
Abstract
Purpose of the Review:
The objective of this study was to do a meta-analysis focusing on the efficacy of psychological intervention for the adolescent population and PTSD as a primary outcome variable.
Collection and Analysis of Data:
An electronic search was conducted on PubMed, Science Direct, PsycINFO, and Cochrane Library databases from January 1, 1990, to March 31, 2023. Original studies and systematic reviews/meta-analyses were segregated. In the first study, 129 meta-analyses (MAs) were screened and 8 MAs were analyzed. In the second study, six RCTs and five non-RCTs exclusively including adolescents with a primary diagnosis of PTSD were analyzed. The MA revealed the average sample size to be 243.33 (SD = 372.94) with 63.98% female participants in RCTs and 153 (SD = 237.17) with 56.99% female participants in non-RCTs. A total of 13 different interventions were analyzed. Cognitive-behavioral intervention had a large effect size of 1.63 for PTSD. Cochrane’s Q test and I2 index revealed considerable heterogeneity among groups. There was no significant difference between RCTs and non-RCTs in the total number and duration of intervention sessions and the duration of each session. However, the average follow-up time points varied significantly between RCTs and non-RCTs. RCTs followed random sequence generation and, hence, had a low risk of selection bias.
Conclusion:
Although the CBT framework with a focus on trauma and traumatic emotions was at the core of treatment efficacy, the type of trauma was the key consideration. Further studies of treatment efficacy moderated by specific trauma characteristics are required to advance the knowledge base in the treatment of PTSD in adolescents.
Adolescence is a crucial, unique, and formative period of development. Some adolescents are at a greater risk of mental health conditions due to their living conditions, adversities, stigma, discrimination or exclusion, or lack of access to quality support and services. Therefore, reducing the risks of adolescents struggling with adversity, promoting positive socioemotional experiences, and ensuring access to appropriate and adequate mental health care services are critical for their physical and mental health, personality development, and cognitive and academic performance. Thus, any methodologically sound psychological intervention for such adolescents has a long-lasting impact during adolescence and adulthood.
Psychological interventions for adolescents have diverse applications in reducing specific or non-specific symptoms of various mental and behavioral disorders. The spectrum of psychological interventions consists of low- to high-intensity sessions ranging from counseling and various types of psychotherapy to short-term or long-term illness-specific interventions, depending upon the objectives and expected outcome of the intervention. These interventions are based on diverse approaches, including behavioral, cognitive, cognitive-behavioral, humanistic, psychosocial, and transdiagnostic, 1 targeting specific behavioral, emotional, and cognitive problems in various mental disorders. These interventions are sometimes stipulated in combination with pharmacotherapy, depending on the severity of the disorder. Whether or not the psychological interventions are combined with pharmacotherapy, it is crucial to estimate their effect size. Overall, psychological interventions have been reported to be useful for adolescents’ mental well-being, the alleviation of non-specific symptoms (such as psychological distress, hopelessness, sadness, intrusions, and impulsive behaviors), 2 and the clinical symptoms of specific mental disorders such as PTSD.
Even a single session of the emotional freedom technique has been found to be effective in reducing trauma symptoms in adolescents. 3 The literature supporting the usefulness of psychological interventions in the alleviation of PTSD clinical/subclinical symptoms also highlights the need for methodologically robust randomized trials. Considering adolescents as a unique group, among the well-established individual format psychotherapies with controlled trials, standard trauma-focused cognitive-behavioral therapy (TF-CBT)4–6 and cognitive-behavioral therapy for trauma in schools (CBITS) 7 have more evidence for PTSD core symptoms compared to stepped care TF-CBT and other forms of therapies. Unified protocols of transdiagnostic psychotherapy are emerging for addressing PTSD and its comorbid depression and anxiety conditions among adolescents. Structured psychotherapy for adolescents recovering from chronic stress (SPARCS) as a group intervention for chronic interpersonal trauma-affected adolescents is also emerging. 8
The efficacy of any intervention for reducing PTSD symptoms may be moderated by specific characteristics of trauma, support provisions received, comorbid mental illnesses, and adolescents. Therefore, a comprehensive sub-group analysis is vital, especially when many studies are combined for meta analysis. Meta-analyses thus help guide clinical decision-making around selecting treatments that might be most effective given the characteristics and circumstances of a particular adolescent. 9 While evidence for interventions has previously been reported for children, adolescents, and adults, a synthesis of findings focusing only on adolescents and wide sub-group analysis needs to be included. Emphasizing the areas less discussed and reasons for less/non-alleviations of symptoms should also be important. 10 Hence, providing a holistic picture of the efficacy status of PTSD interventions specific to adolescents becomes crucial. Thus, the authors assert the need for this study due to these reasons: 11 (a) there was no meta-analysis on PTSD as a primary diagnosis, and adolescents as an exclusive population (as all previous MAs included original studies with mixed samples); therefore, do not provide a specific effect size of intervention for adolescents; (b) the previous MAs that included mixed samples with adolescents did not consider PTSD as a primary diagnosis; and (c) the group analysis done in previous MAs with mixed samples was limited and did not provide sufficient analysis of intervention details (e.g., total duration of intervention, duration of each session, details of intervention components/contents, and follow-up). We also calculated the effect size of interventions in some RCTs and non-RCTs, which were not provided in the original papers we included in this review, and this adds value to the included studies. Therefore, we conducted an MA where we reviewed the systematic reviews and MAs for gap analysis in the first part of this study and included original RCTs and non-RCTs conducted only on adolescents for their efficacy in improving PTSD symptoms (primarily) and associated comorbidity (secondarily) in the second part.
Method
Literature Search and Identification of Studies
An electronic search from five databases, PubMed, Science Direct, PsycINFO, Cochrane Library, and Wiley Library, including publications between January 1, 1990, and March 31, 2023, was conducted. The key search terms/MeSH items with Boolean operators were applied as follows: the first author did the primary search and title/abstract screening, and the second author did the article finalization, meeting the inclusion criteria (Table 1). There were no major disagreements. However, mild disagreements were handled amicably with a consensus. The assessment of the quality of each included study was done separately by each author.
Search Words/Medical Subject Headings (MeSH) Terms Used with Boolean Operators (“AND,” “FOR”).
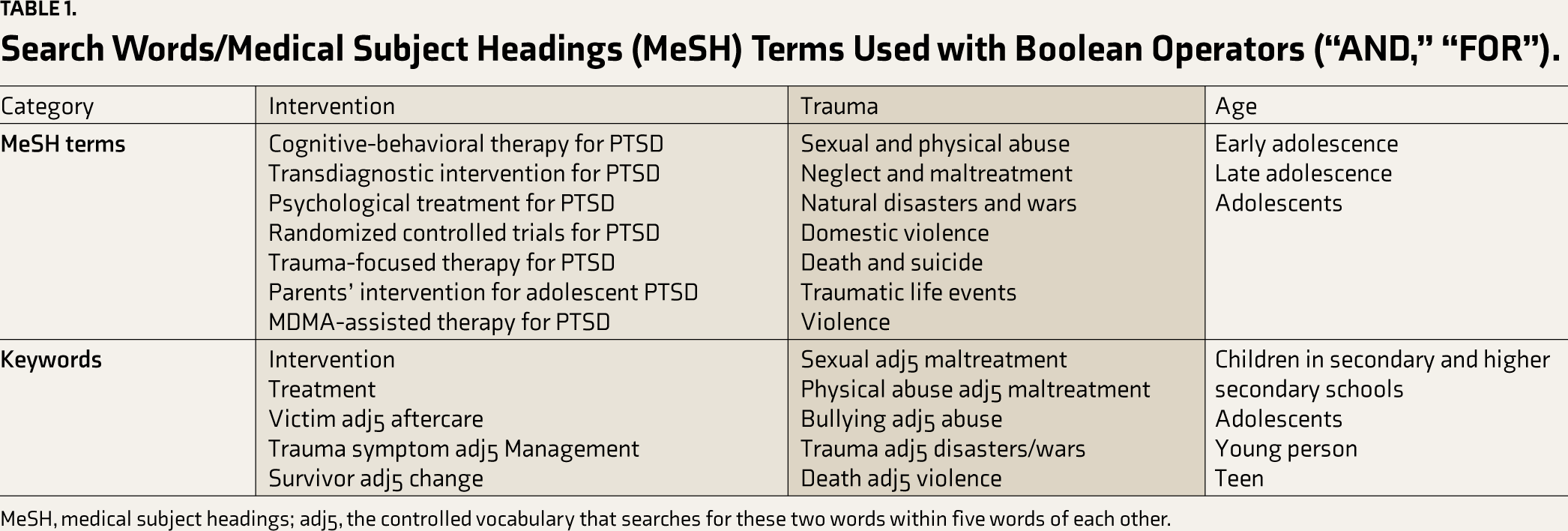
MeSH, medical subject headings; adj5, the controlled vocabulary that searches for these two words within five words of each other.
Furthermore, if they met the exclusion criteria, titles and abstracts were excluded from the selection. Full articles were reviewed if it was unclear from the abstract whether outcome data relating to the primary diagnosis of PTSD was reported or not. We tried, but PROSPERO regretted saying this could not be registered due to COVID-related studies being prevalent. This was a general guideline on their website, too. Then, we registered the PTSD intervention study in CTRI, under which we prepared this article. However, this was part of a larger project already registered under CTRI (No. REF/2024/01/077200AU).
Inclusion criteria (Study 1):
Full-text, open-access systematic reviews and meta-analyses in the English language. The meta-analyses providing pooled intervention efficacy.
Exclusion criteria (Study 1):
The sample does not contain adolescents. PTSD is not an outcome variable.
Inclusion criteria (Study 2):
Openly accessible, full-text, original studies in the English language Adolescents 12–19 years old Psychological interventions primarily target PTSD symptoms. RCTs and non-RCTs between January 1, 1991, and March 31, 2023
Exclusion criteria (Study 2):
Studies with mixed populations, for example, children and/or adults with adolescents Studies where PTSD is not the primary diagnosis Non-psychological interventions, for example, alternative medicine such as acupuncture, aerobics, ayurveda, homeopathy, etc. Case reports, dissertations, reviews, protocols, and abstracts excluded.
Extraction and Organization of Data
To reduce selection bias, articles were included following a strict PICO format (population: male and female adolescents between 12 and 19 years with any traumatic experience; intervention/indicator: only original intervention studies where PTSD was a primary diagnosis; comparator: studies that recruited participants through both random and non-random sampling; outcomes (primarily outcome variable): intervention effect size on PTSD scores). The extractions from selected studies were contained in the master Excel sheet, including information on participants (number, gender, and age); RCT research design (blinding and allocation); sampling type; type of trauma and PTSD diagnosis method; type of control group (age, gender, sample size, etc.); delivery setting (home/hospital/school/community); intervention details (number of sessions, duration of each session, session frequency (daily/weekly/monthly)); intervention format (group/individual); components/contents of intervention; outcome variables and measurement tools; follow-up; reported therapy outcome (significance of impact and effect size); and quality of the study.
Based on CBITS, one study was not included in the comparison of effect sizes because it did not mention the SD or CI values.
Statistical Analysis
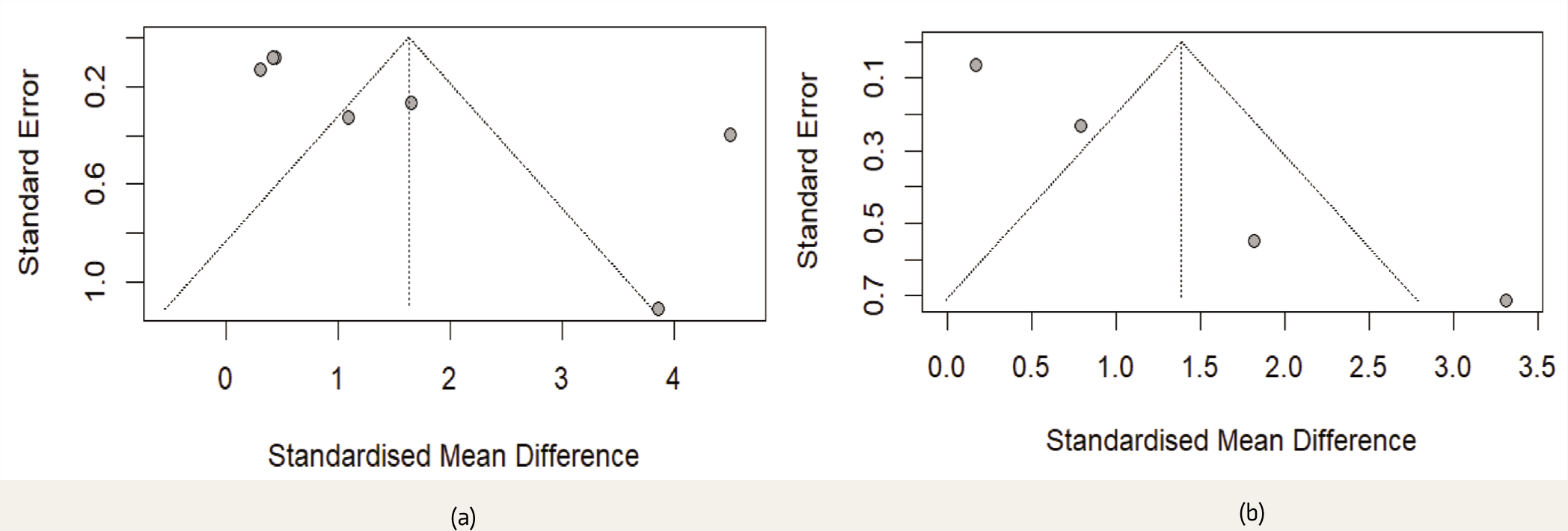
Microsoft Excel and R were used for statistical analysis. 12 The evaluation of effect sizes, also known as standard mean differences, or SMDs (Hedge’s g), was done by using pre- and post-intervention scores for experimental, control, or intervention groups (RCTs and non-RCTs), based on which forest plots were interpreted (Figure 2). Pre–post scores for RCTs (for both intervention and control groups) and non-RCT intervention groups (pre–post intervention) were analyzed through random effect analysis. Cochrane’s Q test and I2 index were applied to determine the presence and quantification of heterogeneity. 13 I2 may not be sensitive to changes in the number of studies in the analyses, and the interpretation of heterogeneity was followed as per the existing standard (I2 ≥ 25%: low; I2 ≥ 50%: moderate; I2 ≥ 75%: substantial; I2 ≥ 90: considerable). A funnel plot was used to address publication bias.
Results
A total of 129 MAs/SRs (Study 1) and 11 publications (six RCTs and five non-RCTs) (Study 2) evaluating the intervention efficiency in alleviating PTSD symptoms in adolescents were included in the current meta-analysis (MA).
Study 1: Analysis of Meta-analyses
A total of 129 systematic reviews/ MAs were screened. No MA had an adolescent-only sample, and 121 MAs were excluded: children (n = 12), adults (n = 32), PTSD not as the primary diagnosis (n = 32), duplicate studies (n = 25), neurological/physiological PTSD (n = 6), non-intervention (n = 8), scoping review (n = 1), pharmacological intervention (n = 3), non-English (n = 1), and no open access (n = 1). Thus, eight mixed MA samples (children–adolescents, adolescents–adults, or children–adolescents–adults) were included for effect size comparison. However, the effect size mentioned in these MAs (Table S3) was not specified for adolescents. Therefore, the distinct pooled effect sizes for adolescents for these eight MAs could not be provided. These effect sizes of these MAs (SMD) were expressed as Hedge’s g or Cohen’s d. The highest effect size for PTSD intervention was present in CBT (g = 1.43). Group interventions had a medium effect size (g = 0.55) in PTSD. One study reported a small to medium effect size (d = 0.39) for CBT in PTSD. The combined effect of psychological interventions for PTSD was found to have a large effective size: RCTs: SMD = 1.63 (95% CI 0.40–2.86) and non-RCTs: SMD = 1.38 (95% CI 0.11–2.66) (refer to Table S1), similar to 1.43 in Peters et al., 14 which was based on seven RCTs and participants were in the age range of 12–25 years, and Wergeland et al., 15 with an effect size of 1.43 based on 21 RCTs/open trials on children and adolescents, and higher than Rolfsnes et al. 16 (children and adolescents) at the post-treatment stage. However, since all these MAs included mixed samples, the effect size of specific interventions, either for adolescents or for PTSD, remains doubtful and inconclusive (Table S3).
Study 2: Selection and Characteristics of Included Studies
After applying filters as per the criteria, a total of 184,355 records were obtained from five databases collectively. Out of 943 potentially relevant studies, 803 were excluded as they had no PTSD measures, were non-interventional, were genetics/neurological/physiological-based PTSD studies, were inventory-related/scale development, had systematic reviews and/or MAs, were repetitive articles, had a mixed sample, and had no open access. The summarized process for extracting relevant studies is displayed in the flow chart in Figure 1.

RCT, randomized controlled trials; non-RCT, non-randomized controlled trials.
Description of Studies
The remaining RCTs had two arms, except for a multi-arm trial 17 (BBN—Bounce Back Now, BBN + ASH—Adult Self-help and Control). In a study, 18 the standard deviation was calculated using CI values and t as the critical value.
Out of these 11 PTSD intervention studies, 54.5% (n = 6) were RCTs, and the rest, 45.5%, were non-RCTs (n = 5). Two RCTs were conducted in the USA and one each in Colombia, Iran, South Africa, and Kosovo. However, 60% of non-RCTs (n = 3) were conducted in the USA, and one each was conducted in Israel and Taiwan. All 11 studies recruited participants from schools, clinics, and communities. The interventions were delivered in various settings: school premises, nature retreat facilities, community welfare agencies, and hospitals/clinics. Details of the intervention, trauma type, PTSD diagnostic tool, participants, allocation, blinding, components, or contents of the intervention are presented in Table 2.
Three RCTs and three non-RCTs reported effect size by Cohen’s d (d = 0.2 indicates small, d = 0.5 represents medium, and d = 0.8 indicates large effect size) and partial eta squared, η2 (η2 = 0.01 indicates a small effect, η2 = 0.06 indicates a medium effect, and η2 = 0.14 indicates a large effect).
Type of Trauma, PTSD Diagnosis, and Comorbidity
Trauma exposure in adolescents reported in the studies included multiple adverse childhood experiences (ACEs), including child sexual abuse, physical abuse, physical assault, threat with a weapon, experiencing and/or witnessing violence/IPV during dating, war, socioeconomic status, natural disaster (typhoon, tornado), sexual assault, and gender minority stress.
In RCTs, 50% (n = 3) were based on trauma exposure by multiple ACEs (interpersonal trauma, low socioeconomic status, and maltreatment) and 50% on physical/sexual abuse and/or COVID, natural as well as human-made disasters. A similar trauma exposure causation for PTSD was seen in non-RCTs, where two studies reported negative experiences of refugee adolescents: death of a loved one/close friend; being badly hurt by a parent, teacher, or caretaker; family fights; and child sexual abuse, and the remaining three studies documented natural, human-made disaster and sexual assault exposure.
PTSD diagnosis in trauma-exposed adolescents was done by self-reporting of CPSS in 66.66% of RCTs (n = 4) and 33.33% of non-RCTs (n = 2). However, PTSD in the remaining RCTs was assessed by HTQ and SCID DSM. In non-RCTs, C-IES-R, the UCLA PTSD index (DSM), and the PTSD-symptom Scale (PTSD-SS) were used. In two RCTs, PTSD was assessed through self-reporting questionnaires and clinical interviews, whereas four used only one tool for diagnosis. In contrast, all non-RCTs (n = 5) used a single tool for assessing PTSD. Three RCTs reported comorbid depression, and one reported comorbidity with both depression and anxiety. Only one RCT reported self-injury in adolescents. Similarly, PTSD with comorbid depression was reported in four non-RCTs.
Types of PTSD Interventions
Interventions based on several approaches, such as transdiagnostic, cognitive with/without behavioral approaches, EMDR, prolonged exposure, and RRFT, were applied for comorbid PTSD symptomatology. UP-A transdiagnostic asserts emotion regulation skills to increase willingness to experience strong emotions without relying on self-defeating escape or avoidance strategies. 19
The cognitive with/without behavioral model (CBITS, TF-CBT, cognitive restructuring, prolonged exposure) was based on guiding adolescents to identify problematic thoughts and beliefs related to their traumatic experiences, evaluate their accuracy, and develop new, more helpful, realistic beliefs and action plans. In “prolonged exposure,” individuals were taught to gradually approach trauma-related memories, feelings, and situations. 20 The web-based BBN intervention was based on principles and procedures associated with efficacious behavioral interventions. The PTSD module provided education as well as evidence-based recommendations focused on exposure, reduction of avoidance of traumatic cues, coping strategies, and anxiety management. The EMDR, on the other hand, was based on the idea that negative thoughts, feelings, and behaviors are the result of unprocessed memories. Treatment involves standardized procedures that include a simultaneous focus on spontaneous associations of traumatic images, thoughts, emotions, and bodily sensations and bilateral stimulation, most commonly in repeated eye movements. 21
On analysis of 11 included studies, it was found that CBITS, cognitive restructuring, counseling based on a cognitive-behavioral approach along with mindfulness-artistic expressions and EMDR, and prolonged exposure (PE) were applied in the case of interpersonal trauma (maltreatment) and lower socioeconomic impoverishment exposure. Mind–body skills and EMDR were applied in natural and human-made disasters (including war). Physical/sexual abuse and COVID-19 cases were addressed through the transdiagnostic unified protocol for adolescents (UP-A) and risk reduction through family therapy (RRFT). Also, 90% of all studies (RCTs and non-RCTs) (n = 10) were face-to-face interventions, except one RCT, which was a web-based intervention. Half of the RCTs (n = 3) were adolescent-focused interventions, and the rest, both adolescents and parents, were centered, where sessions were conducted in an individual, parallel, or conjoint format. Similarly, 60% of non-RCTs (n = 3) had adolescent and parent/caregiver sessions, and two studies involved adolescents.
In RCTs, 66.66% of studies (n = 4) reported an individual or group interventional format. However, 33.33% of studies (n = 2) were a combination of both (group settings with peers/parents and individual sessions). On the other hand, 40% of non-RCTs (n = 2) were administered individually and 60% (n = 3) in a group arrangement with a gender-segregated approach used for sensitive topics. The group sessions were either with peers or parents/caregivers. The following describes the intervention providers’ qualifications and training details.
A parallel intervention design was present in two RCTs, where the control groups received TF-CBT and supportive counseling as active interventions. In one RCT, participants in the control group with usual care conditions did not receive any treatment or services. However, they had no restrictions on the type or number of services they could receive during the study participation in their school or community. However, in another RCT, the care as usual control group included activities similar to those of the experimental groups (e.g., physical exercise, dance, acting, games, and movies). Still, it did not include any approach to address traumatic experiences or attentional and emotional regulation specifically. In a non-RCT case-control study, participants in the treatment-as-usual (TAU) group attended a weekly psychoeducation session.
Intervention Facilitators
Clinical psychologists, psychologists, psychiatrists, licensed CBT therapists and clinicians, counselors, master’s/doctorate-level social workers, master’s-level graduates of clinical psychology, expression-based therapists, and nurses with a one-year psychiatry diploma facilitated interventions in these 11 studies. The facilitators were either certified or trained in the respective intervention facilitation. It is to be noted that psychoeducation sessions in a non-RCT study (for the TAU group) were led by the peer mentors of the class and were supervised by psychologists. Under the training and supervision of psychiatrists and psychologists, school teachers, art and craft teachers, social workers, and occupational therapists also facilitated intervention. The training days for the psychological interventions ranged from one to seven days under the supervision of experienced psychologists and psychiatrists, with regular reviews of audio-taped sessions in three RCTs and one non-RCT session for intervention adherence (Table 2).
Overview of RCT and Non-RCT studies included.
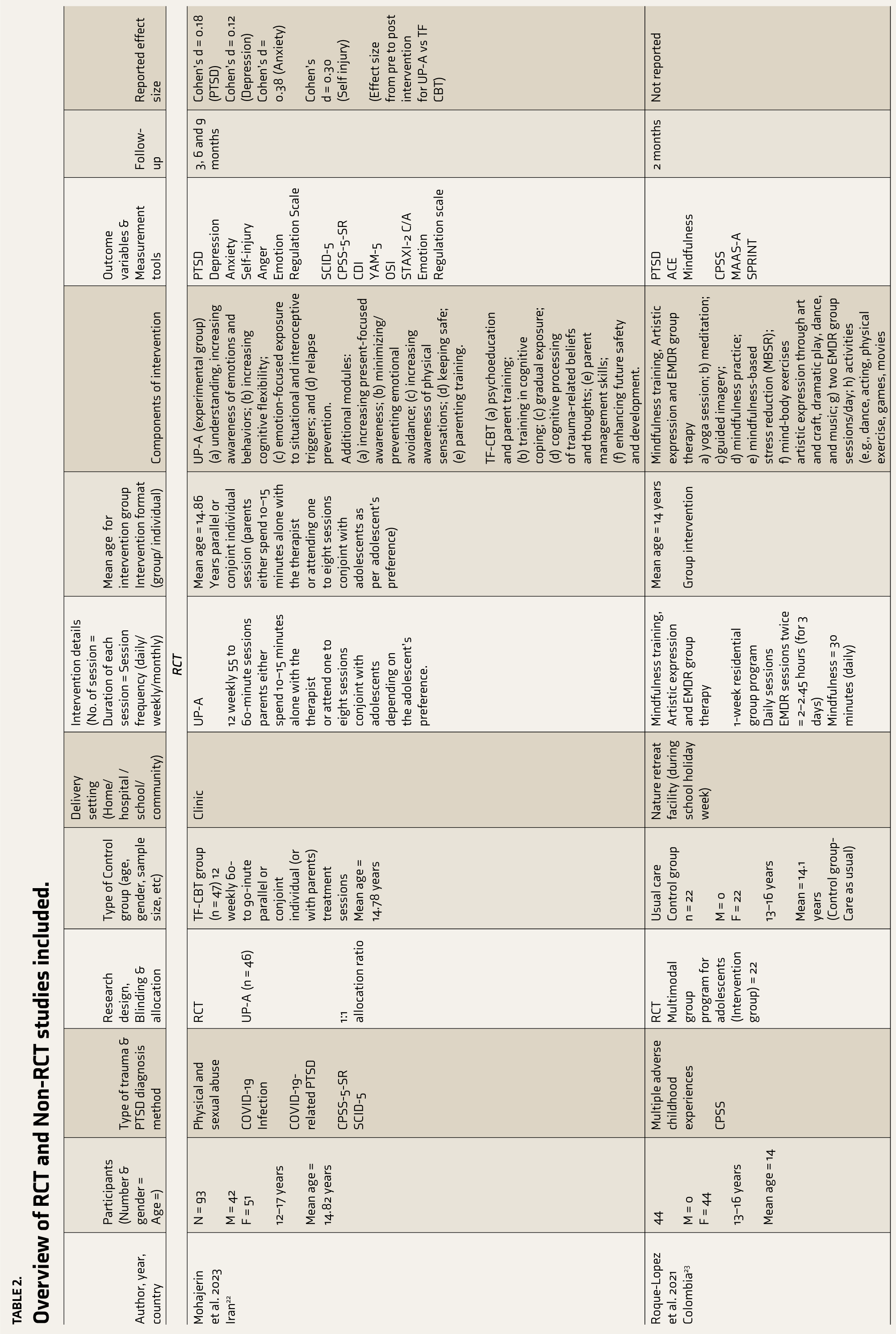



UP-A = Transdiagnostic Unified protocol for adolescents; CBITS = Cognitive Behavioural Intervention for Trauma in Schools; PE = Prolonged Exposure; BBN = Bounce Back Now; ASH = Adult Self Help; TAU = Treatment as Usual; CPSS = Child PTSD symptom scale; HTQ = Harvard Trauma Questionnaire; EMDR = Eye Movement Desensitization and Reprocessing; RRFT = Risk reduction family therapy; TFCBT = Trauma focussed Cognitive Behavioural therapy; DI = Children’s Depression Inventory; BDI = Beck Depression Inventory; UCLA PTSD = The University of California at Los Angeles Posttraumatic Stress Disorder Reaction Index; PTSDSS = Post-Traumatic Stress Disorders Symptoms Scale; MINI-KID = Mini International Neuropsychiatric Interview for Children and Adolescents; SCID = Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders; YAM 5 = Youth Anxiety Measure for DSM-5; OSI = Ottawa Self-Injury Inventory; STAXI-2 C/A = State-Trait Anger Expression Inventory for Children and Adolescents; MAAS-A = Attention Awareness Scale-Adolescents; SPRINT = Trauma Short PTSD Rating Interview; SUDS = Subjective Units of Distress Scale; CIRP = Adapted Child Intervention Rating Profile; W-TECh = War-Traumatic Events Checklist; C-IES-R = Chinese version of the Impact of Events Scale-Revised; MASC-T = Taiwanese version of the Multidimensional Anxiety Scale for Children; CES-D = Mandarin Chinese version of the Center for Epidemiologic Studies Depression Scale; TLEQ = Traumatic Life Events Questionnaire.
Delivery Setting
Interventions were delivered on school premises in 33.3% of RCT studies (n = 2), nature retreat facilities (n = 1), community welfare agencies (n = 1), and clinics (n = 1). Web-based intervention was accessible from anywhere, and this delivery setting was present at one RCT. However, 60% of non-RCT (n = 3) interventions were delivered in school settings rather than clinics/tertiary-level hospitals (
Outcome Variables and Measurement Tools
Four RCTs (66.66%) had combined additional outcome variables with PTSD. CPSS was the prominent measurement tool used in 66.66% of RCTs (n = 4), whereas structured interviews (DSM) and the Harvard trauma questionnaire (HTQ) were used in one study each for PTSD diagnosis. In non-RCTs CPSS,25,28 PTSD-SS, 26 C-IES-R 27 and UCLA-PTSD 29 tools were used. Out of 11 studies, post-intervention feedback from the adolescents was taken only in two non-RCTs and these used Adapted Child Intervention Rating Profile (CIRP) and Measure of treatment satisfaction scales. 29 (Table 2).
Components of Intervention (Experimental Group)
The most common component in all interventions was “psychoeducation,” which was present in nine studies (four RCTs and five non-RCTs). “Relaxation,” “guided relaxation,” and “breathing exercises” were components of seven studies (four RCTs and three non-RCTs). “Cognitive restructuring” in two studies (one RCT and one non-RCT) is an individual component. In contrast, it is a hidden component in cognitive-behavioral-based interventions, present in two studies that involved CBITS and RRFT. The problem-solving component was present in four studies (two RCTs and two non-RCTs). Expressive/artistic expression/body movement was a part of three studies (two RCTs and one non-RCT). EMDR (one RCT and one non-RCT) and narrative/gradual/imaginal exposure (two RCTs) were present in two studies each. The least used components were genograms (one RCT) and gift cards for encouraging adolescents to sustain participation in the intervention (one non-RCT) (Table 2).
Subgroup Analyses of RCT and Non-RCT Studies
Number of Adolescents, Gender, and Age
There was no statistically significant difference in terms of the number of adolescents participating (1,466 vs. 765) between RCTs and non-RCTs, experimental and control groups (968 vs. 493), and gender in RCTs (938 vs. 528) and non-RCTs (329 vs. 436). The overall mean age of adolescents (15.05 years) in the experimental and control groups (14.48) was statistically not different in the RCTs. The mean age was not mentioned separately in the two RCTs for the intervention and control participants.16,22 For the double-arm study, two segregated age values were used. Therefore, the number of intervention groups considered in RCTs was five instead of four. 15 The data distribution in the experimental group was largely not normal (RCT M = 161.33 and SD = 281.67). However, the majority of studies did not comment on data normality.
Details of Intervention Sessions
The duration of individual sessions in RCTs ranged from 55 to 195 minutes. The mean duration of one session in RCT was 89 minutes. Transdiagnostic-UP-A, CBITS, and PE were for 60 minutes on average in three RCTs, with more time involved in EMDR sessions and mind–body skill interventions. The duration was not tracked in the web-based intervention. In non-RCTs, the duration of one session ranged from 30 to 240 minutes, with a mean of 97.5 minutes. Psychosocial programs, including supportive counseling, took around 240 minutes and involved various activities for participants and their parents. In one non-RCT, the duration of individual sessions was not reported.
The mean number of intervention sessions was 11.8 in six RCTs. A web-based intervention was multi-session without a specific number of sessions, due to which it was excluded from statistical analysis. In non-RCTs, a range of sessions was given; thus, the average number of sessions was used for analysis. The mean intervention sessions were 17.8 in non-RCTs, with EMDR sessions being more frequent. The mean total duration of intervention in RCTs (experimental groups) was 10.21 months, whereas in non-RCTs, it was 12.81 weeks. It is to be noted that in a web-based RCT, the duration was not mentioned, so n = 5 for RCTs.
Follow-up
Time points were defined as the junctions in the follow-up intervention period when the participants were assessed for PTSD and its comorbidity. It was found that follow-ups were done at 12 different time points in six RCTs, with the first follow-up done three months after intervention completion. Furthermore, two RCTs had three time points, two had two time points, and two had only one time point in follow-up. It is to be noted that two RCTs were followed up for 12 months after the completion of interventions. However, follow-ups at six different time points were reported in five non-RCTs, with a mean time of first follow-up of 2.2 months. Also, 80% of non-RCTs (n = 4) had only one follow-up time point, except for one that had two time points (three and months months). The mean months of follow-up assessment were 5.75 and 2.83 months in RCTs and non-RCTs. There was a significant difference in the time points of follow-up in RCTs (M = 5.75, SD = 3.52) and non-RCTs (M = 2.83, SD = 1.72; t (16) = 1.89, p = .03).
Heterogeneity and Therapy Outcome on PTSD (Pooled Efficacy)
Following is the effect size/SMD and heterogeneity estimation of RCTs and non-RCTs in the current article. Post-intervention score effect size for intervention and control groups in RCTs yielded a combined medium effect size of −0.44 (95% CI −0.81 to −0.07) with Q = 29.5 and I2 = 79.7% (95% CI 58.5–90.1). The negative value of effect sizes (SMDs) meant that the experimental group exhibited a significant decrease in PTSD scores. A non-RCT comparison of pre- versus post-intervention resulted in an effect size of 1.39 (95% CI 0.11–2.66) with Q = 33.59 (p < .001); I2 index = 91.06% (95% CI 80.23–95.96).
Sensitivity analysis was performed (intervention post vs. control post scores) to examine the extent to which the pooled effect size of the interventions in the MA changes by excluding or including studies in a meta-analysis based on the methodological quality of the included studies. It was found that effect sizes remained the same (medium effect size); however, when Gordon et al.’s or Mohajerin et al.’s study was excluded, the combined effect size decreased to −0.28. Therefore, the findings should be interpreted with caution.
Comparison of Types of Intervention at Post-assessment in RCT Studies
Findings from Table S1 revealed that multimodal intervention (refer to Table 2) and mind–body skill intervention significantly reduced the PTSD scores with a large effect size when compared to usual care in the earlier and delayed intervention in the latter. Interestingly, both were group interventions. Importantly, transdiagnostic unified protocol intervention and TF CBT were similar in their effect size. Forest plots describing the effect size comparison are shown in Figure 2. The funnel plot for addressing publication bias for RCTs and non-RCTs is displayed in Figure 3.
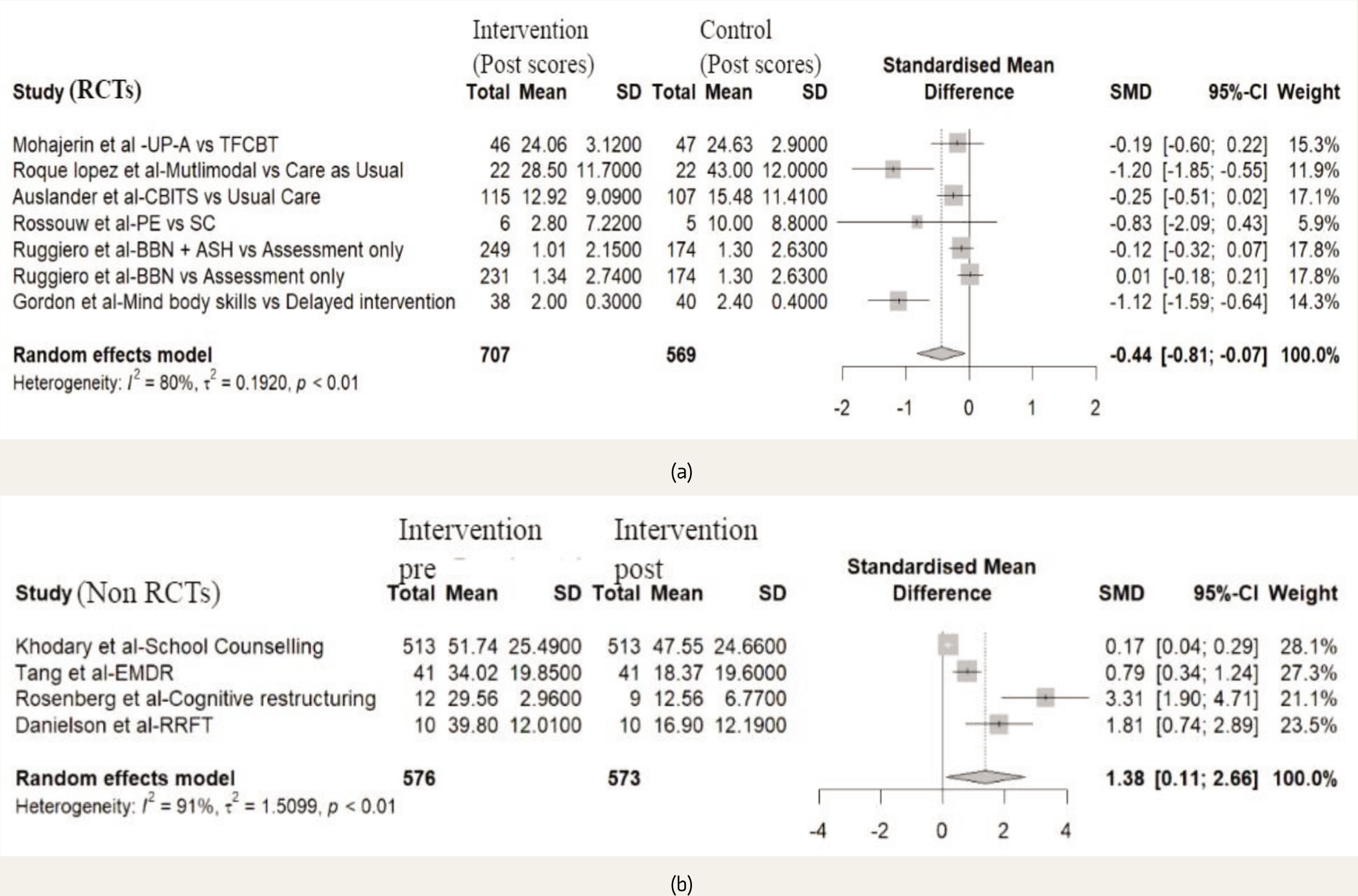
(a) Post-score Comparison of Intervention vs. Control Groups in RCTs.
UP-A, transdiagnostic unified protocol for adolescents; TF CBT, trauma-focused cognitive-behavioral intervention; CBITS, cognitive-behavioral intervention for trauma in schools; PE, prolonged exposure; SC, supportive counseling; BBN, bounce back now; ASH, adult self-help; EMDR, eye movement desensitization and reprocessing; RRFT, risk reduction through family therapy.
Funnel Plots for Publication Bias: (a) RCTs (Experimental Group Interventions) and (b) Non-RCTs (Intervention Groups).
Risk of Bias
Most RCTs had a low risk of selection bias. Five RCTs followed random sequence generation for randomization except in one study, where risk could not be determined. The risk assessment of all included studies is presented in Table S2. The Modified Joanna Briggs Institute (JBI) critical appraisal checklist for an analytical cross-sectional study (last amended in 2017) was used to assess the quality of non-RCT studies. The Cochrane Collaboration’s tool for assessing the risk of bias was used for RCTs.
Quality of Studies
The AMSTAR was used to evaluate eight MA/SRs that included randomized or non-randomized PTSD intervention studies with mixed samples (children–adolescents, adolescents–adults, and children–adolescents). Applying AMSTAR to the MAs reviewed (for Study 1) and included in this current article indicated that 83.8% of criteria were on the checklist.
Discussion
We assessed the efficacy of psychological interventions with RCT and non-RCT study designs for adolescents with PTSD. Our research resulted in 11 studies (6 RCTs and 5 non-RCTs) that met the inclusion criteria. The result of MA shows that psychological interventions can effectively reduce comorbid PTSD. It is to be noted that the PTSD psychological intervention domain has a huge research gap, and as a result, no MA publication based on the core adolescent population (12–19 years) was found under open access. Conclusively, all the previous MAs were based on a mixed sample population: adolescents either with children or with adults or both. While comparing the intervention and control post-intervention scores, it was found that it had a medium effect size, and the maximum reduction of the PTSD score was seen in multimodal versus usual care and mind–body skill training versus delayed intervention. This could be attributed to the non-inclusion of active controls in these two studies, while the remaining studies had active controls. The combined effect of psychological interventions for PTSD was found to have a large SMD similar to Peters et al., 14 which was based on six RCTs and participants in the age range of 12–25 years, and Wergeland et al., 15 with an effect size of 1.43 based on 21 RCTs/open trials on children and adolescents, and higher than Rolfsnes et al. 16 (children and adolescents) at the post-treatment stage. As PTSD can be comorbid with depression, anxiety, suicidal tendencies, substance use, or psychosis, there are other additional symptoms that cannot be alleviated through one particular medium of intervention.30–32 Thus, a transdiagnostic approach has been applied for emotional disorders such as PTSD, which is maintained by (a) frequently experiencing intense emotions; (b) perceiving these emotions as intolerable, unacceptable, or uncontrollable; and (c) engaging in efforts to escape or avoid these emotions, which provides short-term relief but maintains difficulties with emotion regulation in the long term. 33 Transdiagnostic protocols target core elemental vulnerabilities present across diverse diagnostic categories that address the needs of adolescents with co-occurring mental health concerns. In this MA, the highest SMD of PTSD for pre- versus post-intervention was present in transdiagnostic UP-A, followed by TF-CBT, prolonged exposure, and cognitive-behavioral approach-based interventions, which were found to be more efficacious than CBITS, web-based interventions, and supportive counseling, as reported in MA by Xiang et al. 34 as well. While Gillies et al. 35 (children and adolescent sample) and Hudays et al. 36 (children, adolescents, and adults) asserted that EMDR, CBT, and supportive therapy were equally effective, in our analyses, EMDR had a larger effect size than supportive counseling, with a small to medium effect size and variable efficacies of different types of cognitive-behavioral models of therapy. Among these, TF-CBT had large effect sizes and CBITS had small effect sizes. Cognitive restructuring has also been reported to have a large effect size. The RRFT, an integrated approach to the CBT model, motivation, contingency, and other behavioral domains, was found to have a large effect on a specific trauma (sexual assault). A small effect size was present in web-based intervention, possibly due to a weak therapeutic alliance between the facilitator and adolescent or issues related to web accessibility. Low efficacies were also reported in school counseling and control conditions (TAU). Price et al. asserted that a low participation rate was reported by male adolescent participants, specifically in app-based modules for PTSD intervention. 37 Contrarily, higher efficacies were reported in face-to-face interactions of client-therapists, such as in UP-A and TF-CBT, than in online psychological treatments, possibly due to a strong therapeutic alliance formation. 38 The combined effect of psychological interventions for comorbid depression was large 1.29 (RCT), which is higher than the effect sizes reported in Peters et al. 14 and similar medium to large 0.79 effect sizes (non-RCT) as reported in Carlucci et al. (mixed age sample). 39 The analysis of effect sizes suggests that all the psychological intervention groups had large efficacies in alleviating PTSD symptomatology. However, on further segregation, the RCT experimental group was found to have the highest effect size when compared with the control group or non-RCT intervention group for PTSD. According to Davis et al., 40 group interventions for children and adolescents yielded a medium effect size; however, no such comparison was made in this MA. Findings of multimodal intervention and mind–body skill intervention were able to significantly reduce PTSD scores with a large effect size when compared to usual care and delayed intervention. 41 Since both interventions included mind- and body-focused activities, such sessions could have improved non-attachment and empathy, thus reducing interpersonal distress and rejection sensitivity, EMDR reconsolidating painful memories, and promoting trauma recovery due to the focus on attentional regulation and the “present moment.”42–44
Limitations
This MA had a few limitations, such as the use of different diagnostic and screening tools, varied gender participation, and dissimilar traumatic incidents; hence, the interpretation of findings should be done with caution. Including only open-access articles might have led to an inherent bias in selection. Another limitation was the heterogeneity of the studies, as these epidemiological studies had varied trauma exposure, different settings of intervention delivery, different number of intervention sessions, different time points in follow-ups in RCTs and non-RCTs, PTSD comorbid conditions, and thus publication bias was seen. The effect sizes of group versus individual intervention settings were not calculated. Due to the fewer studies (RCTs or non-RCTs) in the current article, meta-regression still needs to be performed. Future researchers can analyze meta-regression to combine and contrast multiple subsets of studies (k > 10) in the presence of considerable heterogeneity.
Conclusion
Various psychological interventions, including CBT, TF-CBT, RRFT, and unified protocol-trans-diagnostic approaches, are efficacious in alleviating core PTSD symptomatology in adolescents. Larger and multi-centric/multi-country RCTs, RCTs in school settings in group format, and RCTs on transdiagnostic protocols for PTSD and comorbid mental health conditions need clinicians’ and researchers’ attention. As PTSD in adolescence could be complex, cultural variations in established psychological interventions can be focused on by future researchers.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
This study is approved by an Institutional Ethics Committee vide reference no. IEC-462/17.06.2022. RP-12/2022.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is part of the research project funded by ICMR (Indian Council of Medical Research) with project number 3/1/3/10/M/2022-NCD II.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.