
Abstract
Schema Therapy (ST) is an integrative therapeutic approach for addressing personality disorders such as Avoidant Personality Disorder (AvPD). This approach emphasizes the identification and healing of Early Maladaptive Schemas (EMS) and the use of schema modes that contribute to the development of PDs. Schema modes are moment-to-moment reflections of emotional and behavioral states triggered by the activation of different EMS. They comprise thoughts, emotions, and behaviors. Coping modes, a subset of schema modes, are unconscious strategies employed to manage distress that obstructs access to an individual’s vulnerabilities. This article illustrates the therapeutic process of ST in working through the dysfunctional coping modes of Ms. A, a 22-year-old female diagnosed with AvPD and Depression. It highlights the significant challenges encountered in therapy with respect to the client’s detached and avoidant protector modes. Therapeutic interventions, such as limited reparenting and empathic confrontation, played a crucial role in addressing dysfunctional coping modes and facilitating access to clients’ vulnerable child modes. This study further underscores the importance of considering therapeutic relationships when engaging with clients’ coping strategies. Finally, the implications of addressing coping modes in the treatment of clients with AvPD are discussed. As a single-case study, its findings have limited generalizability due to the presence of other confounding factors, including the role of concurrent medication in the outcome.
Avoidant Personality Disorder (AvPD) is characterized by persistent social inhibition, hypersensitivity to unfavorable evaluations, feelings of inadequacy, low self-confidence, and avoidance of challenging situations. 1 Psychotherapy is the most effective treatment for clients with AvPD. Despite the high global prevalence of Cluster-C (PD), 2 this group has been overlooked, with no universally accepted international best-practice guidelines.3,4 Severe presentations are complex, with high prevalence of childhood trauma and co-morbid anxiety and mood disorders, posing treatment challenges. Thus, researchers are increasingly advocating for focused attention on cluster-C PD.4,5
Schema Therapy (ST) is an integrative approach to treating PD. 6 It examines environmental influences and unmet childhood needs that give rise to Early Maladaptive Schemas (EMS) and schema modes, which contribute to the development of PD. ST helps clients understand their core emotional needs and learn adaptive ways to meet them. 7 ST focuses on schema modes in treatment, aiming to “heal” the child modes and strengthen the functional modes that represent the client’s well-adjusted side.
Research shows that in Cluster-C PD, modes form interconnected networks. For example, the avoidant protector influences the detached protector mode. In contrast, the compliant surrender and demanding parent modes influence one another, consistent with the schema theory, which posits that modes are interconnected. 8
While these coping modes might generate secondary emotions, they block access to the client’s core vulnerability. In AvPD, schemas related to social isolation, pessimism, emotional inhibition, failure, subjugation, and defectiveness predominate, with detachment and surrender as the primary coping mechanisms. 9 Therapists face challenges in treating them due to their patterns of avoidance, control, and assuming a passive role in therapy. However, they have a strong need for social affiliation and emotional closeness.10,11 This also creates therapeutic challenges involving resistance and ruptures, which must be addressed to access client vulnerability and develop healthier schema modes.
Case Context and Method
This study presents a case example from a larger ongoing Ph.D. study being conducted at a tertiary care setting, illustrating the application of ST in one of the participants diagnosed with AvPD and Depression. The client was referred for addressing the personality problems that were contributing to recurrent episodes of depression. This article provides an in-depth account of the therapeutic process of identifying and working with dysfunctional coping schema modes and enhancing adaptive schema modes.
Case Description
Ms. A, a 22-year-old female who studied until graduation, presented with a prolonged period of low mood, anhedonia, anergia, loss of appetite, difficulty falling asleep at night, nightmares, physical fatigue, aches and pains in the body, feelings of hopelessness, and helplessness with passive death wishes for more than two months. She spent most of her days in her room. She expressed anxiety about being around people, initiating and maintaining conversations, and feeling a deep sense of inferiority since childhood. She further reported feeling anxious when facing new situations or challenges, fearing that she might not meet others’ expectations and preferring to avoid them, which left her feeling lonely.
Case Formulation and Treatment Plan
Ms. A, the elder of the two children, resided in a nuclear family with her parents, younger sister, and paternal grandmother. She characterized her childhood as deficient in emotional support and care, having an ambivalent relationship with her parents, and frequently feeling isolated and vulnerable, indicative of EMS of abandonment and emotional deprivation. During her upbringing, she was exposed to critical messages from her parents and grandmother, which profoundly affected her self-image and self-esteem. As the eldest daughter, she frequently encountered expectations to be responsible, altruistic, and obedient to all directives, potentially fostering an EMS of subjugation. Despite increasing demands placed on her, she perceived a lack of validation and appreciation for her efforts, and she faced criticism when she failed to meet these expectations. She consistently received the message to strive for continuous improvement and never accept anything less than excellence (EMS of unrelenting standards). Her inability to meet the established standards exacerbated her feelings of inadequacy, guilt, and shame. Her social interactions at school were limited. Her childhood memories were of her predominantly sitting alone in classrooms, experiencing anxiety, and perceiving her peers as disinterested in becoming friends with her (EMS of social isolation). She often felt that she had little to offer others, engaged in constant comparisons with others, and felt incompetent (EMS of defectiveness). Although she desired close friendships, she experienced significant difficulty fully expressing her emotions due to fear of being disliked, judged, or even abandoned. When experiencing problems in friendships, she often felt “used” and taken advantage of, which made her apprehensive of others’ intentions and further involvement with them (EMS of mistrust). Her experiences, both at home and in other environments, reinforced her belief that she would never receive the care or love she genuinely deserved from others, a phenomenon consistent with the emotional deprivation of EMS.
Assessment
The Young Schema Questionnaire-S3 (YSQ-S3) 12 and Schema Mode Inventory I+II (SMI I+II)13–15 identified the client’s EMS and schema modes relevant to this study. The YSQ-S3 consists of 90 items rated on a 6-point scale, from “completely untrue of me” to “describes me perfectly.” It gives a total score as well as scores for 18 distinct EMS. The SMI I+II comprises 163 items scored on a 6-point Likert scale, ranging from “never” to “always.” 16 Different schema modes can be evaluated using this scale. Both scales have robust psychometric properties.13,14,17 Higher scores (range 1–6) represent a greater presence of the EMS/schema mode and greater dysfunction, except for the healthy adult mode, where higher scores are desirable. For this article, only the mean scores for the EMS and schema modes relevant to the case study are presented in Table 1. No missing data were found. Figure 1 shows a diagrammatic representation of the schema-mode model.
Mean Scores on YSQ-S3 and SMI I+II.
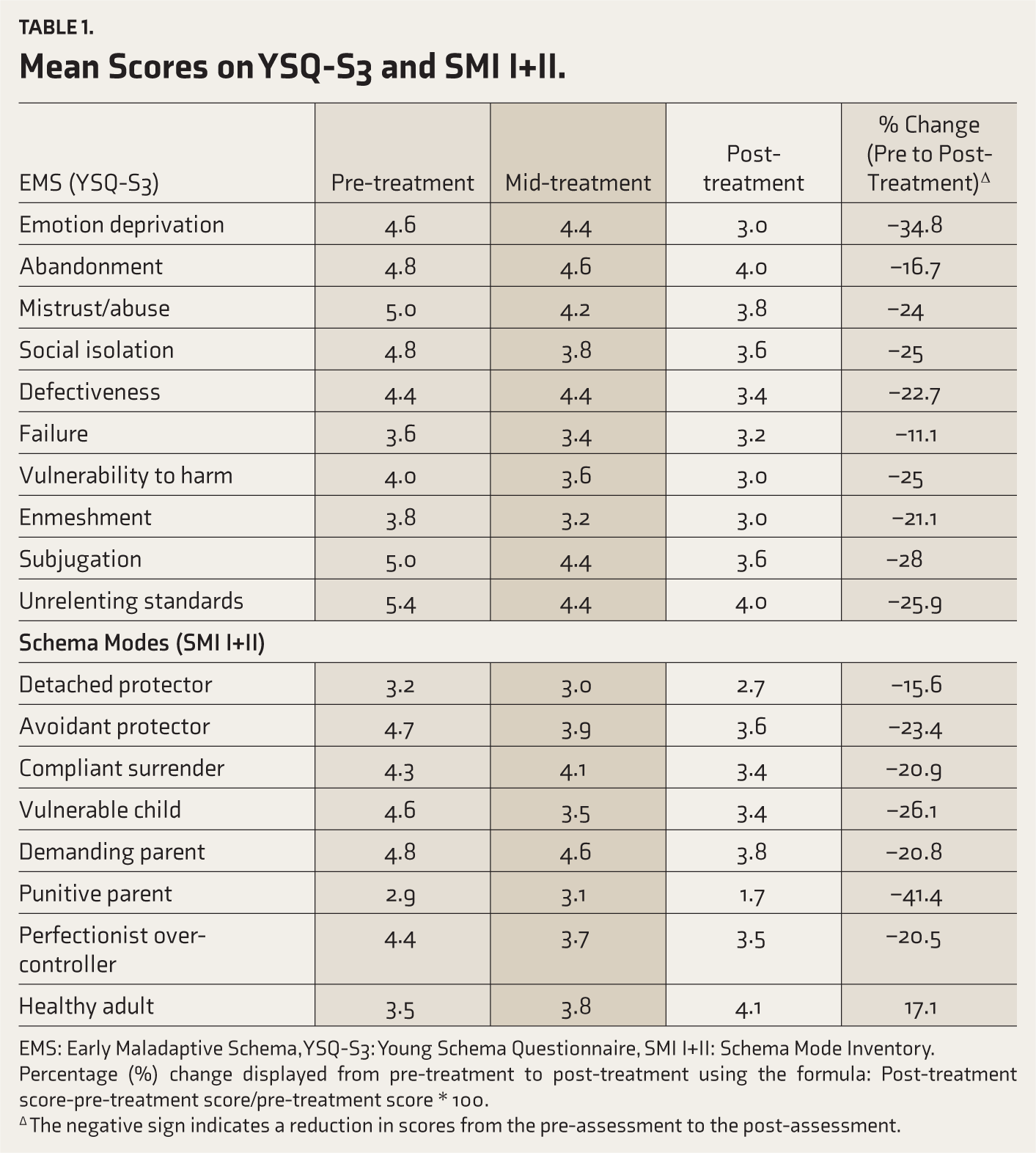
EMS: Early Maladaptive Schema, YSQ-S3: Young Schema Questionnaire, SMI I+II: Schema Mode Inventory.
Percentage (%) change displayed from pre-treatment to post-treatment using the formula: Post-treatment score-pre-treatment score/pre-treatment score * 100.
∆ The negative sign indicates a reduction in scores from the pre-assessment to the post-assessment.
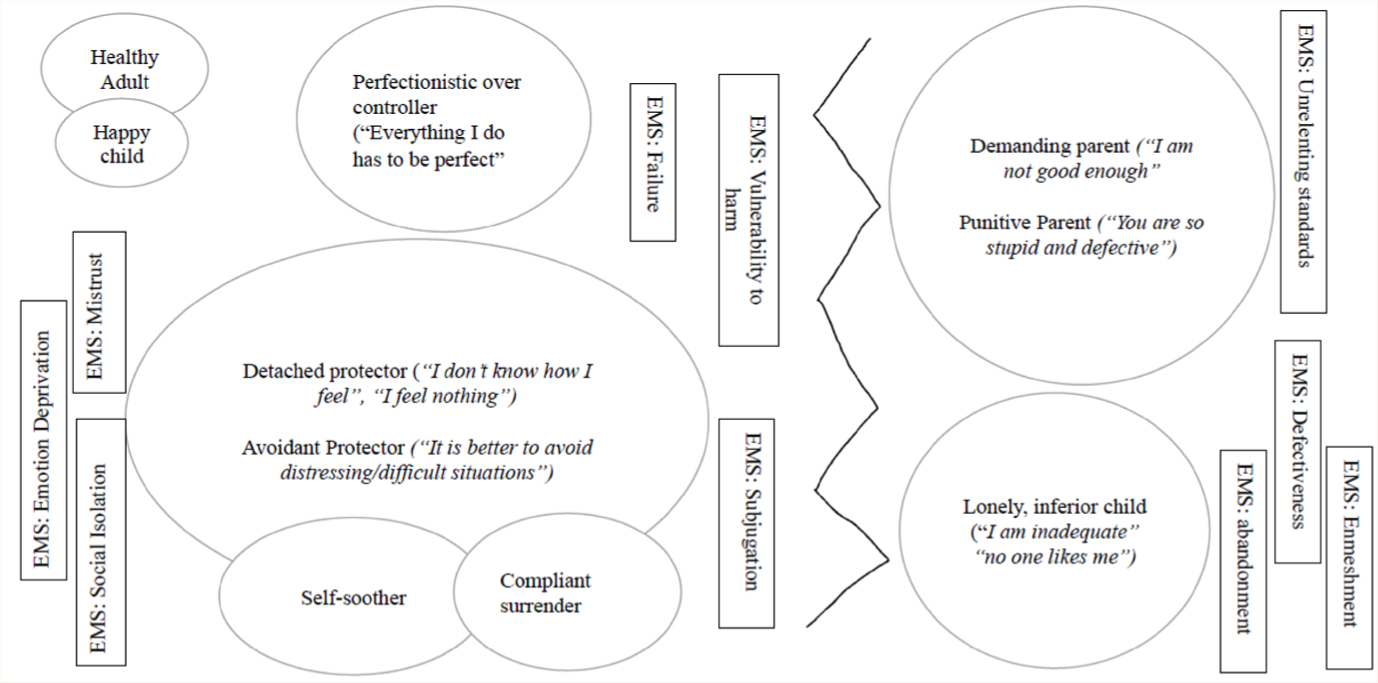
EMS: Early Maladaptive Schema, idiosyncratic schema mode model developed as per the protocol on ST for cluster-C personality disorders. 10
Treatment Plan and Goals
Ms. A was diagnosed with AvPD using the Structured Clinical Interview for DSM-5 Personality Disorders (SCID-5-PD), 18 with a co-morbid major depressive disorder, recurrent episode with moderate severity using the Diagnostic Interview for Anxiety, Mood, and OCD Related Neuropsychiatric Disorders (DIAMOND). 16 She was referred to the therapy unit for treatment of AvPD concerns and entered a trial of ST. She received 45 sessions (5 weekly, followed by 30 biweekly and 10 weekly sessions) and four monthly booster sessions from December ’23 to March ’25. Comprehensive information on the content, course of treatment, and assessment time points is provided in Supplementary Table 1. Although most sessions were held in person, 17 were conducted online. She was prescribed escitalopram (20 mg), quetiapine (25 mg), and clonazepam (SOS), and as required by the larger Ph.D. study, these medications remained unchanged throughout therapy.
The first author conducted all assessments and therapy. Treatment adherence was maintained through monthly supervision by an International Society of Schema Therapy (ISST)-certified ST supervisor.
Course of Treatment and Monitoring of Treatment Progress
The initial sessions explored her concerns and identified the EMS and schema modes. Ms. A entered therapy with a reserved demeanor and communicated minimally. She conveyed her anxiety about therapy, fear of judgment, and tendency toward self-criticism. These behaviors led the therapist to observe her coping and parent modes while maintaining empathy to foster a stronger therapeutic alliance.
‘Something Feels Disconnected’: Detached Protector and Avoidant Protector Mode
Initially, Ms. A presented a factual narrative with little emotion and struggled to recall childhood memories. Her facial expressions reflected fatigue and disconnection. Attempts to address the vulnerability were met with resistance, with the ‘detached protector’ mode dominant (the client being disconnected from, as well as afraid of, her emotions).
Using chair work, this mode was symbolically placed on a chair, and empathic confrontation facilitated access to the client’s vulnerable child mode (representing her innermost feelings/emotionally wounded self).
Ms. A revealed fears about emotional overwhelm: “I am scared if I feel too much, I will not be able to manage that,” and “I cannot feel weaker.” Understanding and empathetically negotiating with this protector mode became key to addressing core vulnerabilities associated with perceived weakness.
In the first half of the treatment, Ms. A often arrived late for sessions, requested more online sessions, and showed poor adherence to her prescribed medication, despite the prescription remaining unchanged throughout therapy, citing lapses in memory and fear of side effects.
At home, she spent most of her time in bed, avoiding activities that she described as being “too much and too difficult,” and reported feeling “horrible” after prolonged phone use. The ‘avoidant protector’ and ‘self-soother’ modes dominated, working together to shield her from distress.
Negotiating with these modes, particularly when they operated in tandem, proved challenging during sessions. Each mode was examined individually through chair work, which revealed its protective functions. Incorporating childhood photographs facilitated her connection with vulnerabilities. Limited reparenting, grounded in genuine understanding and care, made the vulnerable child feel safer. Gradually, diagnostic and safe-space imagery were introduced to regulate emotional arousal and deepen the therapeutic alliance.
‘Taking Two Steps Forward and One Step Back’: Parent Modes Leading to Dysfunctional Coping Mode Activation
Initial imagery rescripting showed promise, but challenges emerged when the therapist accessed her vulnerable (child) modes. Detached or avoidant protector modes began to re-emerge. This was evidenced by the client’s disconnection from the vulnerable child mode during the imagery sessions, including abrupt eye openings, shifts in affect from distress to flatness, and more factual narration of the memory rather than engagement with felt emotions. Consequently, the therapist decided to pause the imagery to address this avoidance. It was identified that the ‘punitive parent mode’ and ‘blaming mode,’ conveying messages of “You are weak,” “Taking help is a sign of weakness,” “You are at fault,” and “You are a burden to everyone,” were becoming dominant. Parent schema modes represent the internalized critical voices stemming from experiences with caregivers who were punitive and excessively demanding. Confronting these parent modes during imagery rescripting resulted in the client experiencing overwhelming guilt. Coping modes were activated in the imagery to manage guilt. Limited reparenting was employed again to ensure a sense of security and validation of her feelings. This facilitated more intensive imagery sessions, allowing access to childhood memories of parentification.
‘Behind the Wall: Unfreezing the Overwhelmed Avoidant and Child Modes’
From the outset, a notable concern was Ms. A’s persistent exhaustion, fatigue, and bodily aches. This hindered her engagement in daily routines and sessions. “When I am stressed, I am not able to move.” “I feel so fatigued and exhausted that I am unable to get up from my bed in the morning.” Initially, this was attributed to her mood, with the expectation that it would improve.
Despite the improvements in mood and overall presentation, her pervasive fatigue persisted. After various attempts to address and process the fatigue, the therapist felt blocked, observing a profound sense of stuckness in the client and within the therapeutic dynamic.
In supervision, what was initially conceptualized as a child mode (of her feeling vulnerable, helpless with distress) was explored to be a more complex internal state, an experience which the client herself referred to idiosyncratically as “The Wall.” This mode functioned as a combination of two existing modes: An avoidant protector mode, shielding her from perceived demands, threats of failure, and judgment, and as a passive, angry child mode, silently protesting for her unmet emotional needs. It represented a frozen, overwhelmed self-state shaped by early experiences of shame, criticism, and emotional neglect. This part of the self appeared to have learnt that collapse and disengagement were the only ways to respond to excessive expectations and early invalidation. “Exhaustion” is the only word learned to express this sentiment. Ms. A described this inner state as a shutdown in which no support could reach her. Empathic confrontation revealed that “The Wall” arose from a punitive internalized parent mode, reinforcing her beliefs of inadequacy and failure. The “Wall’s” function, therefore, appeared twofold: To protect her from further emotional harm through avoidance, and to passively express anger for her needs of care, connection, and acceptance not being met.
A turning point came when Ms. A voiced her fear of recovery: “If I get better, expectations from me will increase, and if I’m not able to fulfil them, I will be a disappointment and criticized again.” With the hypothesis formed during supervision seemingly confirmed, the therapeutic focus shifted to limited reparenting, addressing “The Wall” with warmth, validation, and emotional safety. This involved normalizing her fears, allowing her to express anger in sessions, and affirming her worth beyond achievement. Imagery rescripting was utilized to revisit memories of abandonment, shame, and helplessness, this time incorporating a nurturing figure who could provide the support and attunement she had never experienced before.
Treatment Outcome
As shown in Table 1, Ms. A’s dysfunctional coping modes showed a descriptive downward trend in mean scores of EMS and schema mode by mid and end-treatment. The percentage change reflects descriptive differences in scores between pre- and post-treatment periods. While these descriptive scores help contextualize the clinical process, they are not intended to comment on the efficacy of ST. They add context to the article’s primary aim, which is to detail the process of working with dysfunctional coping modes that were barriers to engagement in and progress in therapy. Although changes were observed in traits related to avoiding social and occupational activities due to fear of rejection, viewing oneself as socially inept, and unwillingness to get involved with others, SCID-5-PD still indicated a diagnosis of AvPD at the end of treatment. Over the sessions, the therapeutic relationship strengthened, and she became more emotionally expressive, both in therapy and with her family. She showed increased openness, initiated discussions about self-conscious emotions, and acknowledged her need for attention and recognition, feelings that had previously embarrassed her. Although coping modes persisted, they were less dominant and continued to require work, particularly through strengthening her healthy adult mode. In an interview post-treatment, the client exclaimed, “I feel like Schema Therapy is right for me and is helping me. It is introspective and compassionate. I am now understanding my feelings and identifying some of them; I’m not avoiding them. I ask for support when I need it, being slightly assertive, I am more positive about the future.”
Discussion and Limitations
This case highlights the critical role of identifying and working with dysfunctional coping schema modes in the treatment of clients with AvPD. ST guidelines emphasize the importance of initially targeting dysfunctional schema modes to reduce their intensity, thereby allowing for greater access to the client’s core emotional needs and vulnerabilities. 8
In this case, early therapeutic gains were achieved by attending to modes characterized by withdrawal, detachment, and emotion suppression. Of particular significance was the recognition that what initially appeared to be only a coping mode was more accurately conceptualized as a frozen, overwhelmed, complex mix of coping and child modes. This mix reflects genuine vulnerability that necessitates validation, reparenting, and confrontation to prevent avoidance. This case highlights the fluidity of schema modes in AvPD, where coping and child modes may overlap. Thus, ongoing attention to the dynamic interplay between coping, child, and internalized parent modes is essential, not only to facilitate deeper therapeutic access but also to manage therapist reactions and maintain attunement. It also highlights the importance of regular therapy supervision and the long-term nature of working with clients with AvPD.
Therapist and Relational Factors
Therapist Reflections: Role of Therapeutic Alliance
The therapist was initially anxious about confrontations triggering the client’s punitive modes. The therapist’s own EMS of self-sacrifice, defectiveness, and unrelenting standards delayed empathic confrontation of the client’s coping modes. By attending to relationship dynamics and embodied countertransference (fatigue and frustration), the therapist recognized that feelings of helplessness were being transferred from the client to the therapist. Processing one’s own vulnerability helped the therapist develop empathy toward herself and the client. This helped her manage the urge to directly confront coping modes while being compassionate about their protective function. This created a safe relational space, allowing the client to slowly recognize her feelings of insecurity, lack of safety, and loneliness. Engaging with the coping mode respectfully and curiously softened defensiveness, revealing glimpses of the vulnerable and wounded self. Similar therapist experiences of helplessness, fatigue, and frustration were reported in Mentalization-Based Treatment for AvPD. 19 This highlights that a nuanced understanding of relational dynamics is crucial in the treatment of individuals with AvPD who have limited access to their own internal states, particularly in the early stages of treatment.
Limitations
As a single-case study, its findings have limited scope and generalizability. The study’s focus on schema modes and the therapeutic relationship limits its capacity to draw causal inferences or to discuss longitudinal post-assessment data. Because the treating therapist administered the assessments without external validation, the possibility of therapist-assessor bias cannot be ruled out. Additionally, the observed changes may have resulted from nonspecific therapeutic factors, concurrent medication, or the overall effects of the therapeutic alliance.
Implications and Recommendations
Implications for Clinical Practice and Theory
Addressing coping modes in clients with AvPD is crucial for effective ST, as it enables access to the vulnerable child mode, strengthens the therapeutic alliance, and reveals the underlying parent modes. It also helps reduce emotional avoidance, prevents misinterpretation of vulnerable states, and supports the development of the Healthy Adult mode, laying the groundwork for lasting emotional integration and change.
Implications for Research
Future research could explore how schema modes, particularly dysfunctional coping and the vulnerable child, maintain patterns of avoidance, emotional suppression, and unmet needs. Examining the effects of mode-specific interventions, such as imagery rescripting and limited reparenting, may clarify the mechanisms of change in ST. Such work could refine ST protocols for Cluster-C PDs and contribute to the development of transdiagnostic models of maladaptive coping.
Conclusion
The primary aim of ST for AvPD is to heal early maladaptive schemas by providing corrective emotional experiences for the inferior and lonely child through limited reparenting and empathic confrontation. Strengthening functional schema modes helps meet core emotional needs, while compassionate engagement with coping modes is key to accessing vulnerability and supporting schema healing.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
The authors assume full responsibility for the entire manuscript content and wish to state that while no part has been written using AI, Grammarly and its generative AI were used while editing the manuscript.
Ethical Statements
The study has received ethical clearance from the NIMHANS Institutional Ethics Committee (IEC)- No.NIMH/DO/BEH.Sc.Div./2021–22.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors confirm that they have secured the necessary patient consent form. This case report pertains to a single patient case, conducted with the endorsement of the relevant department and faculty. The patient consented to both the treatment and the publication of anonymized data.
Prior Presentations
The authors confirm that this case report has not been previously presented at any academic conferences.
Simultaneous Submission to Another Journal or Resource
The authors confirm that this manuscript has not been submitted to any other journal or resource.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.