
Abstract
Background:
Physician grief, as defined by Kenneth Doka as disenfranchised grief, refers to “the grief that individuals experience when they incur a loss that is not openly acknowledged, publicly mourned, or socially supported.” The experience of patient deaths on the emotional health of young doctors is unknown. The after-effects like stress, anxiety, burnout, depression, and others indirectly have a potential impact on decision-making and patient care. The study aims to shed light on this underexplored dimension and advocate for appropriate training and support to promote physician well-being.
Methods:
A qualitative study with a phenomenological approach was used to help explore the lived experience of trainee doctors confronted with patient deaths. The data collection was done through focused group discussions (FGDs) with three groups of trainee doctors. A semi-structured interview guide was framed and focused on their experiences of initial reactions, coping, reflections, and unmet needs among participants. Each interview was manually coded, organized into subthemes, and further into larger themes. All authors agreed upon themes and subthemes.
Results:
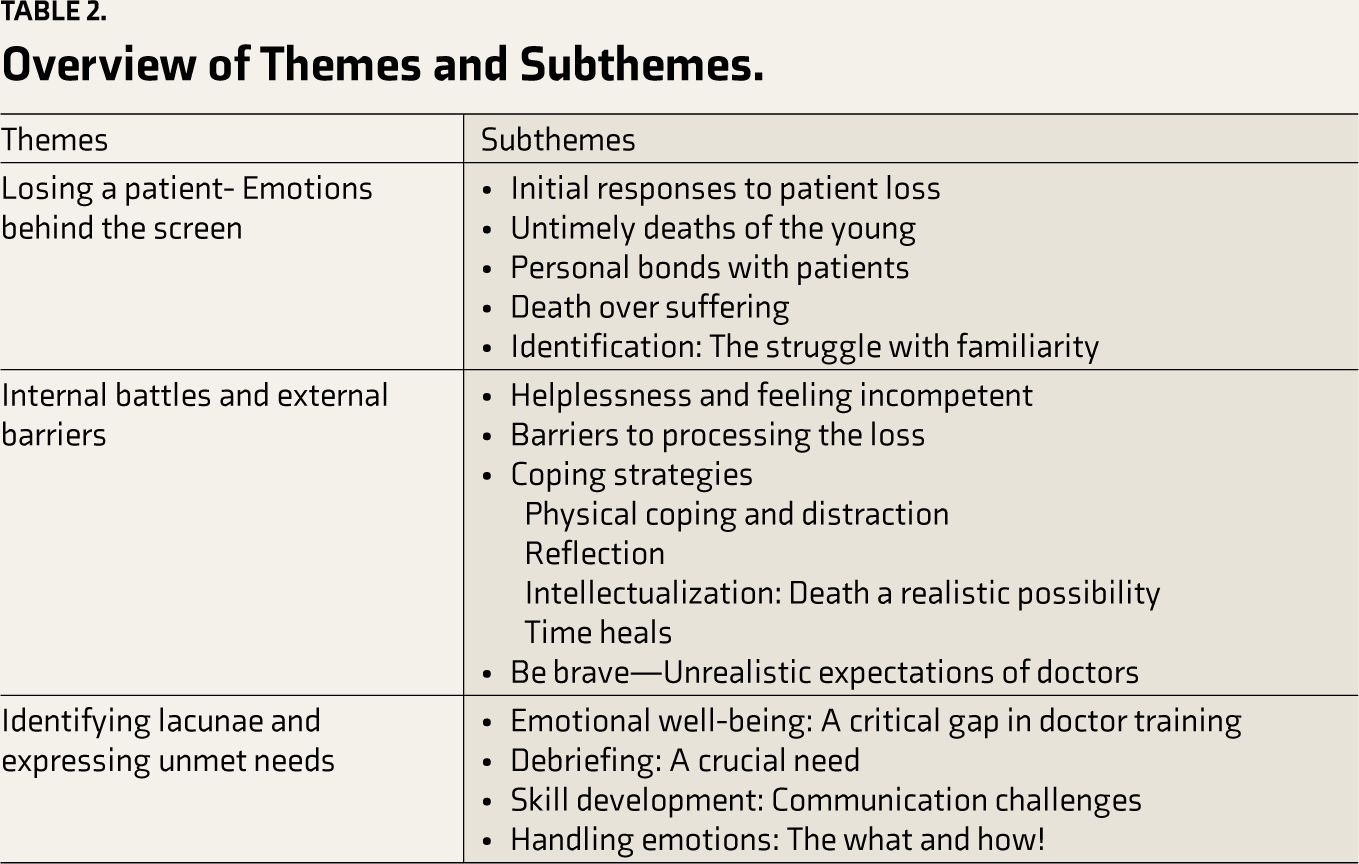
The findings are elaborated with necessary quotes taken from the transcripts of the FGDs. The main themes identified were (a) Losing a patient’s emotions behind the screen, (b) Psychological and Environmental battles, and (c) Identifying lacunae and expressing unmet needs.
Conclusion:
The study findings were corroborated by concepts of disenfranchised grief, iatrogenic distress, emotionally unavailable doctors, and poor coping abilities. It also advocates for protocols and proactive measures to support interns and resident doctors.
Doctors losing patients is inevitable, and the effect it has on young trainee doctors is not well understood. The impact it has on their mental health, physical health, and work is profound. A better understanding can advocate for developing strategies, necessary protocols, and soft skills modules in the early years of training and empower them in handling these difficult situations.Key Messages
While doctors are trained to comprehend the physiological processes of the body, identify disorders and illnesses, and apply their knowledge to alleviate pain. The concept of death is often perceived as a failure on the part of physicians. 1 Seldom do they understand that death is an intrinsic part of being a physician 2 and that the inevitable cannot be escaped. While experienced doctors have learned to deal with this predicament (effectively or otherwise), trainee and young doctors are mostly shocked when they face the death of individuals whose care they are involved in. Though grief is usually discussed at length in the context of caregivers, the immediate reaction to witnessing death by doctors and the emotional turmoil associated with this is less understood. 3 Physician grief, as defined by Kenneth Doka as disenfranchised grief, refers to “the grief that individuals experience when they incur a loss that is not openly acknowledged, publicly mourned, or socially supported.” 4 The impact of experiencing patient loss has a wide range, that is, from being insignificant to traumatic, especially for physicians in high-risk specialities like trauma, emergency, and oncology. Prolonged exposure to patient deaths compounds anguish, increasing the risk for stress, burnout, and depression, and potentially impacting decision-making and overall patient care.1,5 Global literature in the areas of grief awareness and training for young doctors is very limited.
In this study, we try to understand the experience of young- trainee doctors confronted with patient death, their ability to cope, and their perceived unmet needs. As reactions to stress and grief are contextual and extensively shaped by cultural factors, the study attempts to provide insights into experiences from India. The previous studies done in the area have looked at breaking bad news to the family, 6 stress and burnout, 7 anxiety and depression among young doctors. Nevertheless, no study has explored the lived experience of young doctors in losing patients. The study aims to shed light on this underexplored dimension to enhance our understanding and improve the ability to navigate challenging situations through educational interventions, ultimately promoting physician well-being.
Methodology
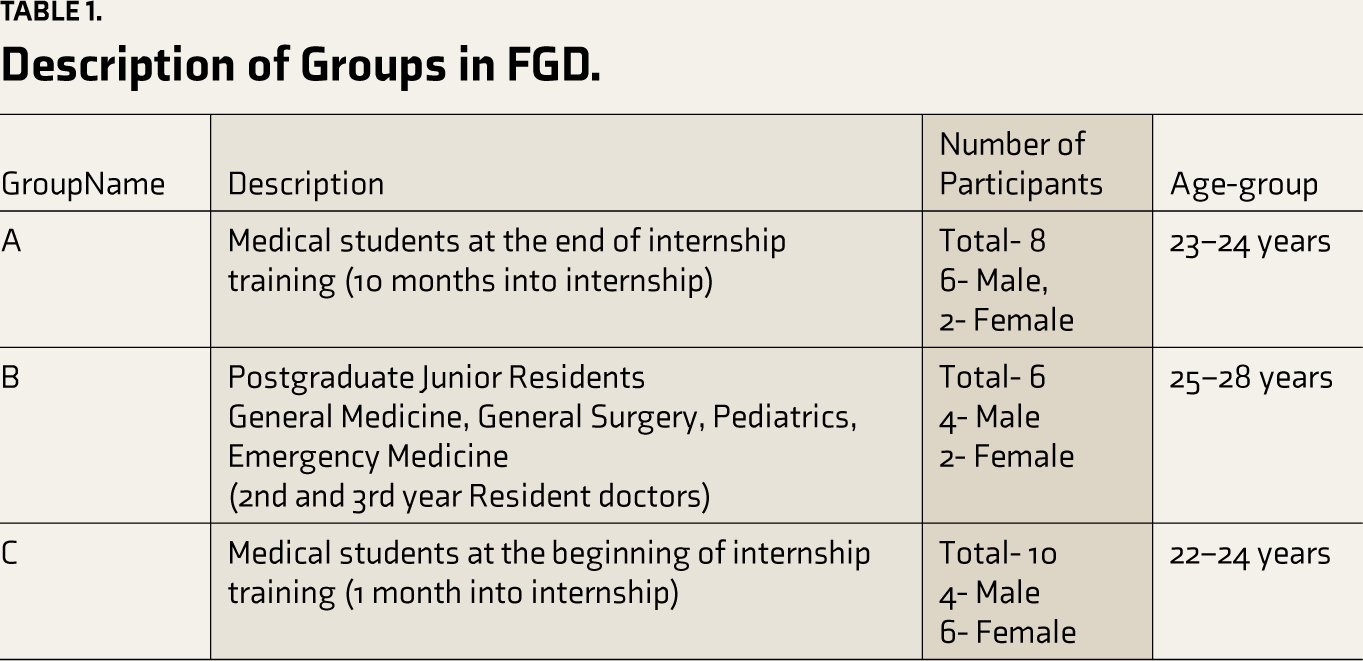
A qualitative study with a phenomenological approach was used to help explore the lived experience of trainee doctors who have experienced and confronted patient deaths. The phenomenological approach helps to understand the essence of a phenomenon (how and what) through the perspective of those who have experienced it. 8 This study was conducted in a tertiary medical college hospital after being approved by the institute’s ethics committee. The data collection was done through focused group discussions (FGDs) of three groups. The FGDs were conducted between October 2022 and March 2023. The three FGDs were of trainee doctors at the beginning of the internship, and toward the end of the internship, and postgraduate residents and groups had ten, eight, and six participants, respectively. A purposive sampling of trainee doctors who have witnessed one or more deaths during the period of training were chosen as participants for the FGD. An open invitation was sent out, and those who volunteered to participate were included on a first-come-first-come basis.
Written informed consent for participation and audio recordings were obtained from all participants prior to beginning the FGD. A semi-structured interview guide was made, which included questions on the experiences of participants on facing the deaths of patients. This gave a brief framework for the discussion and had open-ended questions on initial reactions, coping, reflections, and unmet needs. The questions also had probes enlisted to get a deeper understanding of these experiences. A few examples of the questions were “Describe your First death experience at work,” “Describe the emotions, thoughts, and other significant events attached to the experience,” “Could you describe your relationship with the patient,” “How did you cope?” “How prepared were you to handle such a situation?” “What is your judgment that would have made this difficult situation easier to deal with?” and “What were the difficulties you faced alongside experiencing death as a trainee doctor?” others. The authors conducting the FGDs were also involved in the process of reflexivity through making notes, journaling, bracketing their own emotions, and making observations of non-verbal nature in the interviews. They would then discuss and validate their observations of the interviews. The details of the participants of all three groups are described in Table 1. The FGD was moderated by a trained clinical psychologist (MR) with experience in conducting qualitative research. MR facilitated the discussion and rephrasing and paraphrasing were done when necessary. The first three authors transcribed the audio recordings. They and NV read the transcripts repeatedly. An inductive thematic analysis approach was thought to suit the study question better and give an in-depth understanding of the phenomenon.
Description of Groups in FGD.
To begin with, each interview was manually coded individually, and initial open codes were generated. The open codes were then rearranged and reorganized into subthemes and further into larger themes. The themes were reviewed, combined, and organized to form three major themes under which results are organized. The first three authors independently did these processes of coding and making subthemes and themes, which were then reviewed and concurred by NV. This process was done individually for all three groups, then combined, and overall results were generated. All three authors and NV concurred on the themes and subthemes.
Results
Socio-demographic Details
The participants of the study were medical students and resident doctors of a Tertiary Care Medical College and Hospital.
Thematic Analysis
The results of the thematic analysis are described in three major themes, with subthemes under them, and some also have categories within the subthemes. The results try to give an overview of the emotions, internal battles, and unmet needs.
Table 2 gives an overview of the themes and subthemes.
Overview of Themes and Subthemes.
Losing a Patient— Emotions Behind the Screen
This thematic analysis delves into the intricate emotional landscape of trainee doctors, providing insights into their immediate reactions, differential responses to patient demographics, and the complexities of forming personal connections in the face of loss.
Initial Responses to Patient Loss
Trainee doctors vividly expressed their immediate emotional reactions using terms like “sad,” “numb,” and “helpless.” A spectrum of emotions, like anger, sadness, and numbness, surfaced, and they especially felt angry when the patients were brought in late for care. The emotional toil was palpable and reflected a range of complex feelings.
Helpless, I wish that hadn’t happened. (Female - 24)
I was numb. (Female - 22)
I felt angry about the situation I was in, but it wasn’t directed toward me. (Female - 22)
Untimely Deaths of the Young
Trainee doctors experienced more profound emotional reactions to pediatric and young adult deaths, describing them as “scarring” and emotionally challenging. They experienced sadness and shock, which was related to the fact that they had not lived a full life, they had a family dependent on them, and sadness was also related to seeing devastated family members. However, in comparison, the intensity decreased for older adult deaths as the trainee doctors felt that they had lived a full life.
Losing a child is extremely scarring. (Male 27)
More than adult deaths, pediatric death for me is even more disturbing. (Female 23)
When a 90-year-old dies, you say okay, he lived his life. When a 9-year-old dies, I can’t say he lived his life. (Male 27)
I felt very bad because he was so young, some 29 or 30. (Female - 24)
Actually, affects us depending on the age of the patient… if the patient is young and the family is dependent on them, it will impact us as to how they are going to do and all this. (Male - 22)
Personal Bonds with Patients
Trainee doctors are the ones who see the patient from the time of admission. They see them for a longer duration and have lengthy conversations—history taking, discussing the need for investigations, discussing reports, treatment plans, and also discharge advice. The conversations are usually not limited to clinical conversations, and prolonged interactions and personal conversations make them feel connected and have personal bonds with the patients. Bonding was notably higher when patients shared personal details, were offered food, called by name/dear names, or treated like family. The loss of such patients was particularly emotionally challenging for the trainee doctors to handle.
Depends on the time you spent with the patient. (Female - 22)
More involved in his care and you have a bonding. (Male - 23)
I sometimes talk to the patients there…he used to call me and talk to me so nicely. I felt very weird(death) …especially because he used to call me and talk to me so nicely. (Male, 24)
Death Over Suffering
Trainee doctors revealed they often felt that it was better that a person died and preferred death over prolonged suffering, especially in the case of persons dealing with chronic illness. Some empathized (by putting themselves in the shoes of the patient) with their suffering and expressed a wish to die rather than live. Similarly, some even felt that letting go was a humane choice as compared to inhuman suffering.
I think suffering is much worse than death. (Female 23)
If I were in their position, I would have liked to die rather than to live. (Male 27)
Sometimes it’s better to let them go is what I feel. (Male 27)
Identification: The Struggle with Familiarity
Trainee doctors found it challenging to connect with patients who resembled deceased family members in terms of name, age, looks, diagnosis, or the events preceding death. The similarity of incidents usually led to emotional distancing, avoidance, and emotional hurdles in handling clinical situations.
The first death I saw in my life like my grandma’s, I’m still not able to come out of that. So, anyone with that name in the hospital, it’s very hard for me. (Female-22)
Internal Battles and External Barriers
Helplessness and Feeling Incompetent
Resident doctors, predominantly females, grapple with intense negative emotions—anger, negative intuitions, anxiety, and fear of negative outcomes. This emotional turmoil is closely tied to a cognitive sense of inadequacy, an overwhelming feeling of not having done enough, subsequently questioning their competency, and a pervasive sense of inexperience, particularly in delivering challenging news or discussing patient deaths.
It was an overwhelming feeling that I just watched someone die, and I couldn’t do anything. (Female, 24)
I knew something was going to happen, and I couldn’t do anything. (Female, 22)
I was very consumed by my emotions and couldn’t do anything. (Female, 23)
Barriers to Processing the Loss
Junior doctors face an overwhelming patient load on a daily basis, compelling them to swiftly move on from one task to the next, often without the luxury of processing the emotional weight of losing a patient.
No time to think about personal emotions; you have to move on to the next thing. (Female, 26)
They are not gonna give you timeout after the death. (Male, 28)
Coping Strategies
Physical Coping and Distraction
Residents resort to various physical activities, binge eating, and distractions like social media as coping mechanisms. Socialization emerges as a helpful strategy to navigate distress.
Gym and lift heavyweights.” (Male, 28)
Eating much food, I really wanted ice cream, and it was out of the blue.” (Female, 24)
Binge-watching or just scrolling on social media. (Male, 24)
Reflection
Some doctors highlight the therapeutic power of reflection, emphasizing its importance as a daily practice to process challenging emotions and experiences.
Can process it better on a daily basis, reflecting on what you see every day is important. (Female, 24)
Intellectualization: Death a Realistic Possibility
A coping strategy involves intellectualizing patient outcomes by acknowledging death as a realistic possibility, allowing doctors to approach such situations with a different mindset.
You need to realize that death is also a possibility. Nothing can prepare you for that; it can go either way, right? (Male, 22)
If the situation of the patient is bad, sometimes you need to tell yourself that death is actually a possibility. (Male, 22)
Do the most that you can; you can’t save everyone. (Male, 27)
Time Heals
While few actively engage with their emotions and seek therapy, others acknowledge that actively dealing with grief can lead to emotional strength and eventual acceptance.
I think acceptance that, you know, you try your best. (Male 27)
So dealing with that, I think it changes you over time. It makes you stronger emotionally; I think that’s helpful. (Male 27)
I seek therapy to train my mind. (Female, 24)
Be Brave—Unrealistic Expectations of Doctors
Junior doctors expressed a “felt” pressure to conceal their emotions, which stemmed from the fact that doctors have to get used to facing deaths, and deaths do not affect doctors emotionally. They also needed to conform to these societal expectations that doctors should remain stoic and not express their emotions. They had an intrinsic fear of judgment and were viewed as “weak” by peers, patients, and society, which discouraged them from openly expressing their emotions.
I don’t think people understand what you went through because they think that you’re a doctor; you should not be having those kinds of emotions. (Female, 23)
You have to put it (death) aside and move on. (Female, 23)
I will be judged. (Female, 23)
This nuanced thematic analysis delves into the multifaceted emotional challenges faced by resident doctors, highlighting coping mechanisms and the societal expectations that shape their experiences and emotional expressions.
Identifying Lacunae and Expressing Unmet Needs
Emotional Well-being: A Critical Gap in Doctor Training
The emotional well-being of doctors, particularly in the context of dealing with the profound grief following the loss of a patient, is a frequently overlooked aspect of their training. This deficiency in addressing emotional needs among junior doctors poses a significant challenge that warrants urgent attention.
Nobody is dealing with it, and they are so rude about how they speak about it (about patient deaths and how no discussion happens on the same). (Female, 24)
There may be a team of mental health experts that do routine screenings if some physician is under emotional stress, apart from the usual burnout, so they can pick it up and advise them on what to do. (Male, 22)
Debriefing: A Crucial Need
In the culmination of group discussions, residents and interns highlighted the pressing need for effective strategies to address grief and enhance support within healthcare teams. The absence of routine discussions among healthcare professionals, including consultants, residents, interns, and nurses, about their patients was noted. A considerable lack of guidance and support from seniors to junior doctors, particularly in handling deceased patients, was emphasized. Participants expressed the necessity of taking time out and having debriefing sessions to address their emotions.
Maybe just take a moment with your consultants. Even if a consultant seems like a far stretch, at least your PGs(seniors) because they are just one or two years older than us. I think that would have helped me definitely when that happened. (Female, 22)
A team meeting to discuss the emotions faced by the people. (Male, 22)
Post acknowledgment would be better because prior sensation, not always you will be able to relate because if something has not even happened to you. (Male, 22)
Skill Development: Communication Challenges
The junior doctors in our study candidly acknowledged their awareness of certain limitations, particularly in their ability to effectively communicate sensitive information, such as breaking bad news or declaring a person’s death to their family. Their reflections put forth a perceived deficiency in skills. Many expressed feeling relief not being positioned at the forefront and often finding themselves being observers in these difficult conversations. The recurring sentiment among these young healthcare professionals was a desire for targeted training in communication and positive emotional coping strategies. They believed that such training could not only enhance their ability to handle challenging situations but also alleviate concerns about potential confrontations and violence.
I wouldn’t have handled it, definitely, if I was alone. I was thinking about that aspect—what if I was alone? (Female, 22)
We’re asked to observe but not taught how to. As interns, we kind of hide and just watch what’s happening because we’re not really the forefront people who talk to the family. (Female, 23) [On experience with bereaving families and breaking bad news]
But no one ever explained it; it was like they just wanted to include that in the PowerPoint. It was like, they just wanted to include that. (Female, 23)
Handling Emotions: The What and How!
The junior doctors recognized the imperative need to face emotionally charged situations such as patient deaths. However, they faced difficulties in identifying and processing their own emotions in these difficult circumstances. A recurring theme was the necessity for an effective outlet to channel these emotional experiences, emphasizing the inadequacy of awareness of their own emotions.
You can’t actually process things when you don’t even understand what you’re going through. (Female, 22)
I try to process them, but I’m not really sure what to think about it. (Male, 22)
Discussion
The study looks to understand better “the other side of iatrogenic suffering.” 9 While not all patient deaths lead to significant emotional distress, certain cases profoundly impact the emotional well-being of trainee doctors.10,11 The intensity of emotions in response to the death of patients in trainee doctors was influenced by the age of the patient, relatability, closeness to the patient, and their ability to cope, which were similar to studies done earlier. 12 The participants also felt the need not to have emotional reactions so as to meet societal expectations of emotional strength and avoid being judged by peers. The medical profession fosters and favors the emotionally detached doctor. This has been explored and described in a qualitative study as “anti-emotional expectations,” the effects of which are not entirely known. 13 This “conspiracy of silence” 14 engrained in the minds of young doctors encourages repression of emotions and poses a high risk for developing post-traumatic stress disorder and burnout. However, the demanding workload often limits their capacity for reflective practices, prompting the adoption of indirect coping mechanisms such as physical activities, binge eating, 15 and binge-watching. This is in accordance with Papadatou’s professional grieving model 16 and dual process model, 17 where doctors move away from the experience of loss toward their professional role to get their job done. However, some coped by seeking support from colleagues, family, or friends, engaging in self-care practices and physical activity, and utilizing institutional support structures such as counseling services.
While a few participants dealt with deaths by talking to their colleagues and rarely with senior consultants.
Facing the death of patients was usually associated with a sense of helplessness, feeling incompetent, and questioning their abilities. 18 The trainee doctors also had difficulty in bringing emotions to self-awareness and identifying their distress, which could have a cultural influence, where actions are focused on more than emotions, which is more pronounced when choosing to be a medical professional. For doctors to have good emotional well-being, it is imperative that doctors can express their feelings without fear of judgment and criticism. 19 The trainee doctors acknowledged that they had difficulty in breaking bad news and communication, and that was compounded by the fear of violence from the patient’s relatives. The limitations of the study are that all interviews were FGDs, there is a possibility that if they were one-on-one interviews, we would have richer data to validate, and we did not use triangulation. This could be incorporated into future studies.
This clearly emphasizes the need for targeted curriculum modules aimed at equipping medical students and resident doctors with skills to navigate challenging conversations, particularly those involving delivering distressing news and handling their grief, resulting in maladaptive coping. Trainee doctors perceived a significant lack of support from peers and senior colleagues. 20 At the same time, they expected a debrief and emotional support after the death of a patient, and it is known that recognizing distress and emotional processing contributes to better self-regulation 9 and improves patient care.11,12 This research not only enhances our understanding of emotional intricacies usually bypassed in medical training but also advocates the need to have protocols and proactive measures to support interns and resident doctors. This will enable us to develop a future generation of resilient, empathetic, and communicative medical personnel.
Footnotes
Acknowledgements
The authors acknowledge all the participants for their time and contribution.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
Nil.
Ethical Approval
Ethical approval was obtained by the Institutional Ethics Committee, Ramaiah Medical College (Approval number – MSRMC/EC/AP-04/12-2022).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from participants of this study.
Annexure I:
Questionnaire/Focused Group Discussion:
Describe death experience at work Describe the emotions, thoughts and other significant events attached to the experience, Could you describe your relationship with the patient? How did you cope? How prepared were you to handle such a situation? What in your judgment would have made this difficult situation easier to deal with? What were the difficulties you faced alongside experiencing death as a trainee doctor? Any other experiences you would like to share?