
Abstract
Background:
The coronavirus disease 2019 (COVID-19) pandemic accelerated the utilization of telepsychiatry services across populations. Research on satisfaction with video consultations has yielded mixed results. The utilization of telepsychiatry services in India identifies technological difficulties as a barrier. This study investigates specific access and communication-related factors that affect patient and caregiver satisfaction.
Methods:
A cross-sectional observational study was conducted using a newly developed instrument comprising two domains: access-related and communication-related factors. Data was collected from consenting adult patients and caregivers previously engaging in video consultations. The instrument’s psychometric properties were examined using Cronbach’s alpha, split-half reliability, and factor analysis. Associations were evaluated using appropriate statistical methods.
Results:
A total of 78 respondents were included in the analysis. Four subject experts reviewed the instrument’s content validity, and the scale’s psychometric properties showed an overall Content Validity Index (CVI) of 0.968 and Cronbach’s alpha of 0.917. The study showed high satisfaction with telepsychiatry consultation, with differences in scores attributed more to communication-related factors than access-related factors. A multivariate regression analysis revealed that the type of device (laptop better than phone) and age were significantly associated with total satisfaction scores.
Conclusions:
The study highlights modifiable factors for telepsychiatry satisfaction using a newly developed instrument with robust initial psychometric properties. Limitations include the possibility of a biased sample population and a modest response rate from respondents. Future directions entail external validation of the satisfaction scale and utilization of the findings to broaden the scope of mental health coverage using telepsychiatry.
We conducted a cross-sectional observational study to assess the satisfaction with video consultation among users Overall satisfaction was good, with older patients and individuals using laptops having higher satisfaction. Satisfaction with video consultation can be improved with modifiable factors such as device, thus potentially improving access to care.Key Messages:
The use of video technology in psychiatry started as early as 1950. 1 Coronavirus disease 2019 (COVID-19) has hastened the utilization of telemedicine and telepsychiatry across various healthcare delivery systems, geographical regions, and populations. 2 Although not free of drawbacks, video consultations are now a feasible option for continuing care in psychiatry. 3
Research on the satisfaction of patients with telepsychiatry shows mixed findings.4–9 Some studies show cost-effectiveness with increased acceptability and feasibility of video consultations at the user and provider ends.4,5 But other studies indicate poor satisfaction.6,7 Differences have also been noted in the satisfaction levels between psychiatrists and patients. 10 Better end-user experiences are associated with better adherence and clinical outcomes.11,12
Indian studies in the area tend to have samples that are disproportionately skewed toward urban, male, and educated patients.3,13,14 It is unclear whether this is due to sampling biases or reveals systemic barriers to the utilization of telepsychiatry services by other patient populations.
Comfort with the technology used influences attitudes toward telepsychiatry among patients and clinicians.15,16 Technological difficulties are a significant barrier to widening telepsychiatry services in India. 13
Video consultations have proliferated in lower-middle-income countries (LMIC) like India. This increase has been fueled by the increasing availability of digital services through inexpensive smartphones. Studies have shown that mobile phones are the most common device for video consultations across LMICs.14,17
It is unclear whether specific factors related to access and communication (including device, connectivity, and communication process) affect patient and caregiver experiences of video consultations. This exploratory study aimed to address this lacuna in the literature.
Methods
We conducted a cross-sectional observational study at a tertiary care center in South India using an online survey. The Institutional Review Board approved the study (IRB Min no 13459). Data was collected from May to October 2021. We included all consenting adult patients or caregivers fluent in Tamil, English, or Hindi who had used video consultations. The institution’s protocol specified that video consultations could only be utilized by patients seen previously in an in-person consultation. Video consultations were done using the “Jitsi” application. We chose the Jitsi application as it allowed for video conferencing without any additional details from the patient, thus maintaining patient confidentiality.
Instrument Development
We developed an instrument as no validated questionnaire existed for assessing patient experiences with video telepsychiatry in the South Indian context. The literature review and expert input identified two key domains: “access-related factors” and “communication-related factors.” The “access” domain, with nine 10-point Likert items (1 = complete disagreement to 10 = complete agreement), examined device availability, connectivity, technological ease, service access, and financial concerns. The “communication” domain, including fourteen 10-point items (1 = much worse to 10 = much better experience), evaluated language comfort, consultation environment, audiovisual clarity, confidentiality, doubts expression, and treatment instructions clarity (Appendix 1 online). We constructed items such that higher scores meant better experiences. The questionnaire was validated, finalized in English, and translated into Tamil and Hindi. We back-translated the original English version and reviewed it to ensure comparability. The scores on the scale could range from 23 to 230.
Four subject experts assessed each item for clarity, relevance, and essentiality using a 1–4 Likert scale. The instrument had an item Content Validity Index (CVI) of 0.992, an overall CVI of 0.968, and a Cronbach’s alpha of 0.917.
Variables
The primary outcome variable was the total score on the instrument, which was calculated by adding individual ratings of all the items in the instrument. We also calculated “access” and “communication” domain scores.
We collected the sociodemographic details of the participants, including age, sex, education status, and monthly income of their families. We also collected details of the device used, previous experience with video consultations, reasons for choosing video consultations, and location of attending the video consultation.
Statistical Analysis
We used SPSS version 27 for statistical analysis and summarized variables by frequencies/percentages, or mean median, standard deviation, and range. 18 We assessed continuous variables for parametric distribution. Total and domain scores were computed. Using Cronbach’s alpha, split-half reliability, and factor analysis, psychometric properties were examined. Associations were evaluated using chi-square, t-tests, and Pearson’s correlation. Multivariate analysis of the total attitude score was done using linear regression. We dichotomized the total score into “high” and “low” along the mean and did logistic regression. A p value of less than .05 was considered statistically significant.
Results
Four hundred seventy-five patients had registered for teleconsultation during the six-month study period. After excluding the repeat and missed appointments, 240 patients were included in the study. The validated questionnaire was sent to the registered addresses of these eligible patients. Weekly reminders were sent to those who did not respond. Eighty-four responses were received, but six refused to consent to be included in the study. Seventy-eight responses (32.5%) were included for analysis. Of these, 51 responses were from the patient directly, and 27 were from caregivers.
Descriptive Statistics
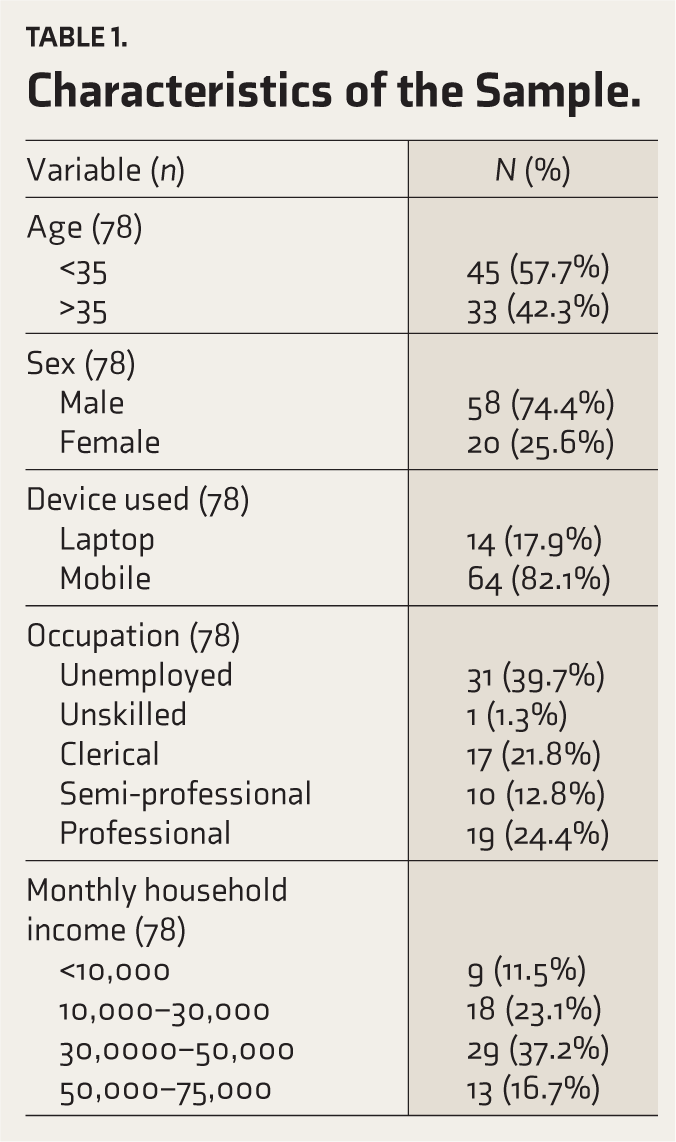
The mean age of participants was 35 years (standard deviation (SD) = 11.8); 74% were male, and three-fourths were first-time video users. Most participants had higher secondary education and were employed, and 65% had a monthly family income of over 30,000 rupees. Eighty-one percent used mobile phones, and 19% used laptops. Reasons for choosing video consultations were COVID-19-related travel restrictions, cost-effectiveness, and emergency needs. Ninety-seven percent of participants attended video consultations from home. Table 1 details the baseline characteristics of the sample.
Characteristics of the Sample.
Psychometric Properties of the Instrument
The complete instrument and its two subdomains, “access” and “communication,” were internally consistent with high Cronbach’s alpha values (0.936, 0.873, and 0.938, respectively). The split-half reliability method showed a high correlation coefficient of 0.925.
The sample was sufficient for a factor analysis as Bartlett’s Test of Sphericity was significant at the p < .001 level and the Kaiser-Meyer-Olkin Measure was 0.835. Three factors were retained. The retained factors explained 85% of the variance. The factor loading pattern corresponded to the theoretical constructs considered while designing the questionnaire.
Patient Satisfaction
Total scores on the instrument were parametric in distribution. The mean score was 165 (SD = 24), with a median of 166. Scores ranged from 105 to 206. Ninety-two percent of users reported overall satisfaction with the results of video consultation compared to face-to-face consultation. Ninety-one percent of the users reported being willing to try video consultation again, and 94% said they would recommend it to others.
Both “access” and “communication” domain scores were parametric in distribution. The mean “access” domain score was 77.8 (SD = 10.36), with a median of 78. Scores ranged from 47 to 90. The mean “communication” domain score was 87.5 (SD = 17.06), with a median of 88.5. Scores ranged from 41 to 116. The mean score per item was significantly lower in the communication domain compared to the access domain (mean difference = 2.39; 95% confidence interval (CI) = 2.13–2.66; p value < .001).
Bivariate Analysis
Patients who used a laptop for the video consult reported higher satisfaction than those who used a mobile phone. They had significantly higher total scores (mean difference = 18.21; 95% CI = 8.15–28.27; p value = .001) and communication domain scores (mean difference = 13.36; 95% CI = 5.30–21.41; p value = .01). There were no significant differences in the access domain scores. Laptop users were likelier to have a monthly income of more than ₹50,000/- per month (odds ratio (OR) = 7.06; 95% CI = 2.02–24.68; p value =.002).
Older patients reported higher satisfaction with video consults. Those with an age of 35 or above had significantly higher total scores (mean difference = 13.83; 95% CI = 2.98–24.67; p value = .01) and communication domain scores (mean difference = 10.89; 95% CI = 3.50–18.28; p value = .01). There were no significant differences in the access domain scores.
Patients with a higher monthly income reported higher satisfaction with video consults. Those earning more than ₹50,000/- per month had significantly higher total scores (mean difference = 12.37; 95% CI = 2.43–22.30; p value = .02) and communication domain scores (mean difference = 9.06; 95% CI = 0.70–17.41; p value = .03). There were no significant differences in the access domain scores.
Patients who were “professionals” by occupation reported higher satisfaction with video consults. They had significantly higher total scores (mean difference = 11.65; 95% CI = 1.01–22.29; p value = .03) and communication domain scores (mean difference = 9.09; 95% CI = 1.38–16.81; p value = .04) compared to other occupations. There were no differences in the access domain scores.
Scores did not vary significantly across gender, educational status, type of internet service, or previous use of video consults. There were no significant differences between responses from patients and those from caregivers.
Multivariate Analysis
We entered age, sex, income, occupation, and type of device used as predictive variables in a stepwise backward linear regression, with the total score as the dependent variable. The regression model was significant (F = 6.108, p value = .003). The R squared of the model was 0.14. Age (p value = .03; B = 0.48; 95% CI = 0.04–0.91) and type of device used (p value = .01; B = 17.73; 95% CI = 4.44–31.02) remained significantly associated with the total score.
Logistic regression (p value = .002; R2 = .27) showed that laptop users were likelier to have high scores (p value = .03; OR = 10.91; 95% CI = 1.27–93.41). Table 2 shows the distribution of scores across groups and significant associations.
Distribution of Scores Across Patient Groups.
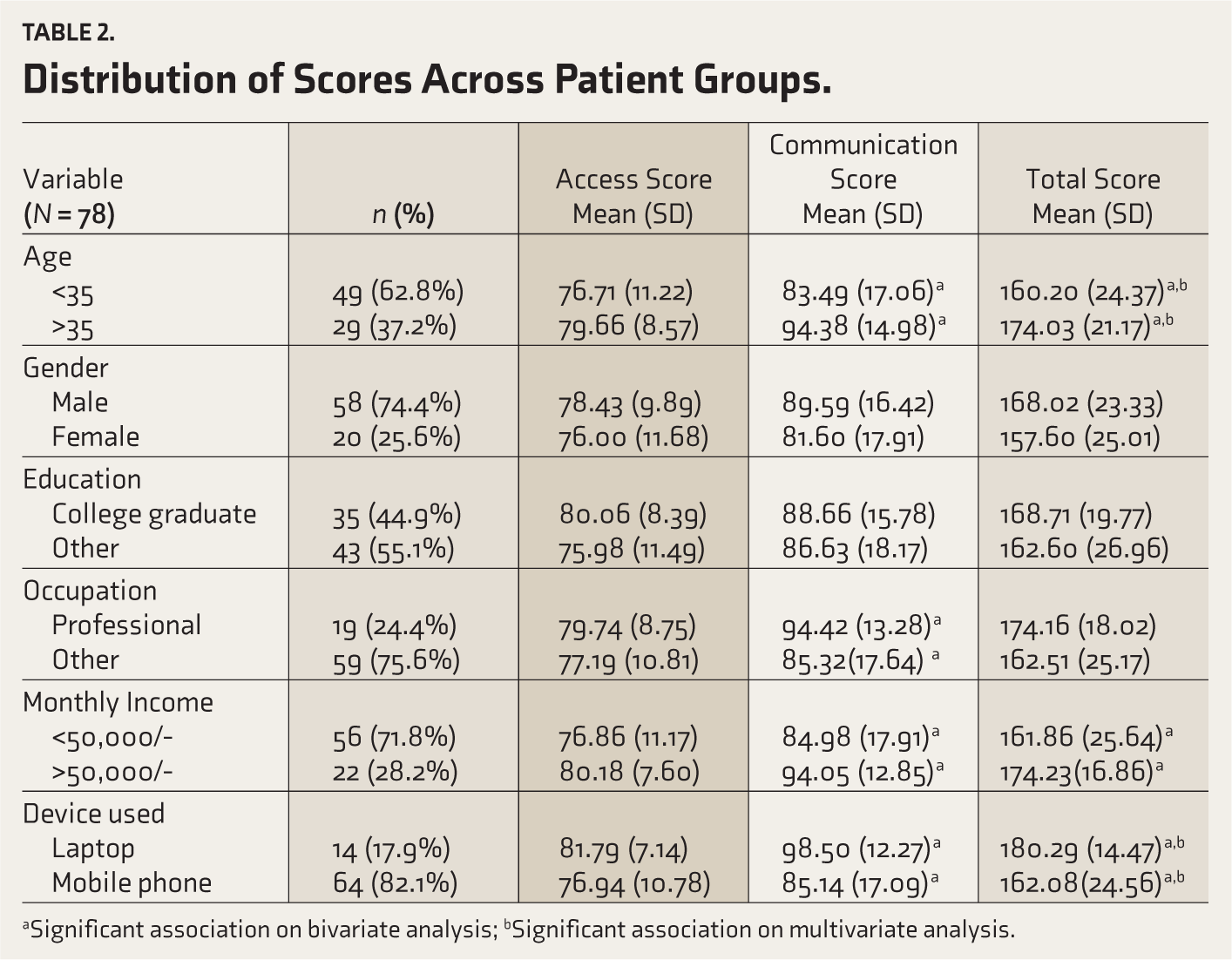
aSignificant association on bivariate analysis; bSignificant association on multivariate analysis.
Discussion
This study reports high satisfaction and positive experiences with video consultations in telepsychiatry. Older, wealthier, and professional patients who used laptops were significantly more satisfied with their experience. These differences in satisfaction are a function of differences in satisfaction in the “communication” domain. Scores in the “access” domain did not vary significantly across sub-groups. This aligns with literature indicating that existing telepsychiatry systems provide reasonable access to video consultation, but smooth communication is a continuing concern.13,19
Some of these factors were associated with each other. Laptop users tended to be wealthier than those using mobile phones. This can be easily understood, as mobile phones have several low-cost options, unlike laptops. Nevertheless, examining the data using regression analysis revealed that the operative factor determining patient satisfaction was the type of device used. Out of the several predictive variables with significant bivariate associations, the type of device and age remained significantly associated with a total score in the linear regression model. Only the type of device showed a significant association with “high” total scores on logistic regression. This study adds to scarce data in the literature in this area. This is a significant finding highlighting the need to optimize video consultation processes for mobile phones, the device most widely used by patients. At the same time, the type of device used can be a modifiable factor. This study suggests that recommending laptops to patients could improve their experiences with telepsychiatry services. However, further research is needed to determine if this association is related to the software used in this institution or is seen across different software platforms.
Interestingly, in this study, patient satisfaction improved consistently with increasing age. While most studies have shown that younger users are more satisfied with video consultations, recent studies have reported a trend toward greater satisfaction in older patients. 20 This study provides further data in support of this trend. This finding could result from increasing awareness and acceptance of video conferencing technology in this age group. 20 The timing of the study and its proximity to the COVID-19 pandemic could have also influenced the acceptability of video consultations in this vulnerable group. 4 However, further research is needed to explore this association.
The study also contributes to the literature by developing a new instrument suited to the local Indian context for assessing satisfaction with telepsychiatry. It demonstrated good initial psychometric properties and good internal consistency. Although the generalizability of this instrument is limited by a lack of external validation, further studies can be planned.
As with other Indian studies in the area, this sample is skewed towards wealthier, more educated males.7,14 This consistent finding across samples of Indian telepsychiatry users suggests systemic inequities in access to video consultations for Indian patients. This finding needs further research and exploration.
Limitations
The modest response rate may have biased the study’s findings by introducing a sampling bias. Other potential sources of bias include recall bias due to retrospective data collection. This study’s single-center, cross-sectional nature limits its generalizability. However, the sample characteristics and study findings are consistent with existing literature and have a measure of external validity.
Conclusion
Though telepsychiatry fills an important clinical care need, better communication and broader access continue to be challenging. Broadening the socioeconomic reach of video consults should be a future focus. Improving patient experience needs further research, but it can be done with modifiable factors like changing the type of device used.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
We would like to acknowledge Department of Psychiatry Unit 2, and the Principal, Christian Medical College Vellore for facilitating and giving permission to conduct this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
We acknowledge the use of AI Microsoft Copilot in March 2025 to refine the language and improve the conciseness of the manuscript. The authors further reviewed and edited the content to ensure accuracy and coherence. We assume full responsibility for the entire content of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Prior Presentation
This study is an original article and it has not been presented elsewhere prior to this manuscript submission.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.