
Abstract

Disulfiram is a US FDA–approved medication for the long-term management of alcohol use disorder (AUD). It is recommended as a second-line treatment in the West. However, the Indian experience with disulfiram has been more positive, leading to its use as the primary drug in multiple treatment programs when given under supervision. 1 However, its use has always remained controversial because of difficulties in proving its efficacy and the severe nature of the disulfiram ethanol reaction (DER).2, 3
Compliance with disulfiram has been the Achilles’ heel of its efficacy. Although multiple strategies have been adopted to enhance compliance with disulfiram (including spouse contracting, incentives, legal orders, contracts, and end-patient information), compliance in the majority of treatment programs has remained low. 4 Some researchers have suggested the implantation of disulfiram (to ensure long-term drug delivery and alcohol abstinence) as a strategy for compliance. However, other than significant questions about the efficacy of implants, there are significant ethical considerations associated with disulfiram implants. 5 As our case will demonstrate, disulfiram implantation (with high-dose disulfiram) can lead to severe complications.
Case Report
A 45-year-old married male presented to the emergency department of a tertiary care hospital in Central India with seizures and disorientation for four days. His wife reported that he had been suffering from AUD for 15 years and had been detoxified at a private hospital in Western India about two months back. Following a month-long detoxification, the wife was informed about disulfiram implantation as a treatment for AUD. She also reported having spoken to multiple families who had opted for disulfiram implantation at the hospital. With her consent, the patient was surreptitiously surgically (under general anesthesia) given a “disulfiram implant” in the right lower abdomen. She was additionally asked to administer (surreptitiously or otherwise) disulfiram tablets to the patient. The recommended dose was 1 tablet daily if he remained abstinent or up to 10 tablets per day if he did not remain abstinent, until he became abstinent again. Following this, he was discharged with some supportive medications.
The patient remained abstinent for a month, was oriented and aware of his surroundings. His mental faculties were as per his usual self, with physical weakness as the only remaining symptom.
When he relapsed after a month, the patient consumed alcohol twice (about 30 units of alcohol combined) over two days. This lapse caused his wife to surreptitiously administer additional doses (as advised), with an estimated 10 disulfiram tablets being given over 96 hours. Two days after he started consuming alcohol, he developed seizures with disorientation and remained in this state when he presented to us. Non-contrast computerized tomography of the head revealed no significant abnormality, a blood investigation revealed mild dyselectrolytemia and raised gamma glutyl transferase (GGT) levels. The patient was provisionally diagnosed with delirium due to organic etiologies and was admitted to our care. Ultrasonography revealed a Grade 1 fatty liver along with four foreign bodies in the subcutaneous plane of the right iliac fossa, indicated as a parallel echogenic focus casting a heterogenous hyperechoic area and shaped like circular discs. This was suggestive that the alleged “disulfiram implant” was a disulfiram tablet.
The patient was initially managed with intravenous lorazepam and thiamine supplementation. After confirming abstinence and correcting dyselectro-lytemia, a final diagnosis of disulfiram-associated encephalopathy (DaE) was made.
The patient regained orientation in four days. Once oriented, he displayed significant cognitive and motor deficits. Assessment with the AIIMS Neuropsychological Battery showed motor, tactile, and cognitive dysfunction (dyscalculia; deficits in working memory, recall, and writing) with more significant loss in right hemispheric functions. Magnetic resonance imaging (MRI) denoted substantial atrophy of the mammillary body, brainstem, and enlarged ventricles. These cognitive dysfunctions gradually improved over the next three weeks with only supportive management, he was subsequently discharged on request. However, we considered the patient’s initial presenting condition (disorientation and seizures) to be a consequence of DER. However, he continued to have neurological deficits even after regaining orientation. These deficits (including impaired memory, decreased concentration, ataxia, dysarthria, and frontal release signs) have been reported to be a consequence of disulfiram use. 6 Additionally, these deficits continued to be present in the absence of autonomic instability that usually accompanies a DER. The duration of the deficits was not consistent with the acetaldehyde’s half-life (the DER’s primary causative agent). The fact that disulfiram is known to accumulate in adipose tissues and has a longer half-life led us to conclude that the neurological deficits were a consequence of DaE. This was also consistent with a similar case reported before. 7 Unfortunately, we could not conduct an EEG to confirm this diagnosis due to a lack of technical staff.
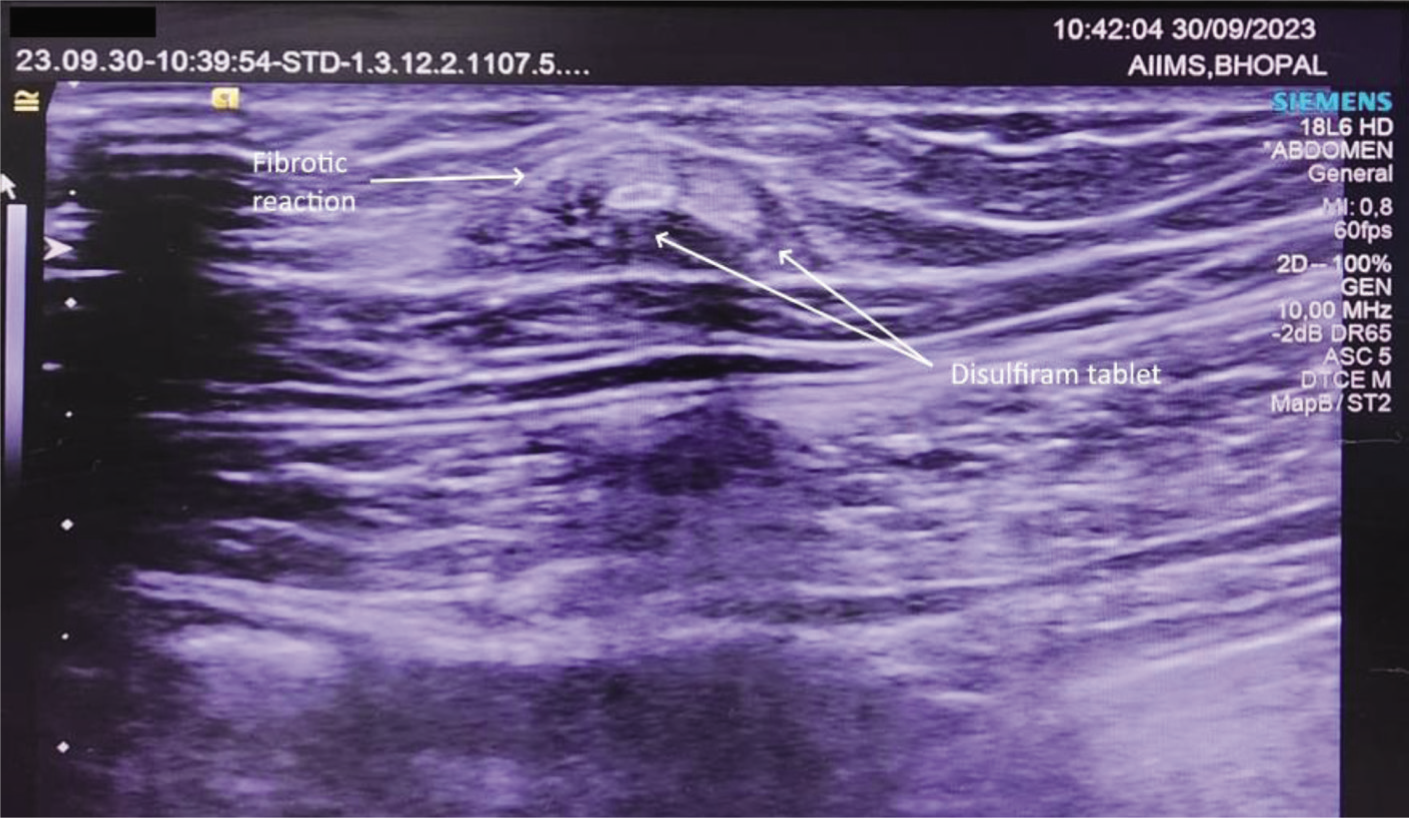
The patient sought admission again after four months with the specific request to remove the implanted disulfiram tablets. Repeat ultrasonography was done, which revealed that the four foreign bodies in the same area had, however, shifted from their original location (Figure 1). However, the size of the foreign bodies had reduced, coupled with an increase in the fibrous tissue in the area. The attending surgeon advised against surgical removal given the already disintegrating nature of the foreign bodies and their mobile nature, which would make removal difficult. The patient was again discharged on naltrexone (50 mg) and has been on follow-up since discharge. He has continued to consume alcohol occasionally (about four to six drinking episodes per month) without any adverse consequences. The patient’s clinical status has remained the same. He has continued to refuse to consider strict abstinence (and disulfiram treatment) as a treatment goal. However, he did not attribute the medical complications as a reason for not considering disulfiram.
Ultrasonography of the Abdomen Wall Showing Two Hyperechoic Circular Masses About 5 mm in Diameter (Indicating Unabsorbed Implanted Tablets).
Discussion
Disulfiram is a known causative agent for neuropsychiatric adverse effects (even in the absence of alcohol) in a few patients. 8 Neurotoxicity in the basal ganglia as a direct consequence of disulfiram metabolite—diethyldithiocarbamate (DDC)—is believed to be the cause of DaE. In this case, the high dose of disulfiram might have led to the accumulation of DDC and its metabolite carbon disulfide (CS2). Both these substances are neurotoxic, and acute exposure to CS2 has been associated with some of the neurological deficits seen in this patient. This might have the causative mechanism for DaE in this patient.
The patient’s initial complaints were suggestive of DER. Delirium usually accompanies psychosis or a disulfiram ethanol reaction.6, 9 In this case, although delirium started when the patient had been consuming alcohol, it lasted long after any alcohol or its metabolites would be expected to be in his body. DaE is usually associated with higher doses, anatomical lesions in the brain, or the presence of psychiatric comorbidities. 10 In our case, the patient had the first two, further supporting our diagnosis.
This highlights the unusual prescription and procedure the patient underwent. Surreptitious administration of disulfiram (although unethical) is quite commonly reported. 11 The practice of implantation of disulfiram tablets, although occasionally by some practitioners, is considered by most clinicians as unethical and ineffective. 12 Higher doses of disulfiram to enforce abstinence, such as the one the patient received, is considered an outdated and risky approach with little clinical benefit. 13
Combining these uncommon and questionably ethical practices precipitated a medical emergency in our patient. DaE is an infrequent occurrence.7, 14 Other neurological adverse consequences of disulfiram administration (mainly due to surreptitious administration) are also uncommon.6, 15 In our case, the combination of implantation and an unlicensed dose presented unique challenges. Disulfiram implants were first developed in the late 1960s and have resulted in mixed outcomes. 13 Significantly higher wound complications, the ethical issues surrounding an invasive procedure for a medication with an unknown mechanism, a substantial placebo effect, and a potentially dangerous pharmacological effect have made disulfiram implantation a fringe procedure in the medical community. It is also important to highlight that no commercial implants are currently approved in India or any Western country.
Conclusion
Our case highlights the myriad medical issues associated with the surreptitious use of disulfiram. The unknown sterilization procedure, lack of informed consent, coadministration of oral disulfiram in unlicensed doses (leading to DaE), and fibrotic reaction to the implanted tablets highlight that the practice of disulfiram implantation or surreptitious administration must be abandoned.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Written consent was taken from the patient for publication of this case report.