
Abstract
Background:
In India, an estimated 3.5 million are affected with schizophrenia, of which more than two-thirds belong to the rural demography. Schizophrenia is one of the most disabling illnesses, causing 10% of the disability adjusted life years, making it a public health concern. We aimed to estimate the treatment gap for schizophrenia in a rural South Indian setting following a community intervention program implemented in two administrative blocks (Thirthahalli and Turuvekere) in the state of Karnataka, India.
Methods:
Population-based screening was conducted by trained Accredited Social Health Activists (ASHAs) to identify persons with symptoms of schizophrenia. Research social workers and psychiatrists interviewed screen-positives to confirm the diagnosis. Prevalent cases were enumerated by adding those already registered under the program to those newly identified through house-to-house screening. The treatment gap was calculated by subtracting the “target population” from those who had received psychiatric treatment at least once.
Results:
In Thirthahalli, of 364 patients, 14 had not received any treatment, indicating a treatment gap of 3.84%. In Turuvekere, out of 236 cases, 29 had not received treatment, indicating a treatment gap of 12.28%. Overall, the treatment gap in both administrative blocks was 7.16%.
Conclusion:
Meaningful reduction of treatment gap for schizophrenia is a feasible target at sub-district levels. Policies commensurate with this aim should be considered
This study aimed to document a low treatment gap for schizophrenia in the rural part of India following a local community-based intervention program. It has utilized fairly rigorous and robust methods of case-finding and thereby estimated a low treatment gap of 7.16% compared to the national estimate. The authors conclude that task shifting/sharing approaches at the grassroots level can substantially reduce the treatment gap for severe mental disorders.Key Messages:
Schizophrenia is one of the most disabling medical disorders, contributing 10% of disability adjusted life years. 1 Though its prevalence is less than 1%, the fact that 3.5 million people are affected in India makes it an important public health concern. This is because of its various adverse social, health, and economic consequences. 2 The social impact is due to its association with poverty, which includes barriers in gaining employment, housing, accessing education, or even health care services, and homelessness. 2 Health impact is a higher incidence of co-morbid physical illnesses, as schizophrenia is usually chronic, relapsing, and remitting, with symptoms that cause a sedentary lifestyle. 3 Lastly, the economic burden includes direct, indirect medical costs, and other indirect costs.4,5 Having said this, early identification and close follow-up for monitoring treatment adherence have demonstrated satisfactory outcomes in their functioning using established community intervention models. 6 In India, the treatment gap for schizophrenia and other psychotic disorders is 75.5% as per the National Mental Health Survey (NMHS) 2015–2016. Of the 3.5 million affected, more than two-thirds belong to rural areas, necessitating a commensurate response from the health care system. 7 The survey investigators recommended strengthening the existing District Mental Health Program (DMHP) by going beyond district hospitals and integrating mental health services into sub-district and Primary Health Centers (PHCs). As mentioned earlier, established community models are present for schizophrenia, ranging from specialist, collaborative care (collaboration between psychiatrists and trained but non-specialist health workers) and task shifting/sharing models.8–12 They have demonstrated comprehensive treatment coverage by addressing morbidity, functioning, and recovery at the administrative block-level. The authors’ experience influenced policymakers in piloting the Taluk Mental Health Program (TMHP). 13 Being an extension of the DMHP, TMHP aims to reduce the treatment gap using task shifting/sharing approaches by involving the community and primary care providers. In this manner, mental health integration is achieved at all levels, aiding stigma alleviation with an increase in mental health literacy among non-mental health care providers and the community. The treatment gap has emerged as an indicator of service provision and is a popular measure for guiding planning and policy-making. Different research groups have documented the effective implementation of community mental health programs, highlighting the impact on common mental disorders, including substance use disorders.14,15 In this study, the authors present the impact of a community intervention program that demonstrated a low treatment gap for schizophrenia in two rural administrative blocks (taluks) of Karnataka State, South India: Thirthahalli and Turuvekere.
Hypothesis
The authors hypothesized that a rural community intervention program in a low-resource setting would result in a low treatment gap for schizophrenia.
Aim
To estimate the treatment gap for schizophrenia in a rural South Indian setting following a community intervention program implemented in two administrative blocks (Thirthahalli and Turuvekere) in the state of Karnataka, India.
Methods
Ethical Consideration
The Institutional Ethics Committee approved the study.
Study Design
The study is a descriptive cross-sectional study to estimate the treatment gap of schizophrenia by ascertaining the treatment status of persons with schizophrenia (PWS) living in two administrative blocks in Karnataka, India. To assess the treatment gap, the authors measured the total number of PWS (target population), the number of treated (referred to as “ever treated” from now on), and the number of untreated (referred to as “never treated” from now on) persons among them. They then final arrived at the treatment gap as per the equations below
16
:
Cases were identified using survey methods and data on their treatment status. The authors defined “ever treated” as those with a history of having consulted an allopathic psychiatrist (with a Diploma in Psychological Medicine [DPM]/Doctor of Medicine [MD]/Diplomate in National Board [DNB] degree) at least once in their lifetime for schizophrenia. Those who never consulted an allopathic psychiatrist even once or consulted other systems of medicine or faith healers were considered “never treated.”
Study Settings
Thirthahalli taluk, in Shivamogga district in the Midwest Karnataka, has a population of 1,42,006. 17 Turuvekere is located in the Tumakuru district of Southern Karnataka, India. Turuvekere has a population of 1,68,994. 18 Participant recruitment and data collection were conducted between July 2018 and February 2019.
Eligibility Criteria
PWS were interviewed if they had the diagnosis of schizophrenia and related disorders, which included unspecified non-organic psychosis and schizoaffective disorder (collectively referred to as schizophrenia in this article). The details of how they were identified are elaborated under “Sources and Methods of Selection of Participants.” Written informed consent was obtained from all subjects. Persons who did not consent to the study were excluded.
Sources and Methods of Selection of Participants
At the time of writing this manuscript, 380 patients in Thirthahalli and 260 in Turuvekere were already registered as PWS cases who were identified, treated, and followed up by a team including the authors, as a part of their affiliated institution-run community intervention programs at both these administrative blocks from 2005 and 2009, respectively. More details about these cohorts can be found elsewhere.12,19–22 In short, the community intervention program is run by collaborating with local health administrations, including the nearest PHC (in Thirthahalli) and the administrative block hospital (in Turuvekere), where patients are regularly attended to. Case identification was with the help of trained community health workers (CHWs), the key-informant method, and snowballing techniques. After confirmation of the diagnosis (by psychiatrists), psychopharmacotherapy and basic psychoeducation were provided. The dosage and choice of medications were determined by the psychiatrists’ clinical judgment. Patients are then regularly followed up. For those who drop out, the team reaches out to them by phone or through periodic house visits. Not all patients wish to be followed up with our team. Such families continue their care with clinicians of their choice, but the team conducts periodic assessments. Psychosocial interventions include education about the illness, addressing barriers to continuity of care, guidance on obtaining disability certificates, and vocational counseling.11,12,22,23
Thus, the existing cohort formed part of the required target population to be estimated in the current study. For measuring the rest of the target population and thereby the treatment gap, we used the following method. 16
Total number of PWS (target population):
This was calculated as the sum of persons already identified and treated in the cohort, plus those living in these administrative blocks who were not part of the cohort. Two rounds of house-to-house surveys were conducted to identify PWS who were not part of the cohort.
First, all households in both taluks were screened by Accredited Social Health Activists (ASHAs). ASHAs are women CHWs in the Indian public healthcare system who reside in the communities they serve. A total of 326 ASHAs (160 and 166 in Thirthahalli and Turuvekere, respectively) were trained for half a day in administering a screening tool named “Symptoms-in-Others (SIO).”24,25 It has 15 questions and takes no more than two minutes to administer per household. Apart from psychoses, the SIO tool contains questions targeting epilepsy, substance use problems, and intellectual disability disorders as well. During her customary visits to each house, each ASHA interviewed one responsible adult (usually the head of the household) using this tool. In addition, they were provided an honorarium for this purpose. They referred screened positive cases to the research social workers. In total, 26,823 and 42,761 households were screened in Thirthahalli and Turuvekere, respectively, between July 2018 and February 2019. Research social workers interviewed them subsequently to rule out other diagnostic possibilities. They referred individuals with features of psychosis to research psychiatrists for a clinical diagnostic interview at PHCs (Thirthahalli) and the administrative block hospital (Turuvekere). This phase was carried out after the completion of the ASHA survey, conducted between February 2019 and October 2020, in both administrative blocks. Persons who had died, migrated, overlapped with the existing cohort, or had a change in diagnosis during the research psychiatrist’s confirmation of diagnosis were excluded from the study.
Second, to estimate the number of cases that ASHAs may have missed, research social workers conducted a house-to-house survey of a random 10% of households. Hitherto unidentified individuals with features of schizophrenia were interviewed by psychiatrists to confirm the diagnosis. This was also carried out in a similar manner and on a similar timeline to the first survey. This case-finding method has been used in an earlier study. 22 The number of individuals with psychosis identified freshly during this visit was multiplied by a factor of 10 to estimate the total number of missed cases. Persons who had died, migrated, overlapped with the existing cohort, or had a change in diagnosis during the research psychiatrist’s confirmation of diagnosis were excluded from the study.
The number of PWS in the already existing cohort, plus the number estimated by two screening rounds, formed the “target population” to estimate the treatment gap.
We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline to draft this manuscript and the STROBE reporting checklist during editing, which are included in Supplement A.26,27
Results
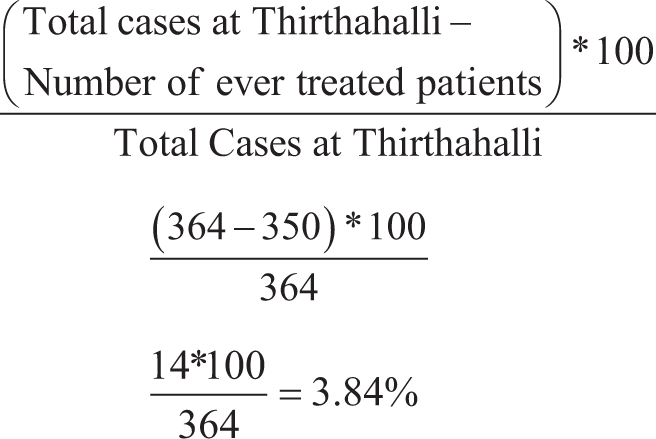
In Thirthahalli (Figure 1), the 380 cases from the existing cohort over the past decade were first reviewed for inclusion in the current study. It was found that 120 patients were either dead (55), migrated (45), or had a change in their diagnosis (20) at the time of conducting the current study. Hence, the remaining 260 cohort cases were deemed eligible, as all were receiving psychiatric treatment. Second, (in addition to the eligible cohort cases), 26,823 households were screened by ASHAs between July 2018 and February 2019. A total of 475 members tested positive on the SIO tool. Four hundred forty-one of them were excluded, as 44 of them refused consent, 306 did not meet the criteria for schizophrenia, and 59 were part of the already existing cohort. Also, 18 subjects had lost their lives, and 14 had migrated from the taluk when the research social worker or the psychiatrist attempted to confirm the diagnosis. Thus, 34 cases from the ASHA survey were eligible for inclusion at the time data collection concluded in October 2020. Of these, 30 and 4 were found to be ever treated and never treated, respectively. Final, the 10% survey found 149 patients screening positive; 142 were excluded as three refused consents, 97 did not meet criteria for schizophrenia, 38 were part of an existing cohort, one had died, and three migrated at the time of the interview by psychiatrists. Thus, seven patients were identified as cases, of whom six had ever been treated, and one had never treated. These numbers were extrapolated to 100% by multiplying by 10; estimating cases missed by the ASHAs at 70, of which ever treated at 60, and the untreated at 10. Overall total cases at Thirthahalli were 364 (260 + 34 + 70), of which “ever treated” were 350 (260 + 30 + 60) and “never treated” were 14 (0+4+10). Hence, the treatment gap at Thirthahalli was calculated as follows:
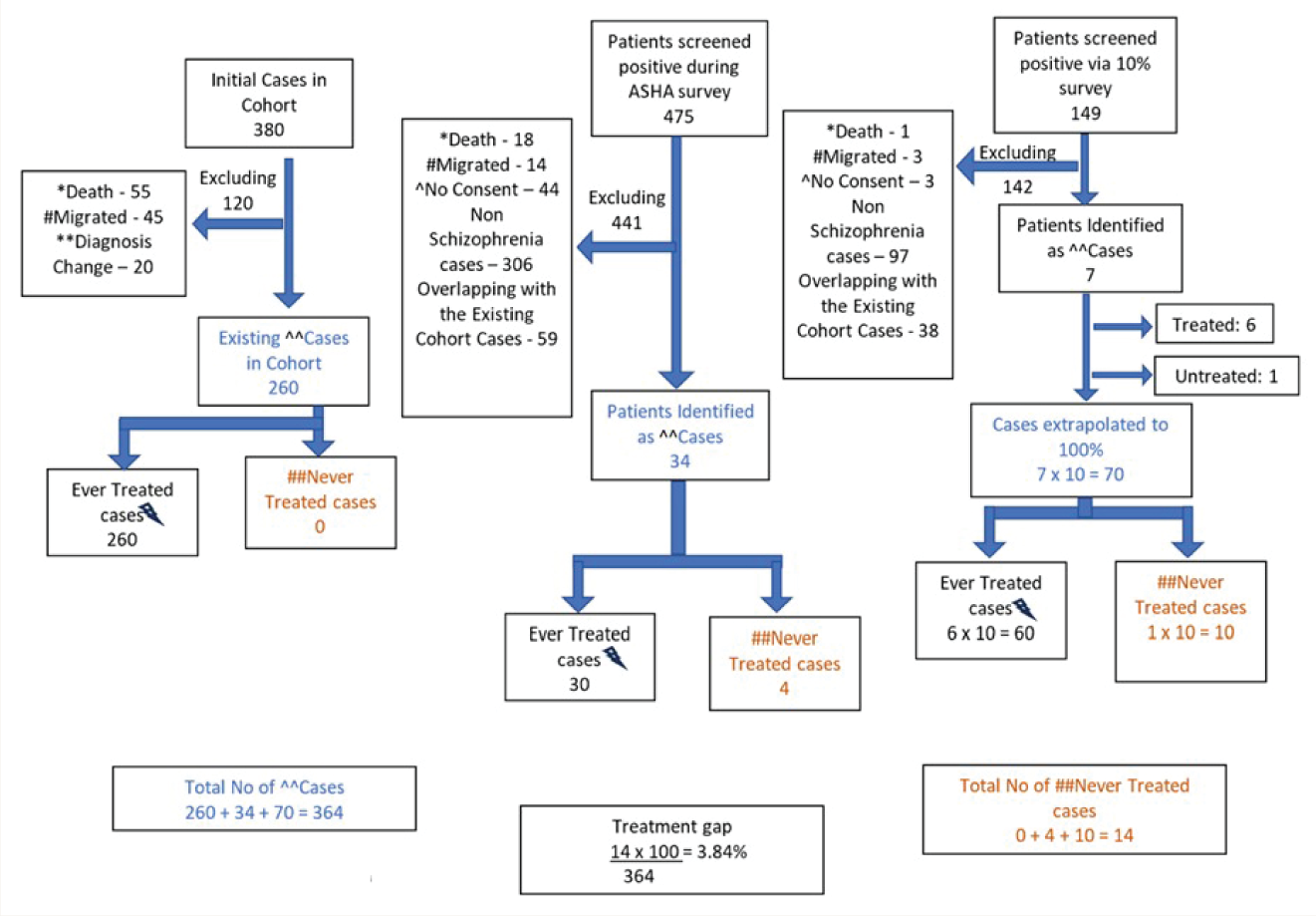
^^Cases denotes Schizophrenia cases after confirmation of diagnosis by research psychiatrist
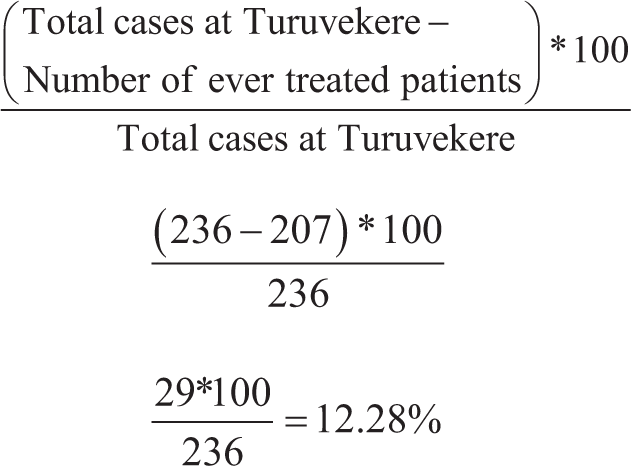
Similarly, in Turuvekere (Figure 2), 260 cases were part of the existing cohort. They were reviewed for the inclusion criteria of the current study. One hundred patients had to be excluded because they were dead (40), had migrated (49), or had a change in their diagnosis (11); hence, the remaining 160 were identified as eligible, all receiving psychiatric treatment. Second, among the 42,761 households screened, 519 subjects tested positive. Four hundred fifty-three were excluded as 59 refused consents, 10 were duplicated subjects by ASHAs, 168 did not meet criteria for schizophrenia, 151 were part of the cohort, 29 had died, and 36 had migrated. Thus, 66 cases of the ASHA survey were eligible, of which 47 were “ever treated” and 19 were “never treated.” From the 10% survey, 41 screened positive; 40 were excluded as they refused consent (seven), did not meet criteria for schizophrenia (18), were part of the cohort (10), or had died (two) or migrated (three) at the time of the interview by psychiatrists. Thus, only one patient was identified as a case who was never treated. Hence, the estimate of the number of cases missed by the ASHAs was 10 untreated patients. Overall, the total cases at Turuvekere were 236 (160 + 66 + 10), of which ever treated include 207 (160 + 47 + 0) and never treated included 29 (0 + 19 + 10). Hence, the treatment gap at Turuvekere was calculated as follows:
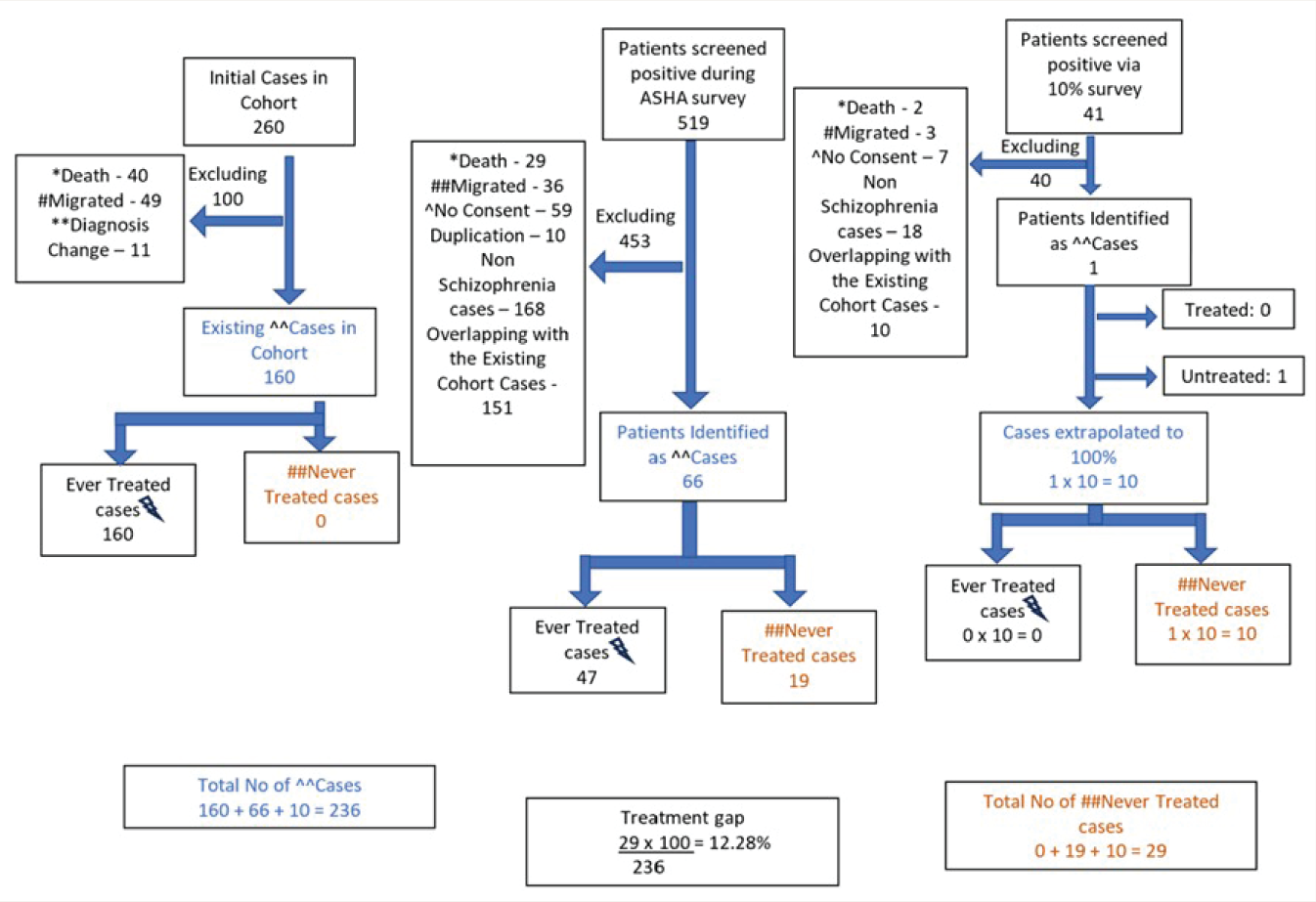
^^Cases denotes Schizophrenia cases after confirmation of diagnosis by research psychiatrist
Final, combining both the administrative blocks (Figure 3), the calculation is performed similarly to derive a total of 600 cases in Thirthahalli and Turuvekere taluks (420 + 100 + 80), of which 557 (420 + 77 + 60) were ever treated, and 43 (0 + 23 + 20) were never treated. Hence, the treatment gap at Thirthahalli and Turuvekere was calculated as follows:
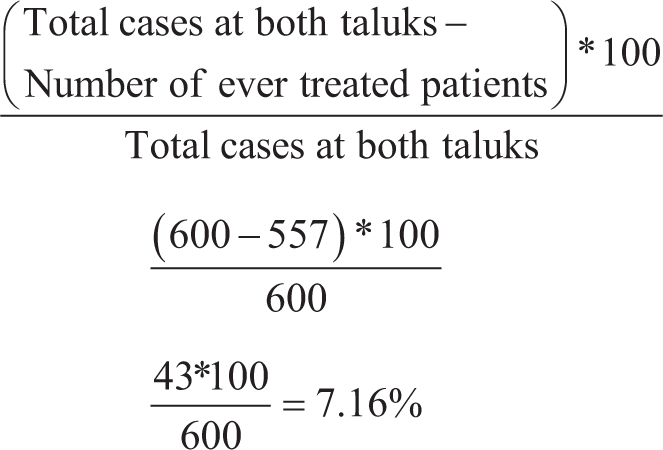
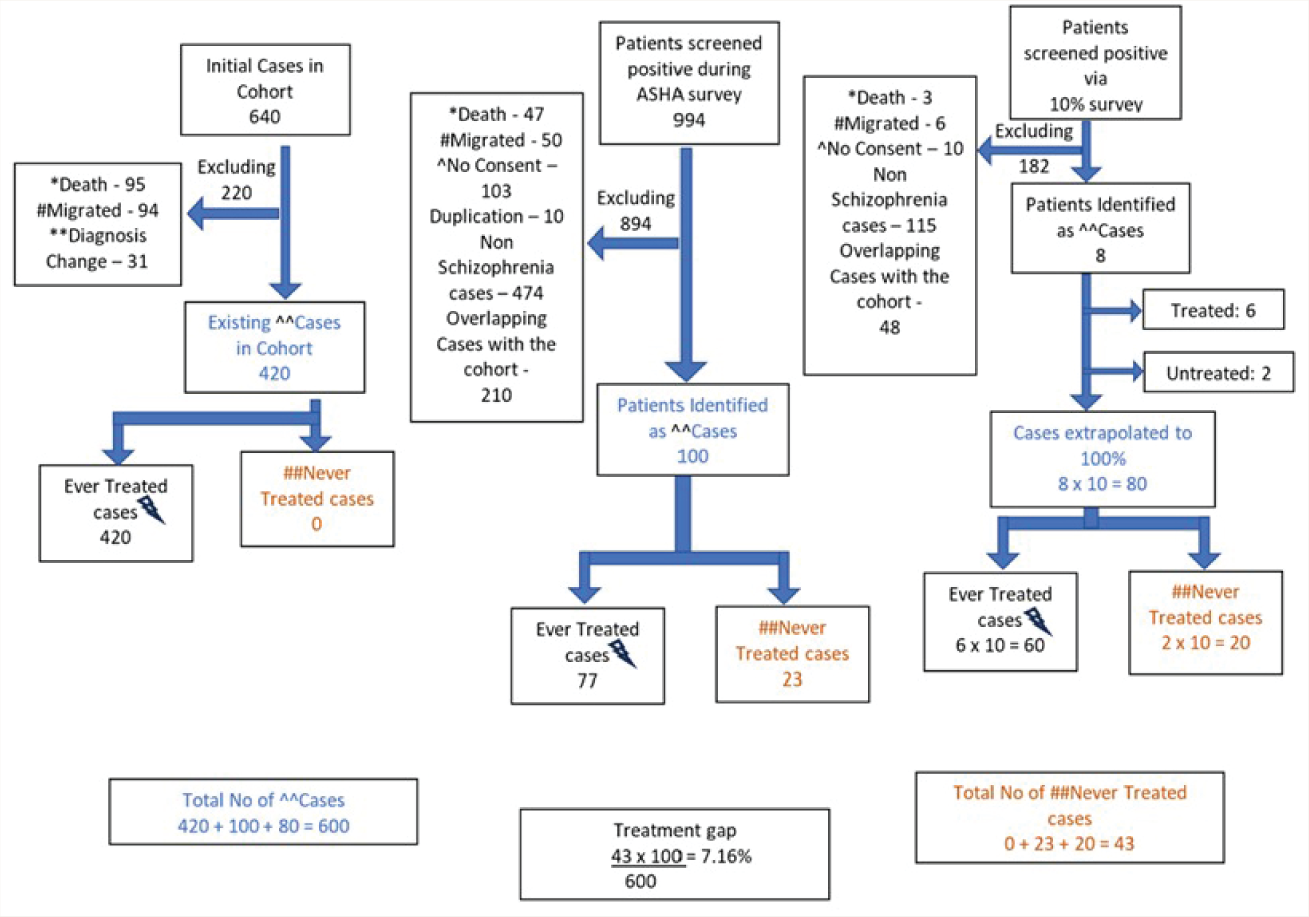
^^Cases denotes Schizophrenia cases after confirmation of diagnosis by research psychiatrist
Thus, to summarize, the treatment gap at Thirthahalli, Turuvekere, and both together was 3.84%, 12.28%, and 7.16%, respectively. We did not report the clinical and demographic details because they were not available for all patients (not collected separately for this study).
Discussion
This study shows that the treatment gap for schizophrenia in the two administrative blocks of South India—Thirthahalli and Turuvekere (of Karnataka state) is lower (7.16%) than the national estimate as per the NMHS 2015–2016 (75.5%). In Thirthahalli, the gap was 58% at the time this cohort was initiated. 22 It reduced to 3.84% over one and a half decades of this intervention program. Studies have demonstrated an increase in treatment-seeking behavior following community intervention programs for various mental health conditions. A cross-sectional study conducted in India and Nepal showed a substantial increase in treatment-seeking behaviour 14 over 12 months following the implementation of a mental health intervention program at PHCs. It was 8.1% in Nepal and 23.5% in India for common mental disorders. As this study was conducted at the PHC level, the possibility of excluding community members exists. Luitel et al. did a similar study comparing baseline and post-intervention contact coverage for depression and alcohol use disorders in Nepal. It found an increase in the treatment-seeking from 8.1% to 11.8% for depression and 5.1% to 10.3% for alcohol use disorders post three years. 15
As of today, the DMHP, the operational arm of the centrally funded National Mental Health Program, is implemented in more than 90% of districts in India (704 as of February 2022), each with a population of roughly two million. 28 Each DMHP consists of one psychiatrist, one psychologist or clinical psychologist, one social worker, or psychiatric social worker, two nurses, and two support staff. Though National Mental Health Program (NMHP) has made psychiatric care available across the country, the evidence for a reduction in the treatment gap by the system is lacking. 29 As it is hard for the relatively small DMHP team to provide care for all individuals who need mental healthcare, the next logical step would be to expand the mental health team to sub-districts or administrative blocks (called taluks). India has about 8,000 administrative blocks, and there is a provision to recruit one medical officer and one social worker exclusively for mental healthcare in each taluk. 30 The current study shows that providing such human resources at this level can substantially bring down the treatment gap, at least for severe mental illnesses. Mere presence of a psychiatrist and a social worker at administrative blocks will enable early diagnosis and medical treatment alongside basic psychoeducation to the family, coordination for regular follow-up visits, and adherence to medications. Ensuring these will reduce the symptoms and improve functioning. These simple measures by themselves reduce stigma and enhance acceptability at the community level. Moreover, the feasibility of ensuring disability benefits and rehabilitation measures can be improved by better alliances and networking with local government bodies for patients with poor outcomes. All these together would further reduce the treatment gap. Furthermore, establishing a provision for the use of digital technology would enable this team to collaborate with primary care doctors and care for patients in need at PHCs as well.31–38 An added advantage is an increase in contact coverage for other psychiatric disorders as well (e.g., common mental disorders and substance use disorders). All these strategies align with the NMHS recommendations for improving the country’s mental health care system.
The reasons why a few patients in the study did not accept treatment and dropped out (i.e., demand-side challenges to the treatment gap) have been explored and documented elsewhere.25,39 The difference in the “gap” between two cohorts can be attributed to differences in service accessibility. While in Thirthahalli, collaborative care is accessible at the nearest primary health center (about 2.5 miles from patients’ houses), in Turuvekere, patients have to visit the administrative block headquarters (which is considerably farther from individuals’ houses). It may be noted that “distance” from the care center is one of the essential reasons for not accessing treatment. 25 Care-at-doorstep models are found to help ensure continuity of care. 40 This should be a part of the TMHP. Last, a cost-effectiveness analysis of this care model is necessary.
Strengths
The study has used fairly rigorous, robust case-finding methods. 22 Initially, ASHAs surveyed all households in both administrative blocks, followed by repeat visits of randomly selected 10% households by social workers, which accounted for missing cases. Subsequently, the presence of schizophrenia was confirmed by qualified psychiatrists. The low treatment gap reported in this article may be due to the community intervention programs that have been successfully running in these two administrative blocks for the past 1.5 decades. 25 It shows what can be achieved if administrative block-level mental health programs are run optimally and highlights the need to initiate such programs elsewhere in the country. Essentially, these community intervention programs consist of regular outpatient services and periodic outreach to those who drop out of the treatment umbrella. One psychiatrist (for regular consultations) and a locally residing non-specialist social worker (for all other psychosocial needs of the patients and logistical aspects of coordinating care) have been serving in each administrative block. This report highlights that “contact coverage” 13 can be improved notably with this approach. We have earlier reported that this approach positively influences several dimensions of schizophrenia, including general and work-related disability and family burden.11,12,19–23,25,41
Limitations
Not using standardized diagnostic tools is a limitation, but qualified psychiatrists evaluated all subjects to confirm the diagnosis. The fact that ASHAs did not identify some patients already existing in the cohort during their survey is another shortcoming. The survey was conducted by interviewing one person in each household. There is a possibility that the respondents might have been unaware that their family member was receiving treatment for a mental illness, particularly if the individual was free of symptoms at the time of the survey. Hence, they might have provided a response of “no” to the question on SIO, “whether any member of your house has received treatment for a mental illness.” However, even if the ASHAs had identified persons with mental illness in these families, it would have been added to the count of “overlapping with the existing cases,” and the count of patients not on treatment would have remained unchanged. A considerable proportion of participants did not consent to take part in the study (103 in the ASHA survey and 10 in the 10% survey). It is possible that some untreated patients in these households were missed, so the treatment gap might be slightly higher than the study estimates.
Conclusions
The study has demonstrated that task shifting/sharing approaches at the grassroots level can substantially reduce the treatment gap for severe mental disorders in low-resource settings. Whether such an approach could reduce the treatment gap for other psychiatric conditions, including common mental disorders, is yet to be explored. Future studies should also examine the cost-effectiveness of this approach.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors would like to acknowledge PWS and their families for having co-operated for the data collection. ASHAs of Thirthahalli and Turuvekere deserve a rich round of applause for their cooperation in the work. The taluk health administration, too, is acknowledged. Authors would also acknowledge several volunteer donors contributing generously toward sustaining the community intervention programs in these two taluks. We also acknowledge the contribution of Chittasanjeevini Charitable Trust, which is contributing free psychotropic medications for patients of both these taluks. Final, Mr Pramodha, a social worker, did contribute parttime for the data collection.
Appropriate Permissions from the Concerned Authorities
N/A.
Data Sharing Statement
Deidentified individual participant data will not be made available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None Used.
Ethics Committee
Name of the Institutional Ethics Committee/Independent Review Board: National Institute of Mental Health and Neurosciences (NIMHANS) Ethics Review Committee. Approval reference number: NIMHANS/EC (BEH.SC.DIV)/11th MEETING/2018. Date of approval: 21 March 2018.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent/Assent
Statement about participant consent (assent from those < 18 years of age and consent from parents or legally authorized representative or guardian) has been obtained and is mentioned in the appropriate section of the main document.
Prior Presentations
The manuscript abstract was presented at the Annual National Conference of the Indian Psychiatric Society 2022 for the “MARFATIA Award.” Hence, the abstract has been published in the Supplement of the Indian Journal of Psychiatry in March 2022, bearing doi:
Simultaneous Submission to Another Journal or Resource
The original manuscript has not been submitted or considered for submission to any other journal.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.