variety of communication, instruction, and assessment strategies. Several strategies special educators reported using were significantly different than those provided by related service providers (e.g., school psychologist, counselor) during school site closures. Implications for future planning, policy, and research are discussed.
Keywords
Nationally, students with disabilities make up 14% of the student population (National Center for Education Statistics, 2019) with 5% of all students with disabilities (i.e., 353,000 students) receiving special education services under the Individuals with Disabilities Education Act (IDEA) disability category of emotional disturbance (National Center for Education Statistics, 2020). An even greater number of Grades K-12 students exhibit emotional or behavioral disorders (EBD) for which they may or may not receive services under other categories (Forness et al., 2012; Landrum, 2017). Researchers in special education and childhood mental health have spent decades examining the effectiveness of practices that target the social, emotional, and behavioral needs of students with EBD (Lloyd et al., 2019). In addition to academic supports, students with EBD who have individualized education programs (IEPs) receive intensive, individualized behavior interventions and support plans. These interventions, which are often based on functional behavior assessments (Cooper et al., 2020), are applied systematically and assessed continuously. Evidence-based behavior interventions may include, but are not limited to, explicit instruction in replacement behaviors (Hirsch et al., 2020), social skills (Gresham & Elliott, 2014), and self-determination skills (Carter et al., 2011); preventive, antecedent-based strategies to improve the classroom environment; consequence-based strategies such as reinforcement; and mental health counseling. As part of the ongoing assessment process to determine if students are progressing toward their behavioral goals and responding to these interventions, data are collected on a regular basis (e.g., daily, weekly). Frequently, assessment data include direct behavior ratings, indirect rating scales, or systematic direct observations (Bruhn et al., 2020). Interventions and assessments are typically managed by special education teachers (SETs) who oversee the IEP and consistently have direct contact with students daily. They are supported by related service providers (RSPs) such as school psychologists, counselors, social workers, behavior specialists, and therapists (e.g., speech, occupational, physical), who may provide more specialized services on a less frequent basis.
Despite having the aforementioned specialized services in place, students with EBD are significantly more likely to be suspended, expelled, and arrested than their peers without IEPs and with IEPs for other disabilities (Lipscomb et al., 2017). These students have the highest dropout rate and lowest graduation rate among all students with any disability (Lipscomb et al., 2017). While the field has identified effective instructional and behavior change strategies for students with EBD (Mitchell et al., 2019); a continuum of risk factors continue to disenfranchise these students. For instance, they are among the most socioeconomically disadvantaged groups of students, with 62% living in low-income households, only 22% having a parent with a college degree, and 33% attending a low performing school (Lipscomb et al., 2017). Under normal circumstances (i.e., outside of the context of a pandemic and the subsequent psychological and physical adversity arising from this type of disruption), these statistics would be alarming. However, in March of 2020, a pandemic was declared which resulted in school site closures; prolonged and serious illness, death, unemployment; and pervasive mental health issues, thus potentially exacerbating the risk factors experienced by students with EBD.
Research has shown that exposure to psychological (e.g., death of a loved one, isolation) and physical adversity (e.g., losing a home, food deprivation, illness) caused by a disaster can lead to EBD or EBD-like risk (e.g., severe disruptive behaviors, mental health issues; McLaughlin et al., 2009). Collectively, this research along with the documented negative outcomes for students with EBD, underscored the concern for this high-risk population as schools began to close in March 2020 due to the COVID-19 pandemic. As such, understanding the supports and services students with EBD received during COVID-19 related school site closures is an urgent matter, as the potential for damaging, long-term, pandemic-related effects are likely imminent absent any mitigation strategies—including the provision of remote instruction and intervention. Further, most attention related to school-age children has focused on the physical effects of COVID-19, while insufficient attention has been paid to social, emotional, and behavioral needs exacerbated by the pandemic (Aishworiya & Kang, 2020). At the same time, few studies related to the initial stages of the COVID-19 pandemic, have exclusively focused on students with EBD. Thus, we conducted a regionally diverse survey to examine the social, emotional, and behavioral supports and services delivered to students with EBD during the initial school site closures in the spring of 2020. Given these students typically receive services from multiple providers including SETs and RSPs, we hypothesized responses about services would vary depending on the respondent’s role. We supported our hypothesis by previous research studies related to SETs experiences working with students with EBD (Bettini et al., 2019) as well as recent research related to therapy services for children with disabilities during the initial phase of the pandemic (Murphy et al., 2021). In addition, we recognized access to technology and school policy on remote learning varied across the country and thus may have impacted the types of services students with EBD received. We address these issues in the following sections.
School Policy and Technology
As students were homebound from March 2020 until the end of the school year, one of the most important decisions schools and districts had to make was whether to provide remote instruction (also known as online, or distance, learning) to students, and whether instruction should be mandatory or optional. In cases of optional learning, students may have been provided materials (e.g., workbooks, laptops), subscriptions to online programs (e.g., Lexia®, DreamBox™®), and then given the option to complete activities or attend synchronous, online meetings, though no systematic instruction nor feedback was provided, and no attendance and grades were recorded. With mandatory learning, however, students were required to complete assigned work and grades and feedback were provided. Instruction may have been synchronous, asynchronous, or a combination. While the decision to transition to online learning was likely impacted by myriad factors (e.g., evolving scientific knowledge of the virus; federal, state, and local guidance). A report by Reich and colleagues (2020), note policies were likely influenced by factors such as remote learning support, equity, and attending to student needs (i.e., students with disabilities).
Specifically, the Individuals with Disabilities Education Improvement Act (IDEA; 2004) legally mandates schools to implement students’ IEPs when schools are open. The U.S. Department of Education, the Office of Civil Rights, and the Office of Special Education and Rehabilitative Services issued multiple statements in March and April of 2020 clarifying compliance with the law (i.e., IDEA) should not preclude schools from offering online educational programming (U.S. Department of Education, 2020). In addition, Secretary of Education DeVos stated on April 27, 2020, that she did not recommend Congress pass waivers that would allow schools flexibility in meeting the legal requirements of IDEA (DeVos, 2020). The implication, then, was that if schools elected to mandate remote learning (essentially opening schools virtually), then students with disabilities must receive the services outlined in their IEPs. Failure to provide services laid out in the IEP could result in lawsuits against states and districts (Jones et al., 2020). We hypothesized that SETs and RSPs working in schools where remote instruction was mandated would be more likely to be implementing evidence-based interventions and conducting assessments as required by the legally-binding IEP. Whereas, in schools where online instruction was optional (essentially meaning the school was closed), SETs and RSPs would not have been required by law to deliver any components of the IEP, perhaps then, making them less likely to do so.
A second major factor related to remote learning policies is technology access (Williamson et al., 2020). Districts had to determine if they had sufficient technological resources (e.g., hardware, software, internet connectivity) to deliver remote instruction. These difficult decisions may have been especially impactful for students with disabilities who require specialized instruction (Kamenetz, 2020). As schools moved to remote learning, the IEP provision of services to students with disabilities could have been hampered by technology barriers (i.e., lower bandwidth, lack of access to appropriate devices), further exacerbating the digital divide between students who do and do not have adequate technology (Kormos, 2018; Williamson et al., 2020). Recent reports have highlighted the technological disparities, particularly in rural communities, that students have faced during the pandemic (Jameson et al., 2020), with some educators reporting they resorted to using the telephone (Nadworny, 2020) or dropping off materials at campus sites for pick-up (Shah, 2020) as computers and internet connectivity were unavailable. If students in a district did not have access to computers (e.g., one-to-one devices provided by the district) and consistent, broadband internet service, then it is logical that these schools and districts would have adopted an optional (rather than mandatory) remote learning policy. As such, we hypothesized that respondents under mandatory remote learning policies were more likely to communicate with their students using platforms that required a computer and internet (e.g., virtual classrooms, email, social media), whereas optional policies may have led to communication via telephone (e.g., Nadworny, 2020).
Purpose
School site closures associated with COVID-19 resulted in a major shift in how educational services were delivered to students. The degree to which schools shifted to online instruction was reflected in their remote learning policy and their use of technology. The impact of this shift may have been experienced most deeply by students with EBD, as the majority of evidence-based interventions for students with EBD are designed to be implemented (a) in person, (b) in a school setting, (c) in real-time, and (d) by a trained practitioner; not via the computer asynchronously or the telephone at home (Kamenetz, 2020; Wagner & Newman, 2012). Given the varied school policies on remote instruction, the reliance on technology for delivering instruction and intervention during school site closures, and the vulnerability of students with EBD, we surveyed SETs and RSPs who were serving students with EBD in spring 2020 at the onset of the pandemic. The term EBD was used throughout the survey and defined as “students with emotional disturbance, emotional/behavioral disorders, or have behavior goals (for non-categorical states” (EBD Pandemic Survey, S. M. McDaniel et al., 2020).
The purpose of this study was to gather information about the extent to which these educators (i.e., SETs and RSPs) delivered the various supports and interventions delineated in students’ IEPs during school site closures. Within the context of the COVID-19 crisis, there are little data available on the experiences of SETs, particularly related to supporting students with EBD. To support educators by leveraging school resources in future emergency school site closures, more data are needed. Therefore, we examined responses based on the provision of optional or mandatory remote instruction (dictated by district policy) and based on their role (e.g., SETs, RSP) during initial school site closures in spring of 2020. With the continued spread of COVID-19 and without immediate, reliable access to a vaccine, this study has implications for policy and practice for current and future crises that threaten the continuity of school-based services. We address the following research questions:
What is the most common method respondents reported using to communicate with students with EBD during school site closures? Were there differences by remote learning policy (e.g., optional, mandatory) or role (e.g., SETs, RSP)?
What intervention strategies for students with EBD did providers report implementing during school site closures? Were there differences by remote learning policy (e.g., optional, mandatory) or role (e.g., SETs, RSP)?
What assessment and progress monitoring data were collected for students with EBD during school site closures? Were there differences by remote learning policy (e.g., optional, mandatory) or role (e.g., SETs, RSP)?
Method
Respondents and Recruitment
Following Institutional Review Board approval, we used snowball sampling methods to recruit the largest number of respondents in the shortest amount of time; our goal here was to capture service-providers’ perspectives and to mitigate the extent to which they would have to recall their actions after the fact (Dillman et al., 2014). We sent approximately 130 emails containing a link to the survey to known contacts in the field of education (e.g., professors, administrators, special education teachers, related service providers). Primarily, emails went to known school administrators and special educators, followed by university instructors, and least often to related service providers. These contacts were known through previous research or service collaborations, technical support provided, and personal contacts in the field of education. The emails contained a link to the survey that the recipient could use to access and complete the survey if they were a SET or RSP or, if they served in another role, could share with eligible respondents. In addition, we posted a link to the survey on personal and professional social media platforms such as Facebook and Twitter accounts and larger groups within these platforms (e.g., Facebook group “Teaching During COVID-19” with 140,000 members). Emails and posting occurred on a variable interval schedule for 52 days (April 30, 2020—June 21, 2020), at which point the survey was closed and no longer accessible. We did not provide financial or other incentives for completing the survey. Though this sampling plan likely affects the precision of estimates and increases the influence of sampling bias (Henry, 1990), we elected to use a convenience sample, due to the urgent and critical need to understand and share supports and interventions provided with limited funding and time. As such, all conclusions should be considered tentative.
In total, we received 596 responses from participants, which included SETs and RSPs (e.g., school psychologists, social workers, school counselors, behavior specialists) working with students with EBD. Of those, we removed four respondents because they were from outside of the United States (e.g., China), 16 who failed to complete the consent form, 78 who answered only the first question, and 28 who completed only the first seven questions (e.g., type of school, location of school community). Thus, the sample size of respondents included in this analysis is 470. Of the 470 total respondents, 397 respondents provided their school or districts current operating policy. Respondents represented 35 states. California, Arizona, South Carolina, and Florida represented the greatest percentage of the respondents (22.1%, 13.3%, 12.5%, and 11.9%, respectfully). Furthermore, though this was not proportional to sample size, all regions of the United States were represented. Our final sample was comprised of 9.3% from the Northeast, 39.0% from the South, 12.2% from the Midwest, and 39.5% from the West. Respondents included 296 special education teachers and 174 related service providers, 420 (89.4%) of whom work in public schools. See Table 1 for demographic information.
Demographic Information.
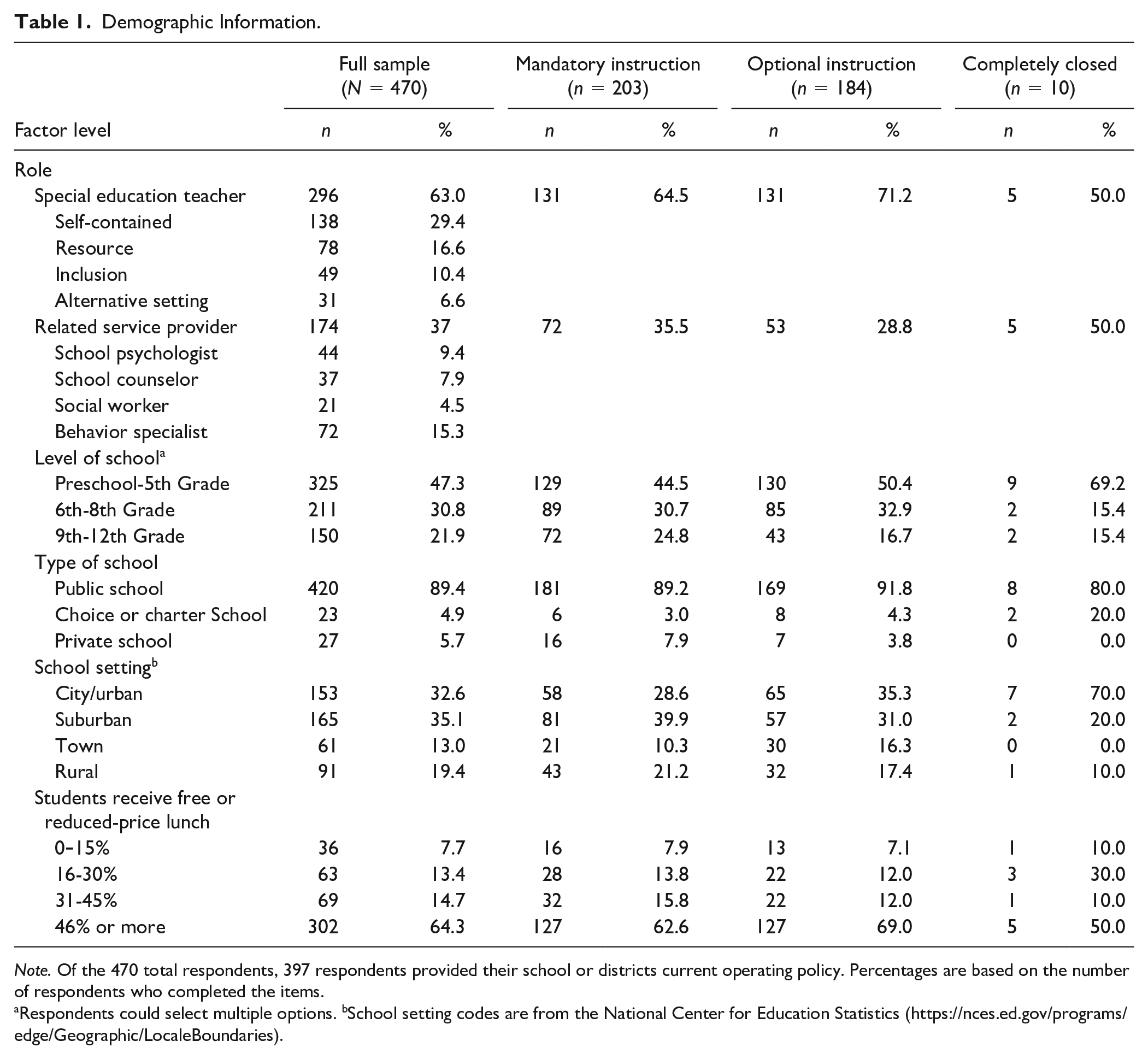
Note. Of the 470 total respondents, 397 respondents provided their school or districts current operating policy. Percentages are based on the number of respondents who completed the items.
Respondents could select multiple options. bSchool setting codes are from the National Center for Education Statistics (https://nces.ed.gov/programs/edge/Geographic/LocaleBoundaries).
Survey Procedures
Development
The purpose of the EBD Pandemic Survey (EBD-PS; McDaniel et al., 2020) was to gather information from SETs and RSPs about the social, emotional, and behavioral supports provided to students with EBD during COVID-19 pandemic-related school site closures in the United States. The unique COVID-19 pandemic introduced unprecedented issues related to service delivery; as such, existing survey measures failed to adequately reflect the unfolding issues faced by educators in providing services to students with EBD. For this reason, we worked collaboratively and with relevant stakeholders to construct a measure that would help us address our research questions.
To develop the survey, the author team who have doctoral degrees in special education and experience developing and conducting surveys (e.g., Bruhn et al., 2014; S. C. McDaniel et al., 2018; Walker et al., 2019) met virtually on multiple occasions to conceptualize the broader purpose of the survey and generate potential survey items that would provide meaningful information relevant to that purpose. Between meetings, authors consulted with two district-level administrators regarding the survey to gather insight regarding the type of information that would be helpful for schools moving forward. After refining the survey, to strengthen face validity, an electronic copy was sent to six administrators, teachers, university researchers, and behavior specialists for a review of content, question structure, response options, and flow. Based on their feedback, we created a final version in Qualtrics (see Appendix A for supplemental materials).
Survey instrument
The finalized survey consisted of 27 questions. Following question one regarding consent, respondents received five demographic questions, five questions regarding their school and/or district (e.g., school type, district enrollment, state, percentage of free or reduced lunch), and 16 questions related to policies and services during COVID-19 related school site closures. These included questions regarding school or district policies and procedures, IEP service delivery, and implementation of social, emotional, and behavioral interventions and collection of assessment data. The survey included fill-in (i.e., type in a number), single-item (i.e., select only one answer), multiple-item (i.e., select all that apply), and scaled response options (i.e., scale of 0–10).
Respondents were asked, “Over the course of COVID-19 school closures, district and state policies have evolved. What is the most recent policy to which you have adhered?” Respondents then indicated if they were (a) completely closed (i.e., no educational services or contact provided to students); (b) offering optional learning opportunities (e.g., instructional resources offered to students, but students not required to use them; no attendance nor assessment); or (c) mandated to provide instruction (e.g., teachers must provide instruction, students must complete assignments, assessments conducted). If respondents answered that they were completely closed, they answered no further content-related questions and were only prompted to provide demographic information; respondents indicating optional or mandatory learning completed all content-related survey questions as well as demographic questions.
Data Analysis
Only data from the survey pertinent to answering the research questions of this study were included in the analysis. For example, data about barriers and facilitators to providing services were not included in this analysis, as they appear in another manuscript (Bruhn et al., 2021). Data were analyzed using SPSS Statistics 26. Prior to analysis, we examined the data for missing responses and outliers and removed incomplete and ineligible responses (see description of respondents). All data were analyzed at the item level; descriptive statistics (frequencies, percentages, mean rates) were calculated for each of the items based on the number of respondents who completed each survey item. All variables were categorical; we conducted chi-square tests for association and independence. Chi-square tests determined whether there were significant differences across the respondents. When significant differences were found, we calculated Cramér’s V (Gravetter & Wallnau, 2013) to measure the effect size of the association.
Results
Communication Resources
When asked to indicate the most common resource used to communicate with students with EBD, 156 respondents (37.9%) indicated virtual meetings (e.g., Zoom™, Facetime®), 103 respondents (24.0%) indicated telephone, 93 respondents (22.6%) indicated virtual classrooms (e.g., Google Classroom™), 51 respondents (12.4%) indicated email, and 9 respondents (2.2%) indicated social media (see Table 2). We conducted a chi-square test of independence between district policy and primary communication method. Two cells related to social media contained cell counts below the minimum of five. We opted to re-run the analysis without social media. There were no changes in significance; for this reason, we report results including social media.
Frequencies and Chi-Square Results for Current School Learning Policy and Primary Communication Method During COVID-19.
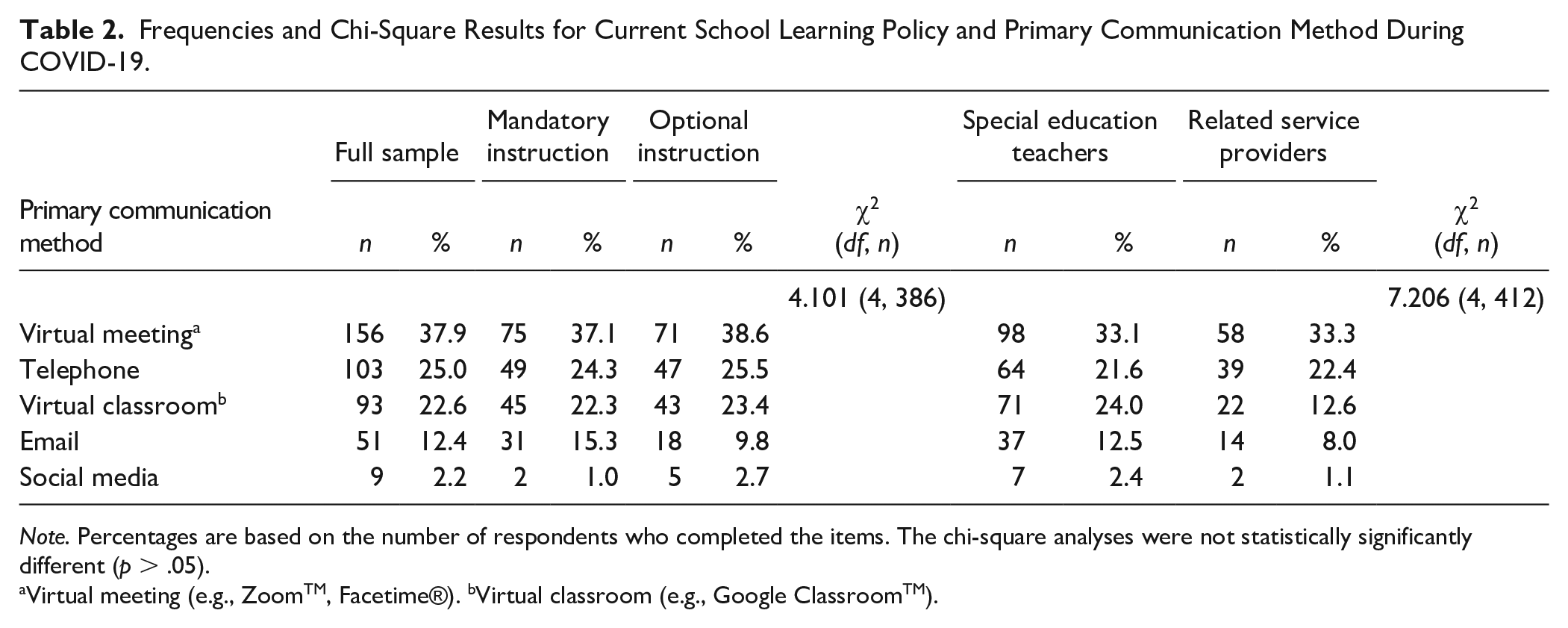
Note. Percentages are based on the number of respondents who completed the items. The chi-square analyses were not statistically significantly different (p > .05).
Virtual meeting (e.g., ZoomTM, Facetime®). bVirtual classroom (e.g., Google ClassroomTM).
When analyzing mandatory and optional instruction, the majority of those who reported mandatory instruction (37.1%) and optional instruction (38.6%) indicated virtual meetings (e.g., Zoom™, Facetime®) as their primary communication resource. Telephone was listed as the second communication resource for both mandatory (24.3%) and optional instruction (25.5%). When analyzing mandatory and optional instruction, all expected cell frequencies were greater than five except for mandatory instruction and social media. There was not a statistically significant association between district policy and communication resources, χ2(4, 386) = 4.101, p = .393.
Provider role was not significantly associated with the method of communication, even when social media was removed χ2(4, 412) = 7.206, p = .125. See Table 2 for details. The majority of SETs and RSPs indicated virtual meetings as their primary communication resource, 33.1% and 33.3% respectfully.
Interventions Strategies
Table 3 and Figures 1 and 2 present information related to strategies respondents reported using during COVID-19 related closures. When asked to select strategies implemented for all students with EBD, 208 respondents (55.2%) indicated checking in on social, emotional, and behavioral needs; 77 respondents (20.6 %) indicated providing structured social skills for all students with EBD; 68 respondents (18.0%) indicated that they implemented prevention strategies; 65 respondents (17.2%) indicated they provided reinforcement strategies; 60 respondents (16.1%) indicated they arranged support from their paraeducator or aide; 55 respondents (14.7%) indicated they used remote counseling or therapy; and 35 respondents (9.3%) indicated teaching replacement behaviors. This suggests that beyond check-ins, most commonly used strategies were not being provided.
Interventions and Strategies Reported by Respondents During Covid-19.
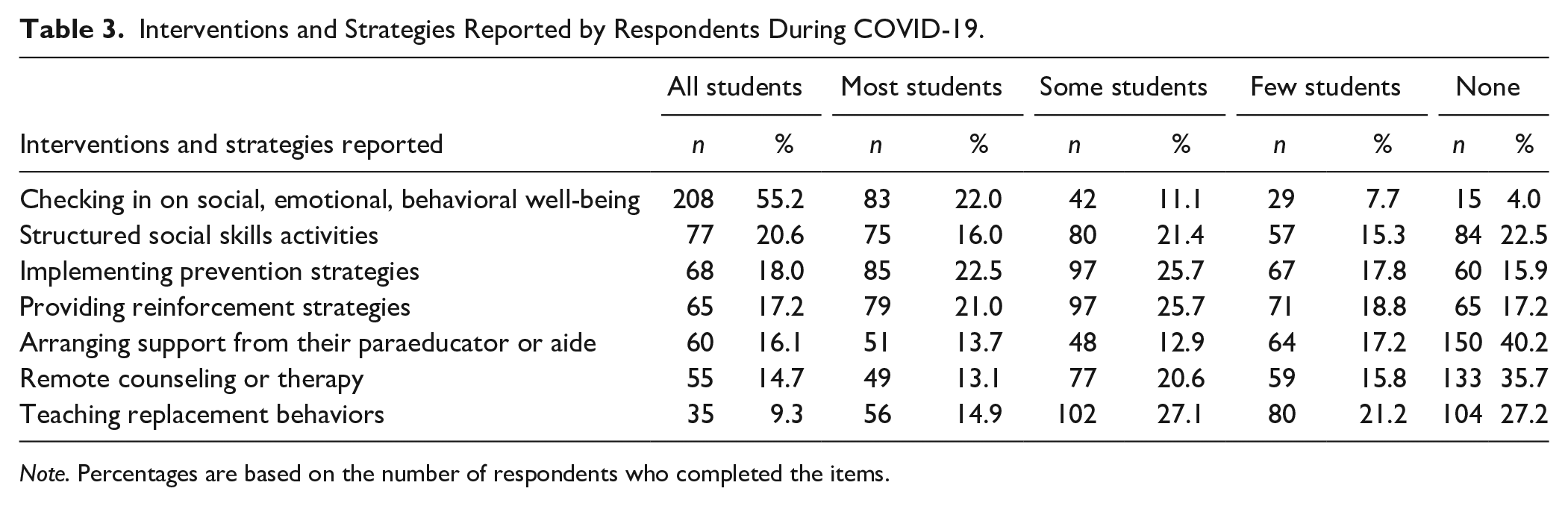
Note. Percentages are based on the number of respondents who completed the items.
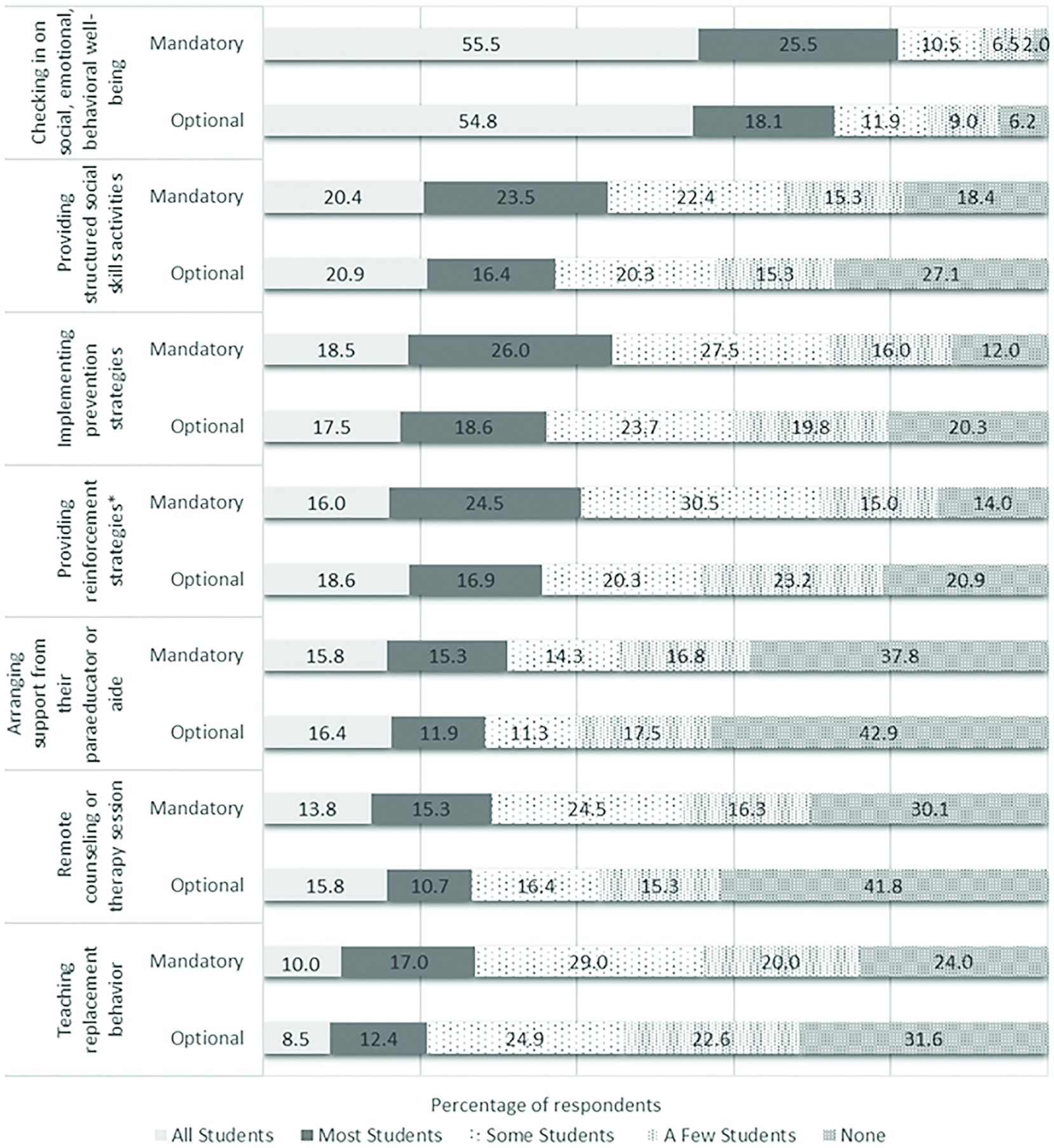
Interventions and supports by district policy during covid-19.

Interventions and supports by provider during covid-19.
Figure 1 presents the strategies implemented by district operating policies. Chi-square tests of independence were conducted between district policy and each strategy. Respondents indicated a significant association between providing reinforcement strategies related to the district policy, χ2(4, 377) = 12.622, p = .013, V = .18. No other intervention strategies were significantly associated with district policy; thus, regardless of school policy, SETs and RSPs reported implementing strategies for students with EBD.
Figure 2 presents the strategies implemented by SETs and RSPs. Chi-square tests of independence were conducted between role and each strategy. Respondents indicated a significant difference on four strategies: (a) checking in on social, emotional, behavioral well-being χ2(4, 377) = 11.836, p = .019, V = .18; (b) implementing prevention strategies χ2(4, 377) = 22.958, p < .001, V = .25; (c) providing structured social skills activities χ2(4, 373) = 9.537, p = .049, V = .16; and (d) counseling or therapy χ2(4, 373) = 9.932, p = .018, V = .18. SETs indicated significantly more of the first three interventions compared to RSPs (i.e., checking in on well-being, implementing prevention strategies, and providing structured social skills activities) and RSPs indicated a significant difference related to implementing counseling or therapy.
Data and Assessment
Table 4 presents the information related to data and assessments. When asked to indicate assessments or progress monitoring data used to evaluate student social, emotional, and behavioral progress during the COVID-19 school site closures, 277 respondents (58.9%) indicated anecdotal parent report, 192 respondents (40.9%) indicated academic work, 189 respondents (40.2%) indicated student self-report, 168 respondents (35.7%) indicated direct virtual observation, 61 respondents (13.0%) indicated progress monitoring tools (e.g., behavior rating), and 47 respondents (10.0%) indicated parent survey measure (e.g., rating scale).
Frequencies and Chi Square Results of Assessment and Progress Monitoring Data for Current School Learning Policy Evaluating Social, Emotional, and Behavioral Progress During COVID-19.
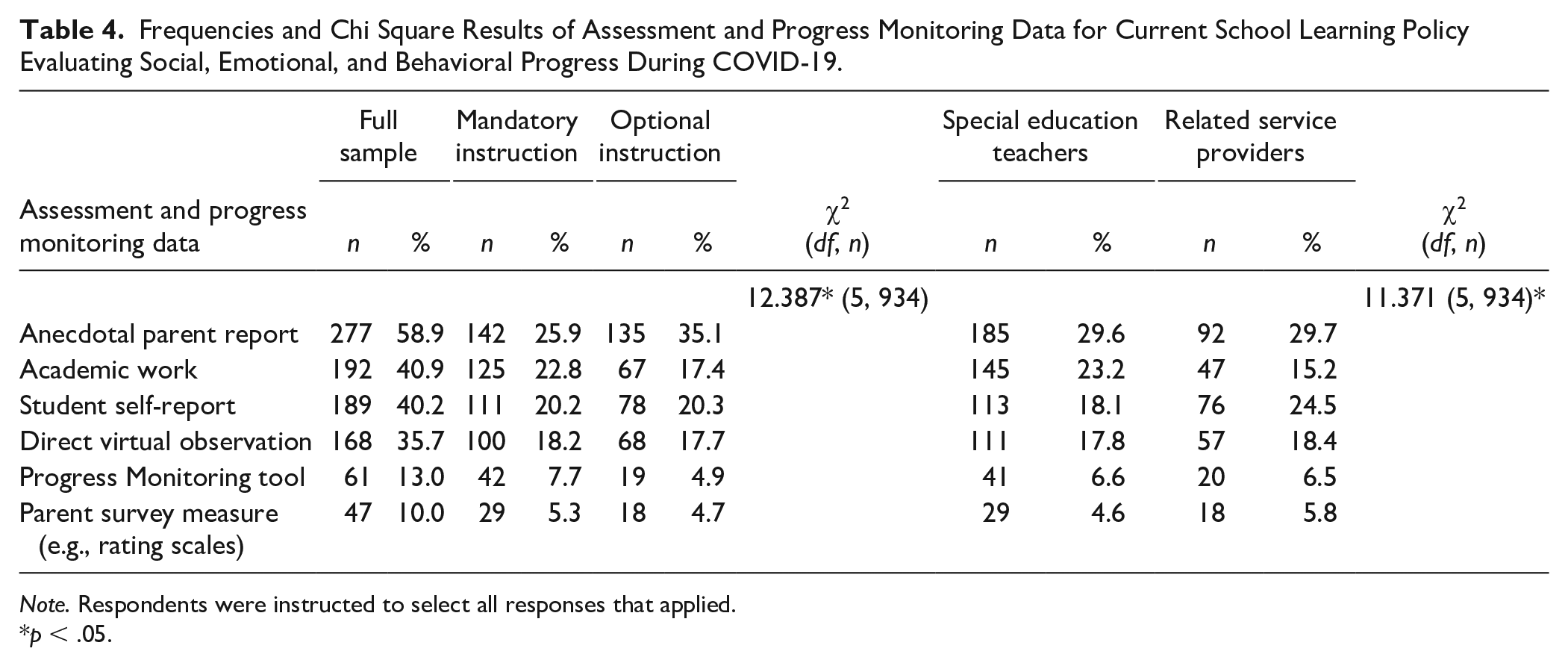
Note. Respondents were instructed to select all responses that applied.
p < .05.
To determine if significant differences existed between schools mandated to provide instruction versus those with optional instructional policies, we conducted a chi-square test for independence. All expected cell frequencies were greater than five. There was statistically significant association between the district policy and use of assessment strategies, χ2(5, 934) = 12.387, p = .03, V = .12; respondents in districts with mandatory instructional policies indicated significantly more assessments compared to districts that used optional instruction. Chi-square tests of independence were conducted between respondent role and assessment strategies. A chi-square test for independence revealed a statistically significant difference between role and assessment strategy, χ2(5, 934) = 11.371, p = .03, V = .11. SETs indicated significantly more assessments and progress monitoring data compared to RSPs.
Discussion
One cannot understate the detrimental impact of COVID-related school site closures on students, and specifically students with EBD (Golberstein et al., 2020). Sadly, as a result of extended school site closures and the shift to remote learning due to the COVID-19 pandemic, students with disabilities are likely to experience significant and pervasive regression (Jones et al., 2020). Given the external risk factors (e.g., poverty, low performing schools), concurrent academic, social, emotional, and behavioral difficulties; and potential outcomes (e.g., suspension, drop-out) students with EBD already face in typical conditions, it is plausible that COVID-19-related regression will be even greater among this population of students (Dorn et al., 2020). As such, understanding the services support personnel in K-12 settings report providing to students with EBD via remote instruction is crucial to understanding how to better prepare for future crises that require extended school site closures. The results of this survey of SETs and RSPs working with students with EBD is a first step toward this effort. This paper provides an initial landscape view of the ways that schools responded to these students’ needs in the midst of this unique crisis.
Our first goal was to understand the most frequently used methods through which SETs and RSPs reported communicating with students with EBD during school site closures. Virtual meetings using platforms like Zoom™ were the most frequently (37.9%) used by all educators. Communication via telephone was the next most frequently used method followed by virtual classrooms (e.g., Google Classroom™, Seesaw™), email, and social media, respectively. This did not vary significantly by policy (i.e., optional or mandatory) or role (e.g., SET or RSP). Interestingly, even when remote learning was optional, SETs and RSPs reported holding virtual meetings with their students or calling them on the telephone. One limitation of note is that we did not inquire about the activities that occurred during this communication. Based on limited knowledge these optional learning opportunities, one cannot assume instruction was provided. As an illustration, in one author’s local district which elected for remote learning to be optional, teachers were instructed to hold optional Zoom™ meetings twice per week, but no academic instruction was allowed to occur; instead, meetings were an opportunity to reconnect socially. Future researchers should consider examining the perceived and observed effectiveness of these communication methods from multiple perspectives (e.g., SETs, RSPs, parents, students) and for multiple purposes. An additional line of inquiry involves examining how access to varying technologies (e.g., devices, high speed internet) impacts the selection of certain communication methods.
Our second goal was to determine the types of strategies SETs and RSPs implemented during optional and mandatory remote instruction. These did not vary according to policy. Over half of respondents who were delivering optional or mandatory remote instruction indicated that they checked in with all of their students with EBD regarding their social, emotional, and behavioral well-being during school site closures, with SETs being more likely to do this than RSPs. This may be because SETs have formed stronger personal relationships with their students with EBD, as they are primarily responsible for executing the IEP and likely have more frequent, sustained contact with the student during the typical school day. It was alarming to note 11.7% of respondents reported checking in on few or none of their students (Table 2). Though the survey methods precluded the opportunity to explain their answers, it would be interesting to understand their reasons for not doing this, particularly given the vulnerability of some of these students during times of unrest and societal upheaval. After checking in with students about their well-being, the most commonly reported strategies were prevention strategies, reinforcement, and structured social skills activities. The least common methods reported were teaching replacement behaviors, arranging support from paraeducators, and providing remote counseling or therapy. Understandably, SETs who work directly with paraeducators were more likely than RSPs to report arranging support from them, whereas RSPs were more likely to indicate they provided remote counseling or therapy.
It is possible that implementation of these strategies was dependent on several factors. One particularly relevant factor is related to respondents’ roles and level of expertise or experience with strategies. Whereas some personnel may feel more efficacious in some strategies, others may not. SETs may be used to delivering social skills instruction, but not counseling. Relatedly, the degree to which these strategies and interventions are portable and effective when delivered remotely is unknown. For example, checking in on well-being was the most widely used strategy, which is not surprising. With all of the varied ways respondents communicated (i.e., virtual meetings, telephone, virtual classroom, email, social media), it would be easy (and also important) to simply ask students how they are doing. However, other strategies (e.g., social skills instruction, instruction regarding emotional regulation) may have been more difficult to deliver depending on the technology available and the structure and timing of remote learning (e.g., synchronous, asynchronous, hybrid). Unfortunately, we did not ask questions related to variables affecting implementation of specific strategies (e.g., IEPs, experience, technology) and, thus, we cannot pinpoint exact reasons for using different strategies. Yet, this study proves generative in that it prompts us to hypothesize and investigate these underlying reasons in future research.
Finally, we examined how SETs and RSPs reported assessing students’ social, emotional, and behavioral progress during the pandemic, as this is a key component to executing a legal IEP. Thus, it was not surprising to see that respondents who were mandated to provide remote learning were significantly more likely to indicate collecting assessment and progress monitoring data than those following optional policies. Also unsurprising was SETs were more likely to report assessing student progress than RSPs. This is logical given the SET is responsible for ensuring the effective delivery of the IEP, which includes documenting student progress and performance. However, the assessment data respondents reported using most frequently was anecdotal parent reports via email or phone call. It is unclear what parents actually reported. Interestingly, respondents indicated academic work was used to assess social, emotional, and behavior progress. Again, it is unclear how academic work would provide an indication of progress in these areas. Respondents did conduct some direct observation virtually, though very few used any behavioral progress monitoring tool.
Limitations
While the results of this survey are both timely and important, our methods were not without limitations. First, the survey was administered in the midst of the pandemic and educators were asked to respond while adjusting to their new instructional and living requirements (e.g., working and caretaking from home). We did not have an opportunity to obtain a fully representative sample; the overall sample was small compared to the total population of educators in the United States and represents a non-probabilistic sample. Furthermore, our use of snowballing sampling prohibited response rate calculation. Due to the critical and sudden need to understand the context as it was unfolding, we relied solely on relevant contacts sharing the survey with their education networks. Given the urgency to collect information, we opted to conduct an exempt survey and not collect multiple demographic variables. The need for this information also resulted in the missed opportunity for pre-notification, follow-up with respondents, and incentives for completing the survey; all of these strategies would have likely increased the number of respondents. Furthermore, the use of a convenience sample affects the precision of our estimates (Henry, 1990). At the same time, we received a substantial number of responses from four states representing South and West regions (i.e., California, South Carolina, Florida, and Arizona). This may have contributed to oversampling in some regions of the country. In addition, as is the nature of survey research, the responses rely only on self-report; we did not triangulate service provider responses with student or parent perspectives and there was no opportunity for direct observation or permanent product review (e.g., receiving lesson plans, student work, call logs). Respondents were also overwhelmingly from public schools (89.%), and 5.7% represented private schools. While the majority of U.S. schools are public, this is not representative of the distribution of public/private schools; respondents from private schools were likely underrepresented in our sample.
In addition, our use of survey data prohibited a more comprehensive, nuanced perspective of the communication, services, and assessments used across respondents. The survey provided an initial snapshot into the services support personnel provided during the beginning of the pandemic while most students were at home. We recognize that historically, most school-based services and supports for students with EBD are delivered in the context of a classroom or school environment. Therefore, it is important to consider that some of the interventions and strategies identified in the survey may not have been able to be implemented with fidelity to typical procedures. With that, we acknowledge that the study provided a brief list of services and supports and therefore there are many other supports that may have been implemented but not captured in this survey. Future work should incorporate qualitative data collection to capture not only respondents’ perspectives on the services offered but also service providers’ sense of efficacy in the midst of school closure, their perspectives on their capacity to fulfill their roles during school site closures, and the organizational factors which may have facilitated or prohibited their enactment of effective practice in the midst of the COVID-19 pandemic. Finally, the results of this study should be interpreted with the caution that these were respondent self-reports without empirical evidence of the continuity of services, communication, instruction, or assessment strategies reported. It is possible the sensitive and legally-binding nature of the IEPs may have impacted responses.
Implications
While we report several limitations of this timely and important work, there are numerous practical, policy, and research implications and directions for future research. First, policy makers and educational leaders should develop guidelines for mandating and supporting continuity of instructional services particularly for students with disabilities during school site closures. It is possible that without clear federal policy guidelines, confusion and lack of planning resulted in missed instructional opportunities critical to the progress toward annual goals and student wellbeing. Next, while many respondents reported the continuation of services, it is possible that access to technology prohibited some educators, families, and students from engaging in instructional opportunities. Future research should include a more nuanced analysis of potential barriers to communication, instruction, and assessment (Bruhn et al., 2021). Relatedly, policy makers and educational leaders should ensure equitable student access to technology devices and broadband (National Education Association, 2020). As we look at the phenomenon first noted as digital divide (i.e., achievement gap between students with access to technology and students without access) this is now known as the “homework gap” as it refers to students with access to devices but without internet or broadband to complete their homework or school assignments (Basu, 2020). The homework gap is particularly relevant for students at higher risk of educational failure and poor long-term outcomes, such as students with EBD.
The results of the study highlight respondents prioritized checking in on the social, emotional, and behavioral wellbeing of their students with EBD, for which the field of education and SETs and RSPs should be commended. This was a priority for both SETs as well as RSPs. The respondents also reported virtual meetings as their primary communication format. At the same time there was a substantial percentage of respondents reported they did not check-in with their students. The reason for this lack of contact could be due to district policies, access to connecting with students, or other unknown reasons. Regardless, it prompts us to think about the methods and mechanisms for communication as well as the resources needed to support SETs and RSPs during remote learning periods. Future studies should emphasize the barriers reported by EBD teachers and RSPs to support students remotely.
Future researchers should also develop and examine evidence-based practices for students with EBD that are easily portable to the home in case of future school site closures. Similarly, researchers should investigate the degree to which caregivers are knowledgeable enough, have the required resources for, and can feasibly implement instructional strategies for students with EBD in the home during school site closures as this could have influenced the ways in which service providers were able to support students in the spring of 2020. It is also important to understand whether educators perceived that their efforts to provide instruction during the COVID-19 school site closures met the needs of their students. Finally, researchers should openly inquire from educators what additional supports, guidelines, and resources they felt would have made their instructional supports more effective during this crisis.
Supplemental Material
sj-pdf-1-bhd-10.1177_01987429211016780 – Supplemental material for A Survey of Educators Serving Students With Emotional and Behavioral Disorders During the Covid-19 Pandemic
Supplemental material, sj-pdf-1-bhd-10.1177_01987429211016780 for A Survey of Educators Serving Students With Emotional and Behavioral Disorders During the Covid-19 Pandemic by Shanna E. Hirsch, Allison L. Bruhn, Sara McDaniel and Hannah M. Mathews in Behavioral Disorders
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available on the Behavioral Disorders website with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.