
Abstract
Background:
Neurotropin-3 (NT-3), a marker of neural plasticity, is reported to be altered in bipolar disorder (BD). This study was designed to evaluate NT-3 gene polymorphism (rs 6489630, rs 6332, and rs 11063714) in BD and its association with disease severity and cognition.
Methods:
The study included 176 BD cases and 176 controls. All the participants were tested for NT-3 polymorphism and plasma NT-3. ACE-III scores were used to analyze cognition.
Results:
The NT-3 polymorphism (rs 6489630) was associated with cognitive impairment in BD (P = .010). The attention score was found to be decreased in the CT genotype (P = .028) when compared to the CC and TT genotypes of the rs6489630 variant. The visuospatial ability score was decreased in the GG genotype (P = .044) compared to the AG genotype of the rs11063714 variant. BD patients with the maniac episode showed a decrease in levels of Neurotrophin-3 in comparison to both the control group (P = .045) and the remission group (P = .017). Plasma NT-3 was associated with the YMRS (r = −0.221, P = .003), HDRS (r = 0.209, P = .005) and visuospatial ability score (r = 0.180, P = .017) in patients with BD.
Conclusion:
Single nucleotide polymorphisms of NT-3 are associated with cognitive dysfunction in BD.
The rs 6489630 polymorphism of NT-3 was related to cognitive dysfunction in BD. The BD patients with the maniac episode showed a decrease in levels of neurotrophin-3. Plasma neurotropin-3 was related to the severity of the disease and cognitive status in BD.Key Messages:
The prevalence of bipolar disorder (BD) is increasing worldwide, and the recent National Mental Health Survey reports a prevalence of 0.5% for lifetime BD in India. 1 The BD patients often exhibit prevalent cognitive symptoms such as changes in fluency, verbal and visual memory, and executive function, which significantly contribute to disability. 2 Brissos S et al. (2008) found that cognitive deficits in executive function and verbal abstraction were linked to lower self-reported quality of life in BD. 3 Earlier studies have indicated that cognitive deficits in BD extend beyond affective episodes, persisting across all phases, including remission, and significantly impacting attention, memory, and executive functions. 4
The exact cause of BD remains uncertain. It was found to involve widespread abnormalities in neurocognitive processes, neurotrophic factors, and neurotransmission, which regulate mood and neuronal activity.5,6 Neurotrophin-3, which belongs to the neurotrophic factor family, is pivotal for fortifying synapses, promoting neuroplasticity, and facilitating regeneration, which is crucial for normal cognitive functions linked to the hippocampus.7,8 Accumulating evidence suggests that dysfunctions of NT-3 lead to impaired brain development and neuroplasticity. 9 Previous studies have demonstrated elevated NT-3 levels in BD patients and its association with duration of illness.10,11 Previous research has indicated that genetic variations within the NT-3 gene, specifically SNPs (rs6489630, rs6332, and rs11063714), are linked to attention-deficit/hyperactivity disorder, adolescent idiopathic scoliosis, and Alzheimer’s disease.12–14
Several studies from India have reported cognitive impairment in BD.15,16 However, the data related to NT-3 levels and its polymorphism in the Indian population is lacking. In previous studies from our laboratory, we documented NT-3 polymorphism and elevated neurotropin-3 levels and their association with cognitive impairment in schizophrenia.17,18 The current study was designed to investigate the polymorphism of the neurotropin-3 gene (rs6332, rs11063714, and rs6489630) in BD and its relation with disease severity and cognitive function.
Methods
This case-control genetic study was approved by the Institutional Ethics Committee (Human). The data collection started in February 2022 and ended in February 2024. We obtained written informed consent from the subjects before starting the study. The study comprises 176 participants with BD-1 (aged between 20 and 50 years), diagnosed clinically using DSM-5 criteria 19 and additionally confirmed using the Structured Clinical Interview for DSM-5, research version (SCID-5-RV) 20 and 176 controls. A qualified psychiatrist administered SCID-5 to all the patients. The BD patients were treated with mood stabilizers. Participants with medical disorders and using substances for 12 weeks prior to the study were excluded. Controls (n = 176) were recruited from the hospital staff and bystanders of other patients. Control subjects with known medical comorbidities and those who were using substances for 12 weeks prior to the study were excluded. The modified Mini-International Neuropsychiatric Interview (MINI) screen was used to screen the controls for psychiatric morbidity.21,22
Sample Size Calculation
The sample size was calculated by considering the minor allele frequency (MAF). In reference to the Asian population, the parameters with the highest sample size calculation were as follows: the power of 0.9 (90%), α of 0.05, the prevalence of BD (0.6%), and the lowest MAF of rs11063714 (0.457). The total sample size was 176 for cases and controls.
The participants were examined for symptoms of depression and mania using the Hamilton Depression Rating Scale (HDRS) 23 and Young’s Mania Rating Scale (YMRS), respectively. 24 The BD patients were classified into mania and depression based on clinical diagnosis of manic episodes and depressive episodes, respectively, and those with YMRS < 7 and HDRS < 7 were considered in remission. Cognition status was assessed using the Addenbrooke Cognitive Examination-III (ACE-III). A 25 ACE-III score of 82/83 was considered for the identification of cognitive impairment. 26
Under sterile conditions, 5 ml of venous blood was drawn from the antecubital vein into an EDTA tube. The collected plasma was stored at −40 degrees Celsius for subsequent NT-3 estimation via ELISA (Elabscience ELISA kit, USA). The DNA was extracted (QIAmp DNA Blood mini kit-Qiagen Germany), quantified with NanoDrop™ 2000, and stored at −40°C for analysis of genotypes. The NT-3 gene polymorphisms were analyzed with (Thermo Fisher gene probes, U.S.) CFX 96 RT-PCR (real-time Polymerase chain reaction) (BioRad Laboratories Inc., California). The probe sequence, location, and functions of NT-3 SNPs were shown in Supplementary Tables 1 and 2. All the SNPs examined in this study adhere to the nomenclature established by the Genome Reference Consortium human (GRCh38.p14) guidelines, which are maintained by the National Center for Biotechnology Information (NCBI). The reaction mixture contained 5 µL of master mix (Thermo Fisher genotyping master mix), 0.25 µL Taqman probe, 2.25 microlites of DNAse free water, and 2.5 µL of working standard DNA, which was constituted to a final volume of 10 µL. The amplification was done for 40 cycles using the protocol standardized in our laboratory.
Statistical Analysis
According to their distribution, continuous variables such as age, sickness duration, BMI, NT-3 levels, etc., were reported as mean and standard deviation or median (interquartile range). The Kolmogorov-Smirnoff test was employed to examine the normality of the continuous variables. The data between BD and controls were compared using the Student’s t-test and the Mann–Whitney U test. The relationship between NT-3 and cognition scores was analyzed using the correlation (Spearman) test. By comparing the observed frequencies to the predicted allele frequencies in the cases and controls, the Hardy-Weinberg Equilibrium was established. 27 Results from the genotyping analysis were reported as percentages and odds ratios with 95% confidence intervals, and the chi-square test was used to examine the data using Graph Pad InStat 3.0 28 and further confirmed by genetic model analysis. 29 Cognitive scores and NT-3 levels were compared among various genetic variants using one-way ANOVA and the Kruskal-Wallis test. Haplo-view software version 4.1 was used to analyze linkage disequilibrium (LD). 30 For all of the tests, P < .05 was considered as significant.
Results
The median age group in cases and controls was 34. Both the groups had 73 females and 103 males. The clinical characteristics and plasma neurotrophin-3 levels in BD cases and controls are shown in Table 1. Plasma NT-3 (P = .269), age, and BMI were not significantly different between both groups. When bipolar patients were divided into three groups based on clinical diagnosis of manic episode, depressive episode, and remission, we found a significant difference in neurotrophin-3 levels among the groups (P = .014). The BD patients with manic episodes showed a decrease in levels of neurotrophin-3 in comparison to both the controls (P = .045) and the remission group (P = .017).
Clinical Characteristics, Cognition Scores and Neurotrophin-3 Levels in Bipolar Disorder-1 and Controls.
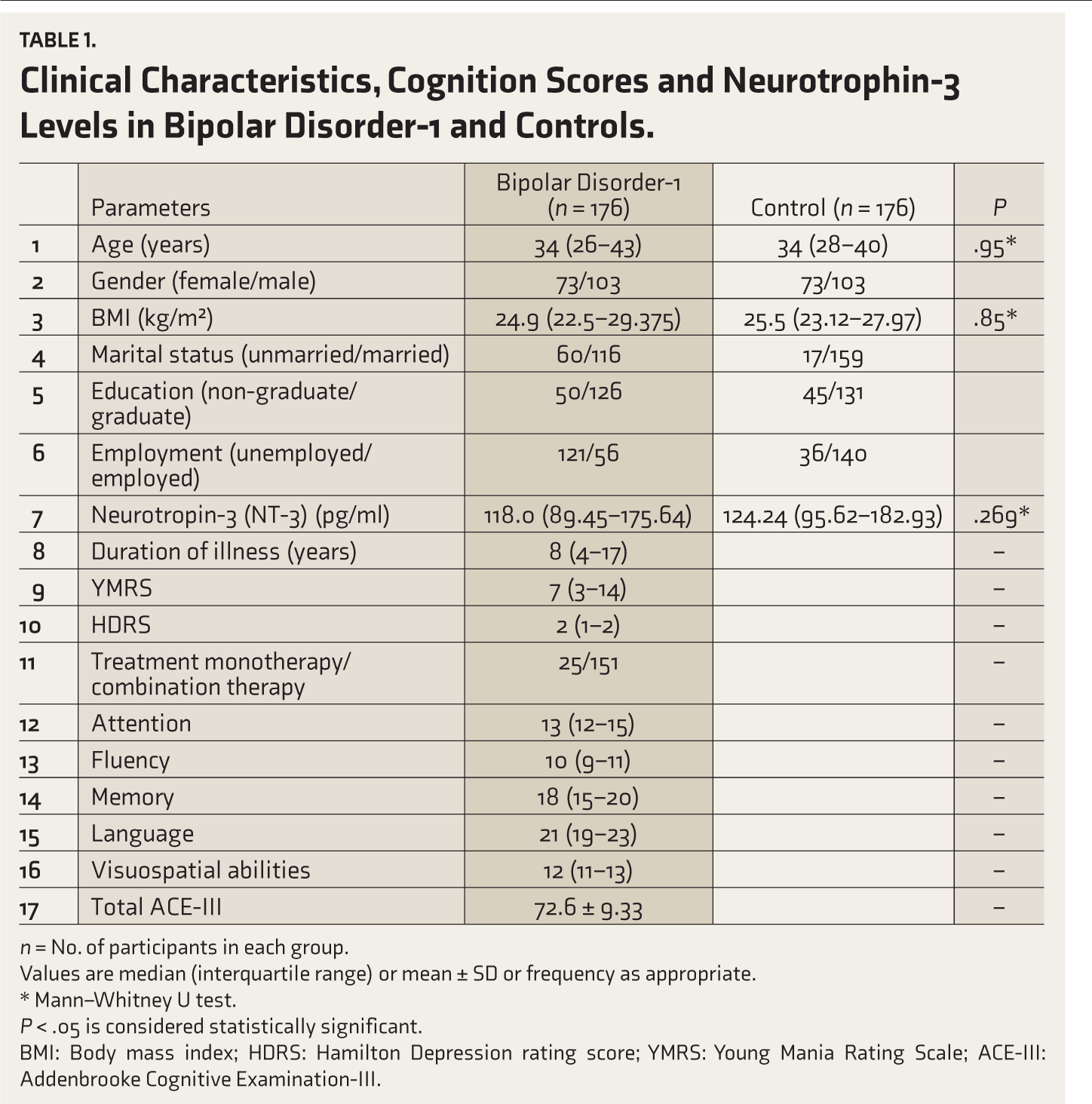
n = No. of participants in each group.
Values are median (interquartile range) or mean ± SD or frequency as appropriate.
* Mann–Whitney U test.
P < .05 is considered statistically significant.
BMI: Body mass index; HDRS: Hamilton Depression rating score; YMRS: Young Mania Rating Scale; ACE-III: Addenbrooke Cognitive Examination-III.
Neurotrophin-3 (NT-3) was associated negatively with the YMRS (r = −0.221, P = .003) and positively with the HDRS (r = 0.209, P = .005) and with visuospatial ability score (r = 0.180, P = .017) in BD.
NT-3 Polymorphism (rs6332, rs6489630, rs11063714) in BD and Controls
The allele frequency and genotype frequency of NT-3 polymorphism in BD and controls are shown in Table 2. We did not find any significant difference in genotype as well as allele frequency of rs6332, rs11063714, and rs6489630 SNPs between BD cases and controls. The results were supported by genetic model analysis.
Genotype and Allele Frequency of NT-3 Polymorphism Between BD Cases and Healthy Controls.
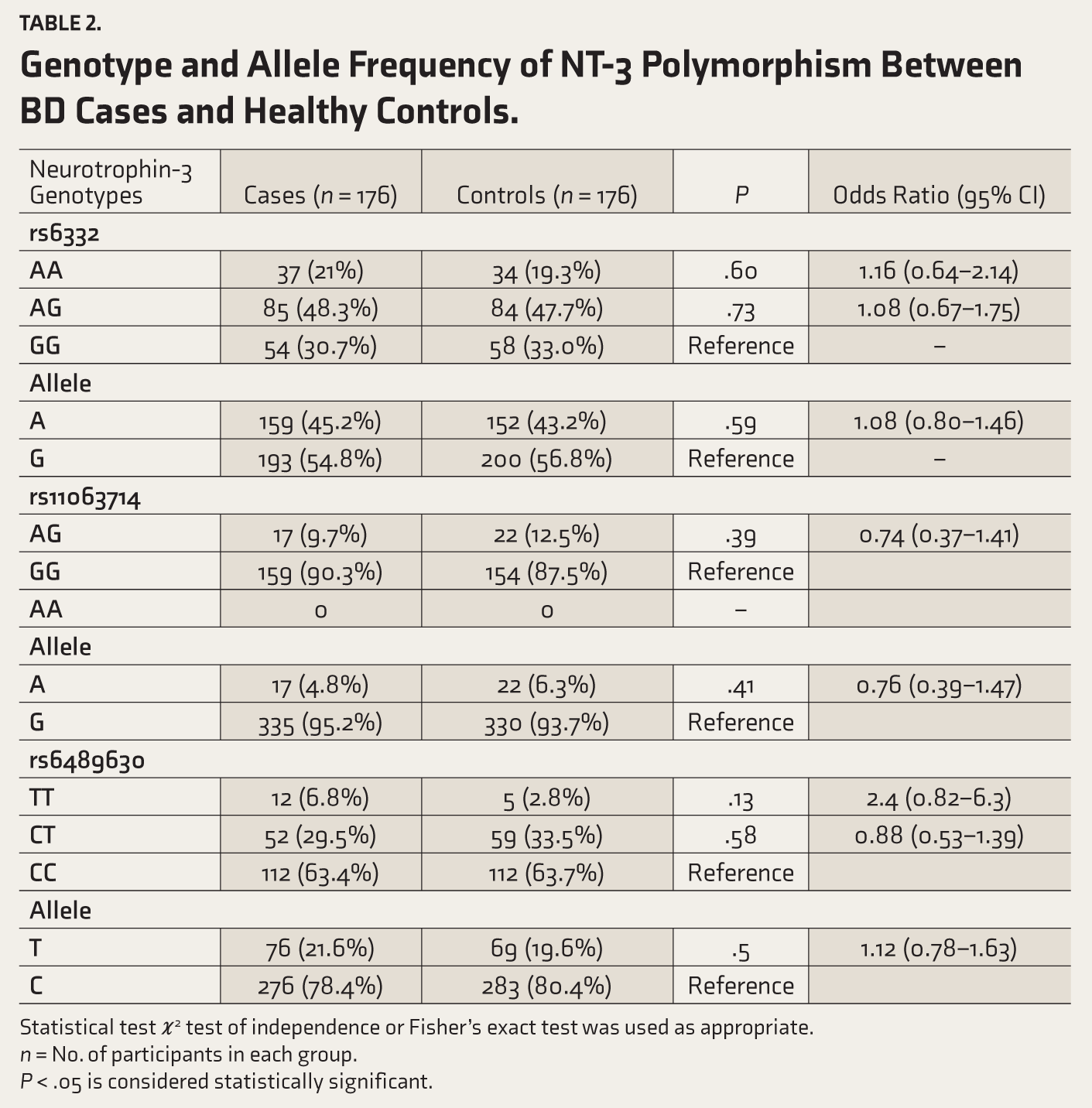
Statistical test ϰ 2 test of independence or Fisher’s exact test was used as appropriate.
n = No. of participants in each group.
P < .05 is considered statistically significant.
Relationship of NT-3 Gene Polymorphism and Cognition Status in BD
Among the NT-3 gene polymorphisms, only rs6489630 polymorphism was related to the cognition status (P = .010) (Table 3). The rs6489630 variant was related to the attention score (P = .028). Among the genotypes of rs6489630, the attention score was found to be decreased in the CT genotype in comparison with the CC genotype (P = .031). NT-3 levels and other cognition scores were not significantly different among the three genotypes of rs6489630 in BD (Table 4). The rs11063714 variant was not associated with cognitive dysfunction. However, the GG genotype of rs11063714 was associated with a significantly lower visuospatial ability score (P = .044) compared to the AG genotype in BD.
Genotype Frequency Distribution of Neurotrophin-3 Gene Polymorphism Among Different Cognitive Groups in Bipolar Disorder.
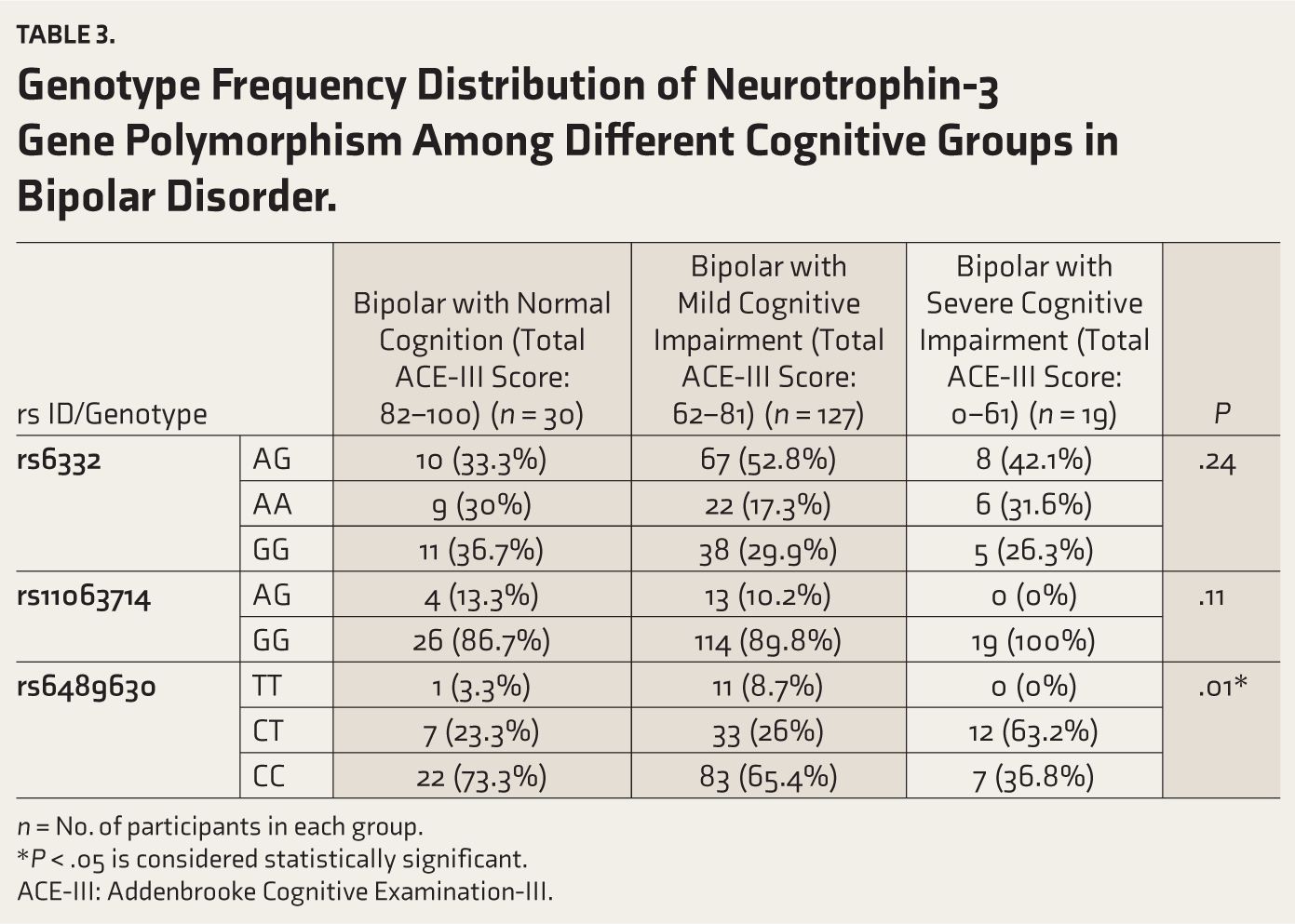
n = No. of participants in each group.
*P < .05 is considered statistically significant.
ACE-III: Addenbrooke Cognitive Examination-III.
Neurotrophin-3 Level, YMRS, HDRS, and ACE- III Scores Among rs6489630 Variant of NT-3 in Bipolar Disorder Cases.
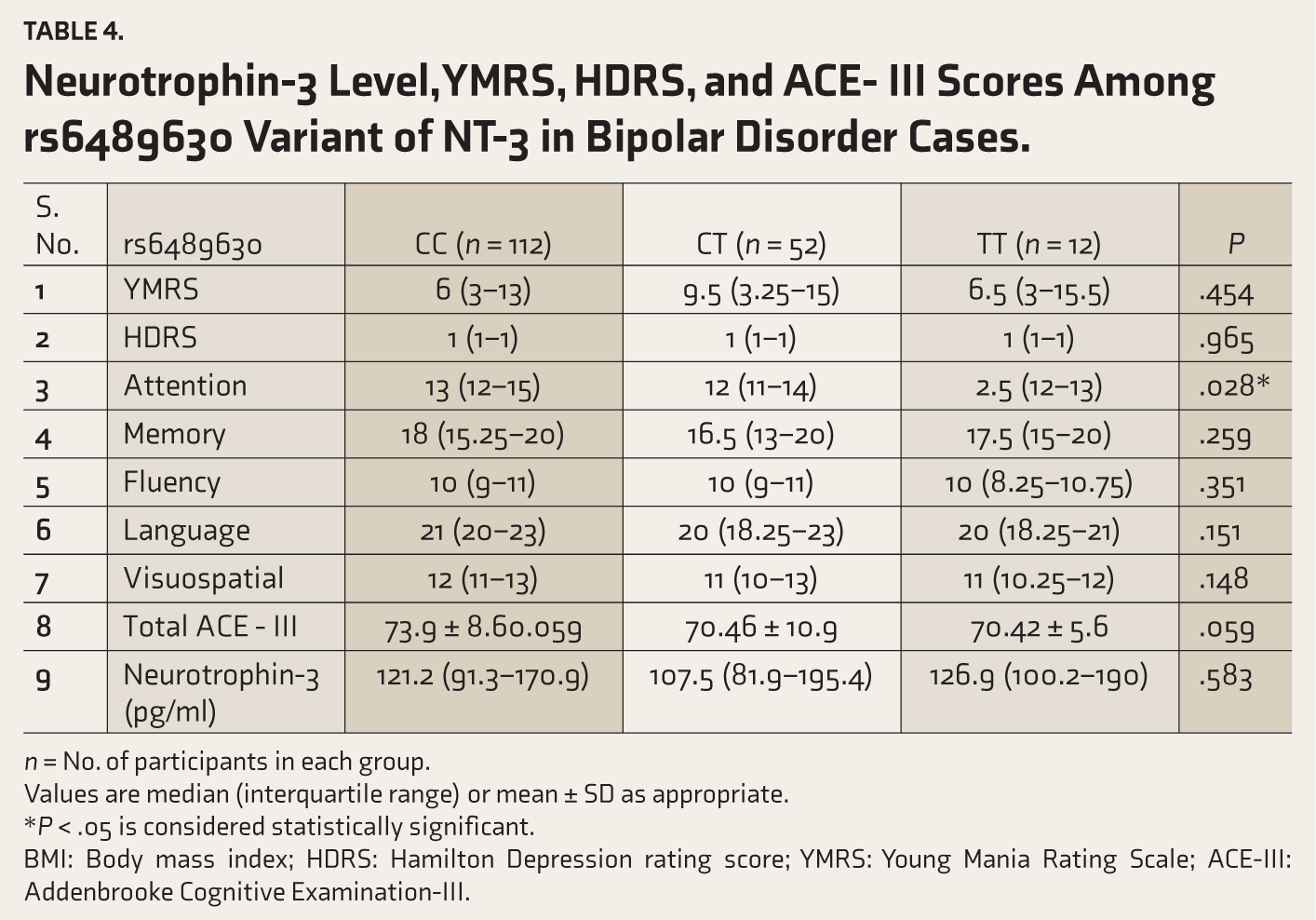
n = No. of participants in each group.
Values are median (interquartile range) or mean ± SD as appropriate.
*P < .05 is considered statistically significant.
BMI: Body mass index; HDRS: Hamilton Depression rating score; YMRS: Young Mania Rating Scale; ACE-III: Addenbrooke Cognitive Examination-III.
Among different groups of BD, the genotype frequency and allele frequency of rs6332, rs11063714, and rs6489630 SNPs between manic episode, depressive episode, and remission groups were significantly different (Data not shown).
LD Analysis of NT-3 Gene
Figure 1 shows the LD analysis of the NT-3 gene. When rs6332, rs6489630, and rs11063714 were examined in pairs, a weak LD was noted.
Linkage Disequilibrium Plot of NT-3 Gene.

Discussion
In the current study, we found that the rs 6489630 variant of NT-3 is associated with cognitive impairment in BPAD. The attention score was found to be reduced in the CT genotype in comparison with the TT and CC genotypes of the rs6489630 variant. The visuospatial ability score was reduced in the GG genotype of the rs11063714 variant.
The NT-3 was explored as a possible candidate gene in BD, with observed reductions in NT-3 mRNA levels among affected individuals. 27 Several studies have investigated the link between NT-3 gene variations (rs6332 and rs6489630) and cognitive function in neuropsychiatric disorders, indicating possible influences on attention deficits, executive function, and amnestic mild cognitive impairment.12–14 In a recent study from our laboratory, we reported that NT-3 gene polymorphism was associated with cognition impairment in schizophrenia. 18 In this study, we analyzed the relation of NT-3 SNPs with cognitive status in BD.
The rs6489630 (C > T) is a downstream variation found within an intron on the 3’-end. The rs11063714 variant (G > A) occurs downstream in the intron of the NT 3 gene. The rs6332 (G > A) is a silent genetic variation within exon 1 of the Pro-NT-3 gene. The distribution of rs6489630, rs11063714, and rs6332 were in concordance with Hardy-Weinberg Equilibrium, suggesting no change in allelic characteristics across generations.
In our study, we did not observe any significant difference in genotype frequency and allele frequency of NT-3 SNPs (rs6489630, rs11063714, and rs6332) between controls and BD. Genetic model analysis supported these findings, suggesting NT-3 polymorphism may not be associated with the risk of BD. Also, we did not find any significant variations in the genotype and allele frequencies of NT-3 variants among BD subgroups (manic episode, depressive episode, and remission) and controls (data not shown). LD analysis demonstrated a weak LD between the NT-3 SNP pairs.
Impaired cognition is intrinsic to BD and is linked with challenges in both occupational and interpersonal functioning. In the current study, 83% of bipolar patients (n = 146) were found to have cognitive impairment. Among the genetic variants of NT-3, rs6489630 was related to cognitive impairment (P = .01). When cognition scores were analyzed between rs6489630 genotypes, we found that the attention score was reduced in the CT genotype (P = .028) when compared to the CC and TT genotypes. The rs11063714 variant was not associated with cognitive dysfunction. However, the GG genotype of rs11063714 was associated with a significantly lower visuospatial ability score (P = .044) compared to the AG genotype in BD. The rs 6332 variant did not show any significant association with cognitive status in patients with BD.
Altered levels of NT-3 may impact BD by affecting neuroplasticity, synaptic function, and the viability of neurons. 9 Previous research has presented conflicting findings on NT-3 levels in BD.29,30 NT-3 levels (P = .269) in our study were not significantly different between bipolar patients and controls, which was consistent with those of Barbosa et al. 30 The differences in findings may be due to various factors such as all patients in our study were under treatment follow-up, with most being euthymic and disparities in inclusion criteria (type I BD in our study versus types 1 and 2 BD in previous studies). When bipolar patients were classified into various mood states, plasma NT-3 was decreased in the manic episode group (P < .05) in comparison with control and remission groups. Also, we observe that NT-3 was correlated with visuospatial ability score (r = 0.180, P = .017), YMRS (Young Mania Rating Scale) (r = −0.221, P = .003), and HDRS (Hamilton Depression rating score) (r = 0.209, P = .005) indicating that NT-3 is linked with the severity of the illness and cognitive status in BD. NT-3 levels were not significantly altered among different genotypes of NT-3, suggesting it was not affected by NT-3 gene polymorphism.
The main limitation of the study was the non-inclusion of drug naïve BD cases since all the patients were on follow-up either with monotherapy or combination therapy, and most of the patients were in remission. Ethical constraints did not permit us to assess cognitive function in controls.
Conclusion
NT-3 genetic variants were not associated with the risk of BD. The rs6489630 variant was related to impairment of cognition in BD. Plasma NT-3 was related to the severity of the illness and cognition scores in BD. Further studies are needed to investigate the NT-3 gene expression and its association with cognition in BD.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The study was approved by the Ethics Committee for Human Studies at JIPMER (Approval Number - JIP/IEC/2022/020).
Informed Consent
Written informed consent was obtained from all the patients prior to the study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.