
Abstract
Trichotillomania (TTM), or hair-pulling disorder, is a chronic psychiatric condition characterized by recurrent, irresistible urges to pull out one’s hair, resulting in noticeable hair loss and psychosocial dysfunction. Classified under Obsessive-Compulsive and Related Disorders (OCRDs) in diagnostic and statistical manual of mental disorders (DSM)-5, 1 TTM often begins in adolescence and follows a relapsing course, contributing to distress, shame, and impaired quality of life. 2
Dysfunctions in cortico-striatal-thalamo-cortical (CSTC) circuits, along with neurotransmitter imbalances involving serotonin, dopamine, and glutamate, underlie its pathophysiology.3–5 Behavioral therapies, particularly habit reversal training (HRT), are first-line treatments,6,7 but accessibility is limited in low-resource settings. Pharmacological options such as selective serotonin reuptake inhibitors (SSRIs) and N-acetylcysteine (NAC) offer partial benefit, especially in cases with co-morbid impulsivity or affective dysregulation. 8
Endoxifen, a selective estrogen receptor modulator and protein kinase C (PKC) inhibitor, 9 has demonstrated early efficacy in impulsivity-spectrum conditions such as bipolar disorder and aggression.10–11 Its mechanism offers theoretical promise for treating TTM by targeting emotional and behavioral dysregulation.
We present a case series of 5 individuals with treatment-resistant TTM who received adjunctive endoxifen and were monitored over 12 weeks for changes in symptom severity and quality of life. Written informed consent was obtained from all participants.
Despite increasing recognition of impulsivity in the pathophysiology of TTM, pharmacological interventions targeting this domain remain underexplored. To date, most research has focused on serotonergic or glutamatergic agents, with limited success in treatment-resistant cases. Our case series is the first in the published literature to explore the clinical utility of endoxifen, a PKC inhibitor, in this population. By addressing affective impulsivity—a core but under-targeted dimension of TTM—our study offers a novel, mechanism-based pharmacological approach that complements existing therapies. Furthermore, the use of both symptom severity and quality of life measures provides a more holistic understanding of treatment outcomes, particularly in real-world settings with limited access to specialized behavioral therapy. This report fills an essential gap in the Indian clinical literature and sets the stage for larger, controlled trials exploring endoxifen in OCRDs.
Case Descriptions
Five patients (3 females, 2 males; aged 18–30 years) were assessed and treated at the psychiatry out-patient department (OPD) of a private tertiary healthcare center from Eastern India, between January and April 2025. All were diagnosed with TTM according to DSM-5 criteria by a licensed psychiatrist. The average illness duration across patients was 4.4 years. All had previously undergone at least 12 weeks of treatment with SSRIs, with or without NAC, and had also received HRT.
Psychosocial interventions were delivered by licensed clinical psychologists trained in cognitive-behavioral therapies. These included HRT as the core intervention, comprising awareness training, competing response training, and stimulus control techniques. Additionally, emotion regulation strategies, stress management, and motivational enhancement components were integrated based on the individual patient’s needs. Psychoeducation about the nature of TTM, relapse prevention, and caregiver guidance (where applicable) was also provided. Each patient received 6–8 structured sessions over 6–10 weeks before the introduction of endoxifen.
Due to persistent symptoms despite these interventions, endoxifen was initiated at a dose of 8 mg/day as adjunctive therapy. All SSRIs were continued at stable doses. The Massachusetts General Hospital Hair-pulling Scale (MGH-HPS) 12 and the World Health Organization Quality of Life-BREF (WHOQOL-BREF) 13 were administered at baseline and at 12 weeks to measure symptom severity and functional outcome, respectively.
Symptom severity was assessed using the MGH-HPS, a 7-item self-report measure specifically designed to evaluate hair-pulling behaviors over the preceding week. It captures the frequency and intensity of urges, perceived control, and associated distress. The MGH-HPS has demonstrated good internal consistency (Cronbach’s alpha = 0.89) and test-retest reliability, and is widely used in clinical research for TTM. 12
Functional outcomes were evaluated using the WHOQOL-BREF. This 26-item tool measures quality of life across four domains—physical health, psychological well-being, social relationships, and environment. It has excellent psychometric properties with demonstrated cross-cultural reliability and validity. 13
Both instruments were administered in English, as all participants were fluent and literate in the language. Formal permission was obtained from the original authors for the use of the MGH-HPS in this study. Informed consent was obtained from all patients who are reported here.
Case 1
A 21-year-old single female, an undergraduate student from an urban background, with a 3-year history of TTM involving scalp hair, reported persistent urges despite fluoxetine (40 mg/day) and HRT. Her MGH-HPS baseline score was 18, indicating moderate severity. Initial treatment with escitalopram (up to 20 mg/day) had been tried for 12 weeks a year prior, but was discontinued due to minimal benefit. She had also undergone 6 sessions of HRT, including awareness training and competing response training, but continued to report hair-pulling triggered by academic stress. NAC was not used. Due to continued symptom severity and functional impairment, Endoxifen was introduced as adjunctive therapy. After initiating endoxifen, she noted better emotional control and reduced frequency of urges. MGH-HPS scores declined over 12 weeks, and improvements were noted in WHOQOL-BREF psychological and social domains. At last follow-up (14 weeks), she remained clinically stable and continued endoxifen with no reported side effects.
Case 2
A 24-year-old unmarried male IT professional from a semi-urban background had a 5-year illness duration with severe eyebrow and beard pulling, partially responsive to sertraline (100 mg/day) and NAC. Co-morbid borderline personality traits were identified. His MGH-HPS baseline score was 22, reflecting high severity. He had been treated with sertraline (up to 100 mg/day) for 6 months and NAC (1200 mg/day) for 8 weeks. Minimal improvement led to the discontinuation of NAC. He had a prior 3-month trial of fluvoxamine (up to 150 mg/day), which was stopped due to sedation and poor compliance. Eight sessions of HRT were completed, but he continued to struggle with impulse control, especially during emotional stress. Due to partial response and co-morbid borderline traits, endoxifen was considered as an augmenting agent. With endoxifen, he exhibited a marked reduction in impulsive pulling episodes and better interpersonal regulation. He reported being “less emotionally reactive,” with significant improvement in quality of life. At 16-week follow-up, he reported continued benefit and remained on endoxifen. He experienced transient morning-time nausea during the first 2 weeks, which resolved with proton pump inhibitors.
Case 3
A 30-year-old married female homemaker from a lower-middle socioeconomic background reported a 7-year history of compulsive pulling from the scalp and arms. The MGH-HPS baseline score was 20. She had previously received escitalopram (20 mg/day) for 4 months and olanzapine (2.5–5 mg/day) for 3 weeks, but discontinued the latter due to excessive sedation and weight gain. NAC had been used briefly (up to 1800 mg/day for 6 weeks) with minimal improvement. She completed 6 sessions of HRT and 3 sessions of individual cognitive behavioral therapy (CBT) over a year, but remained symptomatic, with worsening during family-related stress. Based on chronicity and resistance to conventional agents, endoxifen was added to her regimen. Endoxifen led to reductions in MGH-HPS scores by week 4, sustained through week 12. She described being “able to delay the urge,” and WHOQOL-BREF showed gains in the psychological and environmental domains. At 15 weeks, she remained asymptomatic and continued endoxifen. She reported mild fatigue during evening hours and insomnia in week 3, which resolved with melatonin 5 mg at bedtime and sleep hygiene.
Case 4
An 18-year-old single male undergraduate student residing in a hostel presented with a 2-year history of TTM and co-morbid emotional instability, marked by hair-pulling during interpersonal conflict. His baseline MGH-HPS score was 19. He was initially treated with fluoxetine (20 mg/day), titrated to 40 mg/day over 10 weeks, but remained symptomatic. He had no trials of NAC. Six structured HRT sessions focused on response prevention were conducted, but gains were transient. Due to emotional reactivity and poor frustration tolerance, endoxifen was initiated as an adjunct to fluoxetine. After starting endoxifen, he experienced substantial behavioral regulation and reported “feeling calmer” in social situations. MGH-HPS and WHOQOL-BREF both reflected clinical improvement. At week 20 follow-up, he continued to show improvement and maintained endoxifen therapy without any reported side effects.
Case 5
A 27-year-old unmarried female nurse from an urban background with rotating night shifts had recurrent pulling of eyebrow and scalp hair for 5 years, unresponsive to fluoxetine (60 mg/day) and NAC. Baseline MGH-HPS was 21. She had been treated with fluoxetine (60 mg/day) for over 16 weeks and NAC (up to 1800 mg/day) for 2 months. Both were continued during her trial with endoxifen. She had received prior low-intensity CBT and had practiced relaxation techniques, but pulling episodes intensified during night shifts. Given persistent urges, emotional dysregulation, and occupational impairment, endoxifen was added to address residual impulsivity. Adjunctive endoxifen resulted in fewer episodes and improved emotional regulation. She noted, “I was not reacting the same way emotionally,” and showed increased satisfaction in social relationships and occupational functioning. At her most recent follow-up (17 weeks), she had discontinued endoxifen 2 weeks earlier due to financial constraints but remained relapse-free. Mild nausea was reported throughout the treatment.
Summary of the clinical profile, treatment details, and improvement are provided in Table 1.
Clinical and Treatment Profile of Patients Treated with Endoxifen.
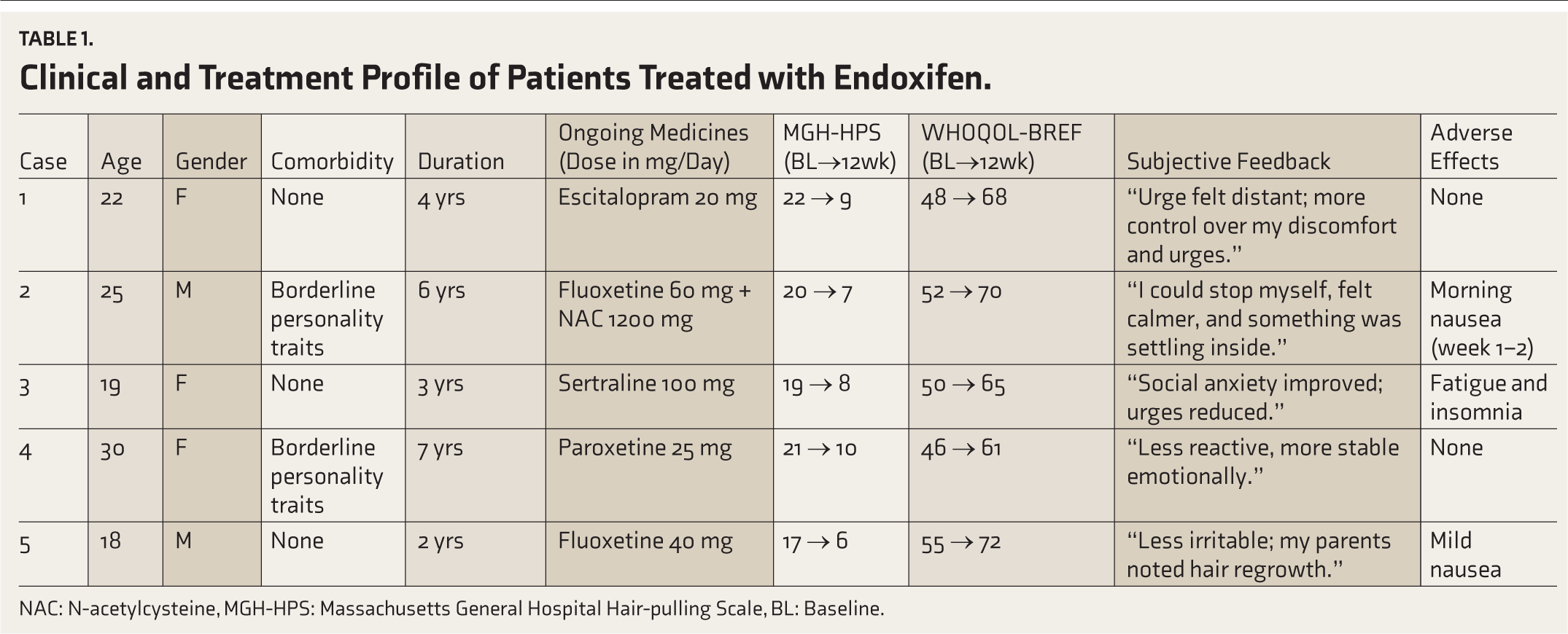
NAC: N-acetylcysteine, MGH-HPS: Massachusetts General Hospital Hair-pulling Scale, BL: Baseline.
Reason for Choosing Endoxifen and Treatment/Response Details
Given the chronicity of symptoms and poor response to standard treatments across all 5 cases, the decision to initiate endoxifen was guided by its emerging evidence in impulsivity-spectrum conditions and its potential to address emotional dysregulation in TTM.
All patients received endoxifen at a fixed dose of 8 mg/day, initiated without titration, and administered orally once daily after breakfast. The treatment duration for all cases was 12 weeks. Patients were monitored fortnightly in the outpatient setting for clinical improvement and tolerability. Medication compliance was monitored through fortnightly in-person follow-up visits and corroborated by caregiver feedback where feasible. Side effects were assessed using structured clinical interviews, and no significant adverse impact or derangement of laboratory parameters was observed during the treatment period. Symptom response was quantified using the MGH-HPS, which showed a 35%–55% reduction across cases at week 12, along with consistent improvement in WHOQOL-BREF psychological and social domains (Table 1), indicating both symptomatic and functional gains.
Discussion
TTM, although categorized under OCRDs, occupies a complex nosological space involving both compulsive and impulsive elements. This duality is reflected in its clinical phenomenology and underlying neurobiology. Patients often describe mounting inner tension or distress followed by the act of hair-pulling, which brings temporary relief, and demonstrates a typical cycle of negative reinforcement. 4 This cyclical behavior pattern is both habit-forming and emotionally driven, suggesting that dysregulation in both cognitive control and affect modulation plays a central role in pathogenesis.5,7
From a neurobiological standpoint, the CSTC circuits have been most consistently implicated in the pathophysiology of TTM. These loops, which are also disrupted in obsessive-compulsive disorder, are critical for motor inhibition, decision-making, and affect regulation.4,14 Within these circuits, dysregulation in the orbitofrontal cortex and anterior cingulate cortex leads to impaired top-down control over habitual and affect-driven motor outputs. Furthermore, the basal ganglia—particularly the striatum—are involved in procedural learning and behavioral sequencing, both of which are aberrant in patients with TTM. 4
Neurochemical abnormalities have also been described. These include serotonin (5-HT) dysregulation, which contributes to compulsivity; dopamine dysregulation, particularly in the mesolimbic pathway and associated with reward anticipation and impulsivity; and glutamate dysfunction in CSTC circuits.4,6 This pathophysiologic mosaic complicates pharmacological targeting and partially explains the suboptimal efficacy of monoaminergic agents such as SSRIs, which were initially extrapolated from obsessive compulsive disorder (OCD) models.6,7 In this context, our case series—where 5 individuals with persistent TTM showed significant improvement after the addition of endoxifen—invites re-examination of the disorder through the lens of impulsivity and emotion-driven behavioral dysregulation.
Endoxifen is a potent active metabolite of tamoxifen with dual pharmacologic properties, namely selective estrogen receptor modulation (SERM) and PKC inhibition.9,10 The SERM properties of endoxifen may contribute to neuroprotection and mood stabilization, particularly in hormonally sensitive circuits. 11 However, its role as a PKC inhibitor is of greater relevance to disorders characterized by emotional dysregulation and impulsivity. PKC is a family of enzymes that modulate synaptic plasticity, neurotransmitter release, intracellular signaling, and gene expression. 15 Elevated PKC activity has been observed in conditions such as bipolar disorder, aggression-spectrum disorders, and in preclinical models of affective lability.11,15
By inhibiting PKC, endoxifen exerts a stabilizing influence on intracellular signaling in neural pathways associated with emotional arousal and behavioral regulation. Prefrontal-limbic circuits, particularly the interaction between the prefrontal cortex and amygdala, are modulated by PKC-dependent phosphorylation cascades. 16 Inhibiting this pathway has been associated with reduced emotional reactivity, better affective regulation, and improved response inhibition—all of which are relevant to the pathophysiology of TTM.6,17
In our case series, the introduction of endoxifen resulted in not only quantitative improvements in hair-pulling severity, as evidenced by lower MGH-HPS scores, but also in subjective enhancements in emotional control and delay of gratification. These findings are consonant with the proposed mechanisms of action of PKC inhibitors. 15 For instance, patients who previously described hair-pulling as an “automatic” or “unstoppable” response to stress reported a newfound ability to “pause” or “choose differently” following endoxifen initiation. This suggests improved inhibitory control, possibly via enhanced prefrontal cortex modulation.
Furthermore, the broader psychosocial improvements reflected in WHOQOL-BREF scores—particularly in psychological and social domains—reinforce the clinical significance of this pharmacologic effect. Quality of life, though not always captured in symptom-centric assessments, is an essential outcome measure in chronic disorders such as TTM, where social stigma, low self-worth, and interpersonal difficulties are common. 18 Improvements in social engagement and interpersonal regulation in our series—particularly among patients with borderline personality traits—highlight the potential of endoxifen to address the affective-interpersonal dimensions of TTM, which are often overlooked in standard therapy.
Interestingly, 2 of our cases had co-morbid borderline personality traits, characterized by marked impulsivity, affective lability, and identity diffusion. These individuals not only responded well to endoxifen in terms of reduced hair-pulling, but also reported reduced interpersonal reactivity, fewer emotional outbursts, and better stress coping. This is significant because PKC inhibition has previously demonstrated mood-stabilizing effects in bipolar mania and aggression-spectrum disorders.11,19 Endoxifen’s impact on emotional reactivity may thus extend beyond the motor act of hair-pulling to the broader domain of behavioral regulation.
It is also worth noting that the onset of clinical benefit occurred relatively early (within 4–6 weeks) and was sustained over the 12 weeks. This aligns with previous findings from trials in bipolar disorder and supports the neurobiological plausibility of endoxifen’s role in modulating rapid signal transduction mechanisms involved in mood and behavioral regulation.11,20
Side effects were minimal, and no patients discontinued the medication. This is consistent with the safety profile reported in prior studies of endoxifen in psychiatric populations.9,10,20
This case series provides preliminary yet valuable clinical insights into the use of endoxifen for treating TTM that is resistant to other treatments. One of the key strengths lies in its mechanism-based pharmacological rationale, targeting affective impulsivity through PKC inhibition—a pathway not commonly addressed in current TTM treatment protocols. The use of validated tools, such as the MGH-HPS for symptom severity and the WHOQOL-BREF for quality of life assessment, enabled a more comprehensive evaluation of outcomes, extending beyond symptom control to encompass overall psychosocial functioning.
However, despite these promising results, several limitations must be acknowledged. The small sample size limits the generalizability of findings. The open-label design introduces the possibility of expectancy effects and observer bias. Although validated scales were used, the reliance on self-reported measures remains a methodological limitation and may have introduced subjective bias. Furthermore, the study lacked neurocognitive assessments (e.g., response inhibition tasks, delay discounting paradigms) and neuroimaging tools, which could have provided more objective markers of improvement and neurobiological correlates of treatment response. Additionally, the 12-week follow-up period, while sufficient for observing the initial response, is inadequate for determining long-term efficacy or preventing relapse.
Conclusion
To our knowledge, this case series is the first in published literature to examine the adjunctive use of endoxifen in TTM. Endoxifen at 8 mg/day was linked with significant improvements in hair-pulling severity and functional quality of life, particularly among individuals with prior treatment resistance. Its dual mechanism of estrogen receptor modulation and PKC inhibition offers a promising neurobiological rationale for its application in impulse control and affect regulation disorders.
Given the high burden and often refractory nature of TTM, these preliminary findings encourage the exploration of endoxifen in larger, controlled studies. Moreover, this report highlights the importance of consultation-liaison psychiatry in integrating novel phar-macological options within multidisciplinary care frameworks for OCRDs. Comprehensive management, especially in resistant cases, demands collaboration between psychiatrists, psychologists, pharmacologists, and primary care physicians. A neurobiologically informed, personalized treatment approach may offer patients with TTM renewed hope and recovery trajectories.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We acknowledge all the participants of the study and their family members.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Statement
Informed consent was obtained from all participants. The study adhered to the CARE guidelines for clinical case reporting.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Prior Presentations
None.
Simultaneous Submission to Another Journal or Resource
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.