
Abstract
Background:
Pornography addiction is a growing public health concern worldwide, with increasing recognition of its prevalence and consequences in India. This study explores the onset, manifestation, and impact of pornography addiction within the Indian context, addressing the need for culturally relevant research.
Method:
A retrospective, observational, cross-sectional study was conducted using data from 589 individuals who sought treatment for pornography addiction through online and offline healthcare platforms. Patients aged 18 and older were included based on the International Classification of Diseases, 11th Revision (ICD-11) diagnostic criteria for Compulsive Sexual Behavior Disorder (CSBD) (6C72). Data on demographic factors, clinical diagnoses, and treatment outcomes were analyzed using International Business Machines Statistical Package for the Social Sciences (IBM SPSS). Participants received either pharmacological treatment, psychotherapy, or a combination of both.
Results:
The sample included 589 participants, predominantly male (n = 583; 98.98%), with a mean age of 28.98 years; 374 (63.5%) were under 30, and 287 (48.7%) were single. Most identified as heterosexual (n = 568; 96.4%) and had no prior treatment history (n = 465; 78.9%). Common co-morbid sexual dysfunctions included erectile dysfunction (n = 232; 39.4%), premature ejaculation (n = 198; 33.6%), and low sexual desire (n = 109; 18.5%). Pharmacological treatment was most common (n = 338; 57.4%), followed by psychotherapy (n = 207; 35.2%) and combined treatment (n = 44; 7.4%). Age showed significant associations with addiction severity (χ² = 17.07, p = .01), relationship status (χ² = 190.11, p < .01), and treatment modality (χ² = 12.25, p = .01), with younger individuals more often receiving psychotherapy. Severity was weakly but significantly correlated with both age (r = 0.149, p < .01) and number of psychiatric diagnoses (r = 0.098, p < .05).
Conclusions:
Pornography addiction in India is shaped by age, relationship status, and cultural context. These findings underscore the need for age-targeted, culturally informed interventions. Future research should examine longitudinal trends and psychiatric comorbidities to guide comprehensive treatment planning.
Keywords
Younger, single males represented the majority of treatment-seeking individuals, highlighting the need for age and relationship-specific interventions. Psychotherapy was preferentially recommended for younger patients, reflecting clinicians’ emphasis on behavioral approaches in this group. Low prior help-seeking (14%) and self-medication (7%) point to stigma and limited sexual health awareness as barriers to care. Weak correlations between severity, age, and comorbidity suggest that clinician-assessed severity reflects broader psychosocial distress. Findings support the need for culturally informed, multidisciplinary treatment approaches integrating psychiatry, sexology, and psychotherapy.Key Messages:
Pornography addiction, classified under Compulsive Sexual Behavior Disorder (CSBD) in the International Classification of Diseases 11th Revision (ICD-11) (6C72) by the World Health Organization, is characterized by a persistent pattern of failure to control intense, repetitive sexual impulses or urges resulting in repetitive sexual behavior. 1 In this study, pornography addiction refers to the compulsive use of pornographic content that leads to significant distress or functional impairment in personal, social, or occupational domains. Diagnostic criteria were based on ICD-11 guidelines as applied in clinical psychiatric evaluations.
Excessive pornography consumption has been associated with a range of adverse outcomes, including relationship difficulties, sexual dysfunction, poor emotional regulation, and co-morbid psychiatric symptoms such as anxiety, depression, and low self-esteem.2, 3 The neurobiological mechanisms underlying CSBD share similarities with behavioral addictions, including altered reward processing, impulse dysregulation, and compulsivity. 4
Global research—primarily from Western countries—has highlighted the growing public health relevance of CSBD, especially among young adults with easy access to internet pornography. 5 However, there remains a dearth of systematic data from low and middle-income countries, particularly India, where socio-cultural norms, stigma around sexuality, limited sex education, and taboo around help-seeking create unique challenges. 6
Indian studies on pornography use primarily focus on prevalence or adolescent behavior patterns, without addressing clinical presentations, psychiatric comorbidities, or treatment responses among those seeking professional help. 7 This leaves a critical research gap in understanding how pornography addiction presents in psychiatric settings in India, and how socio-demographic variables influence severity and clinical decision-making.
Emerging Indian studies have begun to explore the psychological and behavioral dimensions of pornography use, though clinical research remains sparse. 8 A cross-sectional study among Indian medical students found that 11% reported problematic pornography use, which was significantly associated with anxiety, reduced quality of life, and increased emotional distress. 9 A North Indian community-based study found elevated pornography use among unmarried college students, though only a small proportion met diagnostic thresholds for problematic use. 10 Among college students, rates of problematic use have ranged from 4.5% to 12.5%, with impulsivity and compulsivity frequently reported as co-occurring traits. 11 The Indian Council of Medical Research also reported pornography as one of the more prevalent online behavioral concerns among adults in urban centers such as Bengaluru, exceeding even problematic gaming and social media use. 12 However, these studies primarily focus on prevalence or correlational patterns in general or student populations and offer limited insight into clinical presentations, diagnostic challenges, or therapeutic responses in those seeking psychiatric care. This highlights the importance of research involving treatment-seeking individuals in informing culturally sensitive clinical frameworks and mental health interventions.
This study aims to examine the demographic and clinical characteristics of individuals seeking treatment for pornography addiction in India, evaluate patterns in treatment recommendations (pharmacotherapy, psychotherapy, or both), and explore associations between age, relationship status, and addiction severity. By doing so, the study seeks to inform culturally sensitive, evidence-based intervention strategies and add to the limited empirical literature on this topic in the Indian context.
Methods
This retrospective, observational, cross-sectional study was conducted between January and June 2024 across online and offline psychiatric and sexual health service platforms in India. The Institutional Ethics Committee approved the study. It adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, which are provided as supplementary material.
The study included 589 individuals aged 18 years and above who sought treatment for concerns related to compulsive sexual behavior, with problematic pornography use as the primary complaint. All participants provided informed consent at the time of clinical consultation and were included based on a formal diagnosis of CSBD, as defined by the ICD-11 criteria. 1 While the term “pornography addiction” is used descriptively throughout the manuscript to reflect the presenting concern, it is not a formal diagnostic label.
Diagnoses were made by doctors (holding MBBS, MD Psychiatry, DNB Psychiatry, or Diploma in Psychiatry degrees) using structured clinical interviews. No standardized psychometric tools were used for diagnostic confirmation due to the retrospective nature of the dataset. Clinical diagnosis and severity classification were based on ICD-11 criteria and core CSBD features, including impaired control, persistence despite negative consequences, and marked functional impairment.13, 14
The CSBD severity was rated by treating doctors and recorded in the clinical notes. A six-point-clinician-assessed likert scale for severity model (Normal, Borderline ill, Mildly ill, Moderately ill, Markedly ill, and Severely ill) was used, based on the frequency of pornography use, associated distress, functional impairment, and failed attempts at control. Although inter-rater reliability was not formally assessed, all assessments were conducted by licensed psychiatrists trained in ICD-11 diagnostic criteria.13, 14
Data were extracted from electronic health record systems maintained by the clinical platforms. The dataset included demographic variables (age, gender, marital status, and city), clinical diagnoses, substance use, treatment modalities, and outcome documentation. Records with missing key data were excluded. No sample attrition occurred post-diagnosis, as only patients who completed at least one consultation were included.
Patients were Provided Individualized Treatment Plans
Pharmacological treatment, such as selective serotonin reuptake inhibitors (SSRIs: paroxetine, sertraline, fluoxetine) or bupropion, is used to address compulsivity and co-occurring affective symptoms.15, 16
Psychotherapy, delivered by qualified psychologists, incorporates evidence-based approaches such as cognitive-behavioral therapy (CBT), motivational interviewing (MI), and relapse prevention, targeting emotional regulation, behavioral modification, and awareness of triggers.17, 18
Treatment plans were developed collaboratively between clinicians and patients, based on clinical assessments and patient preferences.
Data were analyzed using International Business Machines Statistical Package for the Social Sciences (IBM SPSS) Statistics, version 14. Chi-square tests were used to assess associations between categorical variables (e.g., age group and treatment type, relationship status and severity), while Spearman’s rank correlation was used to examine non-parametric relationships between ordinal variables such as age, number of diagnoses, and severity score. These methods were selected based on the categorical and ordinal nature of the variables under analysis. 19 A p value of < .05 was considered statistically significant. Data normality was assessed using the Shapiro-Wilk test, which indicated a non-normal distribution. Hence, non-parametric tests (Spearman’s rho, chi-square) were used for correlation and group comparisons.
Results
A total of 589 individuals were included in the study, comprising 583 males (98.98%) and six females (1.01%). The participants’ ages ranged from 19 to 48 years, with a mean age of 28.98 years (SD = 6.34). Of the total, 374 participants (63.5%) were under the age of 30. The mean age for males was 29 years, and for females, 27 years. Geographically, the majority of participants were from Bengaluru, followed by Chennai, Mumbai, and Delhi.
Substance use was reported by 156 participants (26.5%) for alcohol (not meeting diagnostic criteria for alcohol use disorder) and 146 (24.8%) for tobacco-based products. Common co-morbid sexual concerns included erectile dysfunction (n = 232; 39.4%), premature ejaculation (n = 198; 33.6%), and low sexual desire (n = 109; 18.5%). Only 83 participants (14.1%) had previously consulted for the same concern, 41 (7.0%) had self-medicated, and the majority (n = 465; 78.9%) had not sought prior help (Table 1).
Demographic Details of all the Participants.
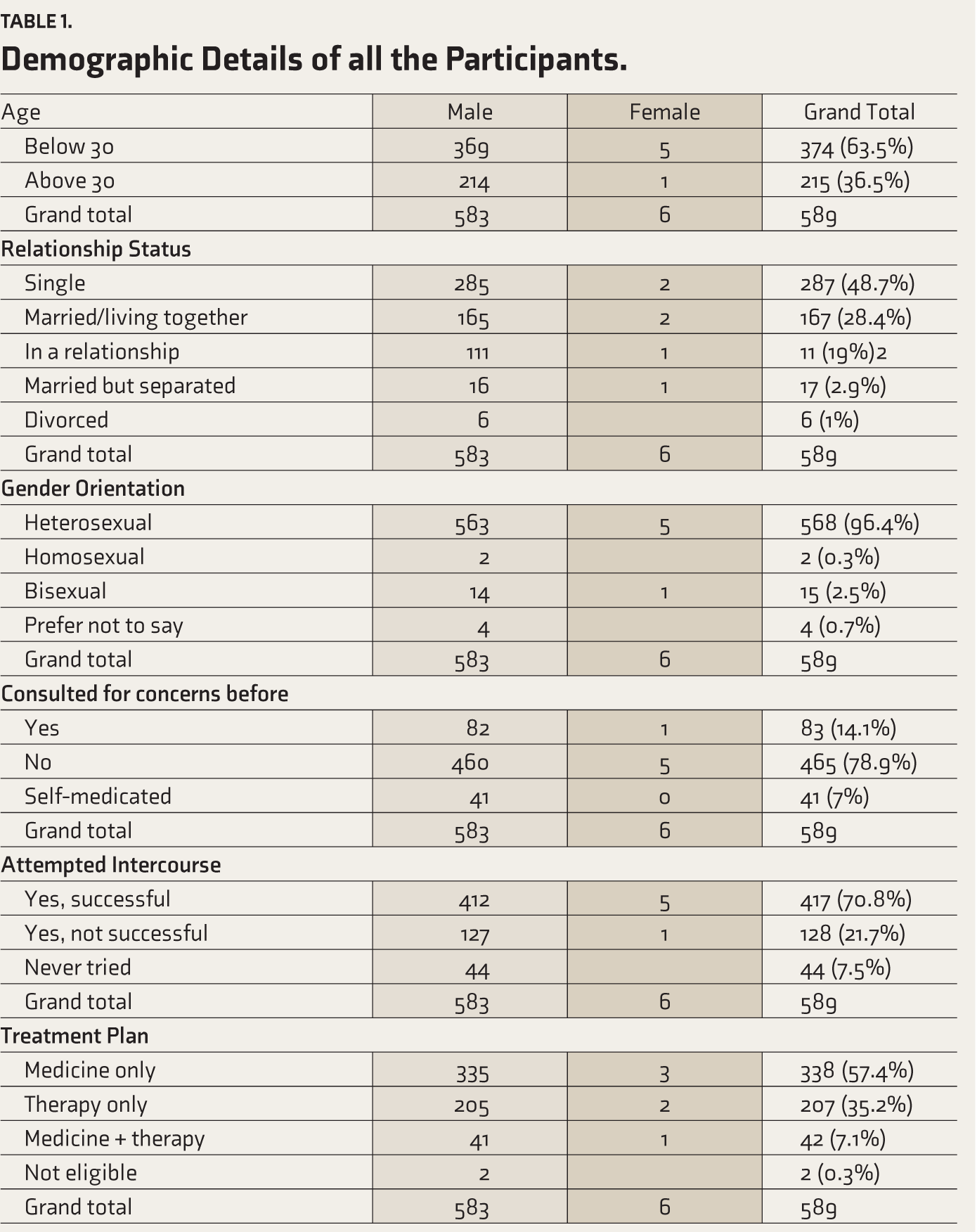
Among all participants, 417 (70.8%) had attempted and successfully completed intercourse, 128 (21.7%) had tried but not succeeded, and 44 (7.5%) had never attempted intercourse. Regarding treatment, 338 participants (57.4%) were prescribed pharmacological treatment only, 207 (35.2%) received psychotherapy only, and 44 (7.4%) were provided a combination of medicine and therapy.
Association Analyses
Age and Severity of Porn Addiction
A chi-square test of independence revealed a statistically significant association between age and the severity of porn addiction, χ²(5) = 17.066, p = .004.
Post-hoc Interpretation
Participants aged 30 and above were overrepresented in moderate-to-severe severity categories, while those under 30 more commonly fell into mild or borderline categories. This suggests that older individuals may present with greater clinical impairment at the time of help-seeking.
Age and Relationship Status
A significant association was found between age and relationship status, χ²(4) = 190.109, p < .001.
Post-hoc Interpretation
Individuals under the age of 30 were disproportionately more likely to be single or in non-committed relationships. At the same time, those over 30 were more likely to be married or cohabiting.
Age and Successful Intercourse
A statistically significant association was observed between age and successful intercourse attempts, χ²(2) = 31.794, p < .001.
Post-hoc Interpretation
Older participants more frequently reported successful intercourse, whereas younger participants more often reported failed or unattempted experiences—possibly reflecting relationship dynamics or performance anxiety.
Age and Treatment Plan Recommended
A chi-square test revealed a significant association between age and the recommended treatment plan, χ²(3) = 12.250, p = .007.
Post-hoc Interpretation
Participants under 30 were more frequently advised psychotherapy, while pharmacological treatment was more commonly recommended for those over 30. This may reflect clinicians’ preference for behavioral interventions in younger individuals.
Correlation Analysis
A Spearman’s rho correlation analysis was conducted to examine associations between age, number of diagnoses, and severity scale (Table 2). A weak but statistically significant positive correlation was found between age and severity (r = 0.149, p < .01), indicating that older individuals may present with slightly greater severity. A similar weak correlation was found between the diagnosis number and severity (r = 0.098, p < .05), suggesting that a higher number of psychiatric comorbidities may contribute to increased clinical burden. The correlation between age and diagnosis number was not statistically significant (r = 0.066, p = .112).
Correlation Matrix for Age, Diagnosis Number, and Severity Scale.
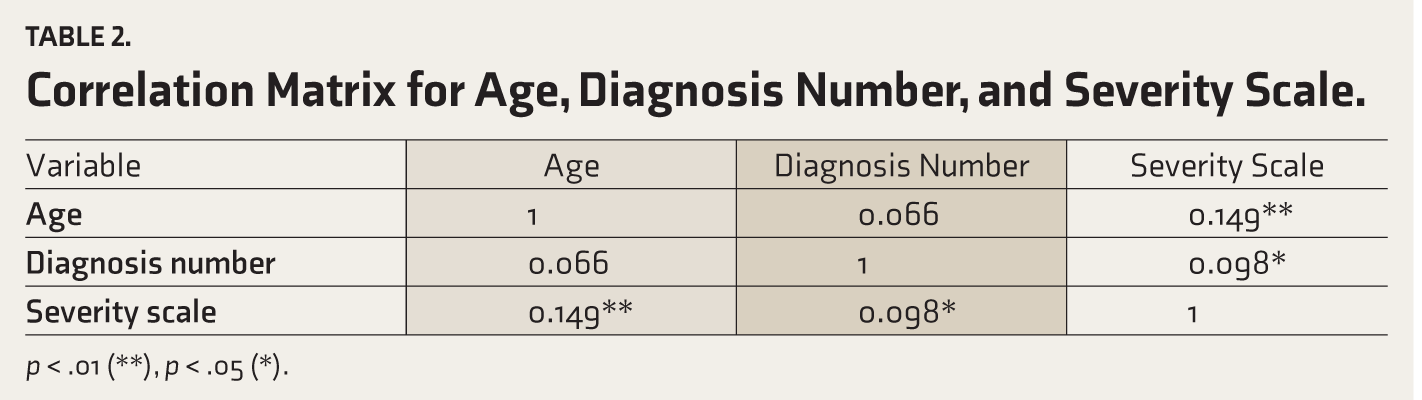
p < .01 (**), p < .05 (*).
Regression Analysis: Predictors of Higher Severity
A binary logistic regression was conducted to identify predictors of higher pornography addiction severity. Significant predictors included younger age (p = .01), being single (p = .01), presence of sexual dysfunction (p = .01), psychotherapy as treatment modality (p = .024), and having more than one psychiatric diagnosis (p = .045). The model explained approximately 21% of the variance in severity (Nagelkerke R² = 0.21) and demonstrated good fit (Hosmer–Lemeshow p = .48) (Table 3).
Binary Logistic Regression Predicting Higher Severity of Pornography Addiction among Participants (
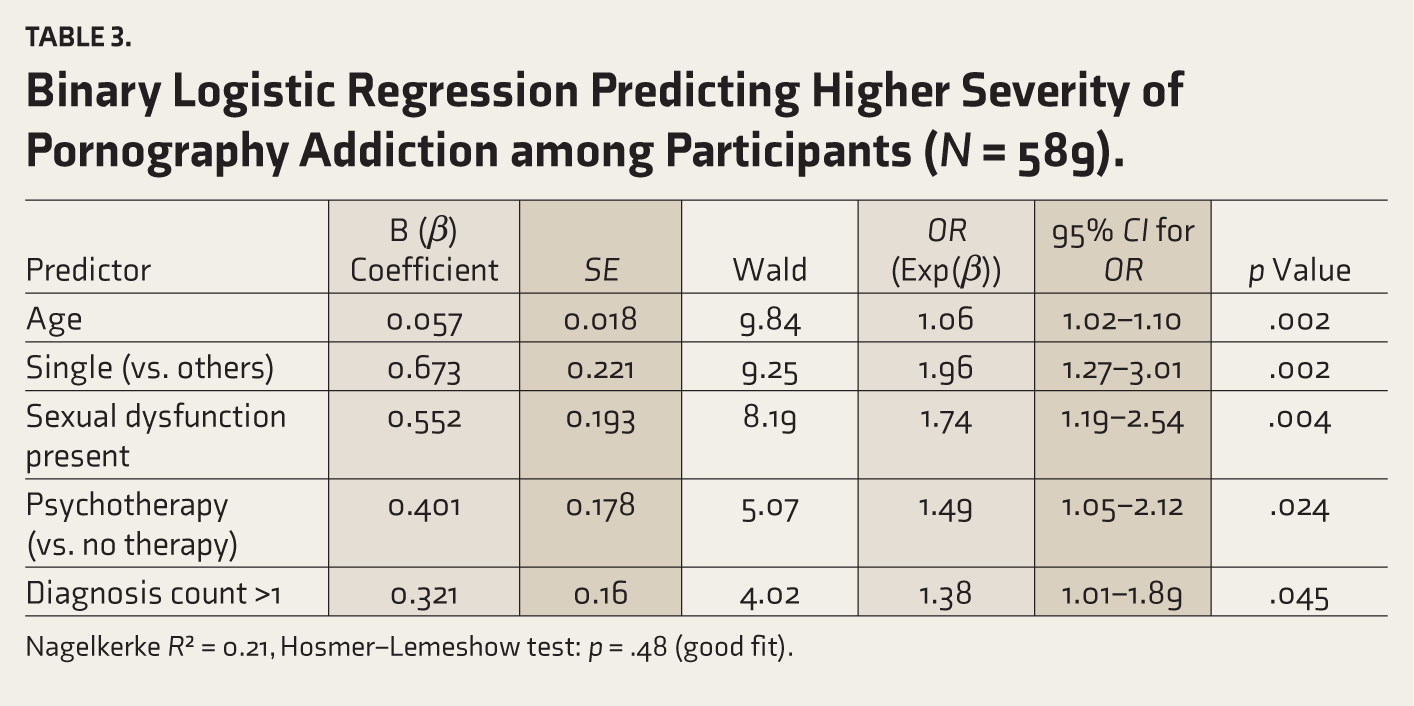
Nagelkerke R² = 0.21, Hosmer–Lemeshow test: p = .48 (good fit).
Discussion
This study provides one of the first clinical profiles of individuals seeking psychiatric help for problematic pornography use in India. The findings illuminate not only demographic patterns and treatment preferences but also cultural barriers and diagnostic considerations within an under-researched domain.
The overwhelming male dominance (98.9%) in the sample mirrors existing literature on pornography use in India and globally, where men are more likely to engage in and seek help for compulsive sexual behaviors.5, 9 A significant proportion of participants were under the age of 30, reinforcing data from both Indian9–12 and Western studies, 5 that identify young adulthood as a period of heightened vulnerability for problematic pornography use.
The study found a statistically significant association between age and the severity of pornography addiction. Interestingly, Spearman’s rho correlation between age and severity (r = 0.149, p < .01) was statistically significant but weak, indicating that while older individuals might report higher severity, the relationship is not strong. Clinically, this suggests that chronological age alone is not a robust predictor of severity, although it may reflect chronicity or delayed help-seeking in some cases. Although statistically significant, the weak correlation (r = 0.098) suggests a subtle influence. This may reflect cumulative distress from comorbidities such as depression or anxiety, though directionality cannot be established in this cross-sectional study. Most patients were managed with either pharmacotherapy or psychotherapy, with only 7.4% receiving combined treatment. Pharmacological treatment, particularly SSRIs and bupropion, was commonly used and is consistent with prior research on their utility in reducing compulsive sexual behavior and co-occurring affective symptoms.15, 16
Psychotherapy was more frequently recommended for younger individuals. This trend may reflect clinicians’ efforts to promote greater cognitive flexibility in younger adults and avoid medication use unless necessary. Approaches such as CBT and MI have empirical support for addressing behavioral addictions, especially in addressing cognitive distortions and emotion regulation.17, 18
The binary logistic regression revealed that receiving psychotherapy was a significant predictor of higher severity (OR = 1.49, p = .024), possibly reflecting the clinical intuition that more severe cases require behavioral restructuring. However, the direction of causality remains unclear due to the cross-sectional design.
The presence of sexual dysfunction (e.g., erectile dysfunction, premature ejaculation, and low libido) was a significant predictor of higher severity of CSBD (OR = 1.74, p = .01). This aligns with previous literature suggesting that problematic pornography use may contribute to sexual dissatisfaction and performance issues, possibly via altered arousal patterns and unrealistic expectations.2, 3
Notably, 70.8% had attempted intercourse successfully, yet many still reported distress—indicating that functional capacity does not negate subjective impairment, a critical distinction in psychiatric evaluation. Being single also significantly predicted higher severity (OR = 1.96, p = .01), suggesting that lack of partnered sexual intimacy may both contribute to and result from compulsive pornography use.5, 11
Only 14% of participants had previously sought help, and 7% had self-medicated, underscoring the cultural stigma and lack of sexual health literacy in India.6, 7 Despite increasing digital exposure, India continues to struggle with open discourse around sexual behavior. This societal discomfort may delay help-seeking and exacerbate distress when individuals are eventually forced to confront their symptoms in a clinical setting.
While global definitions, such as those in the ICD-11, provide a valuable framework, their application in India must be culturally contextualized.1,13,14 The clinical impression of severity, while methodically applied, was not validated with standardized tools, limiting comparability across settings.
Early identification of problematic use among younger individuals is critical. Primary care and university health systems should be empowered to provide early psychoeducation and brief interventions to support individuals who need them. Early psychoeducation about digital sexual behavior, compulsive pornography use, and healthy coping mechanisms should be integrated into youth mental health programs. Psychiatric comorbidity and sexual dysfunction should be screened routinely in CSBD evaluations to tailor treatment better. Interdisciplinary treatment approaches (sexologists, psychologists, and psychiatrists) are likely to yield the most effective outcomes in complex cases.
This study’s retrospective, cross-sectional design limits causal inferences. The reliance on clinician-assessed severity without standardized tools may introduce subjective variability, although the use of ICD-11 criteria adds clinical robustness. The overwhelming male representation restricts gender comparisons. Final, the weak correlations found, though statistically significant, require cautious clinical interpretation and replication in longitudinal studies.
Conclusions
This study underscores how age, relationship status, and socio-cultural context shape both the manifestation and treatment of pornography-related concerns in India. These findings suggest that younger, single individuals may face distinct challenges, requiring targeted and culturally sensitive intervention strategies. The reliance on psychotherapy among this subgroup also points to evolving treatment preferences in modern clinical practice.
This study should be interpreted in light of certain methodological constraints. Its retrospective design limits the ability to infer causality. Assessments of severity and co-morbid sexual dysfunctions were based on clinical judgment rather than standardized psychometric tools, which may introduce variability. The sample was overwhelmingly male, reflecting treatment-seeking patterns but limiting the scope for gender-based analysis. Additionally, the absence of follow-up data restricts conclusions about long-term outcomes or the progression of pornography-related concerns over time.
Future research should incorporate prospective designs, validated assessment instruments, and more diverse populations to enhance the understanding of the phenomenon. Investigating longitudinal patterns, digital media influences, and co-morbid psychiatric conditions will also be essential in developing comprehensive public health responses to pornography addiction.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Ms. Anoush Gomes, Ms. Shreya Lahoty, Ms. Artika Singh, Mr. Pranay Jivrajka, Ms. Sharanya Menon, Mr. Vijay Mohan, Mr. Shubham Dalvi, and Mr. Abhiraj Amish.
Availability of Data and Material
Yes.
Code Availability (Software Application or Custom Code)
Not Applicable.
Data Sharing Statements
The de-identified individual participant data (including data dictionaries) will be made available upon request. Furthermore, study protocols and the statistical analysis plan can also be provided if required by the reviewers.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
This manuscript was prepared with the assistance of ChatGPT for language refinement and clarity enhancement. The authors take full responsibility for the accuracy and integrity of the content, including all sections influenced by AI-generated outputs.
Ethics Committee
Center: Father Muller Institutional Ethics Committee (FMIEC)
Protocol No: 908/2024.
IEC approval number: FMIEC/CCM/005/2025
Approval date: 02.01.2025
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Prior Presentations
Not Applicable.
Simultaneous Submission to Another Journal or Resource
Not Applicable.
Study Centers
A study was conducted at all the offline clinics of Allo Health and online consultation pan-India.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.