
Abstract
Background:
Child sexual abuse (CSA) has profound psychiatric and developmental consequences; however, the relationship between specific abuse characteristics and mental health outcomes in the Indian context remains insufficiently studied. This study examined psychiatric morbidity, developmental psychopathology, and functional impairment among children with CSA.
Methods:
A cross-sectional study was conducted with 100 children aged 6–17 years whose cases were registered under the Protection of Children from Sexual Offenses (POCSO) Act and referred to a government-supported protection center. Data were collected using a semi-structured interview, the Developmental Psychopathology Checklist (DPCL), DSM-5-TR–based clinical evaluations, and the Children’s Global Assessment Scale (CGAS). Associations between abuse characteristics and psychiatric outcomes were analyzed using χ2 tests and logistic regression.
Results:
The mean age was 10.87 years (SD = 3.22). Perpetrators were known to the child in 66% of cases, and 55% of participants experienced vaginal or anal penetration. Overall psychiatric morbidity was 53% (95% CI: 43.2–62.6). Common diagnoses included post-traumatic stress disorder (28%, 95% CI: 20.0–37.6), conduct disorder (21%, 95% CI: 14.2–30.0), and depression (17%, 95% CI: 10.9–25.5). Suicidality was reported in 12% (95% CI: 6.8–19.8). Vaginal/anal penetration was associated with higher rates of PTSD (χ2 = 8.67, p = .003) and depression (χ2 = 4.15, p = .04). Longer duration of abuse was associated with higher suicidality (χ2 = 6.30, p = .01). More severe physical injury was associated with higher suicidality (χ2 = 6.30, p = .01). Self-blame was associated with higher rates of adjustment disorder (χ2 = 4.98, p = .02). The mean CGAS score was 69.20 (SD = 12.16), reflecting mild-to-moderate functional impairment.
Conclusions:
CSA survivors exhibit substantial psychiatric and functional difficulties, with specific abuse patterns linked to distinct mental health outcomes. Early trauma-focused assessment, caregiver psychoeducation, and timely psychosocial interventions are crucial to improving recovery trajectories.
Question: What psychiatric and developmental outcomes are associated with specific abuse characteristics in legally documented CSA survivors? Findings: Penetration, prolonged abuse, physical injury, and self-blame showed significant associations with PTSD, suicidality, depression, and adjustment disorder. Meaning: Targeted trauma-informed assessment and early intervention are crucial for recovery.Key Messages:
Children under 18 account for 37% of India’s population, symbolizing the nation’s future. 1 This formative stage of life is both crucial and vulnerable, with a significant proportion of children exposed to adverse childhood experiences (ACEs), including various forms of abuse. Globally, the World Health Organization estimates that 150 million girls and 73 million boys under 18 have experienced some form of sexual violence. 2 Studies report that the prevalence of child sexual abuse (CSA) is 8%–10% in males and 18%–20% in females worldwide. 3
In India, every second child is subjected to sexual abuse or violence, with a child abused every 15 minutes, as per the 2016 National Crime Records Bureau (NCRB) report. 4 The reported prevalence of CSA in India ranges from 4% to 66% in females and 4%–57% in males. 5 Variations in estimates may be attributed to methodological differences, including inadequate representation of male CSA in existing definitions. 6 Moreover, non-disclosure rates among children range between 30% and 87%, further complicating accurate prevalence estimates. 7 Certain states, including Andhra Pradesh (before partition), Telangana, Bihar, Assam, and Delhi, report the highest rates of CSA. 8
Underreporting of CSA in India is heavily influenced by conservative cultural norms, which render discussions of sexual abuse taboo. Families often discourage victims from speaking out to avoid societal shame, leading to inadequate support for survivors. Additional barriers include ignorance about what constitutes sexual abuse, fear of stigma, and retribution, which collectively hinder prevention and intervention measures. 9
There is a paucity of research on the socio-cultural factors and familial behaviors associated with CSA, particularly in southern India. CSA survivors face developmental regression and a spectrum of mental health issues, including PTSD and depression, which can lead to lifelong psychosocial and economic challenges.10,11
Existing literature has made significant strides in understanding the psychological aftermath of CSA; however, aspects such as guilt, self-blame, and resilience in survivors remain underexplored, particularly in the Indian context. Research from southern India is comparatively sparse, and studies specifically from Telangana that comprehensively evaluate psychiatric morbidity, developmental psychopathology, and global functioning in CSA survivors are lacking. This study sought to contribute to the growing body of evidence by adopting a cross-sectional design to assess these key domains in a cohort of CSA survivors from Hyderabad, Telangana, India.
Hypothesis
We hypothesized that specific abuse characteristics, namely penetrative abuse, intrafamilial perpetration, and longer duration, would independently predict higher odds of psychiatric morbidity (particularly PTSD and suicidality), after adjusting for age, gender, and socioeconomic status. We further anticipated that these associations would remain robust after accounting for demographic confounders. Additional analyses of other psychiatric disorders, developmental psychopathology, and functional impairment were designated as exploratory.
Aim
To examine the association between sexual assault profile (SAP) and psychiatric morbidity in survivors of CSA.
Objectives
To assess the prevalence and types of psychiatric disorders among children with a history of sexual abuse.
To assess the developmental psychopathology and global functioning of CSA survivors.
Methods
Study Design
This was a cross-sectional descriptive study conducted among child survivors of sexual abuse, designed to examine their psychiatric morbidity, developmental psychopathology, and global functioning. The study adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) reporting guidelines, which are uploaded as supplementary online material.
Ethical Considerations and Safeguarding
The study was approved by the Institutional Ethics Committee, Osmania Medical College, Hyderabad, and conducted after obtaining permission from the legal authority in charge of the one-stop crisis center. Written informed consent was obtained from parents or legal guardians of children. Additionally, assent was obtained from children aged 13–17 years. Confidentiality was ensured throughout the study. As per the center’s medico-legal protocol, HIV and STD screening, as well as pregnancy testing, were conducted only in cases of penetrative assault and when clinically indicated. Separate informed consent was obtained before these tests as a part of the center’s medico-legal protocol. The rater was not part of the center’s routine treatment team. All psychiatric assessments were conducted by a single doctor (the first author) as part of a thesis, under the close supervision of a consultant psychiatrist, with case-by-case review to ensure diagnostic accuracy. Clinical interviews were employed, given the center’s feasibility. The same rater conducted both psychosocial assessments and diagnostic interviews. Confidentiality was maintained throughout. Participants identified with urgent psychiatric or medical needs (such as suicidality, positive HIV or pregnancy test results) were referred immediately to a tertiary care center following the standard referral pathway.
Participants and Setting
A total of 100 children aged 6–17 years, all legally documented as survivors of CSA under the Protection of Children from Sexual Offenses (POCSO) Act, 2012, were recruited from a government-supported psychosocial support center. The study period spanned from August 2020 to September 2021. The study was conducted at BHAROSA, a government-supported, one-stop support center for women and children in Hyderabad, Telangana, India. The center functions as a multi- disciplinary service hub offering integrated legal, medical, and psychosocial support to survivors of abuse. Children are referred to the center through various channels, including the police, Child Welfare Committees, and other government or non-governmental agencies, following registration of a case under the POCSO Act, 2012. At the center, trained staff conduct initial screening, crisis counseling, and needs assessment. Based on this evaluation, children requiring mental health intervention are referred to appropriate higher-level mental health facilities for further evaluation and treatment. As a result, the study population primarily comprised children who had been identified and documented as survivors of CSA through legal channels, which may represent more severe or complex cases than those managed solely within community settings.
Study Size
The sample size was calculated based on an estimated psychiatric morbidity prevalence of 47% among survivors of CSA, as reported by Norman et al. 12 Using the formula n = Z2 p(1 − p)/d2 and with a 95% confidence level (Z = 1.96), absolute precision of 5% (d = 0.05), and p = .47, the required sample size was approximately 383. This was rounded to 375 to account for feasibility while maintaining the desired precision. However, due to constraints related to the COVID-19 pandemic, including the center’s temporary closure, restricted access, and the inclusion of only legally reported CSA cases, the final achievable sample was smaller. Of the eligible referrals, approximately 130 children could be approached within operational hours; Thirty were not included due to caregiver refusal, lack of assent, or logistical reasons (e.g., children presenting at night when the research team was unavailable).
One hundred participants provided assent and caregiver/guardian consent (or consent from the nominated representative in cases of parental/caregiver perpetration) and were enrolled. This number remained adequate to meet the minimum requirement for detecting the expected prevalence with acceptable precision (Figure 1). All participants were referred within one week of the most recent incident of abuse. Research assessments were conducted after medico-legal registration and crisis intervention, typically at least 1 month after the incident. This ensured that immediate safety and medico-legal procedures were prioritized while still capturing early psychiatric outcomes.
Flowchart Showing Participant Recruitment.
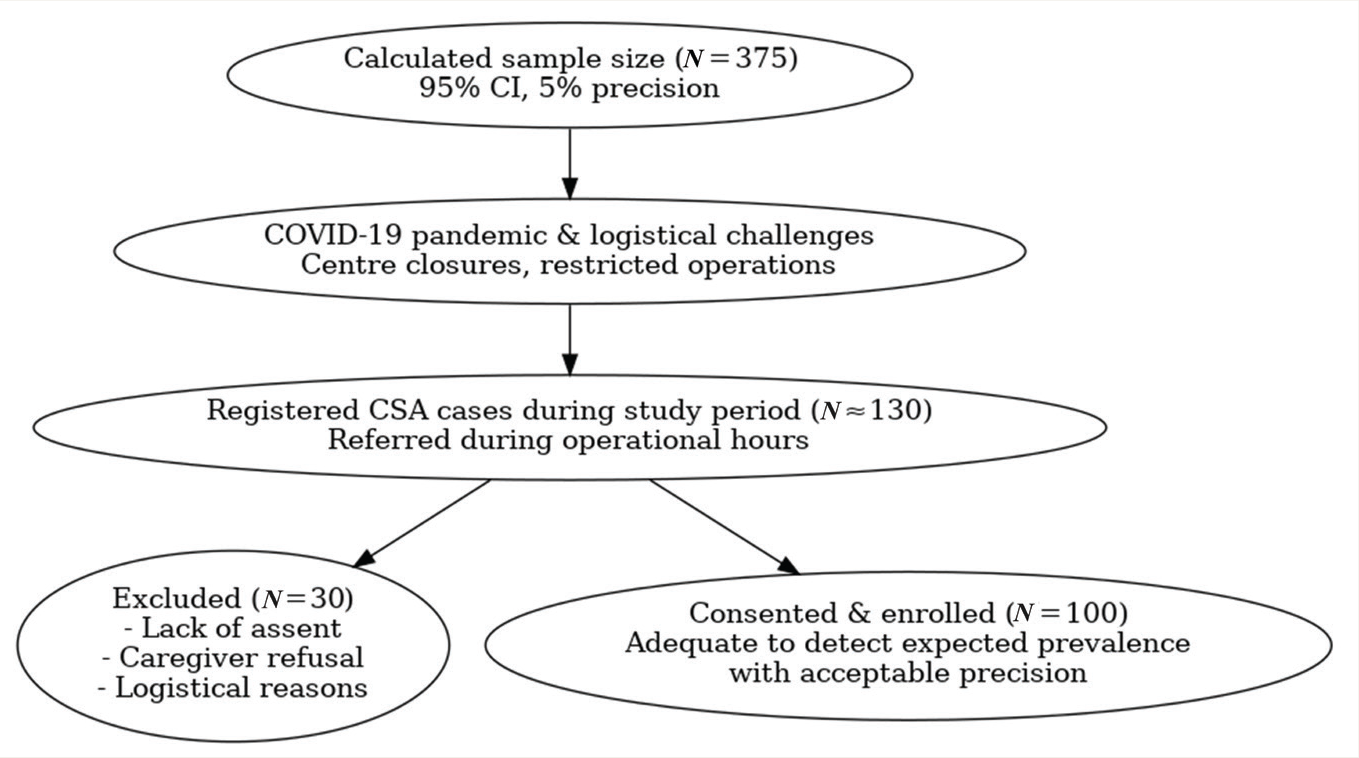
The participant recruitment is depicted in Figure 1.
Procedure
Participants were prepared for the interview through a rapport-building session that used age-appropriate play methods to reduce anxiety and build trust. Interviews were conducted in private spaces by a mental health professional, ensuring confidentiality and comfort. For participants without parental caregivers, data were supplemented using institutional case records and staff inputs. Caregivers of children displaying acute symptoms or screening positive for psychiatric conditions were psycho- educated and referred to higher centers per institutional protocols.
Confidentiality and Reporting Procedures
All cases included in the study were already registered under the POCSO Act and referred for evaluation as part of ongoing medico-legal and psychosocial support processes. Confidentiality was maintained by conducting interviews in a private setting, securely storing data without identifiable details, and restricting access to authorized research team members only.
Measures
Semi-structured Interview Guide
Developed by the investigators through literature review and expert consultation, the guide was pre-tested for clarity and cultural relevance. It included questions on socio-demographic background (age, gender, education, SES, family type), parental substance use, post-abuse custody status, family history of mental illness, and reproductive health concerns (HIV and pregnancy).
Sexual Assault Profile
The SAP by Conte and Berliner was used to document abuse-related characteristics, including age of onset, perpetrator relationship, type, frequency, and disclosure context. 11 Although initially unpublished, the SAP remains a widely cited reference in CSA research and has informed several empirical studies. In this study, only its conceptual structure was adapted to match Indian medico- legal and clinical definitions, rather than used as a standardized tool.
Diagnostic Criteria
Psychiatric diagnoses were made in accordance with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). 13
Developmental Psychopathology Checklist
The Developmental Psychopathology Checklist (DPCL) by Kapur and Barnabas, adapted from the Child Behavior Checklist, was used as a dimensional screening tool for developmental and emotional disturbances. 14 It is a culturally validated Indian screening tool comprising 124 caregiver-rated items assessing domains of developmental history, developmental problems, psychopathology, psychosocial stressors, temperament, and protective factors. The tool has demonstrated high inter-rater reliability (ICC = 0.96, p < .001) and significant convergent validity with the CBCL in Indian samples. In this study, symptom clusters were scored using established cut-offs, enabling the identification of both syndromal and subsyndromal presentations.
Psychiatric morbidity was assessed using a detailed clinical interview in accordance with DSM-5-TR clinical guidelines to establish diagnoses, alongside the DPCL, which allowed for the systematic documentation of both syndromal and subsyndromal psychopathology. The use of both approaches ensured comprehensive coverage of categorical diagnoses and dimensional symptom profiles.
Children’s Global Assessment Scale
The Children’s Global Assessment Scale (CGAS) provides a clinician-rated global score of psychological, social, and academic functioning, measured on a 0–100 scale, with higher scores indicating better overall functioning. 15
Statistical Analysis
Data analysis was conducted using IBM SPSS Statistics for Windows, Version 30.0.0 (IBM Corp., Armonk, NY). Descriptive statistics (frequencies, percentages, means, and SD) were used for demographic and clinical variables. Inferential statistics, including Chi-square tests and Spearman’s rank correlation, were used to examine associations. Logistic regression models were used for these analyses, and adjusted odds ratios with 95% confidence intervals were reported. Proportions are presented with 95% Wilson confidence intervals. All p < .05 were considered statistically significant. References to p = .000 were corrected to p < .001 as per journal guidelines.
The analyses were pre-specified as follows: a priori analyses examined associations between abuse characteristics (penetrative abuse, intrafamilial perpetration, duration) and psychiatric morbidity, adjusting for demographic variables (age, gender, socioeconomic status). Exploratory analyses included developmental psychopathology (DPCL domains), reproductive health outcomes (HIV and pregnancy), and functional impairment (CGAS).
In instances where expected cell counts were low, χ2 test assumptions may not have been fully satisfied. Given the exploratory nature of this study, these analyses were retained for completeness, and the findings should be interpreted with caution.
Results
Participation and Socio-demographic Characteristics
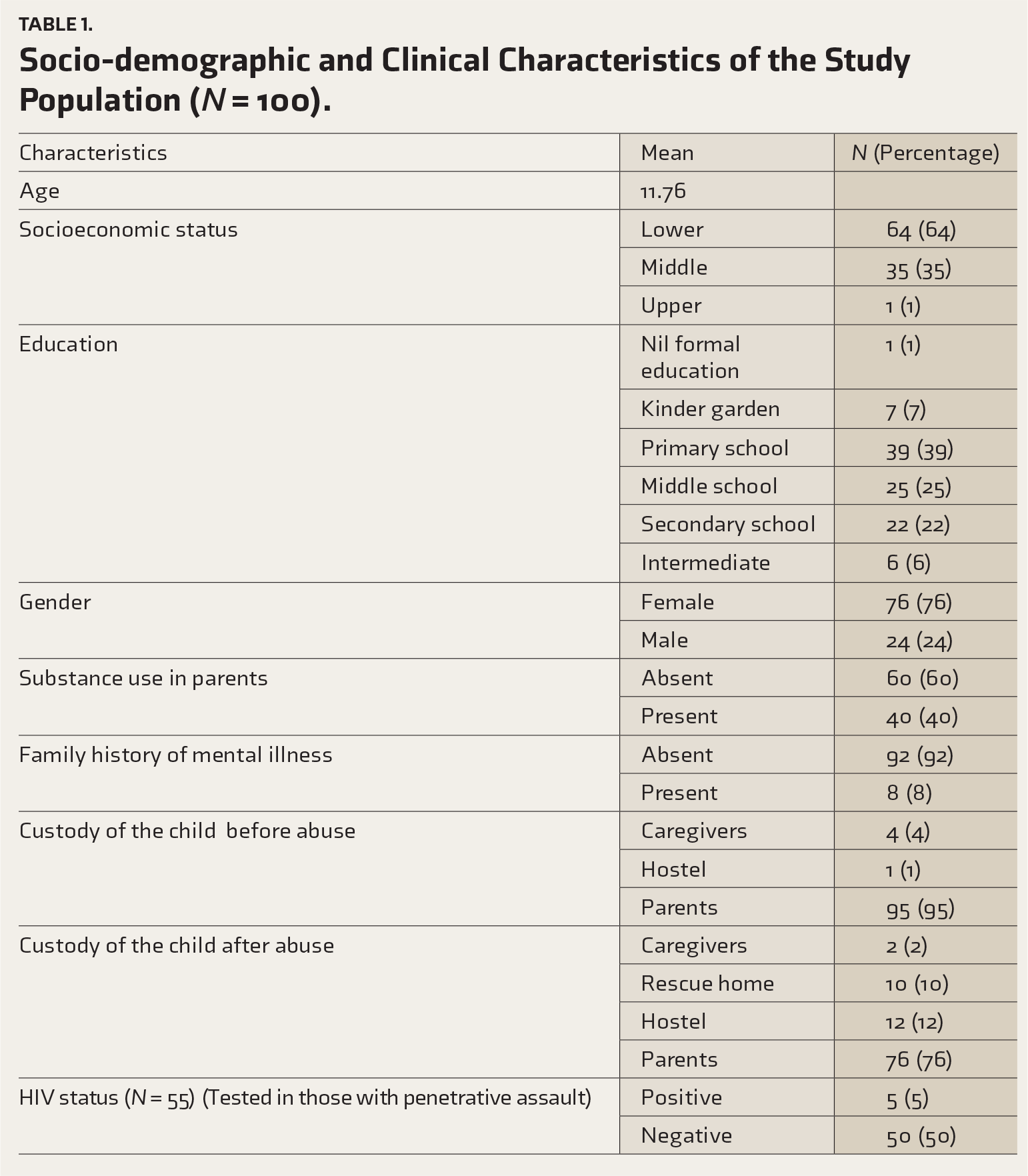
A total of 130 children were referred during the study period. Of these, 30 declined or were unable to participate due to logistical constraints, resulting in a final enrolled sample of 100 participants. The mean age of the participants was 11.76 years (SD = 3.46). Females constituted 76% of the sample, and males comprised 24%. The average family size was 5.56. Educationally, most participants were either in primary school (39%) or middle school (25%).
A family history of mental illness was reported in 8% of the sample, and 64% of participants belonged to a lower socioeconomic status (LSES). Before the abuse, 95% of participants were under parental custody. Post-abuse, 76% continued living with their parents, while others stayed in hostels (12%), rescue homes (10%), or with non-parental caregivers (2%).
HIV positivity was identified in 5% of participants, while the HIV status of 17% remained unknown. Two participants were pregnant at the time of evaluation. Further socio-demographic details are provided in Table 1.
Socio-demographic and Clinical Characteristics of the Study Population (
Profile of Sexual Assault
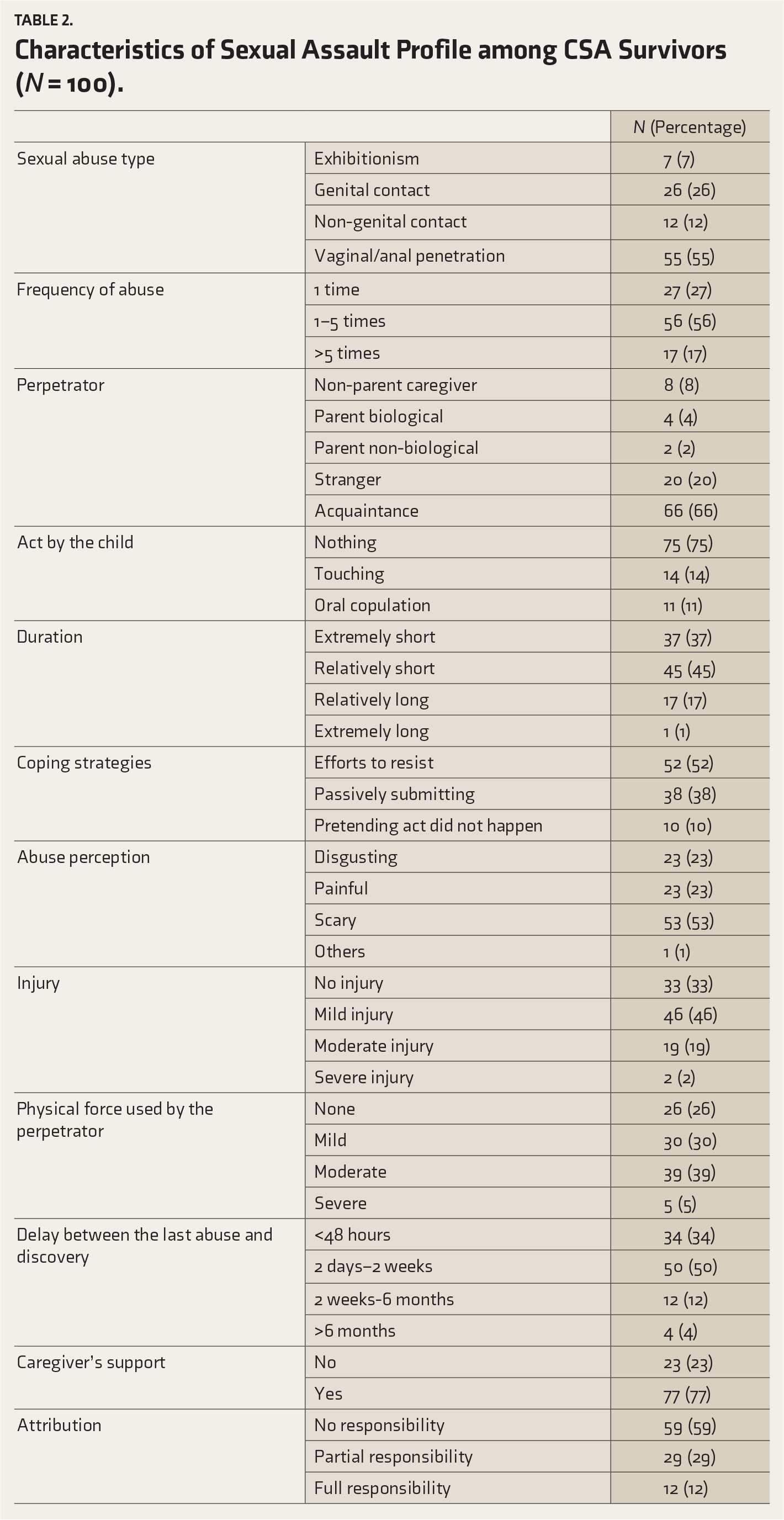
The mean age at first CSA encounter was 10.87 years. More than half of the participants (56%) reported being abused 1–5 times. In 66% of cases, the perpetrator was an acquaintance of the child’s family. The most common form of abuse was vaginal/anal penetration (55%), followed by genital contact such as touching or fondling (26%). Oral copulation (11%) and forced touching of the perpetrator (14%) were also reported.
Delays in reporting the abuse were common. Half of the participants experienced delays of 2 days to 2 weeks, while four participants reported delays exceeding 6 months. Moderate injuries, including bruises, pain, and bleeding, were reported in 19%, and severe injuries were noted in 2%, where participants were physically tied and beaten.
Active resistance to the abuse was reported by 52% of the children, while 10% pretended the act did not occur. Self-blame was significant: 12% attributed full responsibility to themselves, and 29% attributed partial responsibility. Unsupportive caregiver responses, such as dismissal or blaming, were reported by 23% of the participants. Additional details are presented in Table 2.
Characteristics of Sexual Assault Profile among CSA Survivors (
Psychiatric Morbidities
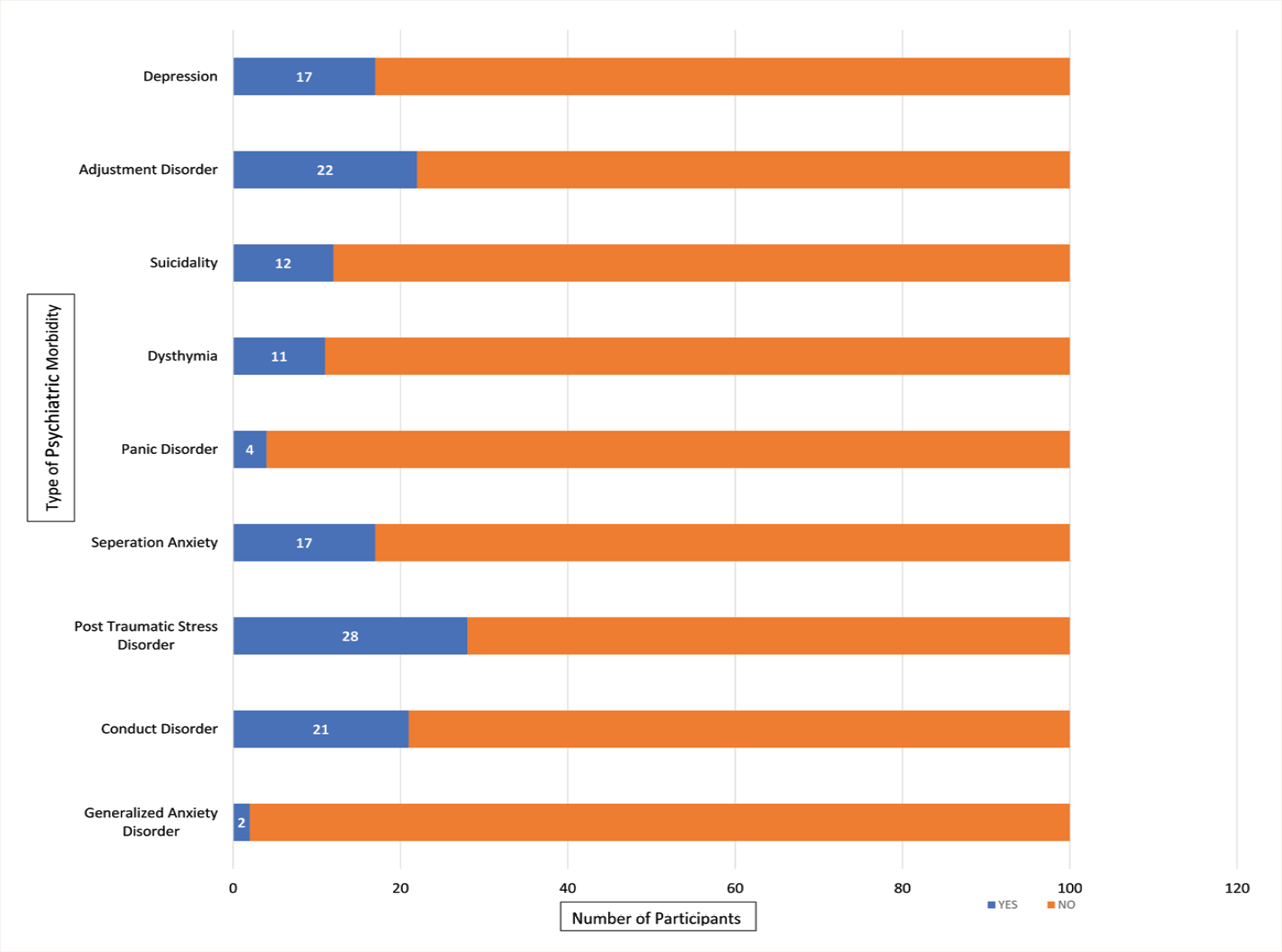
Psychiatric disorders were identified in 53% of participants. It was found that 2% (n = 2; 95% CI: 0.6–7.0) had generalized anxiety disorder (GAD), 21% (n = 21; 95% CI: 14.2–30.0) had conduct disorder, 28% (n = 28; 95% CI: 20.1–37.5) had post-traumatic stress disorder (PTSD), 17% (n = 17; 95% CI: 10.9–25.5) had separation anxiety, 4% (n = 4; 95% CI: 1.6–9.8) had panic disorder, 11% (n = 11; 95% CI: 6.3–18.6) had dysthymia, 12% (n = 12; 95% CI: 7.0–19.8) expressed suicidality, 22% (n = 22; 95% CI: 15.0–31.1) had adjustment disorder, and 17% (n = 17; 95% CI: 10.9–25.5) had depression. Further breakdowns are provided in Figure 2. Some participants had >1 diagnosis; therefore, category percentages can exceed the overall morbidity percentage.
Psychiatric Morbidities in the Study Population (N = 100).
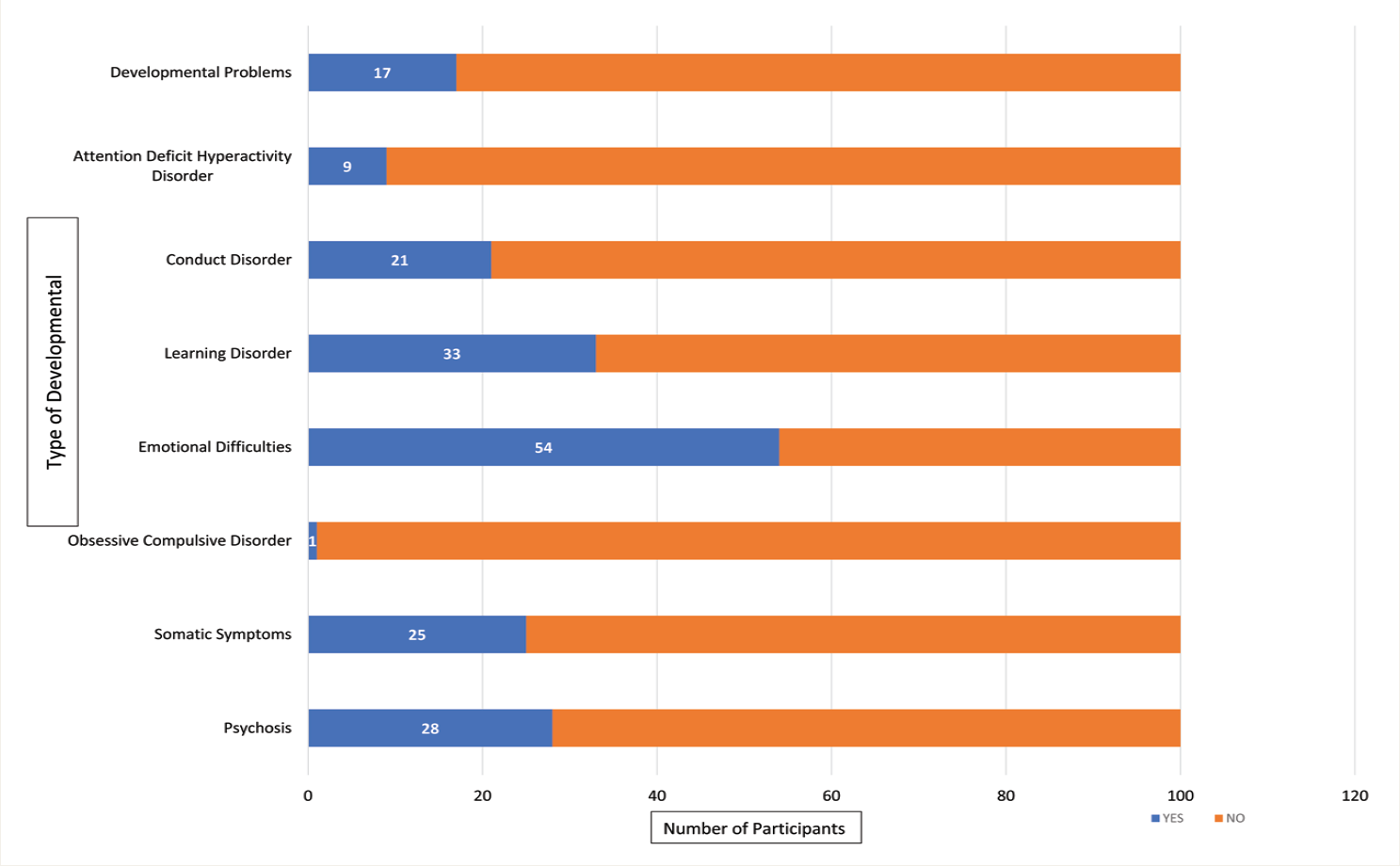
Subsyndromal Presentations and Developmental Psychopathology
Screening with the DPCL identified 25% (n = 25; 95% CI: 17.5–34.3) of participants with somatic symptoms, 54% (n = 54; 95% CI: 44.3–63.4) with emotional difficulties, 33% (n = 33; 95% CI: 24.6–42.7) with learning difficulties, and 9% (n = 9; 95% CI: 4.8–16.2) with ADHD. Developmental problems such as stammering, wetting clothes, and cyanotic spells were observed in 17% (n = 17; 95% CI: 10.9–25.5). Emotional difficulties commonly include daydreaming, poor memory, withdrawal, and excessive worry. Detailed data are illustrated in Figure 3.
Frequencies of the Developmental Psychopathology (N = 100).
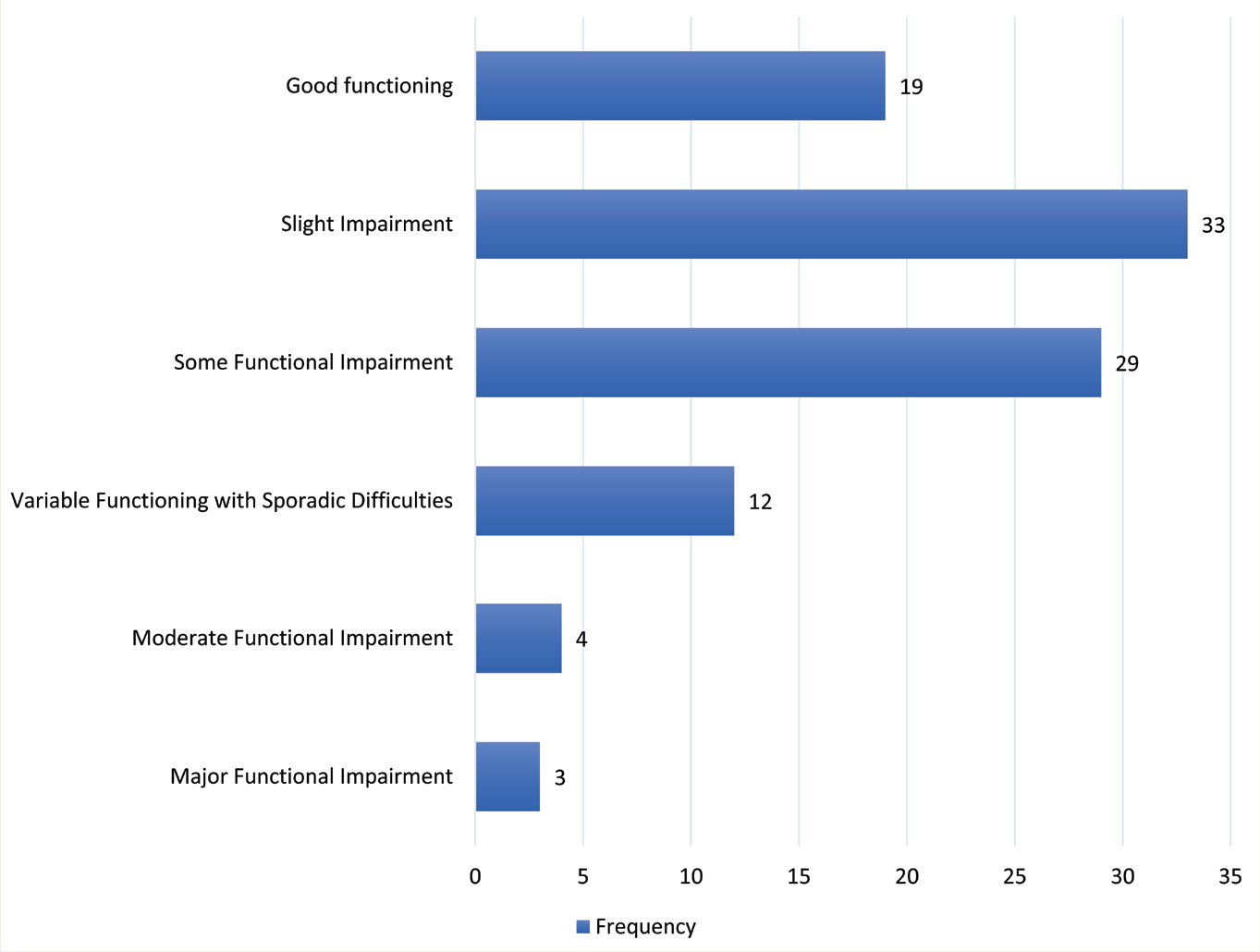
Children’s Overall Functioning
The mean CGAS score was 69.2 (SD = 12.2). Functioning levels were distributed as follows: 19% (n = 19; 95% CI: 12.5–27.8) had “Good Functioning,” 33% (n = 33; 95% CI: 24.6–42.7) had “Slight Impairment,” 29% (n = 29; 95% CI: 21.0–38.5) had “Some Functional Impairment,” 12% (n = 12; 95% CI: 7.0–19.8) had “Variable Functioning with Sporadic Difficulties,” 4% (n = 4; 95% CI: 1.6–9.8) had “Moderate Functional Impairment,” and 3% (n = 3; 95% CI: 1.0–8.5) had “Major Functional Impairment.” Details are visualized in Figure 4.
Global Functioning of Child Sexual Abuse Survivors.
Association Between SAP and Psychiatric Morbidity
Logistic regression analysis revealed statistically significant associations between various characteristics of the SAP and psychiatric morbidities:
Depression
Children who experienced vaginal or anal penetration had significantly higher rates of depression (χ2 = 4.15, p = .04). Those who coped by pretending the act had not occurred also showed greater depression rates than children who resisted or submitted passively (χ2 = 3.99, p = .04).
Adjustment Disorder
Adjustment disorder was significantly associated with active resistance during abuse (χ2 = 6.0, p = .009), male gender (χ2 = 4.0, p = .04), and self-blame for the incident (χ2 = 4.98, p = .02).
Suicidality
Suicidality was significantly higher among children who experienced vaginal/anal penetration (χ2 = 15.6, p < .001), longer durations of abuse (χ2 = 6.3, p = .01), greater physical injury (χ2 = 6.3, p = .01), and those who used denial as a coping strategy (χ2 = 9.77, p = .002).
Dysthymia
Higher dysthymia rates were seen in children with vaginal/anal penetration (χ2 = 4.69, p = .03), prolonged abuse (χ2 = 8.8, p = .003), and denial coping (χ2 = 9.28, p = .002). Females were more likely to experience dysthymia than males (χ2 = 6.4, p = .01).
Panic Disorder
No significant associations were found between panic disorder and any individual SAP variable.
Separation Anxiety
Separation anxiety was significantly associated with supportive caregiver reactions (χ2 = 12.27, p < .001), abuse by non-parent caregivers (χ2 = 10.4, p = .03), perceiving the act as frightening (χ2 = 4.89, p = .02), and prolonged duration of abuse (χ2 = 6.29, p = .01).
Post-traumatic Stress Disorder
Post-traumatic stress disorder (PTSD) was more frequent in children subjected to greater physical force (χ2 = 8.67, p = .003), visible injury (χ2 = 11.8, p = .001), and those from lower socioeconomic backgrounds (χ2 = 6.2, p = .04).
Conduct Disorder
Conduct disorder was significantly associated with vaginal/anal penetration (χ2 = 6.2, p = .01), physical injury (χ2 = 5.2, p = .02), and self-blame for the incident (χ2 = 4.2, p = .039).
Generalized Anxiety Disorder
Longer duration of abuse was significantly related to higher rates of GAD (χ2 = 4.9, p = .026).
Custody and Separation Anxiety
Children placed in hostels or rescue homes post-abuse had significantly higher rates of separation anxiety compared to those residing with family (χ2 = 74.72, p < .001).
Discussion
The present study addresses a critical gap in Indian literature by examining the association between SAPs and psychiatric morbidity among legally documented CSA survivors referred to a medico-legal crisis center. This cross-sectional work highlights the high burden of psychiatric morbidity in this population, identifies important risk factors, and provides a foundation for future longitudinal research.
Previous Indian studies, such as Bhaskaran et al., have extensively examined psychiatric morbidity in CSA survivors presenting to psychiatric services, often after significant delays from the index event. 10 In contrast, the present study was conducted in a one-stop crisis center (BHAROSA) where children were referred through the legal system within one week of the most recent incident of abuse. This early referral pathway allowed for the identification of acute psychiatric presentations and functional impairments soon after the event. Additionally, while prior studies have relied mainly on diagnostic interviews alone, we incorporated the DPCL, enabling the assessment of both syndromal and subsyndromal psychopathology within a culturally validated framework. The study also uniquely links psychiatric morbidity profiles with global functioning scores in this acute phase, offering insights that may guide early intervention strategies in similar medico-legal contexts.
The mean age of participants was 11.76 years, and 64% had a LSES. This aligns with findings from Sedlak et al., who reported that children from LSES families are significantly more vulnerable to sexual abuse and other forms of endangerment. 16 Specifically, children from LSES were twice as likely to experience sexual abuse and three times as likely to face endangerment compared to those from higher socioeconomic groups. Females accounted for 76% of the sample, consistent with evidence suggesting that girls are 1.5–5.5 times more likely to experience sexual abuse than boys. 17 Boys often remain underrepresented in studies due to underreporting, especially as older boys may avoid disclosing abuse because of stigma or involvement in juvenile justice systems. 18 Bhaskaran et al. reported similar demographics, with children from LSES comprising 60% of their study and a mean age of 11.65 years, indicating comparable trends in CSA prevalence across studies in southern India. 10
The study also revealed that 73% of participants had experienced CSA on more than one occasion, highlighting the recurrent nature of such trauma. Evidence suggests that females with CSA histories are 3–5 times more likely to experience revictimization, whether sexual or physical, often before completing high school. 19 Vaginal or anal penetration was the most frequently reported form of abuse (55%), consistent with findings from Bhaskaran et al., who identified these as the most common forms in their retrospective chart review in Bangalore. 20 Moreover, 80% of participants in this study knew their perpetrator, reflecting global evidence that CSA is predominantly perpetrated by individuals known to the victim, such as family members, family friends, or neighbors. Studies have shown that intrafamilial abuse is linked to more severe consequences, including earlier onset, longer duration, and greater physical and psychological harm compared to abuse by acquaintances or strangers. 21
Self-blame emerged as a significant finding in this study, with 12% of participants attributing full responsibility for the abuse and 29% attributing partial responsibility. The role of self-attribution in mediating the psychological impact of CSA has been well-documented. Cohen and Mannarino have shown that self-blame amplifies the emotional consequences of abuse, contributing to depression, interpersonal difficulties, and intrusive symptoms. 22 The prevalence of psychiatric morbidity in the present study was 53%, with PTSD being the most commonly diagnosed condition (28%). This finding is lower than the 75% morbidity reported by Bhaskaran et al., likely due to methodological differences. That study employed a retrospective design over three years, potentially capturing more severe cases referred for tertiary care. 10
The CSA is a well-established risk factor for a range of psychiatric conditions, including depression, PTSD, low self- esteem, suicidality, and substance use. 23 Participants who experienced vaginal/anal penetration or coped by pretending the abuse did not occur exhibited higher rates of depression, PTSD, and suicidality. Severe physical injuries, such as those reported in this study, were strongly associated with PTSD, conduct disorder, and suicidality. These findings underscore the complex interplay between the nature of the abuse and its psychological outcomes.
Children placed in hostels or rescue homes post-abuse demonstrated higher rates of separation anxiety disorder. While such placements protect children from abusive caregivers, they can disrupt recovery by separating children from their familiar environments and social supports. This finding aligns with studies suggesting that children removed from their homes often experience heightened anxiety and emotional distress. Furthermore, previous research has linked CSA to externalizing behaviors, including delinquency and conduct symptoms, particularly during adolescence. 24
The study also identified learning disorders (LD) as a significant concern, with 33% of participants screening positive for LD. National-level data from the United States indicate that children with LDs are 2–3 times more likely to experience sexual abuse compared to their peers. 25 This heightened vulnerability may stem from cognitive or social challenges that make children with LDs easier targets for perpetrators. Additionally, 25% of participants reported somatic complaints, including dizziness, fainting spells, and unexplained aches. These findings are consistent with Kirmayer et al., who noted that somatic symptoms are common among sexually abused children. 26 This may reflect an interpretation of emotional distress through physical manifestations, a phenomenon frequently observed in trauma survivors.
Emotional difficulties, reported by 54% of participants, warrant special attention as they place children at high risk for developing psychiatric conditions such as depression and PTSD. Symptoms included withdrawal, excessive worrying, and social timidity, all of which require closer monitoring and intervention.
Reproductive health consequences were also evident in this study, with five participants testing positive for HIV and 17 having unknown HIV status. Vaginal or anal penetration significantly increases the risk of HIV transmission due to mucosal breaches and the immaturity of the anogenital tract. Additionally, two participants were pregnant at the time of evaluation, emphasizing the role of CSA as a significant risk factor for adolescent pregnancies. Such outcomes highlight the need for integrated health services to address both the physical and psychological sequelae of abuse.
The findings of this study underscore the substantial impact of CSA on children’s mental, emotional, and physical health. Among legally documented CSA survivors, we observed a high prevalence of psychiatric morbidity alongside significant somatic and emotional symptoms. These results highlight the urgent need for comprehensive, trauma-informed interventions tailored to this group. Early identification and treatment of psychiatric conditions, coupled with supportive rehabilitation strategies, are essential to improve recovery trajectories and long-term outcomes for affected children.
Clinical Implications
The findings underscore the need for active screening of psychiatric morbidities, including depression, PTSD, conduct disorders, and suicidality among all legally documented CSA survivors. From a developmental psychopathology perspective, the co-occurrence of psychiatric, somatic, and functional disturbances highlights how early trauma disrupts emotional regulation, attachment, and cognitive development. Such disruptions increase vulnerability to internalizing and externalizing psychopathology. 27 Supportive caregiving and early therapeutic engagement, however, can foster resilience and mitigate long-term impacts.
Early identification and timely intervention are essential to reduce long-term psychological consequences. A 2023 meta-analysis has affirmed robust associations between CSA and adolescent psychopathology, reinforcing the clinical imperative of early surveillance and intervention. 28
Multisectoral engagement is critical. Awareness programs must emphasize education on safe and unsafe touch, consent, and rights, notably through school-based sex education that equips children to recognize and report abuse. Teachers serve as crucial first responders and should be trained to identify behavioral and emotional indicators of trauma and refer children for mental health assessment.
Caregiver involvement plays an equally vital role. Parents and guardians should receive guidance on offering psychological support and reassurance to children. Pediatricians and family physicians, who often encounter families early, can reinforce awareness by disseminating educational materials such as brochures and posters.
Despite the enactment of the POCSO Act (2012), delays in reporting and psychological care remain common, often due to stigma and the frequent involvement of known perpetrators. Targeted awareness efforts, especially in schools and community health programs, can help overcome these barriers and ensure earlier access to psychosocial support.
Finally, although the present study did not examine longitudinal outcomes, an umbrella review of meta-analyses has documented substantial long-term psychiatric, social, and physical health sequelae of CSA. 29 This underscores that early interventions may have enduring preventive benefits.
Additionally, this study observed that three participants had below-normal intelligence, although formal IQ assessments were not conducted. Research suggests that children with intellectual disabilities or LD are at increased risk of CSA, emphasizing the need for targeted prevention programs in this vulnerable population.
Preventive Interventions
Teachers, parents, and healthcare professionals across disciplines, including residents, play a vital role in preventing and detecting CSA. Teachers can help by creating safe classroom environments, teaching children to recognize red-flag behaviors, and encouraging open communication with trusted adults. Parents, likewise, should be sensitized through structured conversations during outpatient or community visits by trained professionals.
Healthcare providers should actively consider CSA as a possible differential diagnosis when faced with children presenting with vague somatic or behavioral symptoms, such as recurrent abdominal pain, anxiety, regression, or withdrawal. Integrating CSA awareness into clinical and academic curricula ensures early recognition and trauma-informed care.
Finally, addressing stigma and improving disclosure is crucial. Sole reliance on police or proxy reports underestimates the actual burden. Empowering children through education, sensitizing families, and equipping all professionals to respond compassionately can collectively strengthen detection, intervention, and rehabilitation for survivors.
Strengths
This study stands out as one of the few in India to assess the prevalence and correlates of individual psychiatric disorders in child survivors of CSA. The inclusion of the DPCL, a culturally adapted Indian tool, enabled the identification of developmental regression and subsyndromal presentations often missed by standard measures. Furthermore, by evaluating global functioning using the CGAS, this study provides a comprehensive view of the child’s holistic well-being, a dimension rarely addressed in previous research. The study was conducted at BHAROSA, a registered support center for women and children, which ensured reliable data collection and active screening for reproductive health factors such as HIV and pregnancy status. These factors, often overlooked, were systematically assessed in this study, adding depth to the findings and addressing an important gap in the existing literature.
Limitations
The study was primarily exploratory, with a priori analyses restricted to abuse- profile–psychiatric morbidity associations. Other domains (DPCL, CGAS, reproductive health) were exploratory and should be interpreted with caution. The small sample (n = 100) limited statistical power and generalizability. Subgroup analyses may be underpowered, increasing risks of both Type I and Type II errors. Some contingency tables had small cell sizes, potentially violating χ2 assumptions. While Fisher’s exact test would be ideal, analyses were retained for transparency. Findings are therefore best viewed as preliminary and hypothesis-generating. The sample, drawn from a medico-legal crisis center, likely represents severe or legally pursued CSA cases, differing from community samples. Results should not be generalized to all CSA survivors. This study’s diagnostic procedures relied on single-rater assessments without structured diagnostic instruments (e.g., MINI-Kid, K-SADS). Although each case was reviewed under close consultant supervision, the absence of blinding and formal inter-rater reliability assessments increases the risk of rater bias. Blinding was not feasible because the same rater conducted both psychosocial and diagnostic evaluations, potentially introducing rater bias. Absence of a control group limits direct comparison with non-abused populations and precludes causal inference due to the cross-sectional design. Additionally, comparisons involving reproductive health outcomes such as HIV and pregnancy were based on small subsamples and limited event counts. These analyses were therefore underpowered and exploratory, and the findings should be interpreted cautiously as hypothesis-generating rather than confirmatory.
Despite methodological constraints, this study offers valuable insights for Indian child psychiatry practice. The early medico-legal sample, drawn from a one-stop crisis center, represents a rarely documented clinical population in whom psychiatric assessment, developmental screening, and reproductive health needs converge. By combining categorical DSM-5-TR diagnoses with dimensional measures such as the DPCL and CGAS, the study provides a holistic view of morbidity and functioning in CSA survivors. The inclusion of reproductive health outcomes (HIV and pregnancy) adds further clinical relevance, as these domains are often neglected in psychiatric studies. Notably, the study was conducted in collaboration with local services, ensuring immediate pathways for safeguarding and treatment.
Recommendations for Future Research
This study highlights the urgent need for more research to establish the mental health consequences of CSA in the Indian context. Larger, multicentric studies with comparison groups are essential to enhance the generalizability of findings. Future research should focus on: (a) Understanding the complexity of risk factors, including socio-cultural influences such as patriarchy, victim-shaming, and gender biases, which perpetuate the stigma and underreporting of CSA, (b) Investigating resilience factors that may mitigate the psychological impact of CSA, providing a balanced perspective for intervention planning. (c) Addressing the growing prevalence of non-contact CSA, particularly through digital platforms such as the internet and mobile phones, which is increasingly relevant in the adolescent population, and (d) Developing holistic treatment interventions not just for the child but also for caregivers, emphasizing the role of family support in recovery.
Conclusions
This exploratory study highlights the psychiatric morbidity, developmental challenges, and functional impairment observed among legally documented CSA survivors referred to a medico-legal crisis center. These findings underscore the importance of early psychiatric evaluation and integrated care pathways in similar medico-legal settings. Broader generalization to all CSA survivors, especially those who do not access legal or crisis services, should be made with caution, and future community-based research is warranted.
This study highlights the substantial psychological and functional burden faced by legally documented CSA survivors. Significant associations were observed between abuse characteristics and psychiatric morbidity, particularly depression, PTSD, suicidality, and poor global functioning. Factors such as self-blame, duration and severity of abuse, and reproductive health outcomes (HIV and pregnancy) underscore the need for comprehensive medical and psychological support.
Given the modest sample size and the exploratory nature of the analyses, the findings should be interpreted as hypothesis-generating and provide critical groundwork for larger, longitudinal studies.
Early recognition and treatment of psychiatric sequelae remain key to recovery and prevention of revictimization. Implementation of the Mental Healthcare Act (2017) must prioritize accessible, trauma-informed services for survivors, especially those from disadvantaged backgrounds.
Finally, sustained awareness and capacity-building among teachers, parents, and healthcare providers are essential. Integrating CSA education and support frameworks within schools, healthcare, and legal systems can strengthen early detection, ensure coordinated care, and foster a safer environment for children.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
We express our heartfelt gratitude to our guide and co-guide for their invaluable mentorship throughout the course of this study. We sincerely thank the Department of Psychiatry, Osmania Medical College, for granting permission and the opportunity to conduct this study. We are deeply thankful to the BHAROSA Centre, Hyderabad, for their cooperation and for their continued service in protecting and supporting survivors. Finally, we offer our deepest appreciation to the survivors and their caregivers who participated in the study. Their courage and resilience remain an enduring source of inspiration.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethics Committee Approval and Permissions
The study was approved by the Institutional Ethics Committee of Osmania Medical College, Hyderabad (Approval No: ECR/300/Inst/AP/2013/RR-19; Date: 8th May, 2019). Written permission to conduct the study at the BHAROSA Centre was obtained from the Additional Commissioner of Police, Hyderabad.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Written informed consent was obtained from the parent/legal guardian of all participating children, and assent was obtained from children wherever developmentally appropriate. All procedures were approved by the Institutional Ethics Committee, and confidentiality of participants was strictly maintained.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.