
Abstract
Purpose of the Review:
Psychotherapy remains a fundamental component of mental health treatment, yet it encounters significant barriers to accessibility and efficacy. The integration of digital therapies, encompassing e-Health, m-Health, and artificial intelligence (AI) offers the transformative potential to enhance therapeutic processes through automated systems that improve access and personalize treatment. This integration, however, involves complex considerations, including health-related quality of life (HRQoL) and the dynamics of the therapeutic alliance. This narrative review synthesizes current literature on the application of digital therapies in psychotherapy, with a focus on attention-deficit/hyperactivity disorder (ADHD), obsessive-compulsive disorder (OCD), schizophrenia, and substance use disorders (SUDs). The review evaluates the effectiveness of these interventions, their impact on HRQoL, therapeutic relationships, and the associated ethical considerations.
Collection and Analysis of Data:
Following Green’s checklist for narrative reviews, a systematic literature review was conducted on studies published from January 2009 to May 2024. Inclusion criteria centered on digital therapies, including AI-based, Internet-based, and mobile-based interventions in psychotherapy. A total of 23 studies were analyzed.
Conclusions:
The findings indicate that digital therapies hold substantial promise for enhancing therapeutic interventions across various mental health disorders, particularly through chatbots and Internet-based psychotherapy. However, successful integration requires careful attention to the therapeutic alliance, HRQoL, and ethical implications. This review highlights the significant potential of digital therapies, including AI-driven psychotherapy, in managing diverse mental health disorders. A balanced approach to integration, prioritizing patient well-being and addressing ethical complexities, is essential for optimizing treatment outcomes.
Digital health integrates emerging technologies to transform mental healthcare through e-Mental health platforms, m-Health applications, and artificial intelligence (AI)-based tools, improving self-management, patient care, and treatment. e-Health leverages digital technologies like online health information, telemedicine, and electronic health records to enhance healthcare delivery. m-Health, a subset of e-Health, focuses on mobile interventions via smartphones and wearable devices for health services and self-management.1,2 In contrast, AI-based interventions employ machine learning and natural language processing for personalized therapy, automated assessments, and improved decision-making through chatbots and virtual therapists. AI also offers innovative diagnostic tools and enhances psychotherapy for disorders like anxiety and depression, akin to e-Health and m-Health interventions, by providing personalized support. Despite their potential, these technologies face challenges in effectiveness, clinical relevance, accessibility, privacy, security, personalized care, and integration with traditional healthcare, necessitating robust, large-scale studies.3,4,5 Outcome measures for digital interventions are crucial in evaluating their impact on mental health. These include user engagement, which indicates satisfaction and adherence; symptom reduction, which captures the alleviation of psychological symptoms; and effectiveness, which evaluates the overall therapeutic success, enhancement of quality of life, and sustained benefits.6,7
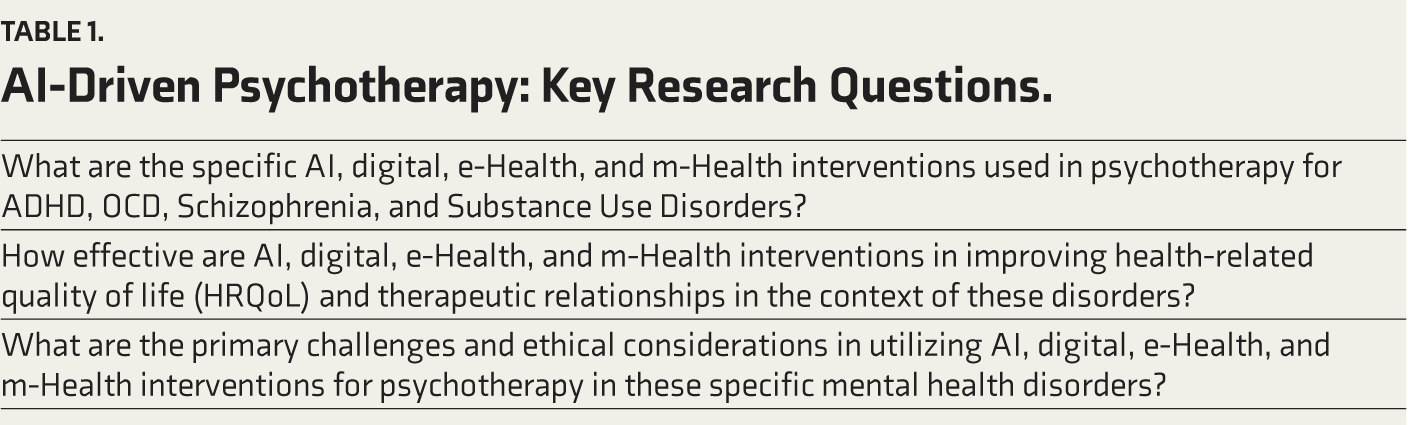
The current review extends our previous study on AI in psychotherapy for anxiety and depressive disorders. Despite promising developments, there remains a significant knowledge gap in understanding the effectiveness of digital interventions within the context of attention deficit/hyperactivity disorder (ADHD), obsessive compulsive disorder (OCD), schizophrenia, and substance use disorders (SUDs). Building on these insights, this article aims to fill the identified gap by examining digital interventions for ADHD, OCD, schizophrenia, and SUDs, with a particular focus on their impact on health-related quality of life (HRQoL) and the strength of the therapeutic alliance (TA) (Table 1).
AI-Driven Psychotherapy: Key Research Questions.
Methodology
We conducted an extensive literature review between December 2023 and May 2024, covering different forms of digital therapies (including AI-based, Internet-based, and mobile-based interventions) for treating mental health disorders. The search was performed across several online databases, including Scopus, PsycINFO, PubMed, and Google Scholar. The search strategy included terms such as “artificial intelligence,” “machine learning,” “deep learning,” “mental health,” “psychotherapy,” “digital health interventions,” and “Internet-based cognitive behavioral therapy (CBT),” combined with specific disorders like “ADHD,” “OCD,” “schizophrenia,” and “Substance Use Disorders.” Additional search terms like “chatbot,” “conversational agent,” “m-Health,” “mobile health,” “online therapy,” and “digital therapeutics” were incorporated to capture various forms of digital interventions. Boolean operators (AND, OR, NOT) were used to refine the search and link relevant concepts, ensuring comprehensive coverage of AI-based, m-Health, Internet-based cognitive behavioral therapy (iCBT), and digital therapeutic interventions in mental health. We restricted our search to English papers published between January 2009 and May 2024. The search entailed employing diverse terms in numerous permutations and combinations, with the aim of capturing studies relevant to both AI-based interventions and other forms of digital psychotherapy. In order to assist the selection of relevant papers for our thorough review study, we have defined the following inclusion and exclusion criteria: Inclusion: (a) Articles discussing AI-based, Internet-based, or mobile-based interventions in psychotherapy; (b) studies examining the efficacy, acceptance, or application of these digital interventions in treating mental health disorders; (c) focus on ADHD/OCD/Schizophrenia/SUDs; (d) use of randomized trials or observational studies or review studies. Exclusion: (a) Articles discussing digital interventions outside psychotherapy; (b) nonempirical discussions on digital interventions in psychotherapy; (c) general mental health topics; (d) nonempirical designs like opinions or editorials; and (e) focus on depressive/anxiety disorders. The study adhered to Green’s checklist for narrative reviews. 8 The first author independently searched the literature using set terms and criteria, consulting a second author for discrepancies. Publications were selected based on titles and abstracts, and full texts were further assessed. Additional articles were found through references. Data extraction focused on capturing key outcome measures–user engagement, symptom reduction, and overall effectiveness. The study synthesized themes, patterns, trends, gaps, and issues regarding digital therapies, with particular attention to the evolving role of AI in psychotherapy, providing a foundation for future research (Multimedia Appendix).
AI Applications for Enhancing Health Outcomes and Quality of Life
HRQoL reflects an individual’s physical and mental well-being in the context of their health conditions. It captures the impact of illness on daily life and serves as a valuable tool for understanding how a disease affects a person’s life.9,10 Chronic illnesses significantly reduce HRQoL, highlighting the need for effective management strategies. Digital technologies offer promising interventions to address this challenge. Mobile health tools like chatbots (e.g., Wysa) can help individuals manage mild mental health concerns and enhance their HRQoL. 11 This link between mental health and HRQoL is well-established across both adult and pediatric populations. 12 Mental health disorders significantly impact HRQoL by disrupting daily functioning, social interactions, and goal achievement. They can also exacerbate physical health problems, creating a downward spiral. For example, ADHD, OCD, SUD, and schizophrenia all contribute to diminished HRQoL across various domains.13,14,15,16 Artificial intelligence (AI) has the potential to improve HRQoL further. AI advancements are revolutionizing mental healthcare through enhanced diagnosis, treatment selection, and patient monitoring. Machine learning offers valuable insights into human behavior patterns and disease progression. However, quantifying the impact of these technologies on HRQoL remains challenging. This necessitates integrating human-centric outcomes in studies evaluating digital interventions. 17
Digital Therapeutic Alliance in AI-Based Psychotherapy
The TA, the bond between a mental health professional and a patient, is integral to the success of psychological treatments. 18 It enhances the engagement and effectiveness of therapy. Research indicates a consistent, moderate correlation between TA and treatment outcomes across various mental health issues and therapeutic approaches for all age groups. 19
Digital therapeutic alliance (DTA) refers to a broad range of digital mental health treatments and interventions, including computer-facilitated teletherapy, web and mobile applications, and AI-powered therapeutic methods. 20 Human-computer interaction (HCI) theories suggest the potential for DTA, highlighting how applications can promote empathy, 21 task completion and goal achievement, 22 therapy accessibility, 23 user-app attachment, 24 and self-determination. 25 However, some digital interventions may yield benefits without a DTA, potentially through promoting self-management and help-seeking behaviors. 13
Review by Henson et al. 26 Highlights the understudied role of DTA in evaluating mobile mental health tools. App design and functionality are crucial for building DTA, suggesting the need to consider user goals when designing interventions. While smartphones can improve engagement, the impact of clinician interaction on DTA remains unclear. Notably, limited research exists on DTA for solely smartphone-delivered interventions, and simply translating therapy manuals to mobile formats has not yielded optimal results. Investigating DTA could be key to enhancing the effectiveness of digital mental health interventions.
AI and Digital Interventions for Enhancing ADHD Outcomes
Jang et al. 27 A pilot study was conducted on 46 adults with attention deficit symptoms to test the efficacy of Todaki, a chatbot for CBT and psychoeducation. The chatbot group showed significant symptom reduction, correlating with the frequency of psychoeducation program use. Detailed results and statistical tests, including p values, were reported but lacked power calculation and confidence intervals. Participants valued the chatbot’s empathy but found its conversation flow unnatural. The study concluded the chatbot’s potential for symptom improvement and recommended large-scale trials for further verification.
A comprehensive analysis by Shou et al. 28 Six randomized controlled trials involving 261 ADHD patients, including both children and adults, utilized data from PubMed, EMBASE, and Cochrane libraries. The study employed the Cochrane bias risk tool and standardized mean difference (SMD) as effect indicators. Results indicated that online interventions significantly improved attention deficit and social function compared to a waiting list control group, with combined SMDs of −0.73 and −0.59, respectively. Despite the small sample size and potential heterogeneity, the study highlighted the need for further research to assess the efficacy and cost-effectiveness of online ADHD treatments.
In another study, Selaskowski et al. 29 Compared chatbot-based psychoeducation (CBP) and app-based psychoeducation (ABP) with 34 adults with ADHD. Both CBP and ABP were found to be equally effective in reducing symptoms. The study faced limitations such as short duration, technical issues, and lack of control groups. However, randomization was applied, equal care was provided, and no significant dropout or harms were reported. Detailed reporting of intervention effects, power calculations, and outcomes was provided.
Terabot, an interface designed to facilitate online discussions among adults with ADHD, was introduced through a study utilizing Wizard of Oz trials, design workshops, prototyping, and iterative testing. Nordberg indicated Terabot’s potential to guide group discussions and aid mental health interventions. 30 The study called for further development and high-fidelity testing for validation, acknowledging prototype limitations such as low fidelity and potential real-world errors. It advocated more research on chatbot design, particularly in prototyping scripts and mental health support experiences.
An AI system designed to help students with ADHD identify behavioral patterns was developed at Malmö University. Utilizing a Double Diamond design framework and co-design methods, Ravishankar aimed to foster understanding and personal reflection about the disorder. 31 The prototype showed promise, but the study’s scope was limited. Due to time constraints, the “Design after Design” phase was not fully explored, indicating potential for future work.
Effectiveness of Internet-based CBT for OCD
A 12-week single-blind randomized controlled trial by Lenhard assessed the feasibility and efficacy of iCBT for adolescents with OCD, involving 67 participants aged 12–17. 32 The study found that iCBT significantly reduced OCD symptoms and demonstrated cost savings of–$144.98 per patient. Despite potential sample bias, possible recall bias, measurement error in cost data, and short duration, the study concluded that iCBT is a viable treatment for adolescent OCD and advocated for further research to assess long-term cost-effectiveness.
In a comparison of iCBT and Internet-based progressive relaxation training (iPRT) for OCD, Kyrios et al. 33 Conducted a randomized controlled trial with 179 Australian residents aged 18 or older. The study found no significant differences in demographic or mental health between the two groups. Despite 54% of treatment completers no longer meeting OCD diagnostic criteria, the iCBT group showed significant improvement in OCD severity. However, limitations included challenges in engaging participants for post-treatment assessments and deviations from the original protocol.
Andersson et al. 34 Studied the effectiveness of iCBT for obsessive-compulsive disorder (OCD) in a 15-week program involving 23 participants. The program included psychoeducation, cognitive restructuring, and exposure to response prevention. Results showed significant improvement in primary and secondary outcomes, including OCD symptoms, depression, general functioning, anxiety, and quality of life. However, the study’s limitations, including a small sample size and self-reported measures, warrant cautious interpretation.
A randomized controlled trial by Andersson et al. 35 In 2012, a 10-week iCBT program with online supportive therapy for OCD in a Swedish adult population. Both groups showed significant improvements on the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS), with larger improvements in the iCBT group (Cohen’s d of 1.12 at post-treatment). Despite lacking a placebo control group and potential generalizability issues due to its Swedish context, the study suggests iCBT’s effectiveness for OCD.
In a 2014 study by Andersson et al. 36 Examined the long-term efficacy of iCBT for OCD, involving 101 participants, with 93 randomized to receive either a booster program or not. The study showed sustained long-term effects from pre-treatment to all follow-up assessments and significant symptom reduction in the booster group at seven months. Despite limitations such as a lack of simultaneous procedures and potential biases due to participant withdrawals, the study concluded that iCBT and an Internet-based booster program can enhance outcomes and prevent relapse in some OCD patients.
m-Health and AI Interventions for Schizophrenia
Gire et al. (2017) reviewed m-Health interventions for psychosis, focusing on their feasibility and effectiveness. The study included seven randomized controlled trials with 1,105 participants in Europe, the USA, and China. The interventions used mobile devices for medication adherence, cognitive training, and symptom monitoring. Results showed significant improvements in medication adherence and cognitive functioning. However, the study was limited by the small number of included studies and relatively small sample sizes, highlighting the need for larger, well-designed trials to evaluate further the potential benefits of m-Health technologies for psychosis treatment. 2
Over a 12-week randomized controlled trial, Schlosser et al. 37 Evaluated the efficacy of the PRIME mobile app in enhancing motivation among young individuals with recent-onset schizophrenia spectrum disorders (SSDs). With 43 participants aged 16–36, divided into PRIME and treatment-as-usual/waitlist (TAU/WL) control groups, the study revealed significant improvements in depression, defeatist beliefs, self-efficacy, and social motivation within the PRIME group, which persisted post-trial. However, limitations included a small sample size, a short follow-up period, and the lack of comparisons with other interventions due to the TAU/WL control condition.
Evaluating the TechCare App for individuals with psychosis in the North West of England, Gire et al. 38 Found it to be both acceptable and feasible. This study involved 16 participants aged 18–65 from early intervention services (EIS) who utilized the app for real-time, personalized, guided self-help interventions based on CBT. Results indicated that 83.33% completed the six-week study, with 70% achieving compliance thresholds. Although participants found the app acceptable and feasible, the small sample size and location in one EIS may limit the generalizability of the results.
A systematic review by Yang et al. 39 The review covered 70 studies on AI in schizophrenia rehabilitation, revealing that AI enhances rehabilitation through real-time data analysis despite challenges like algorithmic transparency and data security. It highlighted the need for high-quality data, user-centered design, and more qualitative studies for a comprehensive evaluation of AI’s impact. The authors adhered to PRISMA guidelines for study quality assessment, focusing on AI applications, technologies, and data types in rehabilitation management. However, they did not provide numerical results or confidence intervals.
Nwoye et al. 40 Developed an AI-based chatbot, SchizoBot, to provide CBT to schizophrenia patients. By training an artificial neural network (ANN) on a dataset that includes CBT details and frequently asked questions (FAQs) of schizophrenia patients, the model achieved a 93.97% accuracy score. SchizoBot is envisioned as a cost-effective and accessible tool to improve patient health and assist clinicians. However, the study’s limitations include the need for real-time validation and user satisfaction assessment, suggesting further research with larger datasets and clinical consultations.
Digital and Chatbot-Assisted Interventions for Substance Use Disorders
In 2021, Prochaska et al. 41 assessed the effectiveness of Woebot-substance use disorders (W-SUDs) in reducing substance misuse during the coronavirus disease 2019 (COVID-19) pandemic. The study involved 180 US adults screened for substance misuse, and results indicated significant reductions in substance use occasions and improved mental health outcomes. Despite a small sample size, self-reported data, and high attrition, the study suggests that W-SUDs can help alleviate the population-level burden of SUDs
Elmasri and Maeder investigated chatbots for assessing alcohol habits in mental health interventions for young adults aged 18–25 in Australia. 42 A chatbot was developed to assess drinking habits and health risk levels and was positively received in a cohort study of 17 participants. The study suggested enhanced user satisfaction with chatbots of varying behavior and sophistication. Limitations included a small sample size and the absence of a control group.
In 2021, Prochaska et al. 43 Evaluated the efficacy of W-SUD in treating probable SUDs in a predominantly non-Hispanic white female cohort aged 18–65. The eight-week intervention used the W-SUDs app to deliver CBT. Post-intervention, 76% of participants positively rated W-SUDs, with 43% feeling their needs were met. The single-arm design and short duration limit causal inference and long-term effects, suggesting a need for further randomized controlled trials to confirm W-SUDs’ clinical utility and effectiveness.
Robo, a chatbot designed to provide instant answers to opioid-addicted patients on social media, was introduced by Moghadasi et al. 44 That utilized deep learning techniques to retrieve answers from a Reddit-sourced dataset of questions and answers, employing single-turn response matching and query semantic understanding (QSU) components. The study featured three real use cases where Robo effectively responded to patient inquiries. However, limitations included reliance on a single data source and the chatbot’s inability to provide medical advice.
The effectiveness and usability of connected health interventions for SUD in adults were evaluated in a systematic review by Carreiro et al. 45 In 2020, 32 studies were analyzed, with a focus on interventions using mobile phones or wearable devices to collect data and trigger real-time responses. The most common SUD studied was alcohol use disorder, with interventions often involving craving management and tailored feedback. Results showed positive effects on SUD outcomes and high acceptability, but limitations included small sample sizes, potential publication bias, and a focus on younger populations.
In a 2023 randomized controlled trial, Chun-Hung et al. 46 Investigated chatbot-assisted therapy (CAT) for methamphetamine use disorder. The study reported minor improvements in treatment retention and fewer MA-positive urine samples in the experimental group but no significant clinical difference. Despite CAT’s potential benefits, the study emphasized the need for more research. Limitations included masked therapeutic effects, a predominantly male and employed sample, selection bias, exclusion of individuals with acute mental illness, and resource-constrained assessment. The study concluded that CAT’s benefits outweighed its harms but lacked a cost-effectiveness analysis.
Echo-APP, a virtual digital psychotherapist app for patients with methamphetamine use disorder, was developed and evaluated by Chen et al. 47 In a 2023 study. The app aimed to improve treatment motivation and reduce psychological cravings through a tablet-based interface. The study involved 47 patients from the Shanghai Drug Rehabilitation Center. Results showed significant improvements in treatment motivation and reduced cravings. However, limitations include reliance on scale-based assessments, lack of a control group, and the focus on a specific substance use disorder.
A systematic review by Ogilvie et al. 48 examined six studies on chatbots as supportive agents for SUD patients, indicating potential for substance use reduction. Despite promising results, the need for more research was highlighted due to limitations like small sample sizes, reliance on user scenarios, a lack of longitudinal studies, and the necessity for expert input for ethical data use. The review’s generalizability is limited, and the balance of benefits against harms and costs was not addressed.
Discussion
This narrative review underscores the promising role of AI and digital therapies in reducing symptoms and improving patient outcomes, introducing innovative strategies for psychological disorder management. Through a comprehensive review of 23 studies, the impact of digital interventions on psychotherapy for ADHD, OCD, schizophrenia, and SUDs is examined, focusing on outcomes, such as user engagement, symptom reduction, and overall effectiveness.
Digital and AI-based interventions for ADHD, explored across five studies, demonstrate significant potential for symptom reduction. In one study, Jang et al. found that the AI chatbot Todaki reduced attention deficit symptoms, though issues with conversation flow affected user engagement. Another study by Shou et al. noted that online interventions improved both attention deficit and social functioning. Selaskowski et al. compared app-based psychoeducation with AI chatbots, suggesting limited added benefits of AI. Additional systems like Terabot and Malmö University’s prototype have shown promise for group discussions and promoting understanding but face early-stage limitations. AI therapies offer personalized interaction and facilitate deeper self-reflection, although natural conversation flow and user engagement remain areas for improvement. While symptom reduction has been observed, enhancing user engagement with AI systems warrants further research.
In studies on OCD, the effectiveness of digital interventions emerges prominently. Lenharde and Kyrios et al. demonstrated significant symptom reduction with iCBT despite challenges related to biases and short study durations. A series of studies by Andersson et al. reported consistent improvements with iCBT, though they emphasized the need for randomized trials and long-term studies. Although iCBT’s efficacy for OCD is well-documented, research on AI-based treatments remains limited. This gap calls for future studies on AI-driven interventions, which could provide adaptive, personalized treatments and real-time engagement monitoring. Without empirical AI-based studies, direct comparisons are lacking, leaving questions about the efficacy and scalability of AI technologies for OCD treatment unresolved.
A review of digital interventions for schizophrenia across five studies reveals advancements in feasibility and patient outcomes, though focused research on AI-specific interventions remains limited. For instance, Gire et al. reported improvements in medication adherence and cognitive functioning with m-Health interventions, albeit with small sample limitations. Another study by Schlosser et al. highlighted the PRIME app’s potential for enhancing motivation and mental health, though short follow-ups and small samples constrained broader applicability. The TechCare App demonstrated high user engagement in a study by Gire et al., though a localized sample limited results. Some AI-based interventions, such as SchizoBot and those reviewed by Yang et al., have shown promise for symptom reduction and scalability but face challenges in algorithmic transparency and validation. While AI enhances personalization and real-time feedback, m-Health apps continue to play a crucial role in medication management and cognitive support.
Digital and AI-based interventions for SUDs present the potential to support treatment and recovery across eight studies. Prochaska et al. observed that W-SUDs reduced substance use and improved mental health, though small samples and single-arm designs constrained results. Moghadasi et al. reported effectiveness with Robo, a chatbot for opioid inquiries, though clinical validation and dataset scope were limited. Studies by Elmasri & Maeder and Chun-Hung et al. found chatbots beneficial for alcohol and methamphetamine use but noted biases and small sample sizes. Carreiro et al. reviewed mobile and wearable interventions, which yielded positive outcomes. Chen et al. introduced Echo-APP, a virtual psychotherapist that reduced methamphetamine cravings, although without a control group. AI-based therapies enhance user engagement with real-time responses and personalized feedback, though they still face validation and ethical challenges. Both AI and digital interventions prove effective for substance use reduction, though further studies are needed to evaluate long-term treatment outcomes.
The challenge of measuring AI’s impact on intangible outcomes like HRQoL and DTA necessitates more nuanced and extensive research. Future studies should prioritize human-centric outcomes and focus on application design to enhance therapeutic relationships and user engagement. Understanding clinician interaction and the potential for improved outcomes through DTA is crucial. The effectiveness of digital tools depends on their design and functionality. The limited literature on DTA, especially for smartphone-based self-guided treatments, highlights the need for comprehensive research to maximize AI’s potential in mental health interventions.
Our review offers valuable insight into the effectiveness of digital and AI-based interventions in reducing symptoms in psychotherapy. However, it is crucial to acknowledge its limitations. Our search parameters, restricted to English-language publications and specific databases, may have excluded relevant studies in other languages or time periods. Additionally, while we focused on digital interventions, including AI-based, e-Health, and m-Health therapies, diverse research methodologies prevented us from comprehensively assessing the overall quality of the studies.
Several avenues for future research warrant exploration. Despite progress in digital health, the absence of AI interventions in long-term addiction recovery and severe mental health disorders (such as OCD) highlights a significant research gap. Understanding transference and countertransference dynamics in AI-based psychotherapy is crucial. Studies point to users forming relationships with AI bots mimicking human interactions. 49 Investigating the impact of anthropomorphism, consistent responses, personalization, long-term interactions, emotional needs projection, and attachment dynamics on therapeutic outcomes can provide valuable insights. For instance, how do users anthropomorphize AI, and what emotional patterns emerge during therapy? Additionally, studying how AI’s consistent responses affect transference patterns can reveal user expectations and their impact on therapy. Long-term studies are essential to evaluate how continuous interactions and AI memory build rapport and trust, understand user emotional projections, and guide the development of effective, ethical AI mental health systems.
Conclusion
The review of 23 research studies, including ADHD, OCD, schizophrenia, and SUDs, highlights the promising role of AI and digital therapies for symptom reduction and improved patient outcomes. Nevertheless, it also emphasizes the need for extensive and varied studies, ongoing verification and improvement of technologies, and tackling obstacles such as data accuracy, algorithm clarity, and user-focused design. The review also emphasizes the need for more sophisticated and comprehensive research to assess the influence of AI on intangible outcomes such as HRQoL and the digital therapeutic relationship. In addition, studying how users interact with AI programs, including the dynamics of transference and countertransference, will enhance future research. The study emphasizes the need for ongoing research to address methodological limitations, ensure efficacy, enhance feasibility, and fully exploit the potential of AI in mental health treatment.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflicts of interest regarding the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None Used.
Ethical Approval
Ethical permission was not applicable for this article, as this is a review article drafted from various research articles and not from patients directly.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Multimedia Appendix.
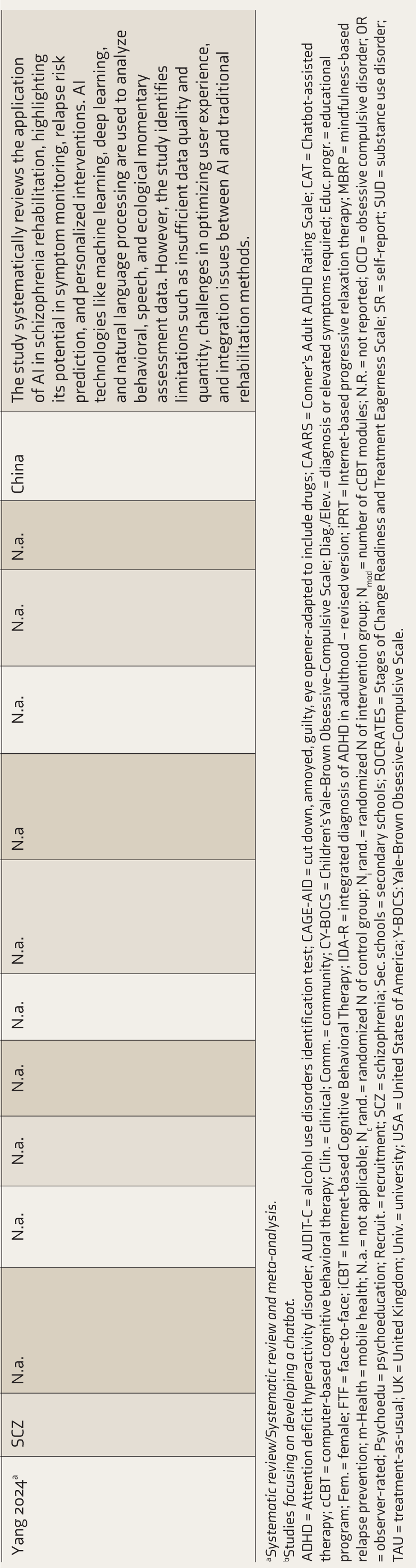
Selected characteristics of the included studies examining the effects of cCBT for ADHD, OCD, Schizophrenia and substance use disorders in adolescents and young adults.
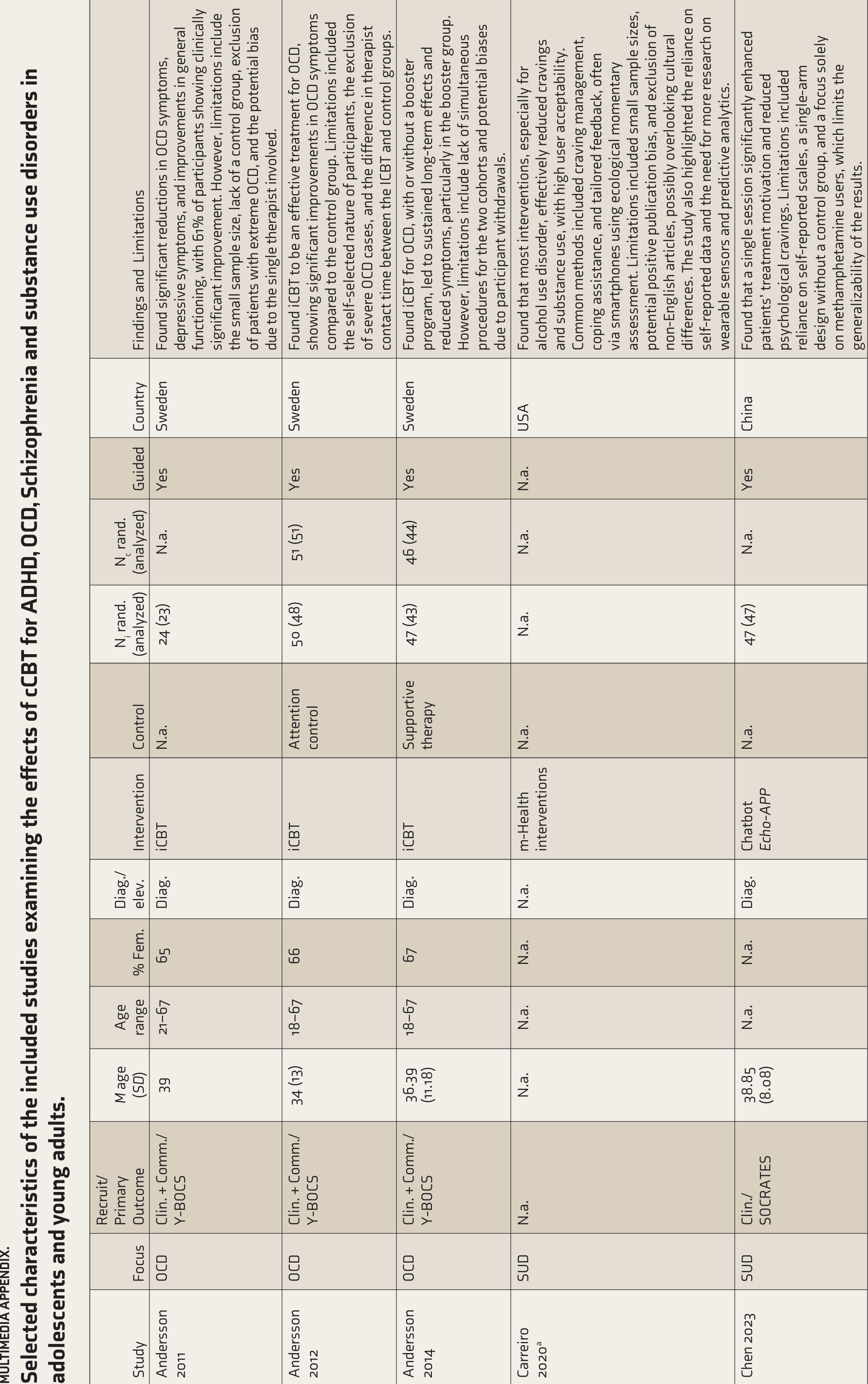
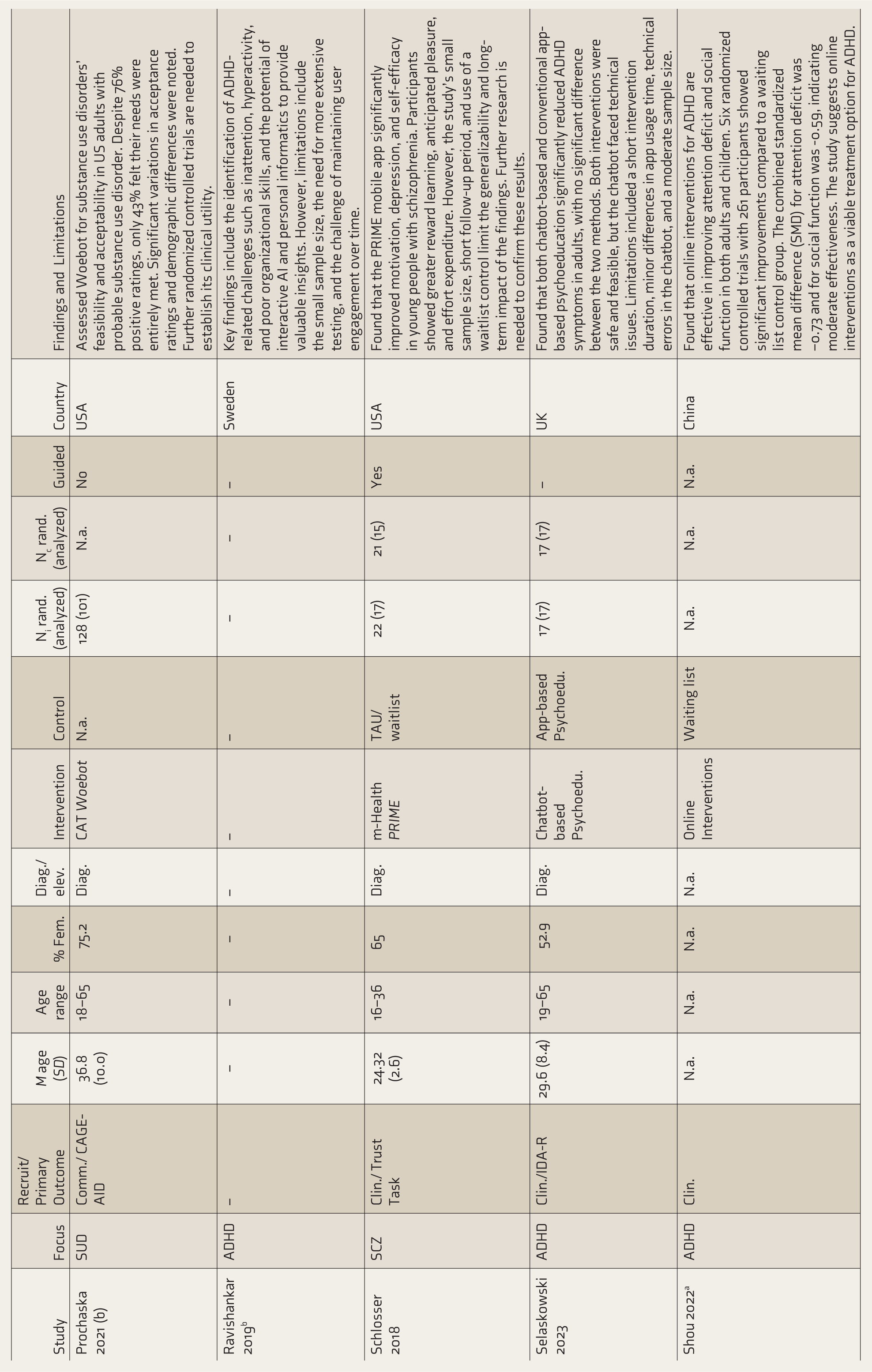
| Study | Focus | Recruit/ Primary Outcome | M age (SD) | Age range | % Fem. | Diag./elev. | Intervention | Control | Ni rand.(analyzed) | Nc rand. (analyzed) | Guided | Country | Findings and Limitations |
| Andersson 2011 | OCD | Clin. + Comm./ Y-BOCS | 39 | 21–67 | 65 | Diag. | iCBT | N.a. | 24 (23) | N.a. | Yes | Sweden | Found significant reductions in OCD symptoms, depressive symptoms, and improvements in general functioning, with 61% of participants showing clinically significant improvement. However, limitations include the small sample size, lack of a control group, exclusion of patients with extreme OCD, and the potential bias due to the single therapist involved. |
| Andersson 2012 | OCD | Clin. + Comm./ Y-BOCS | 34 (13) | 18–67 | 66 | Diag. | iCBT | Attention control | 50 (48) | 51 (51) | Yes | Sweden | Found iCBT to be an effective treatment for OCD, showing significant improvements in OCD symptoms compared to the control group. Limitations included the self-selected nature of participants, the exclusion of severe OCD cases, and the difference in therapist contact time between the ICBT and control groups. |
| Andersson 2014 | OCD | Clin. + Comm./ Y-BOCS | 36.39 (11.18) | 18–67 | 67 | Diag. | iCBT | Supportive therapy | 47 (43) | 46 (44) | Yes | Sweden | Found iCBT for OCD, with or without a booster program, led to sustained long-term effects and reduced symptoms, particularly in the booster group. However, limitations include lack of simultaneous procedures for the two cohorts and potential biases due to participant withdrawals. |
| Carreiro 2020a | SUD | N.a. | N.a. | N.a. | N.a. | N.a. | m-Health interventions | N.a. | N.a. | N.a. | N.a. | USA | Found that most interventions, especially for alcohol use disorder, effectively reduced cravings and substance use, with high user acceptability. Common methods included craving management, coping assistance, and tailored feedback, often via smartphones using ecological momentary assessment. Limitations included small sample sizes, potential positive publication bias, and exclusion of non-English articles, possibly overlooking cultural differences. The study also highlighted the reliance on self-reported data and the need for more research on wearable sensors and predictive analytics. |
| Chen 2023 | SUD | Clin./SOCRATES | 38.85 (8.08) | N.a. | N.a. | Diag. | Chatbot Echo-APP | N.a. | 47 (47) | N.a. | Yes | China | Found that a single session significantly enhanced patients’ treatment motivation and reduced psychological cravings. Limitations included reliance on self-reported scales, a single-arm design without a control group, and a focus solely on methamphetamine users, which limits the generalizability of the results. |
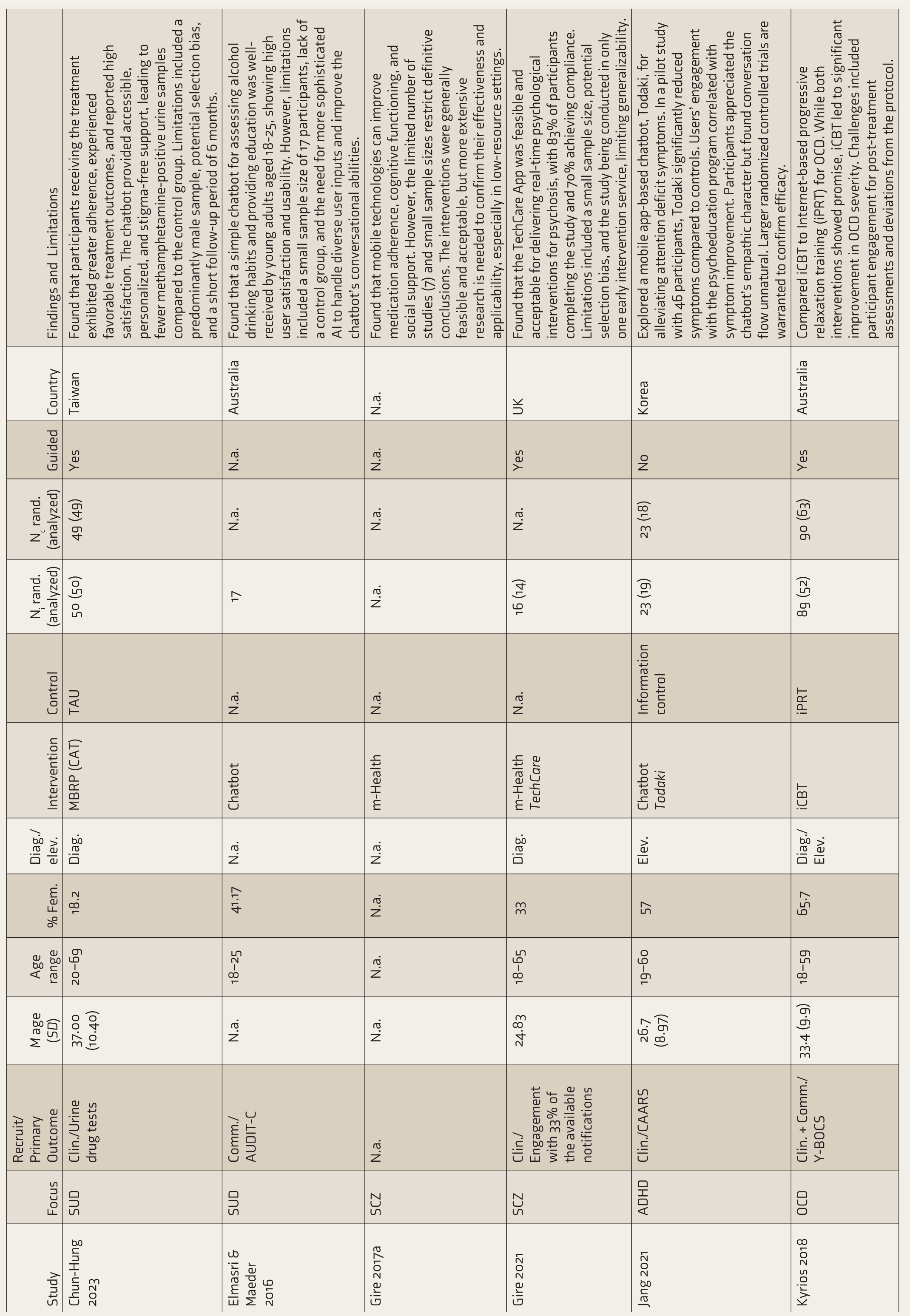
| Chun-Hung 2023 | SUD | Clin./Urine drug tests | 37.00 (10.40) | 20–69 | 18.2 | Diag. | MBRP (CAT) | TAU | 50 (50) | 49 (49) | Yes | Taiwan | Found that participants receiving the treatment exhibited greater adherence, experienced favorable treatment outcomes, and reported high satisfaction. The chatbot provided accessible, personalized, and stigma-free support, leading to fewer methamphetamine-positive urine samples compared to the control group. Limitations included a predominantly male sample, potential selection bias, and a short follow-up period of 6 months. |
| Elmasri & Maeder 2016 | SUD | Comm./AUDIT-C | N.a. | 18–25 | 41.17 | N.a. | Chatbot | N.a. | 17 | N.a. | N.a. | Australia | Found that a simple chatbot for assessing alcohol drinking habits and providing education was well-received by young adults aged 18-25, showing high user satisfaction and usability. However, limitations included a small sample size of 17 participants, lack of a control group, and the need for more sophisticated AI to handle diverse user inputs and improve the chatbot’s conversational abilities. |
| Gire 2017a | SCZ | N.a. | N.a. | N.a. | N.a. | N.a. | m-Health | N.a. | N.a. | N.a. | N.a. | N.a. | Found that mobile technologies can improve medication adherence, cognitive functioning, and social support. However, the limited number of studies (7) and small sample sizes restrict definitive conclusions. The interventions were generally feasible and acceptable, but more extensive research is needed to confirm their effectiveness and applicability, especially in low-resource settings. |
| Gire 2021 | SCZ | Clin./ Engagement with 33% of the available notifications | 24.83 | 18–65 | 33 | Diag. | m-Health TechCare | N.a. | 16 (14) | N.a. | Yes | UK | Found that the TechCare App was feasible and acceptable for delivering real-time psychological interventions for psychosis, with 83% of participants completing the study and 70% achieving compliance. Limitations included a small sample size, potential selection bias, and the study being conducted in only one early intervention service, limiting generalizability. |
| Jang 2021 | ADHD | Clin./CAARS | 26.7 (8.97) | 19–60 | 57 | Elev. | Chatbot Todaki | Information control | 23 (19) | 23 (18) | No | Korea | Explored a mobile app-based chatbot, Todaki, for alleviating attention deficit symptoms. In a pilot study with 46 participants, Todaki significantly reduced symptoms compared to controls. Users’ engagement with the psychoeducation program correlated with symptom improvement. Participants appreciated the chatbot’s empathic character but found conversation flow unnatural. Larger randomized controlled trials are warranted to confirm efficacy. |
| Kyrios 2018 | OCD | Clin. + Comm./ Y-BOCS | 33.4 (9.9) | 18–59 | 65.7 | Diag./Elev. | iCBT | iPRT | 89 (52) | 90 (63) | Yes | Australia | Compared iCBT to Internet-based progressive relaxation training (iPRT) for OCD. While both interventions showed promise, iCBT led to significant improvement in OCD severity. Challenges included participant engagement for post-treatment assessments and deviations from the protocol. |
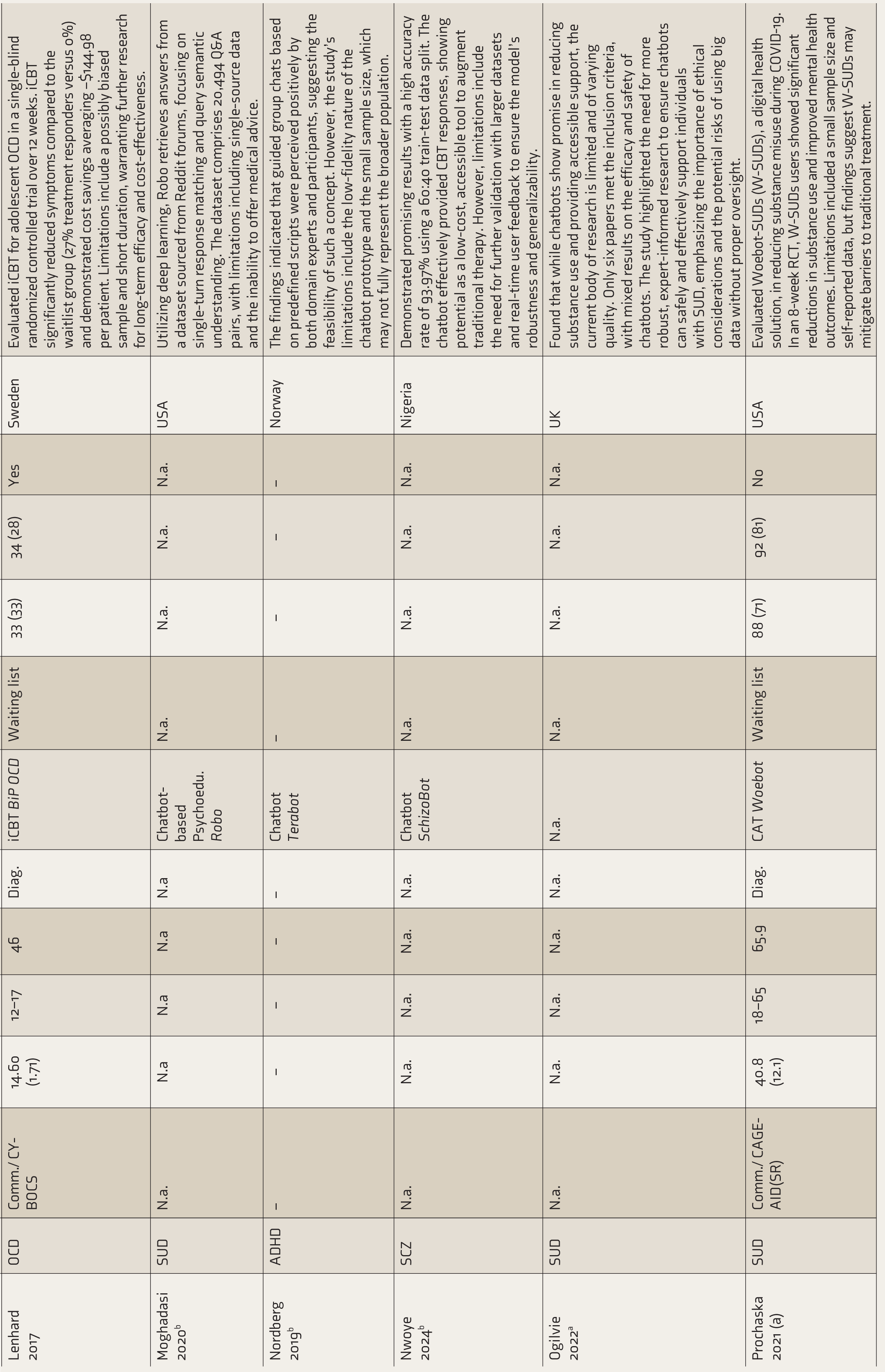
| Lenhard 2017 | OCD | Comm./ CY-BOCS | 14.60 (1.71) | 12–17 | 46 | Diag. | iCBT BiP OCD | Waiting list | 33 (33) | 34 (28) | Yes | Sweden | Evaluated iCBT for adolescent OCD in a single-blind randomized controlled trial over 12 weeks. iCBT significantly reduced symptoms compared to the waitlist group (27% treatment responders versus 0%) and demonstrated cost savings averaging −$144.98 per patient. Limitations include a possibly biased sample and short duration, warranting further research for long-term efficacy and cost-effectiveness. |
| Moghadasi 2020b | SUD | N.a. | N.a | N.a | N.a | N.a | Chatbot-based Psychoedu. Robo | N.a. | N.a. | N.a. | N.a. | USA | Utilizing deep learning, Robo retrieves answers from a dataset sourced from Reddit forums, focusing on single-turn response matching and query semantic understanding. The dataset comprises 20,494 Q&A pairs, with limitations including single-source data and the inability to offer medical advice. |
| Nordberg 2019b | ADHD | – | – | – | – | – | Chatbot Terabot | – | – | – | – | Norway | The findings indicated that guided group chats based on predefined scripts were perceived positively by both domain experts and participants, suggesting the feasibility of such a concept. However, the study’s limitations include the low-fidelity nature of the chatbot prototype and the small sample size, which may not fully represent the broader population. |
| Nwoye 2024b | SCZ | N.a. | N.a. | N.a. | N.a. | N.a. | Chatbot SchizoBot | N.a. | N.a. | N.a. | N.a. | Nigeria | Demonstrated promising results with a high accuracy rate of 93.97% using a 60:40 train-test data split. The chatbot effectively provided CBT responses, showing potential as a low-cost, accessible tool to augment traditional therapy. However, limitations include the need for further validation with larger datasets and real-time user feedback to ensure the model’s robustness and generalizability. |
| Ogilvie 2022a | SUD | N.a. | N.a. | N.a. | N.a. | N.a. | N.a. | N.a. | N.a. | N.a. | N.a. | UK | Found that while chatbots show promise in reducing substance use and providing accessible support, the current body of research is limited and of varying quality. Only six papers met the inclusion criteria, with mixed results on the efficacy and safety of chatbots. The study highlighted the need for more robust, expert-informed research to ensure chatbots can safely and effectively support individuals with SUD, emphasizing the importance of ethical considerations and the potential risks of using big data without proper oversight. |
| Prochaska 2021 (a) | SUD | Comm./ CAGE-AID(SR) | 40.8 (12.1) | 18–65 | 65.9 | Diag. | CAT Woebot | Waiting list | 88 (71) | 92 (81) | No | USA | Evaluated Woebot-SUDs (W-SUDs), a digital health solution, in reducing substance misuse during COVID-19. In an 8-week RCT, W-SUDs users showed significant reductions in substance use and improved mental health outcomes. Limitations included a small sample size and self-reported data, but findings suggest W-SUDs may mitigate barriers to traditional treatment. |
| Prochaska 2021 (b) | SUD | Comm./ CAGE-AID | 36.8 (10.0) | 18–65 | 75.2 | Diag. | CAT Woebot | N.a. | 128 (101) | N.a. | No | USA | Assessed Woebot for substance use disorders’ feasibility and acceptability in US adults with probable substance use disorder. Despite 76% positive ratings, only 43% felt their needs were entirely met. Significant variations in acceptance ratings and demographic differences were noted. Further randomized controlled trials are needed to establish its clinical utility. |
| Ravishankar 2019b | ADHD | – | – | – | – | – | – | – | – | – | – | Sweden | Key findings include the identification of ADHD-related challenges such as inattention, hyperactivity, and poor organizational skills, and the potential of interactive AI and personal informatics to provide valuable insights. However, limitations include the small sample size, the need for more extensive testing, and the challenge of maintaining user engagement over time. |
| Schlosser 2018 | SCZ | Clin./ Trust Task | 24.32 (2.6) | 16–36 | 65 | Diag. | m-Health PRIME | TAU/waitlist | 22 (17) | 21 (15) | Yes | USA | Found that the PRIME mobile app significantly improved motivation, depression, and self-efficacy in young people with schizophrenia. Participants showed greater reward learning, anticipated pleasure, and effort expenditure. However, the study’s small sample size, short follow-up period, and use of a waitlist control limit the generalizability and long-term impact of the findings. Further research is needed to confirm these results. |
| Selaskowski 2023 | ADHD | Clin./IDA-R | 29.6 (8.4) | 19–65 | 52.9 | Diag. | Chatbot-based Psychoedu. | App-based Psychoedu. | 17 (17) | 17 (17) | – | UK | Found that both chatbot-based and conventional app-based psychoeducation significantly reduced ADHD symptoms in adults, with no significant difference between the two methods. Both interventions were safe and feasible, but the chatbot faced technical issues. Limitations included a short intervention duration, minor differences in app usage time, technical errors in the chatbot, and a moderate sample size. |
| Shou 2022a | ADHD | Clin. | N.a. | N.a. | N.a. | N.a. | Online Interventions | Waiting list | N.a. | N.a. | N.a. | China | Found that online interventions for ADHD are effective in improving attention deficit and social function in both adults and children. Six randomized controlled trials with 261 participants showed significant improvements compared to a waiting list control group. The combined standardized mean difference (SMD) for attention deficit was −0.73 and for social function was -0.59, indicating moderate effectiveness. The study suggests online interventions as a viable treatment option for ADHD. |
| Yang 2024a | SCZ | N.a. | N.a. | N.a. | N.a. | N.a. | N.a. | N.a | N.a. | N.a. | N.a. | China | The study systematically reviews the application of AI in schizophrenia rehabilitation, highlighting its potential in symptom monitoring, relapse risk prediction, and personalized interventions. AI technologies like machine learning, deep learning, and natural language processing are used to analyze behavioral, speech, and ecological momentary assessment data. However, the study identifies limitations such as insufficient data quality and quantity, challenges in optimizing user experience, and integration issues between AI and traditional rehabilitation methods. |
aSystematic review/Systematic review and meta-analysis.
bStudies focusing on developing a chatbot.
ADHD = Attention deficit hyperactivity disorder; AUDIT-C = alcohol use disorders identification test; CAGE-AID = cut down, annoyed, guilty, eye opener-adapted to include drugs; CAARS = Conner’s Adult ADHD Rating Scale; CAT = Chatbot-assisted therapy; cCBT = computer-based cognitive behavioral therapy; Clin. = clinical; Comm. = community; CY-BOCS = Children’s Yale-Brown Obsessive-Compulsive Scale; Diag./Elev. = diagnosis or elevated symptoms required; Educ. progr. = educational program; Fem. = female; FTF = face-to-face; iCBT = Internet-based Cognitive Behavioral Therapy; IDA-R = integrated diagnosis of ADHD in adulthood – revised version; iPRT = Internet-based progressive relaxation therapy; MBRP = mindfulness-based relapse prevention; m-Health = mobile health; N.a. = not applicable; Nc rand. = randomized N of control group; Ni rand. = randomized N of intervention group; Nmod = number of cCBT modules; N.R. = not reported; OCD = obsessive compulsive disorder; OR = observer-rated; Psychoedu = psychoeducation; Recruit. = recruitment; SCZ = schizophrenia; Sec. schools = secondary schools; SOCRATES = Stages of Change Readiness and Treatment Eagerness Scale; SR = self-report; SUD = substance use disorder; TAU = treatment-as-usual; UK = United Kingdom; Univ. = university; USA = United States of America; Y-BOCS: Yale-Brown Obsessive-Compulsive Scale.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.