
Abstract
Background:
Attention Deficit Hyperactivity Disorder (ADHD) is among the most prevalent psychiatric disorders observed in children, which causes significant caregiver burden in terms of psychological, emotional, physical, and financial status. The current study correlates the severity and subtypes of ADHD with caregiver strain in children with ADHD.
Methods:
A cross-sectional study in which 40 caregivers of children with ADHD were assessed using a semi-structured proforma, Caregiver Strain Questionnaire (CSQ), and Vanderbilt ADHD Diagnostic Parent Rating Scale (VADPRS).
Results:
The mean global score of caregiver strain in this study was suggestive of moderate caregiver burden. The combined subtype of ADHD was the most common (42.5%) and had the greatest mean score of severity in this study, but it caused the least caregiver burden (P < .05). The inattentive subtype of ADHD was causing the greatest caregiver strain in all the domains of strain (objective, subjective externalized, and subjective internalized) [P < .05]. Most of the children had co-morbid psychiatric conditions (67.5%), of which oppositional defiant disorder was the commonest (60%) and caused significant caregiver strain in all the domains (P value even up to <.01 and <.001 for some domains).
Conclusion:
The severity of caregiver burden is influenced by the subtype of ADHD and the existence of co-morbid psychiatric conditions. Applying such findings in routine clinical practice can be more helpful for improving the overall well-being of the child and the caregiver.
To better understand the caregiver burden, a detailed evaluation of caregiver strain and its various domains is needed. The current study findings suggest that the caregiver burden is not always directly proportional to the severity of symptoms of ADHD. It is determined by the subtype of ADHD and the presence of co-morbid psychiatric conditions.Key Messages
Attention Deficit Hyperactivity Disorder (ADHD) is characterized by a consistent pattern of inattentiveness and hyperactive-impulsive behavior that is not aligned with an individual’s developmental stage, negatively impacting their functioning in social, academic, or occupational environments. 1 It ranks as one of the most prevalent psychiatric disorders in childhood, with prevalence rates ranging from 5.9% to 7.1%. 2 These children tend to be more challenging, disruptive, impulsive, loud, and prone to injuries. 3 They find difficulty in regulating their behavior. They are unable to meet the expected norms, which is further worsened by co-morbid psychiatric conditions like behavioral disorders (conduct disorder, oppositional defiant disorder), emotional disorders (like depression or anxiety disorders), learning disabilities, etc. It causes a significant caregiver burden.
Caregiver burden refers to the emotional, social, financial, physical, and psychological challenges that arise in response to the needs and demands of assisting someone unable to care for themselves due to illness or disability. 4 Caregiver strain quantifies the caregiver burden in terms of observable changes in the distress felt by the caregiver. It mainly assesses the effect of the child’s behavioral and emotional symptoms on the caregiver rather than the caregiver’s biases. Elevated levels of caregiver burden negatively influence the well-being and quality of life of caregivers and, in turn, affect the care provided to those children. 3 The factors related to caregiver burden remain to be fully comprehended. Strategies aimed at alleviating caregiver burden depend on the availability of information regarding the level and associated factors of the burden.
The Children’s ADHD Telemental Health Treatment Study (CATTS) done in the United States evaluated the cumulative effects of co-morbid conditions with ADHD with caregiver distress. 5 Caregivers’ distress was assessed with the Patient Health Questionnaire-9, Parenting Stress Index, and Caregiver Strain Questionnaire (CSQ). The results revealed higher caregiver distress among children having co-morbid conditions with ADHD. They concluded that caregivers’ distress needs to be considered when creating treatment models for children with ADHD. Another study done in Iran used the Zarit Burden Interview to assess the caregiver’s perceived burden and discovered a notable connection between the severity of ADHD and caregiver burden, 6 with the highest in the combined subtype. A study done in Hyderabad, 7 Pakistan, determined the level of burden among caregivers of children with ADHD using the Burden Assessment Scale (assessment of objective and subjective consequences) and correlated it with the socio-demographic details. They found that single parenting and higher education were associated with a considerably higher burden of care. A study done in Rohtak, 8 India, measured stress levels in parents of ADHD children. Parent Stress Scale was used to assess subjective stress in the parents. In the different studies quoted here, some have not evaluated the relation between the subtypes of ADHD and caregiver burden. Most of them have not assessed the caregiver burden in terms of caregiver strain, which is mainly a function of the child’s behavioral and emotional symptoms rather than the caregiver’s biases. Some of them have taken into account parental psychopathology but did not measure indices of life functioning or impairment.
Many studies have been done in other countries on ADHD. However, more research is needed in India, especially on the burden of caregivers. The burden of caregivers can be an important concept in a developing country like India. This study is the first of its kind in India to assess caregiver burden in terms of caregiver strain. Therefore, the present study aimed at assessing the levels of caregiver strain in children diagnosed with ADHD in South India.
Methods
The study was conducted following the guidelines outlined in the Declaration of Helsinki. The Institutional Research Ethics Committee granted Ethics approval for the study. Assent from participants and written consent from parents/guardians were obtained. This study, which was cross-sectional in design, was carried out in the following outpatient units of a tertiary healthcare center located in a metropolitan city: the Department of Clinical Psychology, the Child Development Unit in the Department of Pediatrics, the Department of Psychiatry, and the Child Rehabilitation Center. The sample comprised 40 caregivers of children diagnosed with ADHD. The data collection was done over twelve months, from October 2018 to September 2019. The purposive sampling method was used to collect the samples for this study. The maximum number of samples was collected from the Department of Clinical Psychology (24 samples), where the patients were referred (mainly from the Child Development Unit in the Department of Pediatrics) for assessment. The samples used to be selected only after the child was diagnosed with ADHD after the assessment. Some samples were known cases collected directly from the Child Development Unit in the Department of Pediatrics (six samples), the Department of Psychiatry (five samples), and the Child Rehabilitation Center (five samples).
The study included the caregivers (parents or legal guardians) of children aged 6–12 years who were diagnosed with ADHD as per DSM-5 criteria. 1 The caregivers should have resided for at least 50% of the time during the last 6 months from the time of interview and be willing to consent to participate in the study. The caregivers of those children were not taken for the study who had intellectual disability (IQ < 70), co-morbid cerebral palsy, or co-morbid chronic physical illness; children with psychiatric disorders other than ADHD and its co-morbidities [conduct disorder, oppositional defiant disorder, anxiety or depression]; and the caregivers who were diagnosed with mental illness or were not willing to provide informed consent.
Tools and Instruments
Caregiver Strain Questionnaire
The CSQ was used to assess caregiver strain. 9 It evaluated the level of extra demands, responsibilities, and challenges that caregivers and families faced due to caring for a child with emotional or behavioral disorders. It also assessed the psychological impact of the caregiving function. It contained 21 items, which assessed strain over the previous six-month period. It had three related but distinct subscales. Objective strain (observable negative events such as interruption of personal time, missing work or other duties, etc.), subjective externalized strain (such as feeling embarrassed or angry toward the child, etc.), and subjective internalized strain (such as feeling sad, guilty, etc.).
Vanderbilt ADHD Diagnostic Parent Rating Scale
The Vanderbilt ADHD Diagnostic Parent Rating Scale (VADPRS) was utilized as a psychological evaluation instrument for evaluating symptoms of ADHD and their impact on behavior and academic achievement in children between the ages of 6 and 12 years. 10 It also included items related to oppositional defiant disorder, conduct disorder, anxiety, and depression, often found co-morbid with ADHD. The parent version of the VADPRS contains six subscales. The scale has a good test-retest reliability of more than 0.80, with high concurrent validity and a sensitivity of 0.80.
Permission to use the assessment tools mentioned above was obtained from the relevant copyright holders.
Statistical Analysis
The data analysis was conducted using SPSS version 20, employing both “descriptive” and “inferential” statistical methods. Frequency counts were generated for each discrete variable. For all continuous variables, the mean and standard deviation were calculated. Analysis of variance, along with Pearson’s product-moment correlation tests, was utilized to explore the relationship between the severity of ADHD and the caregiver burden.
Results
Socio-demographic Characteristics of Caregivers
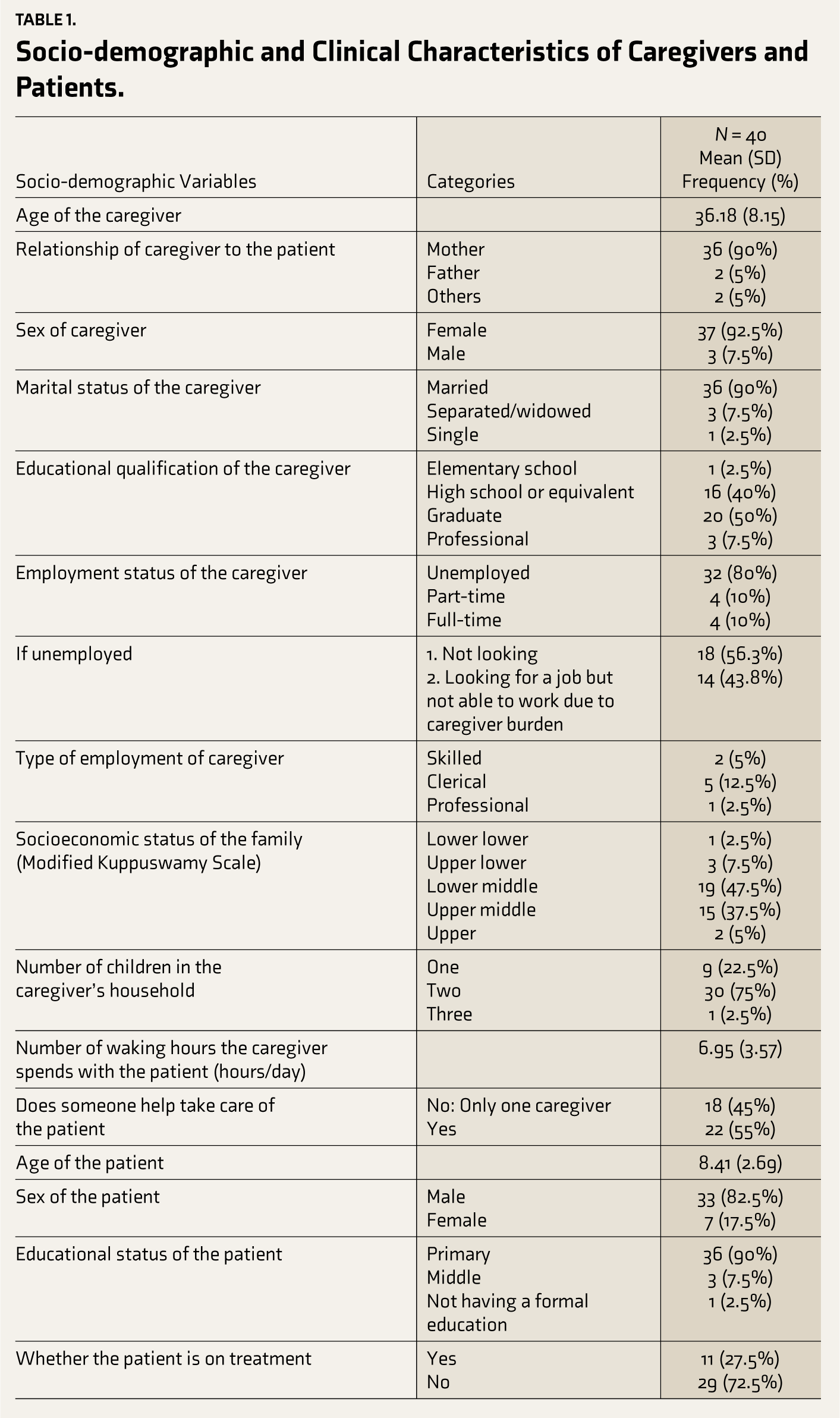
Most of the caregivers in the study were females, such as mothers, grandmothers, etc. The majority of the caregivers had completed high school education or graduated. More than three-fourths of the caregivers were unemployed. Nearly half wanted to go to work but were not able to because they needed to take care of the child. Nearly two-thirds of the caregivers had clerical jobs. More than three-fourths of the caregivers belonged to the middle socioeconomic class. Three-fourths of the caregivers had two children in their family. The average time (waking hours) spent by the caregiver with the child in the current study was seven hours. More than 50% of the caregivers had support from other family members or relatives in taking care of the child (Table 1).
Socio-demographic and Clinical Characteristics of Caregivers and Patients.
Socio-demographic and Clinical Characteristics of Children with ADHD
The mean age of children with ADHD in the current study was between eight to nine years. Around 80% of the children in the current study were males. Three-fourths of the children were not on treatment (Table 1).
Caregiver Burden in Children with ADHD
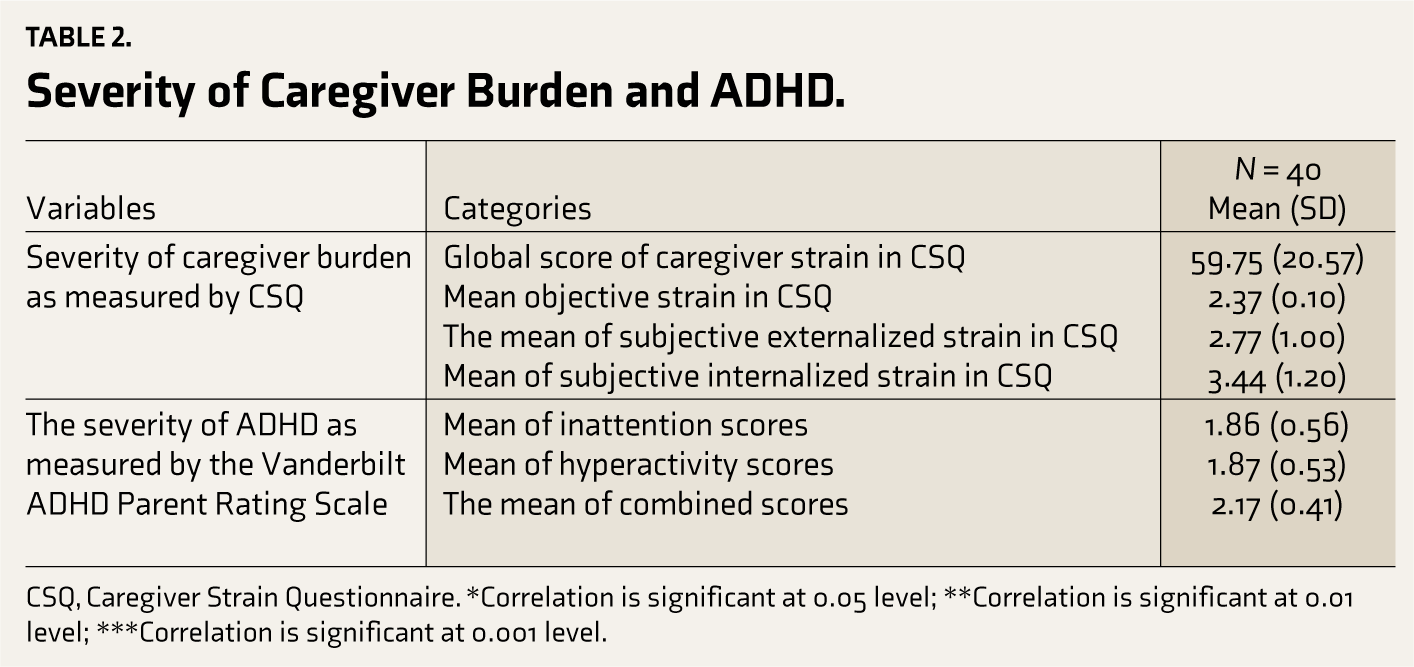
The mean global score of caregiver strain suggested a moderate burden among caregivers of children with ADHD. The mean of subjective internalized strain was the greatest among all three subscales. The mean of subjective externalized strain was slightly higher than the mean of objective strain (Table 2).
The Severity of ADHD in the Children
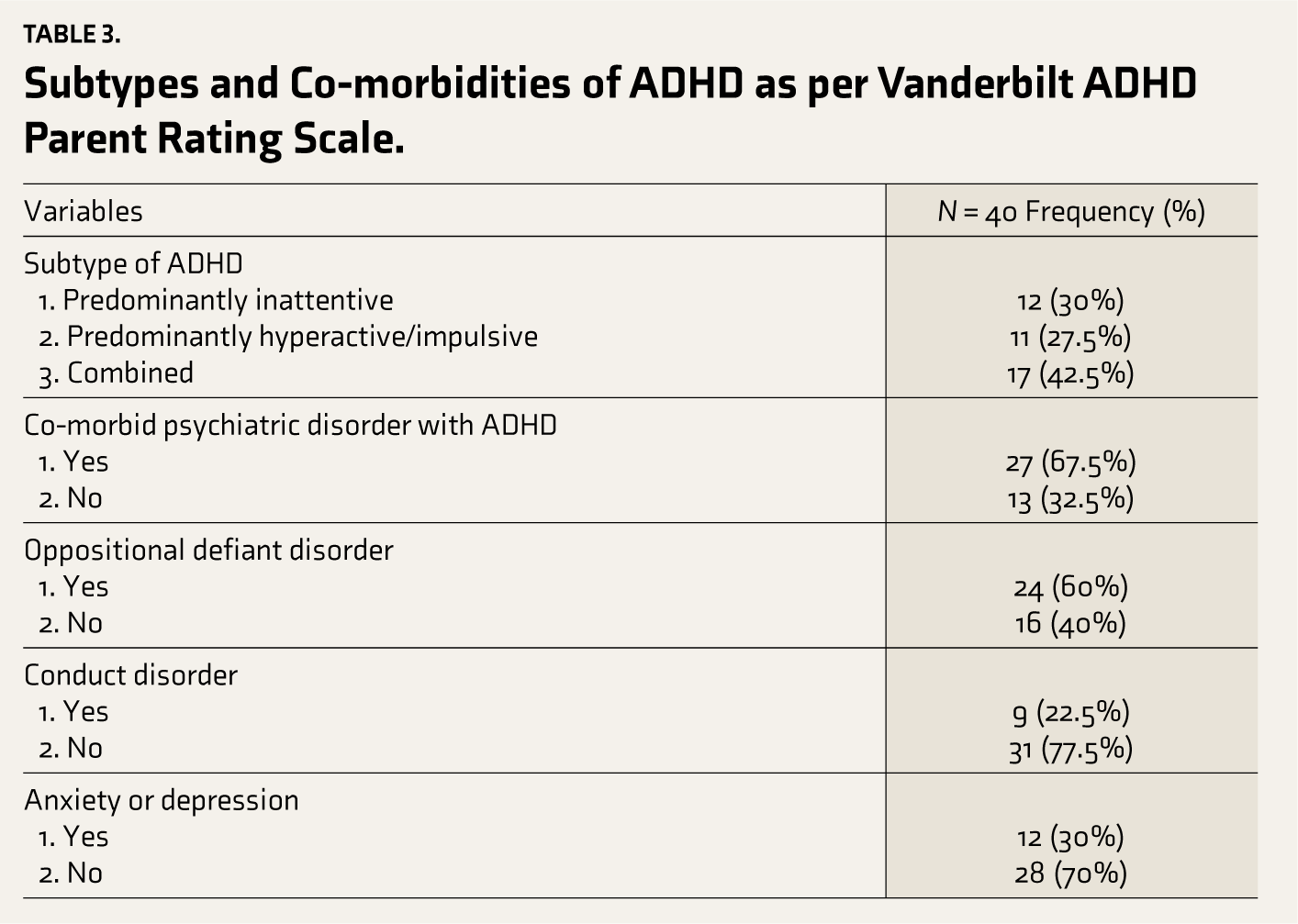
Most of the caregivers reported greater severity of inattentive symptoms. Likewise, they reported moderate to severe severity of hyperactivity/impulsive symptoms. Very few caregivers reported conduct problems in their children. Only a few caregivers reported anxiety/depressive symptoms in their children, but in some, it was slightly severe. In the current study, more children were qualifying for the combined subtype of ADHD (around 40%), followed by the inattentive subtype, which was more common (30%), and then the hyperactive/impulsive subtype (27%). Also, the mean scores of the combined subtype were the highest. On the other hand, the mean scores of inattention and hyperactivity were nearly the same. This suggests that the combined subtype is the most severe form of ADHD, having symptoms of both hyperactivity and inattention.
Anxiety/depressive disorder was the second most common co-morbid psychiatric condition after oppositional defiant disorder (Tables 2 and 3).
Severity of Caregiver Burden and ADHD.
CSQ, Caregiver Strain Questionnaire. *Correlation is significant at 0.05 level; **Correlation is significant at 0.01 level; ***Correlation is significant at 0.001 level.
Subtypes and Co-morbidities of ADHD as per Vanderbilt ADHD Parent Rating Scale.
Correlation Between Subtypes of ADHD and Caregiver Burden
The inattentive subtype of ADHD had a statistically significant association with all the domains of caregiver strain, which are objective strain, subjective externalized strain, subjective internalized strain, and the global score of caregiver burden. However, the severity of the hyperactive subtype of ADHD had a statistically significant association with the objective strain, subjective internalized strain, and the global score of caregiver strain but not subjective externalized strain. The combined subtype had a significant association with only subjective externalized strain and the global score of caregiver strain. The inattentive subtype of ADHD has caused maximum caregiver strain in all domains. Likewise, the hyperactive subtype of ADHD has caused caregiver burden in all the domains except for subjective externalized strain (Table 4).
Correlation Between Severity of Subtype of ADHD and Caregiver Burden.
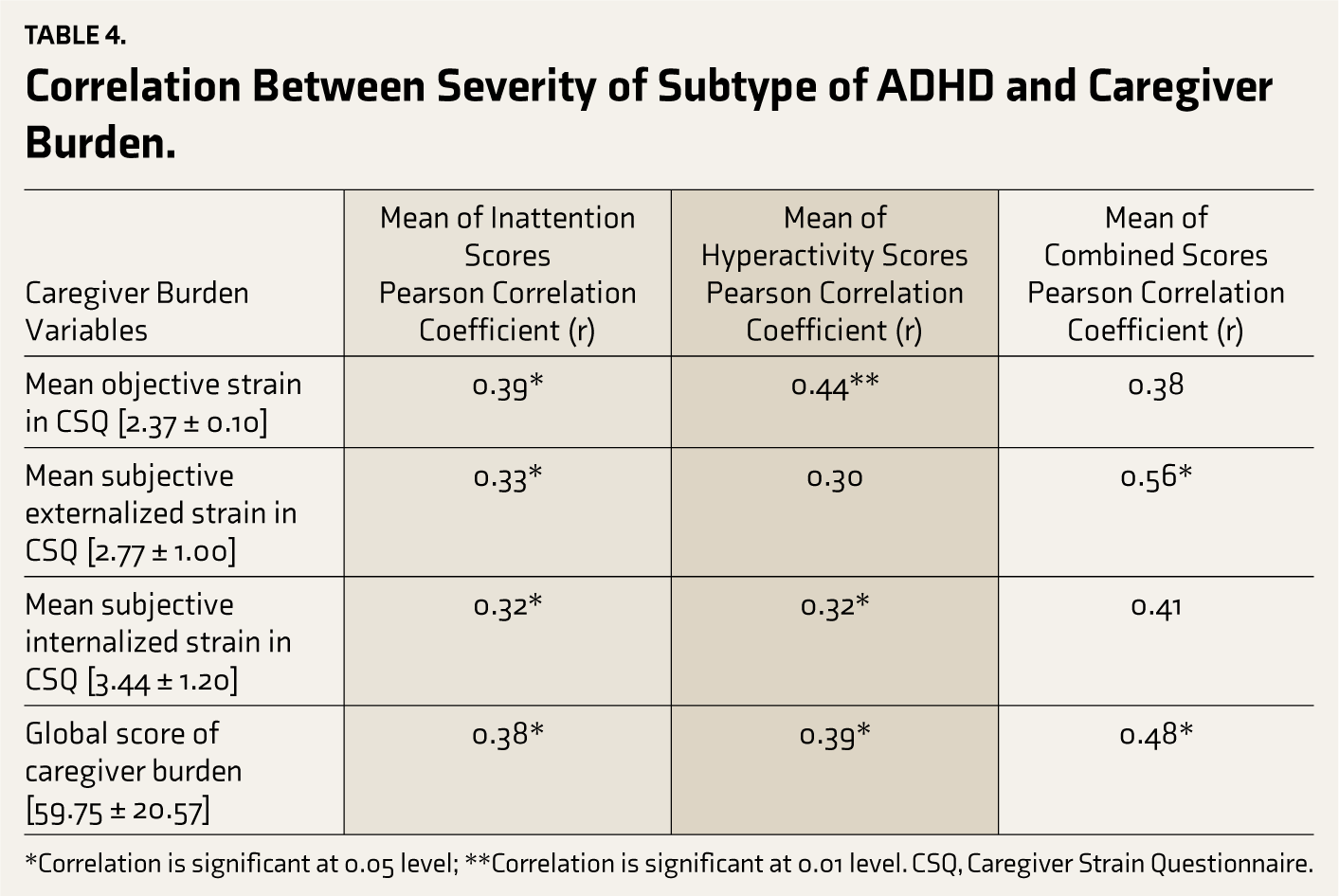
*Correlation is significant at 0.05 level; **Correlation is significant at 0.01 level. CSQ, Caregiver Strain Questionnaire.
Correlation Between the Presence of Psychiatric Co-morbidity in ADHD and Caregiver Burden
The presence of psychiatric co-morbidity caused caregiver burden in all aspects, such as objective strain, subjective internalized strain, and the global score of caregiver burden, except for the subjective externalized strain. The presence of oppositional defiant disorder caused statistically significant caregiver burden in all the domains of objective strain, subjective externalized and internalized strain, and overall scores of caregiver burden. At the same time, the presence of conduct disorder and anxiety/depression in the child had no statistically significant association with the caregiver burden and its domains (Table 5).
Association Between Co-morbid Psychiatric Disorder and Caregiver Burden.
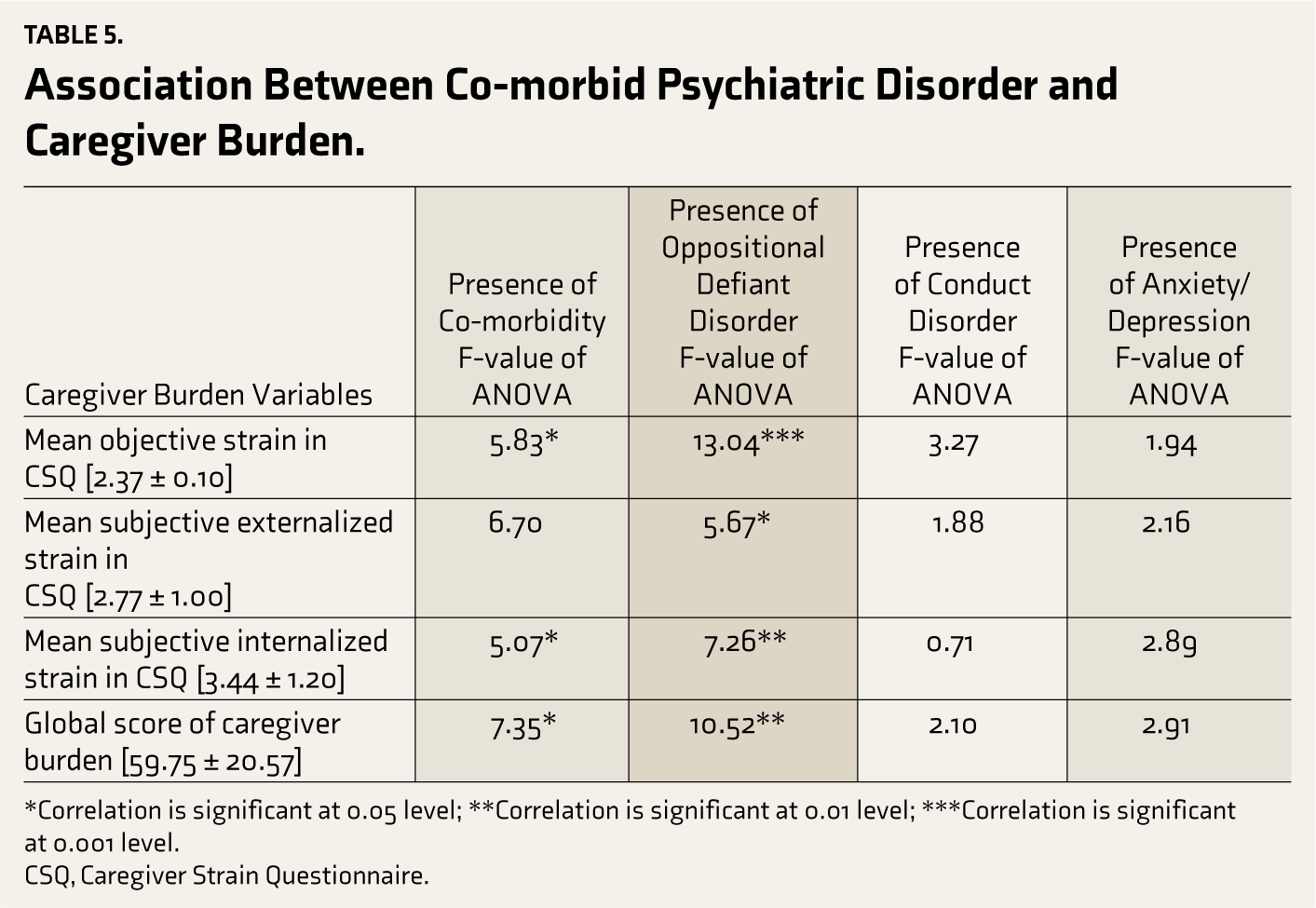
*Correlation is significant at 0.05 level; **Correlation is significant at 0.01 level; ***Correlation is significant at 0.001 level.
CSQ, Caregiver Strain Questionnaire.
Discussion
Correlation Between Subtypes of ADHD and Caregiver Burden
The combined subtype was the most severe form of ADHD, but it does not lead to the greatest caregiver burden as compared to the other subtypes. Thus, in the current study, it was found that the inattentive subtype of ADHD had caused maximum caregiver strain in all the domains. This could also be due to more concern and worries related to the child’s learning skills and academic performance, leading to parents spending more time making them practice, causing exhaustion. These results aligned with the findings from the study conducted by Bussing and colleagues, who found that inattentive symptoms predict caregiver strain. 11 On the other hand, it was contrary to the results of the research conducted by West et al., who had found higher rates of depression in the mothers of children with the combined subtype of ADHD. 8 Yang et al. and Tzang et al. also found higher stress levels in parents due to the combined subtype. 12 Even an Indian study had revealed greater stress levels due to the combined subtype of ADHD than any other subtype. 8 One of the reasons for these contradictory findings is the difference in the quality of caregiver strain from caregiver burden and parenting distress. The caregiver strain quantifies the burden and the experiences of the caregiver and measures it in various dimensions, like the observable changes and the magnitude of distress. It is also largely a function of the child’s behavioral and emotional symptoms rather than the function of the caregiver biases. 13 Hence, the study done by Bussing and colleagues measured caregiver strain and found its significant association with the inattentive subtype of ADHD and not the combined subtype. However, the other studies with contradictory findings measured parental psychology and stress levels, which are more of the subjective version of the caregiver. This could be the possible explanation for the difference in the results of the studies mentioned above.
Likewise, the hyperactive subtype of ADHD has caused caregiver burden in all the domains except for subjective externalized strain. This possibly may be due to more externalizing behavior found in children with the hyperactive subtype of ADHD. 14 Also, psychiatric co-morbidities like oppositional defiant disorder and conduct disorder are found more in association with hyperactive symptoms either in the hyperactive subtype or the combined subtype of ADHD. 14 There is difficulty in dealing with the externalizing behavior of the child by the caregiver, and this leads to lesser satisfaction in their relationship with the child and more negative beliefs. 15
Correlation Between the Presence of Psychiatric Co-morbidity in ADHD and Caregiver Burden
The findings of the current study, as explained in the results section, are similar to the previous studies where oppositional defiant disorder symptoms caused more caregiver strain due to difficulty in dealing with the opposition by the child.16,17 The parent may deal with such problems with less effective parenting strategies, express lesser satisfaction in their relationship with the child, and hold more negative beliefs. 17 At the same time, the presence of conduct disorder and anxiety/depression in the child had no statistically significant association with the caregiver burden and its domains. No other previous studies also mentioned the relation between the presence of conduct disorder in ADHD and caregiver burden. Also, the presence of anxiety and depression may have caused more impairment and distress in the child. However, it might be often overlooked by the caregiver and hence does not contribute much to the caregiver’s burden.
Thus, caregiver burden is a broader concept and consists of multiple dimensions and factors that interact and play a role. Many studies have attempted to study the quality of caregiver burden in terms of parental psychopathology, strain, etc. The current study has assessed the caregiver burden in terms of “caregiver strain,” which is a slightly different concept of measuring caregiver stress. Multiple other factors and dimensions of the caregiving concept still need to be explored and studied for better understanding and to meet the unmet needs of the caregivers. All these will lead to improvement in the management and providing proper support to the children with ADHD and their families and planning a holistic approach and management.
Implications
The caregiver burden is not directly proportional to the severity of symptoms of ADHD. The results revealed moderate levels of caregiver burden in the current study. The further intensity of caregiver burden is determined by the subtype of ADHD and the presence of co-morbid psychiatric conditions like oppositional defiant disorder. Because of the quality of symptoms in the hyperactive and combined subtypes, it may manifest as slightly severe behavioral problems. However, it was found in this study that the inattentive subtype causes the greatest caregiver strain in all domains. There should be suggestions for measures in routine clinical practice regarding how to prevent caregiver burnout. There is scope for further research on ADHD in the near future because it is emerging as a common childhood disorder because of increasing awareness. There is hope for improvements in treatment modalities in the near future, which may give better treatment satisfaction.
Limitations
The socio-demographic factors of the caregivers and children with ADHD were not assessed in detail. Studying caregiver burden in each stratum of the various socio-demographic factors can give more clues in predicting caregiver burden and its interaction with other factors. This was a cross-sectional study. A longitudinal study would have given better results because the long duration of the caregiving role and the need to adjust to it could decrease the caregiver’s reporting of burden. In addition, the demands and the challenges faced by the child and the caregiver can change with time and accordingly can affect the intensity of the burden. A comparatively modest sample size was used. The effect size of the results will, therefore, be smaller if a link between variables is discovered with such a small sample size. The study samples were collected from the Department of Psychiatry, the Child Development Unit and Rehabilitation Center, and the Department of Clinical Psychology of our hospital. Selection bias is likely to occur because it was a general hospital setting. A metropolitan city’s tertiary care facility served as the source of the study samples. Therefore, it was not possible to extend the results to the population samples.
Conclusions
Currently, the available pharmacological and non-pharmacological management may not lead to complete improvement of symptoms; thus, appropriate measures should be taken to prevent caregiver burden. The findings of the current study can have important implications for understanding the broad concept of caregiver burden and how to mitigate it apart from managing the symptoms of ADHD. Understanding such a concept can improve the quality of care and support for the child. The current study findings suggest that apart from the self-reported stress and the psychopathology by the caregiver, there is a need for detailed evaluation in terms of caregiver strain and its various domains to get a better picture of the caregiver burden.
The present study will initiate future research in India. Addressing such findings in routine clinical practice can be more helpful for improving the overall well-being of the child and the caregiver.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
Karthikeyan Child Development Unit (SRIHER), Vidya Sudha (Special Education School, SRIHER, Chennai) and Dr Vivian Kapil (Psychiatrist).
Authorship Approval
All authors have read and approved the manuscript, confirming that the requirements for authorship have been met and that each author believes the manuscript represents honest work.
Copyright and Property Rights
To the best of the authors’ knowledge, the manuscript does not infringe upon any copyright or property rights of any third party.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration regarding the use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The ethical approval was obtained from the Institutional Research Ethics Committee, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai, Tamil Nadu (Ref. No: CSP-MED/18/JUN/44/103, Date: 24.09.2018).
Patient Consent
Written informed assent and consent were obtained from all participants in the study.
Presentations or Awards at a Meeting
There were no presentations or awards related to this article at any meeting.
Prior Presentation
The article has not been presented elsewhere prior to submission.
Publication Status
The article being submitted has not been published, simultaneously submitted, or accepted for publication elsewhere.
Study Location
The current study was conducted at Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.