
Abstract
Background:
A healthy lifestyle is important for recovery, coping with life’s stresses, minimizing the occurrence and impact of health issues, and improving quality of life. Maintaining a healthy lifestyle may help in preventing or delaying the onset of many health problems.
Methods:
A quantitative research approach with a randomized control trial (RCT) was adopted. 130 outpatients were randomized to experimental and control groups. The data were analyzed by SPSS version 28.8 and R software.
Results:
Waist circumference (WC) significantly differed between the experimental group and the control group (F = 14.87, P < .001). There was a decreasing trend in weight in the experimental group across the three time points (baseline to the second assessment), as compared to the control group (F = 4.29, P = .01). Quality of health of the subjects as measured by the visual analog scale (VAS) of the Euro Quality Of Life (EQ5D) significantly differed (F = 87.47, P < .001). Post-intervention, the percentage showed marked improvement in the experimental group.
Conclusion:
The results of this study support that counseling about a healthy lifestyle is effective as long-term strategies to avoid weight gain, engagement in adequate physical activity, taking nutritious food and maintaining healthy sleep can, in the long run, prevent metabolic syndrome. These interventions can be delivered at a low cost, are safer and practically feasible and may have a long-term impact on the quality of life.
Counseling about healthy lifestyle is effective as a long-term strategy to avoid weight gain. Engagement in adequate physical activity, eating nutritious food and maintaining healthy sleep, can in the long run prevent metabolic syndrome, among persons with severe mental illness (SMI).Key Message
Worldwide, depression affects 264 million, bipolar disorder affects 45 million, and schizophrenia and other psychotic disorders affect 20 million people. 1 Second-generation antipsychotics (SGA) have emerged as the main pharmacological treatment for persons with severe mental illness (SMI) as these drugs have lower extrapyramidal side effects.2,3 However, patients treated with SGA have raised concerns about increased metabolic effects. 4 Furthermore, they suffer from obesity, lifestyle issues, and poor physical fitness, all of which are exacerbated by the use of SGA. 2
Additionally, they are linked with abnormal metabolic alterations (dyslipidemia and insulin resistance), which can also be thought of as independent risk factors for cardiovascular disease (CVD) and diabetes. 4 Persons suffering from mental illnesses may face stigma and inadequate physical and mental health care, causing them to struggle with ADL (activities of daily living). 5 A healthy lifestyle is important for recovering, coping with life’s stresses, minimizing the occurrence and impact of health issues, and improving quality of life. Maintaining a healthy lifestyle may help prevent or delay the onset of many health problems. 6 Keeping healthy is rarely at the top of most people’s lists of “things to do” in their busy lives. 7 Patient-centered approaches in healthcare settings can have better outcomes than traditional advice-giving, especially related to lifestyle change.
Observational studies have consistently shown that making healthy lifestyle and behavior choices such as being more physically active, maintaining a healthy weight, and eating a diet that is low in fats and rich in fruits, vegetables, and whole grains can prevent or delay the burden of chronic disease and their consequences. 8 Research indicates that people with SMI can prevent and reverse psychotropic-associated weight gain, develop healthier eating and exercise habits, and benefit physically by losing weight. 9 Holistic health services offered by the nursing team in the adult psychiatry unit had shown a reduction in body mass index (BMI). 10
Despite the value of a comprehensive approach to care, mental and physical health services are frequently separated for those with SMI. Mental health nurses are crucial for promoting health, enhancing general well-being in those with SMI, and creating a more person-centered, integrated approach to physical and mental healthcare (Plourde, 2012). 11
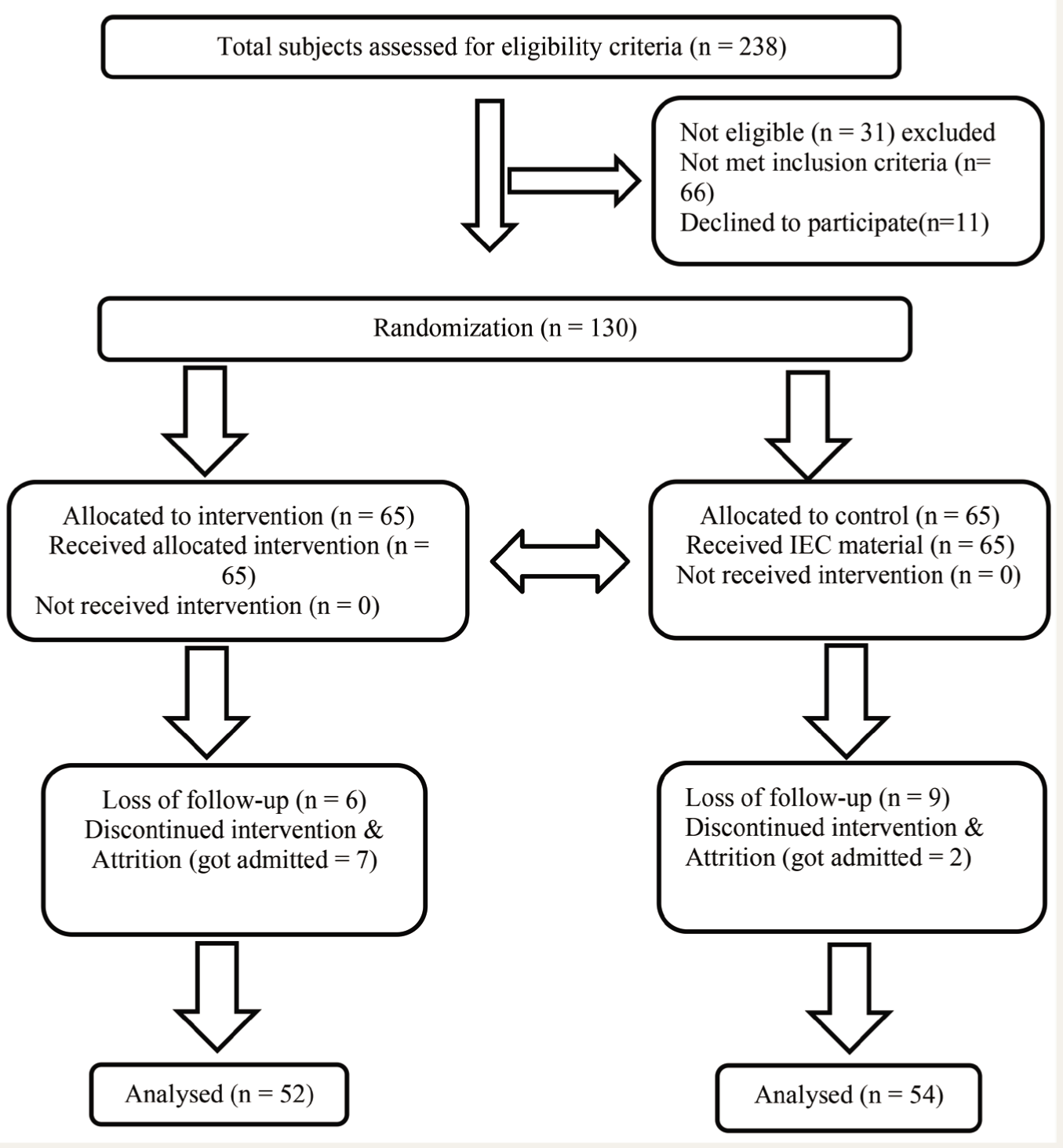
The aim of the present randomized control trial (RCT) was to test the efficacy of nurse counseling versus information, education, and communication (IEC) material on the promotion and maintenance of healthy lifestyles among outpatients receiving antipsychotics (Figure 1). The present study was based on Pender’s health promotion model. 12
CONSORT Flow Diagram of Outpatients on Antipsychotics who Received Healthy Lifestyle Counseling and IEC Group.
Methods
Study Design
For the present study, a quantitative research approach with a RCT was adopted.
The setting of the present study was the outpatient department (OPD) of adult psychiatry services at the tertiary mental health institute of South India. The sample included outpatients receiving antipsychotic treatment, meeting the inclusion criteria, and being accompanied by their family caregivers, those who stayed with them for 6 months or more.
Inclusion and Exclusion Criteria
Subjects between the ages of 18 and 45 years and both genders were diagnosed with schizophrenia (F20-29), bipolar affective disorder (BPAD) (F30-39), or schizoaffective disorder (F25) as per ICD-10 classification of mental disorders, on the same antipsychotics for a minimum duration of 3 months and above, with a waist circumference (WC) below 40 inches for males and 35 inches for females (As per NCEP/ATP-III guidelines for metabolic syndrome), and family caregivers staying with the patients for 6 months or more were invited to participate in the study. Outpatients who could not attend regular follow-ups on the scheduled dates or had deterioration of symptoms and were admitted to the hospital were considered dropouts.
Patients
Patients receiving the same antipsychotics for a minimum period of 3 months and above were identified to ensure the consistency of the antipsychotic effect. The researcher explained the purpose and nature of the study as well as the risks and benefits of participating in the study. Patients who met the inclusion criteria and consented (written informed consent) to participate were assigned a code number and randomized to the experimental group (intervention group) and control group (IEC group) by the clinical senior residents (qualified psychiatrists) who were not part of the research team. Informed written consent was obtained from the patients who were included in the study.
Subjects were randomized by the biostatistician using the research randomizer (version 4.0) software and a computer-generated random number table. These randomization codes were implemented using an allocation concealment method. The entire process of generation of randomization codes, as well as the allocation concealment procedure, was coordinated by the biostatistician, who was not involved in the recruitment, assessment, or intervention to prevent bias.
“G power software” was used to calculate the sample size for the study. Given the nature and the various time points, the sample size for each group was calculated as 47 by keeping cohort effect size at 0.15, α at 5%, power at 80%, and assuming correlation among Repeated Measures at 0.5. Keeping the attrition rate at 30%, the sample size was calculated to be 65 in the experimental group and control group.
The experimental group received counseling on healthy lifestyles, including diet, physical activity, and healthy sleep, along with their usual care. The control group received IEC material on healthy lifestyles based on the components of a healthy diet, physical activity, and sleep quality, along with treatment as usual (TAU). The content of counseling and IEC was finalized by consultation with experts in the fields. The nurse counselor received training in behavioral therapy and lifestyle medicine.
The Procedure of Data Collection
Based on their individual needs and socio-economic background, and following a comprehensive assessment of the tools outlined in Table 1 as well as each patient’s diet, physical activity, and sleep quality, the intervention group subjects (experimental group) received personally relevant feedback and patient-tailored individualized counseling in a single session lasting for 30–40 minutes when the subjects came to the follow-up OPD and after that by phone call every week up to 1 month. Every 15 days, up to 6 months, motivational phone calls were made to the subjects to identify their barriers (e.g., not feeling like exercising, getting tired, lack of time, feeling more sleepy, unable to control hunger, lack of motivation, increased screen time and medication non-compliance) and encourage them to follow a healthy lifestyle (i.e., counseling components on diet, physical activity, and healthy sleep). The second and third assessments with WHO STEPS 9 , Euro QOL (EQ-5D-3L) (EQ, 2013), Pittsburgh Sleep Quality Index (PSQI), 13 anthropometric and biochemical parameters such as fasting blood sugar (mg/dL), and lipid profile—were done in the 3rd month, and the 6th-month, respectively, when the subjects visited the hospital for their regular follow-up. The counseling was given by the nurse researcher under the guidance of senior nursing faculty and psychiatrists in the OPD.
Tools Used for Data Collection.
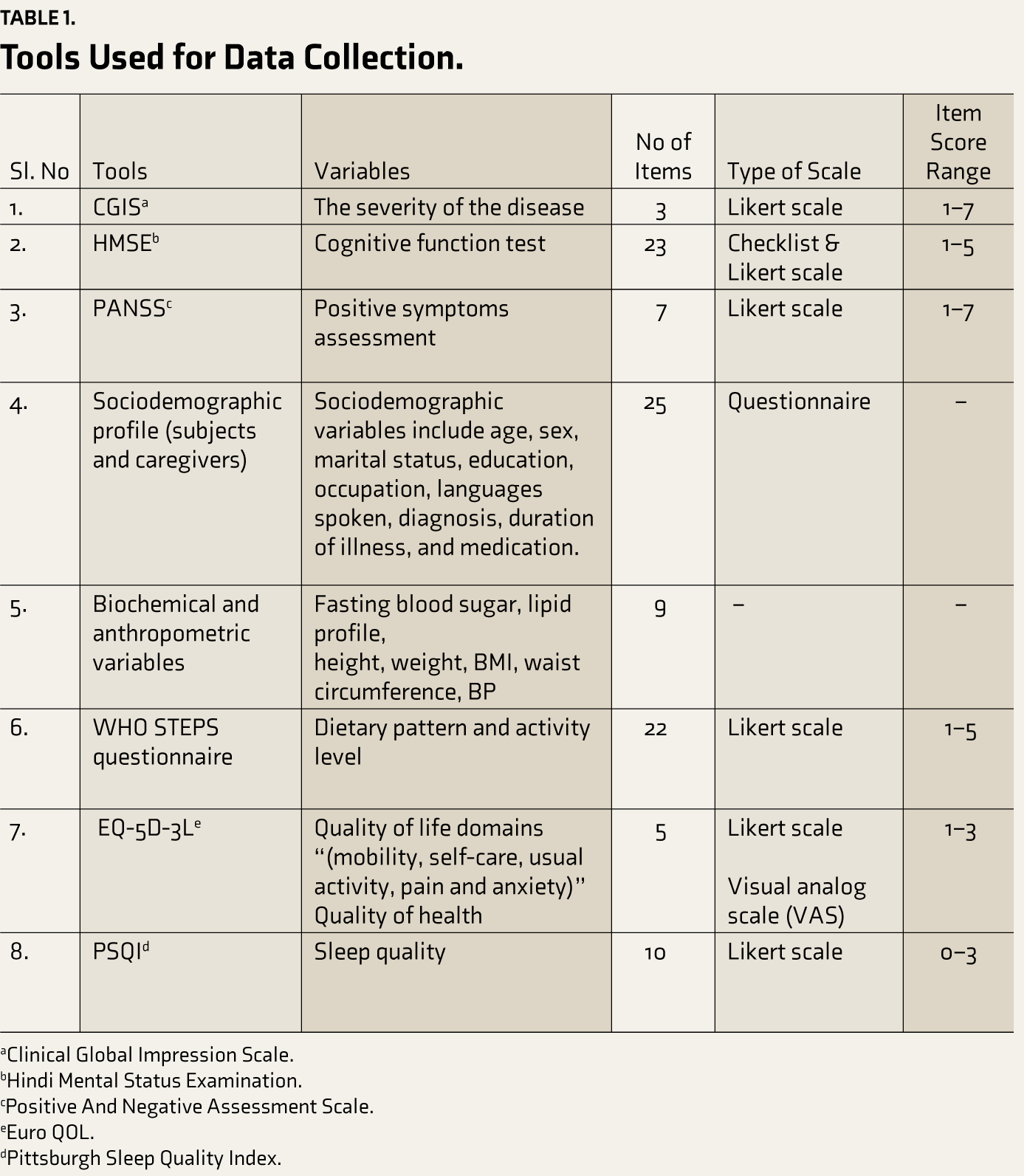
aClinical Global Impression Scale.
bHindi Mental Status Examination.
cPositive And Negative Assessment Scale.
eEuro QOL.
dPittsburgh Sleep Quality Index.
The subjects assigned to the control group received TAU with IEC material on healthy lifestyles. After the final data collection, the control group was also invited to attend healthy lifestyle counseling.
Data Analysis
The collected data were coded, entered, and analyzed by using SPSS version 28.8 and R software. Of the 130 subjects who were randomized to the intervention group and IEC group, 24 subjects who had dropped out of the follow-up were considered non-completers. Thus, for the analysis, data was available from 106 subjects in total, that is, 52 subjects in the experimental group and 54 subjects in the control group. The normality of all variables was tested with the Kolmogorov-Smirnov Z test. Normally distributed study variables were summarized using the mean and standard deviation (SD). Continuous study variables (both subjects and outcome) that did not meet the assumptions of normality were summarized using the median, 25th and 75th interquartile range. The clinical parameters did not follow normality at three-time points; thus, Analysis of Variance “Aligned Rank Transformed Data ANOVA (ART ANOVA)” was applied to check for the existence of a significant relation between the three-time points, that is, at the line, at 3rd month and 6th-month post-counseling assessments.
Results
Out of 130 subjects randomized to the experimental group and control group, 24 subjects had dropped out. The dropouts were due to loss of follow-up (n = 6 in the experimental group & n = 9 in the control group), discontinued intervention due to change in symptoms, and hospitalization due to illness relapse (n = 7 in the experimental group & n = 2 in the control group).
The demographic variables showed that 52.3% of the subjects were male in the intervention group, that is, the experimental group, and 55.40% in the control group. A majority of the subjects in both groups were educated up to the intermediate level, that is, 46.2% and 56.9%, respectively. The median, 25th and 75th percentile of the duration of illness in the experimental group and control group was found to be 6.00 (4.00, 10.00) and 5.00 (4.00, 10.00). Among experimental group subjects, 61.10% were diagnosed with schizophrenia, 10.80% with schizoaffective disorder, 6.20% with depression, 3.10% with mania, and 16% with BPAD. Among control group subjects, 58.50% were diagnosed with schizophrenia, 21.50% with schizoaffective disorder, 18.50% with BPAD, and 1.53% with mania. Among the experimental group, 98.46% and control group, 93.84 % were taking SGA. Also, it was observed that 89.20% of the subjects in the experimental group and 95.40% in the control group received no counseling on healthy lifestyles before (Table 2). A comparison of the demographic characteristics of the experimental group and control group shows that the groups were homogeneous.
Baseline Clinical and Demographic Profile of the Groups.
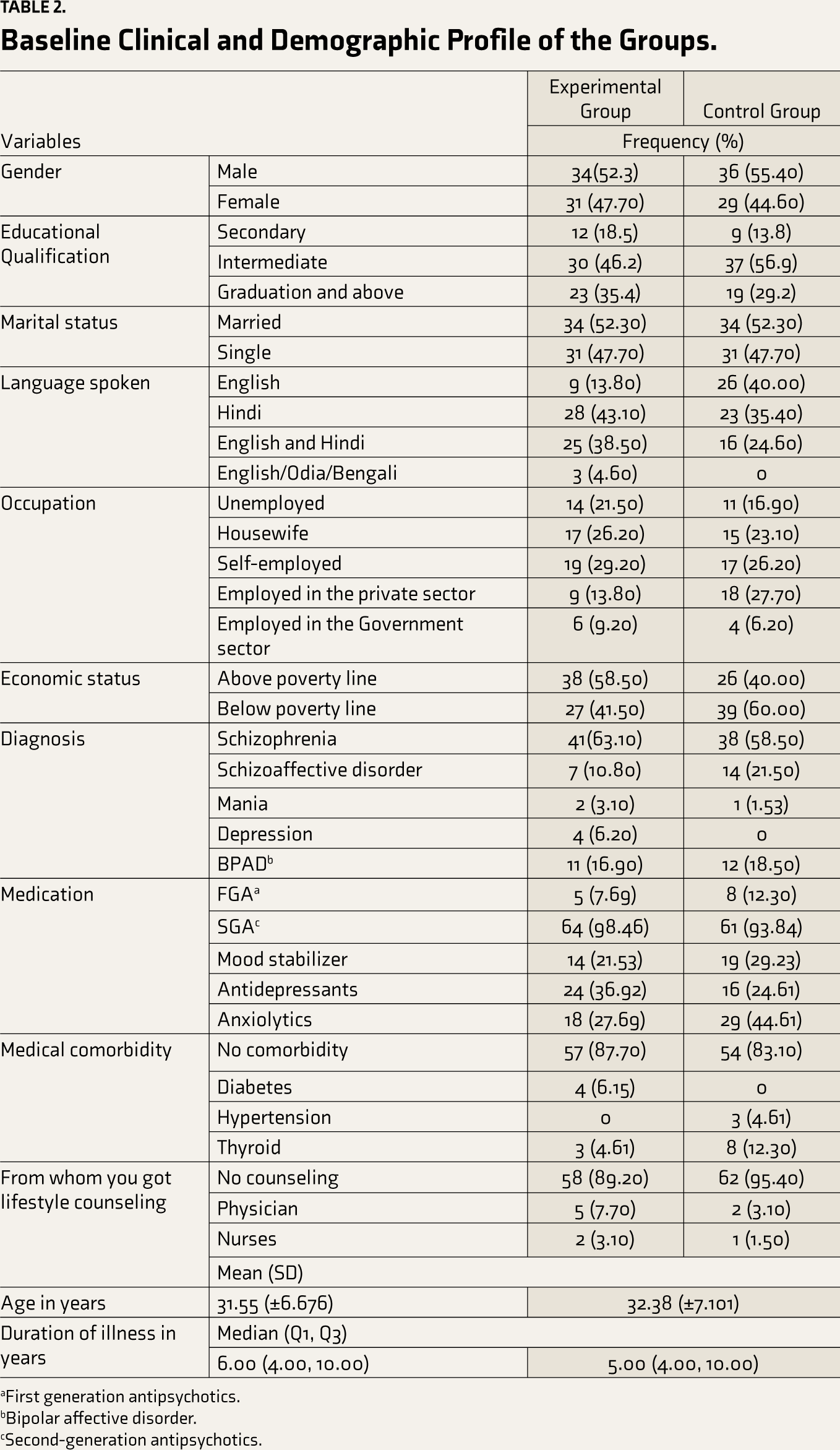
aFirst generation antipsychotics.
bBipolar affective disorder.
cSecond-generation antipsychotics.
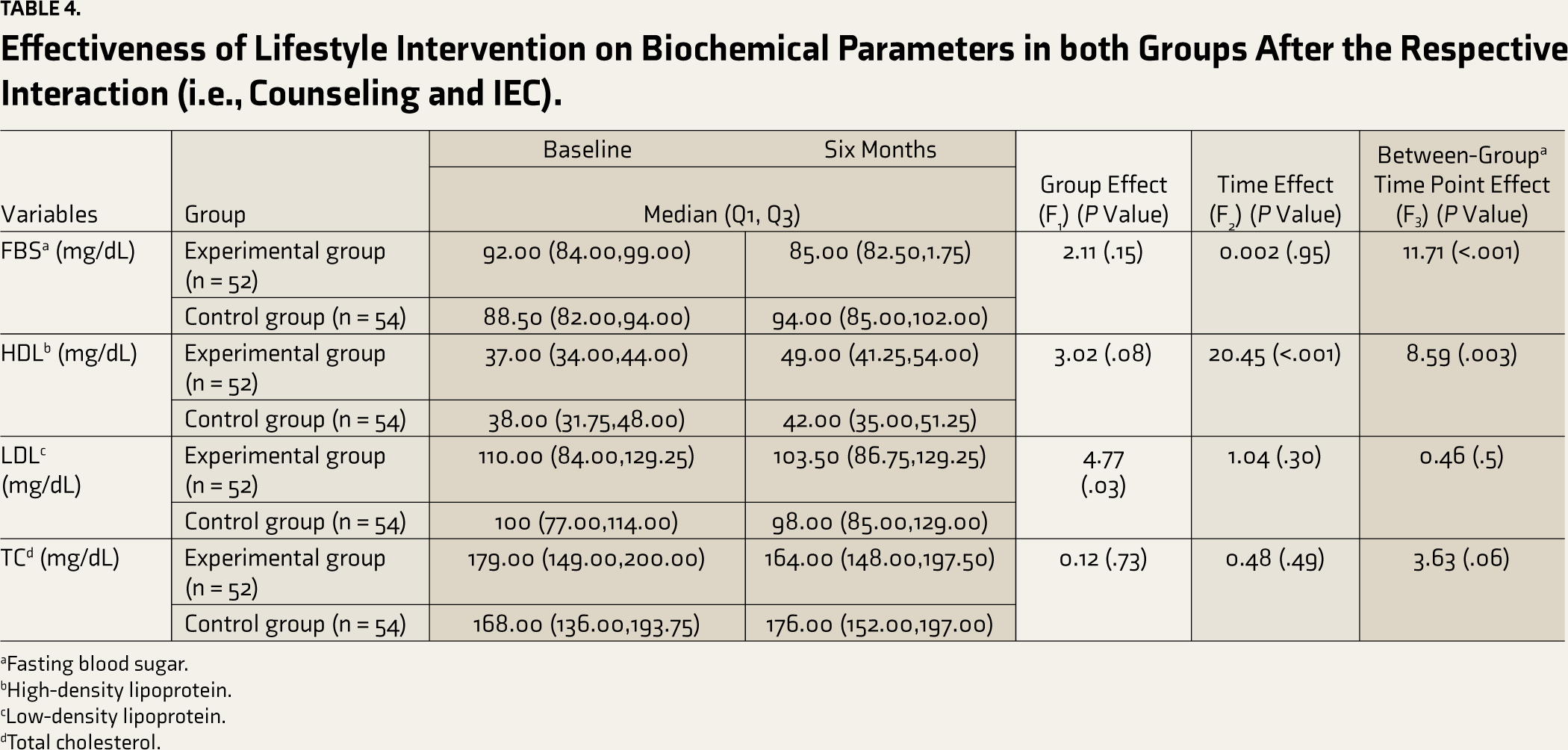
WC significantly differed between the experimental group and control group (F = 14.87, P < .001). In the first and second follow-ups, the results show that there was a slight increase in the WC in the control group. In contrast, there was a relative decrease in the experimental group that differs significantly between the groups (F = 15.42 & P < .001). The overall weight difference is significantly (F = 4.90, P = .03) more in the experimental group than in the control group. There was a decreasing trend in weight in the experimental group across the three-time points (baseline to the second assessment) as compared to the control group (F = 4.29, P = .01). In the experimental group, compared to the baseline, there was a decreasing trend in BMI. Meanwhile, the control group showed an increase in BMI over time. The change in BMI from baseline to two post-intervention time points differed significantly between the experimental group and control group (F = 12.80, P < .001) (Table 3). Diastolic BP showed a significant difference between the groups (F = 4.18, P = .04). The levels of FBS (fasting blood sugar) (mg/dL) (F = 11.71, P < .001) and HDL (High-density lipoprotein) (mg/dL) (F = 8.59, P < .003) significantly differed between and within the group. The ART ANOVA value between the group and three-time point of LDL (low-density lipoprotein) (mg/dL) (F = 0.46, P = .50) and of total cholesterol (mg/dL) (F = 3.63, P = .06), was not statistically significant (Table 4).
Effectiveness of Lifestyle Intervention in both Groups After the Respective Interaction (i.e., Counseling and IEC).
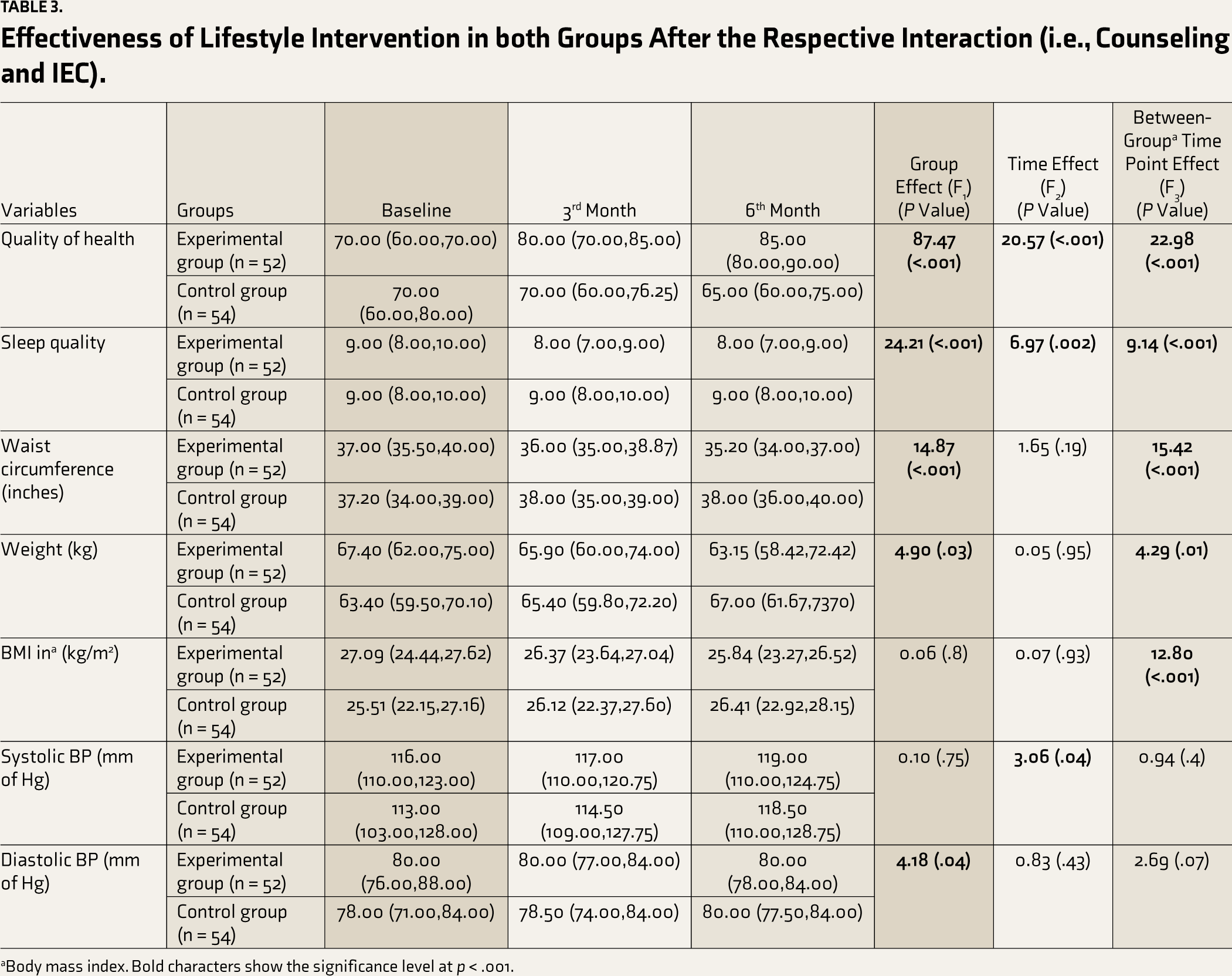
aBody mass index. Bold characters show the significance level at p < .001.
The quality of health of the subjects as measured by the visual analog scale (VAS) of the Euro QOL (EQ5D) significantly differed between the experimental group and the control group (F = 87.47, P < .001). There was an increase in the scores of VAS of Euro QOL at the first and second follow-ups in comparison to the baseline in the experimental group with the control group. The change in VAS score (from baseline to third and sixth follow-up) was found to differ significantly between the two groups (F = 22.98, P < .001). Sleep quality measured by (PSQI significantly differed between the two groups (F = 24.21, P < .001). In the experimental group, the global PSQI (Pittsburg Sleep Quality Index) score decreased over time. Meanwhile, in the control group, the same. The change in PSQI (from baseline to 3rd and 6th-month assessment) was found to differ significantly between the groups (F = 9.14, P < .001) (Table 3).
The dietary pattern as measured by WHO STEPS was compared within and between the groups at three different time points, that is, at baseline, 3 months, and 6 months. The results showed an increase in the weekly consumption of fruits. In the experimental group, 53.8% started consuming fruits 3–4 days a week, whereas 64.6% consumed fruits 0–2 days a week. This shows there was an increment in their fruit intake. A chi-square test was conducted to assess the difference in the percentage of improved versus not improved. It turned out to be statistically not significant (χ2 = 0.08, P = .78). In the experimental group, at baseline, 44.6% reported consuming vegetables 3–4 days a week. This percentage increased to 64.6% (5–7 days a week) at the 6th-month post-counseling assessment, whereas, in the control group, the percentage decreased from 50.8% at baseline (consuming vegetables 3–4 days a week) to 15.4% at the 6th-month (consuming vegetables 5–7 days a week). The vegetable intake increased in the experimental group as compared to the control group, but this change was not statistically significant (χ2 = 2.72, P = .09).
Effectiveness of Lifestyle Intervention on Biochemical Parameters in both Groups After the Respective Interaction (i.e., Counseling and IEC).
aFasting blood sugar.
bHigh-density lipoprotein.
cLow-density lipoprotein.
dTotal cholesterol.
In the experimental group, the percentage of subjects eating food prepared outside the home decreased from 3-4 (56.9%) times a week at the baseline to 0–2 (78.5%) times a week at the 6th-month post-intervention, that is, improved as compared to the control group. The test statistics showed a significant difference in the reduction of food intake (χ2 = 159.7, P < .001) that was not prepared at home. In the experimental group, the percentage of subjects working 3–4 days a week increased. The test statistics showed a significant improvement in the experimental group as compared to the control group in the 3rd month and the 6th-month assessments (χ2 = 108.98, P < .001). However, post-intervention, the percentage showed marked improvement in the experimental group.
In terms of the component of physical activity related to traveling, there was a significant improvement in walking and cycling among the subjects of the experimental group as compared to the control group across the time points (χ2 = 55.02, P < .001). In terms of recreational activities, the test statistics showed a significant difference between the groups with regard to the improvement in doing vigorous-intensity activities (χ2 =159.7, P < .001). The test statistics also revealed that there were significant improvements in the experimental group as compared to the control group in doing moderate-intensity activities (χ2 = 139.55, P <.001). In the component of time spent sitting and reclining in a day, the test statistics showed a significant reduction in the sitting time in the experimental group post-intervention at the 6th-month assessment as compared to the control group (χ2 = 173.89, P < .001). The outcomes demonstrated that lifestyle counseling was successful in increasing the amount of activity.
The results of the present study revealed that lifestyle counseling for outpatients receiving antipsychotics was an effective intervention in improving both dietary patterns and activity levels, as assessed by WHO STEPS in the experimental group, as compared to the control group.
Discussion
A randomized controlled trial (RCT) was conducted to evaluate the efficacy of nurse counseling in promoting and maintaining a healthy lifestyle among patients taking antipsychotics and attending outpatients at a tertiary hospital in south India. To the best of the researcher’s knowledge, this RCT is the first study to evaluate the efficacy of nurse counseling in promoting a healthy lifestyle among PwMI. The findings of the study demonstrated a positive change in the outcome variables (weight, WC, BMI, quality of life, diet, physical activity, and sleep) in the experimental group that had received nurse counseling on the promotion and maintenance of a healthy lifestyle. However, the IEC group (control group) showed little improvement. The support of family members could be an important motivation for maintaining a healthy lifestyle among persons with SMI. Thus, including family caregivers in counseling on healthy lifestyles could increase adherence.
It can be inferred that when clinical symptoms improve, BMI, weight, and WC also improve. Sleepiness decreased in the healthy lifestyle intervention group as compared to the control group, even though the sleep quality did not change significantly. The change in blood pressure from baseline to two post-intervention time points did not differ statistically between the experimental group and the control group. The biochemical variables did not show significant differences as not statistically significant. This might be because the assessments were done at 6-month intervals, and variables like LDL (low-density lipoprotein) and TC (total cholesterol) require more time for significant changes to occur. The quality of life observed by Euro QOL 5D has shown that the subjects have verbalized that they observed improvement in all five domains, specifically in anxiety level and pain. The VAS shows that after continuous counseling sessions, the subjects experienced better health between the first and third assessments. The results contradicted the “multidisciplinary lifestyle-enhancing treatment for inpatients with SMI (MULTI)” study that reported the linear multilevel regression estimating treatment effects showed insignificant differences between EQ-5. Nearly all variables in both MULTI and TAU, where further within-group results were shown, showed a rise in QoL. 14
Dietary patterns, as measured by WHO STEPS, showed an increase in the weekly consumption of fruits. In the experimental group, 53.8% started consuming fruits and vegetables 3–4 days a week, whereas 64.6% consumed fruits and vegetables 0–2 days a week. In the experimental group, the test statistics showed a significant difference in the reduction of food intake (χ2 = 159.7, P < .001) that was not prepared at home.
In terms of doing an activity, the test statistics showed a significant improvement in the experimental group as compared to the control group in the 3rd month and the 6th-month assessments (χ2 = 108.98, P < .001). Even though the test statistics showed no statistically significant difference between the groups with regard to the improvement in moderate-intensity activity (χ2 = 30.19 P = 3.92). However, post-intervention, the percentage showed marked improvement in the experimental group. In terms of traveling, there was a significant improvement in walking and cycling among the subjects of the experimental group as compared to the control group across the time points (χ2 = 55.02, P < .001).
The change in WC from baseline to two post-intervention measures was found to differ significantly between the experimental group and control group (F = 15.42 & P < .001). Comparable results were found in study, 19 where a statistically significant difference in WC was detected differences between the control and intervention groups. The change in weight from baseline to two post-intervention differed significantly between the two groups (F = 4.29, P = .01). These results are in line with those of previous studies.15,16 The change in BMI from baseline to two post-intervention time points differed significantly between the two groups (F = 12.80, P < .001). This change is due to a significant change in the weight in the experimental group as compared to the control group. The results agree with the results of some previous studies.16-18 A systematic review 20 showed that when compared to the TAU group, the intervention group’s mean difference of mean weight loss across all trials was statistically significant and favorable (0.64, 95% CI: 0.89, 0.39) (Z = 5.03, P < .001). The change in blood pressure from baseline to two post-intervention time points did not differ statistically between the experimental group and the control group. It has been found that BP takes a longer duration to show significant effect. 21 The ART ANOVA value between the group and three-time point of LDL (mg/dL) (F = 0.46, P = .50) and of total cholesterol (mg/dL) (F = 3.63, P = .06) was not statistically significant. This might be because the assessments were done at 6-month intervals, and variables like LDL and TC require more time for significant changes to occur.5,17 On the contrary, studies 22 reported that biochemical parameters were within normal range. Lifestyle counseling for outpatients receiving antipsychotics can be an effective intervention in improving both dietary patterns and activity level.23,24
Strengths and Limitations of the Study
The strengths of the present study are that it is a first-of-its-kind study using a “Randomized control trial” to evaluate the efficacy of nurse counseling in the promotion and maintenance of a healthy lifestyle among outpatients receiving antipsychotics. The samples are homogenous. Telephonic follow-ups and meeting the subjects during follow-up in the OPD at 3-time points ensured motivation as well as helped to identify and respond to the doubts, challenges, and problems encountered by the persons with mental illness receiving antipsychotics. Counseling was individually tailored to suit each patient’s needs and cultural practices related to diet and physical activity. The regional language was used for the data collection and intervention. The intervention was formulated based on the need perception of persons with mental illness receiving antipsychotics and their caregivers. The limitations of the study are that it was conducted in a specific geographic area in a single mental health center with a small duration of intervention and follow-up. The present study was not blinded. Although the change in clinical, anthropometric, and biochemical correlates of metabolic syndrome was found, to what extent the subjects will continue to adhere is uncertain. The study only included individuals with SMI, so direct comparisons with other mental illnesses and with the general population were not possible. The measures of diet, exercise, and sleep were based on subjects’ verbalization, which is an element of subjectivity.
Conclusion
This RCT highlights the outcomes of the nurse counseling on the promotion and maintenance of healthy lifestyles among persons with mental illness taking antipsychotics and getting treatment on an outpatient basis. The counseling was effective, and there was significant improvement (P < .05) in the clinical, anthropometric, and biochemical correlates of the outpatients taking antipsychotics. The novelty of the present study is that no such study has been conducted in the field as per the researcher’s knowledge. This study identified that caregivers, family, friends, and mental health professionals should support healthy lifestyle changes among persons with SMI taking antipsychotics. The results of this study support that counseling about a healthy lifestyle is effective as long-term strategies to avoid weight gain, engagement in adequate physical activity, taking nutritious food, and maintaining healthy sleep can, in the long run, prevent metabolic syndrome among this population. These interventions can be delivered at a low cost, are safer and practically feasible, and may have a long-term impact on quality of life and increased longevity among persons with SMI.
Footnotes
Acknowledgements
The authors acknowledge the authors whose studies were included in the meta-analysis. The authors also acknowledge all the subjects those who have participated in the study.
Data Sharing Statement
The data obtained from the patient could not be shared due to the patient confidentiality and the consent taken from the participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval
The study protocol was approved by the Institute Ethics Committee of Behavioural Science division of NIMHANS in March 2020. Institutional Ethics Committee letter No. NIMH/DO/IEC (BEH. Sc. DIV)/2020, also registered in the Control Trial Registry of India (CTRI). Registration number: CTRI/2020/07/026887, on: 29/07/2020]
Funding
The authors received no financial support for the research, authorship and/or publication of this article.