
Abstract
This article focuses on the ‘internal’ histories of the lunatic asylums in colonial north India. It looks closely at the asylums in the Punjab and the United Provinces. The routinized life of the inmates revolved around ‘employment and amusement’, ‘diet and space’, ‘reform and reward’ and ‘resistance and adjustment’. The trope of the mundane provides a microscopic lens to delve deeper into the banal social lives of inmates behind the asylum walls. Work was emphasized for its therapeutic value but profits were central in order to make asylums self-sufficient. Work, in fact, became the yardstick on which a patient’s recovery was measured, and insanity was conceptualized as curable or incurable. An investigation into diet and recreation patterns helps construct the social history of psychiatry in colonial India. The complex temporal and spatial materialities of everyday lives inside the asylum are studied here in order to comprehend the role played by various actors and discern how authority was constantly reordered and redefined.
I believe that by scrupulous cleanliness, liberal diet, affording them means of recreation or occupation, and attention to the function of body are the foundation of the medical treatment and moral management of lunatics. 2
J.C. Penny, the Civil Surgeon of Delhi, firmly believed in the curative powers of the moral management system. He argued that ‘the insane are not slow in sagacity and the power of comprehending what is done for their good, and thus will appreciate kindness’. 3 The ‘kind’ language of moral management often couched the inherent ‘unkindness’ of the lives of the insane. 4 The moral management system was pioneered by Philippe Pinel, a French physician whose acts of freeing the insane in the eighteenth century at the Bicêtre and Salpêtrière asylums have been regarded as key moments in the history of madness. The principles of moral management aimed to deal with madness compassionately. Hence, the combination of healthy diet, regimented routine and systematic observation was believed to help in curing insanity. It was also propounded that madness had to be disciplined by exercising moral control over the insane.
Moral management was employed in England by Samuel Tuke at the Retreat at York. The Retreat was an asylum built by and for the Quakers in 1796, and it gained repute for the humane treatment of the mad. Robert Gardiner Hill introduced total non-restraint for the first time at the Lincoln county asylum, England. John Conolly popularized the principles of moral management and the non-restraint movement.
5
He was the superintendent of Hanwell, the largest public asylum in England. Conolly paid attention to minute details of asylum life. He regarded time as an important factor in determining asylum regimen and for handling insanity. He stated that
great regularity of hours tends much to break the monotony of private as well as public asylum, and should be strictly attended to. Everything should be performed or appointed or ready at the appointed hours and the tediousness of waiting entirely unknown, as it always leads to complains and irregularities.
6
Control was thus exerted or restored through the regulation of rhythms of everyday life.
The practitioners of moral management gave due importance to time and regarded the system of time management to be therapeutic. The superintendents-in-charge of the Indian lunatic asylums were aware of the principles of moral management. Routine was strictly enforced, as it was believed to have a healthy impact on the mind and body of the inmates. This article attempts to explore questions such as: how did the inmates get attuned to everyday rhythms of life in such closed-door institutions? How did the ‘mad’ live their everyday lives in these alienating spaces? What were the patterns of everyday resistance or acceptance?
Based on primary material available in the National Archives of India (NAI) and the State Archives of the United Provinces and the Punjab, this article takes a closer look at the inner lives of inmates in the asylums of these two regions. While earlier research 7 has focused on the emergence of and the role that psychiatry played in colonial India, this work delves into the micro-histories of asylums. It investigates the routinized lives of the inmates, which often revolved around ‘employment and amusement’, ‘reform and reward’, ‘diet and recreation’ and ‘rebellion and accommodation’. 8 By studying the segmented and the regimented lives of the insane in colonial asylums, this article seeks to unravel how madness and delinquency were managed within the asylum walls.
The broad period covered, from the 1850s to the 1940s, helps in grasping the dynamics of hierarchical relationships. It provides evidence of the connections between the efforts to enforce discipline on the lives of inmates and the problems related to the workings of the colonial asylums. The study of patterns of everyday life would help in discerning relationships of domination, adjustment and resistance.
The article is subdivided into four sections. The first section looks at the relationship between routine, work and discipline. Thereafter, the diet patterns and the significance of food in the mental institutions are explored. The article also looks at the role recreation played in breaking monotony in the lives of inmates in the asylums. The last section throws light at survival and resistance strategies adapted on an everyday level by the inmates and the staff in order to survive behind the asylum walls.
Routine, Work and Discipline
With the emergence of Protestantism, the ethic of work became crucial. Sloth became a sin par excellence.
9
Foucault has argued that, in order to chastise and discipline deviants, the notion of ‘labour’ became imperative. In this sense, ‘houses of correction were economic institutions—a solution for the economic problems. Private entrepreneurs used the labour of asylum inmates for their own profit.’
10
He further asserts that, ‘In Paris several attempts were made to transform the buildings of Hôpital General into factories.’
11
James H. Mills has looked at the issue of labour in the context of the Indian lunatic asylum. He observes:
Work was central to the asylum regime and the inmates were put to a range of tasks in the asylums of India, from attending to the farms established within the asylum walls to performing maintenance around the asylum and even to participating in cottage industry processes such as spinning and weaving.
12
Mills suggests that ‘the political economy that emerged in nineteenth-century Britain redefined the concept of “normal” and “abnormal”. Since labour remained central to the political economy, those individuals who refused to work were regarded as troublesome.’ 13 Furthermore, the discourse on ‘lazy natives’ reinforced the notion that ‘natives’ have to be ‘civilized’ through labour.
Mills throws light on the question of labour in relation to insanity, an aspect that historians have largely ignored. The emphasis on work (and thrift) should be seen against the backdrop of a longer process that was triggered by industrialization and the changing conception of time. E.P. Thompson, in his well-known article, ‘Time, Work-discipline and Industrial Capitalism’, postulates that, from ‘the spread of clocks in the fourteenth century to the Elizabethan age, the notions of time had not only emerged but also led to an advancement of morality related to work ethic’. 14 He further argued that by the beginning of the nineteenth century, the ideas regarding time, work and discipline had become rigid. Thompson asserts that the colonized were regarded as ‘indolent and childlike’. He points out, for instance, that in the early years of the Bombay cotton mills, serious attempts were made to make labour conscious about time and regularity. 15
The lunatic asylums in colonial India were supposed to be philanthropic institutions set up by a benevolent state. Such benevolence, however, was considered to be an onerous responsibility. Thus, the Government of Punjab reprimanded the surgeon general of the Lahore asylum for extending its responsibility to those patients who could easily be kept outside the asylums:
There are a considerable number of harmless lunatics in the asylum whom the superintendent says they are obliged to retain, as, if let loose they could only make their living as wandering mad beggars. This class of patients should never have been admitted to the asylum at all. It is contrary to the frequently reiterated orders of Government of India, which lay down those only dangerous or criminal lunatics, or harmless lunatics in the acute stage, who might reasonably be benefited by treatment, should be admitted into asylums. The police likes to send them there in order to avoid the trouble they frequently experience in consequence of their wandering about.
16
The superintendents of asylums were given the responsibility to keep only two categories of patients, that is, ‘dangerous’ and ‘curable’, while the ‘harmless’ and ‘incurable’ were regarded as particularly burdensome. The asylums had to justify their financial viability. The ‘dangerous’ and ‘curable’ were considered somewhat fitter to perform labour in the asylums than the ‘incurables’. Waltraud Ernst has argued that the asylum system was regarded as costly and efforts were made to make it cost effective. 17 This research places labour within the larger attempts to make asylums a financially viable project.
The turnover of annual profits had become a special feature of the annual reports of the Indian lunatic asylums. A regimented routine was crucial in order to enforce the productivity of this so-called philanthropic institution. The accounts of Indian asylums are replete with examples of the strict regimentation of everyday routines. The Civil Surgeon of the Delhi asylum, Dr Taylor, pointed out:
The whole of the inmates are awoke at about sunrise and are taken out. They go to the latrine and have a smoke if they like, and they go to their work. They have their breakfast at 10 am and rest till about 3; after 3 they go out to work again till 5; then they are bathed and washed, and then have their dinner; after dinner they are talking and smoking till sunset or dark, when they go to bed. They are treated with greatest kindness.
18
Ernst has remarked that
these accounts describe the institutions’ daily routine in almost idyllic terms—the narrative resembling descriptions of prestigious places in England well known for their decidedly humane approach. Although their veracity may be doubted, they can be interpreted as representing part of the rhetoric in which the medical professionals themselves preferred to represent or legitimise their work to the outside world.
19
Ernst is right in her appraisal that the description of ‘the ideal routine’ led to the validation of the superintendent’s medical authority. The routine, on one hand, allowed entrenchment of the authority and, on the other hand, instilled a sense of discipline in the everyday lives of the inmates and the staff. The notions of routine were integrated with the idea of labour.
These asylums often acted like small-scale cottage industries that aimed at self-sufficiency. Attempts were also made to market the products manufactured within the asylum walls. The Government of the North-Western Provinces and Oudh informed the surgeon general of the province that
all the asylums now manufacture a large share of their own clothing and bedding. This industry is [a] somewhat new one in the North Western Provinces, so that one may hope that before long they will be able to supply the whole of their requirements of this kind.
20
G.F.W. Ewens, the superintendent-in-charge of the Punjab asylum, wrote in the triennial report for the years 1906–08:
Though the manufactures carried on in the male asylum are primarily for its actual maintenance requirements, a small gang of men in excess of those so required, is employed on making munj matting for which there is great demand, far in excess indeed of what can be turned out were more men available, while others cut the grass growing on the asylum land in the summer which sells readily, and a profit of some Rs 2,831, Rs 2,908, Rs 1,041 in the three years, respectively, was made in this way…
21
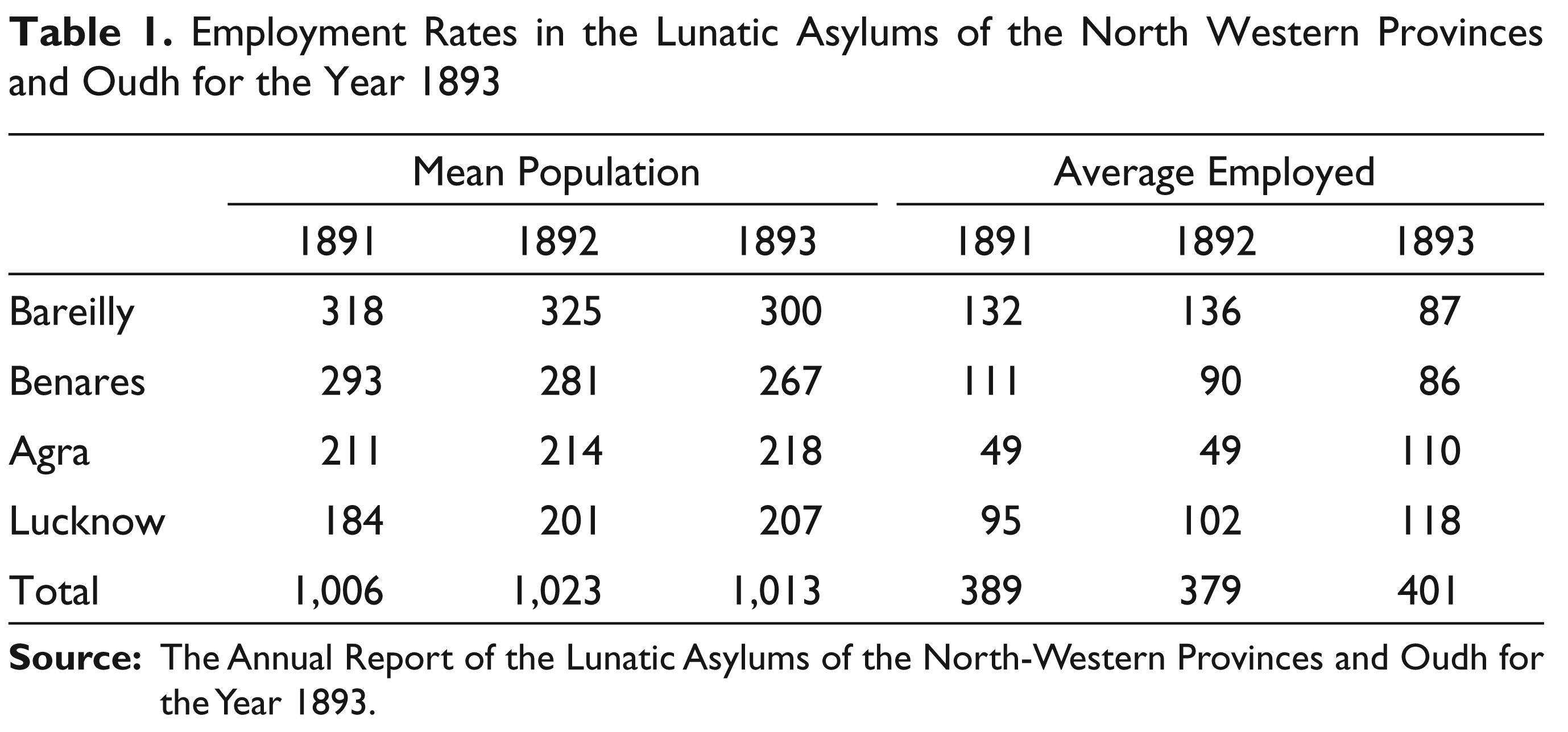
The inmates performed a variety of tasks. They worked in the garden, cooked food, weaved blankets and even cultivated land. Gender-based division of labour was prevalent. Women were occupied in spinning, weaving, cleaning and cooking. Men were employed in manufacturing, cleaning, cultivating land and work related to dairy farming. A look at the asylum statistics of employment and profit would allow us to further understand the way in which the system worked. The Report on the Lunatic Asylums in the North-Western Provinces and Oudh for the Year 1893 provides us with the information given in Table 1. 22
The table reflects the attempts made by the authorities not only to show the rates of employment, but also to record the efforts put in to engage the lunatics in useful work. This was necessary to justify the existence of these institutions.
Employment Rates in the Lunatic Asylums of the North Western Provinces and Oudh for the Year 1893
By the beginning of the twentieth century, a system of rewards was formalized. The inmates were not only given incentives in the form of additional allowance of food, but monetary rewards were also offered to maintain the stability of the labour force. The inspector general of the civil hospital, Bengal, wrote to the secretary of the Government of Bengal:
[This] system is in the force in the Dullanda and Patna Asylums. At the former a sum of Rs. 2 is distributed every month to two such lunatics one of whom is a good weaver and the other a good worker in the store godowns. The superintendents say that the system has been successful in encouraging lunatics to work. At Patna one rupee is at present drawn from the treasury and distributed among the hardworking and well-behaved lunatics, who spend the amount in buying sweets, fruits, etc., for themselves.
23
Experiments with new forms of crops and products for marketing were also not uncommon. Dr Scriven, the superintendent of the Lahore asylum, noted in the annual report for the asylum that
a small number are employed in manufactures which have never been very profitable in this asylum…the following articles have been made: 188 blankets, 276¼ yards garrah cloth, 16 darrees, 7 seers 1 chattak newar, 54 reed chicks, 113 kilchee as kets, a maund 7 seers cotton thread, 17 yards doossuttee cloth, 8 moonj pardahs and 38 seers 3 chattaks munj ropes and twine.
24
In Delhi, the land near the lunatic asylum was reclaimed and crops were grown through the efforts of the inmates. Dr Fairweather wrote in 1879:
The lunatics have been employed in the same way as last year. Their heaviest piece of work has been reclaiming the waste land belonging to the asylum. This was begun about two years ago, and two third of the field have now been trenched to a depth of 3 feet: and 2, 360 cubic feet of large stone have been taken out of it during the year. The crop off this ground fetched Rs 44 during the hot weather and it is now being planted with tobacco, which it is hoped will bring a considerable sum.
25
From this period onwards, manufacture and hard labour became an integral part of life of the Delhi lunatic asylum.
A huge dairy farm was maintained at the Bareilly asylum. As the Annual Report of the North-Western Provinces for the Year 1891 noted:
This important farm, which was started at the close of 1890, and is separately reported on, has, under the able management of Dr. Anderson, proved an unqualified success. On 31st December 1890 the stock, excluding calves, consisted of 69 cows and 4 buffaloes, which supplied the whole of the milk necessary for the Station Hospital and for Officers’ Mess, 1st Hants Regiment. The surplus milk and butter were sold to individual purchasers, the balance sheet showing a net profit at the close of the year of Rs 4008. It is probable that during 1892 the debt of the Military Department will be paid off, when the net receipts will form part of Provincial revenues.
26
These experiments sometimes met with success but mostly failed. The dairy farm was closed down in 1908 due to high mortality rates among the cattle. 27 However, what remained consistent were the efforts to make these institutions as profitable as possible.
Jennifer Laws has analyzed Western notions about madness and the therapeutics of work. Her research spans the period from the nineteenth century to the twenty-first century. She points out that it was the moral management system that emphasized the significance of work and its related efficacy for curing insanity.
28
Samuel Tuke in the York Retreat promoted employment of the insane for inducing recovery. Laws further states that work, however, was not the sole basis of cure at the York Retreat. Rather, the holistic organization of time based on the principles of ‘work, rest and worship’ was the cornerstone on which notions regarding cure rested.
29
She further notes that the
professional organization of ‘occupational therapy’ did not begin until the mass return of shell-shocked soldiers at the end of the First World War, and the term ‘occupational therapy’ was not coined until 1914 at a professional meeting in New York. The movement arrived in Britain a decade later, when Scottish-born Margaret Fulton became Britain’s first qualified occupational therapist at the Aberdeen Royal Asylum.
30
The moral management system regarded work as being essential for restoring sanity. The occupational therapist, too, relied heavily on work ethic. Occupational therapy was more, in a way, a product of the war economy. Moral therapy structured cure around the notion of time and work.
The limited nature of psychiatric infrastructure made asylums a place for profit earning and experimentation. This is not to deny the belief that work was considered therapeutic. The rhetoric differed dramatically from reality since, in the absence of poor laws, asylums in India became substitutes for institutions for poor relief, as throughout the nineteenth century asylums were peopled by the poor. David Arnold has looked at the issue of poverty and state-sponsored poor relief in colonial India. He remarks that ‘the 1837–1838 North Indian famine saw a widespread use of such terms as paupers, vagrants and the able-bodied and deserving poor (emphasis in original) that echo poor law legislation in Britain. But despite this rhetoric, there was extreme reticence about adopting similar measures in India.’ 31 This reluctance was due to the fact that the colonial state was not willing to take responsibility for the Indian population. Arnold pointed out the argument at the time that ‘while poverty and nakedness were universal in India, this did not signify the same degree of suffering as in Europe’. 32
The belief that the insane could be disciplined with labour continued to hold grip on the asylum personnel. The Triennial Report on the Working of the Punjab Lunatic Asylum, Lahore, for the Years 1912–14 noted:
[I]t has been found that the insane is very much better controlled and more amenable to discipline when he can be induced to take up some form of avocation, [and] of these there are many in the asylum. All the cooking, washing, weaving, mulling of blankets, cleanliness and the endless varieties of occupation common to an asylum, are carried out by the inmates. The larger number of whom are chronic maniacs. They are often good, harmless workers, who under supervision perform most of the ordinary duties of the institution, and without whose presence a vastly multiplied staff of attendants and servants would be necessary.
33
These so-called voluntary activities were tiresome and competitive. One can also witness a continued hankering for experimentations in the twentieth century. Charles J. Lodge Patch, the superintendent-in-charge of the Lahore asylum, mentioned:
The asylum gardens used [to] formerly compete in the annual horticultural shows held in Lahore. In 1913 an exhibit was sent to the show in which every vegetable presented some abnormality. In that year as well as in 1914 and 1915, the asylum won the second prize, and in 1916 the first prize for vegetable gardens. Since then however, government gardens are no longer allowed to compete in these exhibitions but the institution can still hold its own with any other garden in Lahore. In 1929, for the first time, an experiment was made to grow rice. The suggestion was Dr. Sharma’s and the object was not so much to provide the patients with particular grain as to obtain large amounts of straw for the bedding of animals and those dirty and destructive patients who destroy every article of clothing which is placed within their reach. The experiment has been an unqualified success, and it is no longer necessary to purchase straw from the slender budget grant allotted for clothing and bedding.
34
These experiments can be regarded as constant attempts to make these institutions financially viable. They reveal the limited nature of psychiatric infrastructure. The disciplinary aspect of asylum life can be discerned, as a reform-like zeal was present in these novel ideas. Self-sufficiency of these institutions was a desired aim but it was hardly ever met.
Much before the birth of occupational therapy, the professionalization of ‘insane’ labour occurred in the Indian asylums. Lodge Patch mentioned that
the term ‘Occupational Therapy’ is comparatively recent in medical literature, but occupational therapy has been carried out in a practical manner from very early times in the asylums of the Punjab. The occupations and vocations on which the patients are engaged have been enumerated at length in the Annual Report for 1866 (page 28) and these have continued down to the present day.
35
Work was the index by which a patient’s recovery was measured. Patients who had the ability to work were declared ‘improved’ or ‘cured’. According to G.F.W. Ewens:
In some of the cases their insanity has for one of its symptoms the utter refusal to do anything whatsoever, but in all the first step towards recovery is taken when they can be induced to occupy themselves in some way, and the benefit both to themselves and coincidently to the institution is incalculable. It would, of course, be impossible to work the asylum with its present staff and at its present cost without a large number of its inmates being employed in its actual maintenance, and thus the cooking, cleaning, sweeping, washing, & c., employs a good number. The large garden also provides an excellent and healthy form of labour for many…Nothing is more striking than to note the gradual improvement in a man once induced to labour, or to see an acute maniac raving, shouting, gesticulating, tearing everything within his reach, soften down, after a few days’ violent exercise at mulling blankets, into a quiet and reasonable patient.
36
This vocational economy of asylums sustained the asylum’s system throughout the colonial period. The notion of work became a key principle for the treatment of the insane. However, in these circumstances, cure often became coercion and therapeutics turned out to be hard labour. It has been argued elsewhere that ‘From clothing to bedding and from diet to treatment nothing was “free of charge”; since the inmates had to actively work to run these institutions.’
37
At the same time, ‘it was believed that European insane persons of any social class in India would debase themselves by carrying out tasks which the natives could do. In the colonial context, work was impracticable, if not “injurious to Europeans”.’
38
Jonathan Saha has worked on the Rangoon lunatic asylum and has aptly argued that
the asylum was a neglected institution, which was improved only episodically following internal crises and public scandals: it is an example of the general indifference of the colonial regime towards insanity and the insane. The general neglect of the mentally ill can be regarded as a salient feature of colonial psychiatry.
39
Daily Diet
Ashraff Khan, the criminal lunatic, on one occasion, in the hot weather refused to leave his sleeping ward until he has seen me, and I found the reason was that he has been cheated of his proper quantity of food by the jemadar 40 whom he still looks upon as his enemy, and who he believes wishes to kill him. He first asked me the weight of the bread and dal which he ought to get, and on being told this he brought out the whole of his previous day’s ration, which he had hidden away in the corner untouched, and requested that it might be weighed there and then. Fortunately both the bread and the dal, although they had kept so long, were rather over the prescribed weight. He was quite crestfallen at the result, but apparently satisfied. 41
The incident shows that food occupied a significant place in the daily lives of the inmates. It also reflects the inner struggles of the asylum life that were often coalesced around food. Ashraff Khan was sane enough to keep his previous day’s food and question the authorities. Food was given in limited quantity and the insane often felt its meagreness. This section elaborates upon the diet patterns and significance of food in the daily lives of the insane.
Proper sleep, healthy labour and nutritious diet were considered to be the main principles of moral treatment. Samuel Tuke, in his book Description of the Retreat, underlined the fact that in the York Retreat food was given three times a day and included milk, bread, porridge, animal food, bread and beer. Tuke believed that diet was an imperative part of treatment and he asserted that the diet in the Retreat was ‘more liberal than judicious’.
42
Robert Gardiner Hill, the superintendent of the Lincoln lunatic asylum, was a great proponent of the non-restraint movement. He, like other advocates, averred that a
generous diet implies a daily supply of animal food with different vegetables, varied as much as possible, and supplemented from time to time with fish, fruit, and farinaceous compounds—well cooked and well served adequate proportions, so that no one at the conclusion of the repast shall be able to say that he has not had enough.
43
Leonard D. Smith has researched early nineteenth-century asylums in England and he states that ‘asylum food exemplified the interface between principles of economic management and those of curative treatment. With the improvement of physical health deemed an essential element in the restoration of mental health, patients’ diet was a central part of the treatment armoury.’ 44
Ernst’s investigation into the ‘native’ asylums showed the importance of diet in the treatment regimen of Indian asylums. She argued that ‘…a balanced dietary regime was seen as an important constituent of traditional curative and preventive medicine, but food supplies were insufficient and unwholesome’.
45
The officials in charge of the Indian asylums were well aware of the significance of diet in the moral management system. C.M. Smith, the superintendent of the Lahore asylum, pointed out in the annual report for the year 1868 that
every attention has been paid to the diet; the rations are inspected and passed by the deputy superintendent, both in their raw and cooked state. The meals have been issued at regular hours twice a day, and the same order and decency of conduct during meals has been enforced.
46
Food was given twice a day; breakfast was served at 9 a.m. and supper at 5 p.m. Contrary to the suggestions of pioneers of giving three meals, only two meals were offered at strictly regulated timings in the Indian asylums in the nineteenth century. These meals consisted of vegetables, rice, wheat, milk and ghee (clarified butter). Mutton was issued twice a week in summer, and in winter, three or four times a week. 47 Milk, ghee and rum were usually given to convalescents. Fruits and sweetmeats were given on festive occasions. 48 The diet was given in limited quantities. Men were given 10 chittacks, 49 while women were given 8 chittacks. Throughout the nineteenth century, the quantity and the quality of diet were not standardized; it depended on the superintendents’ and the local government officials’ understanding of how to qualify and quantify the diet of the inmates. Therefore, the expenses related to diet differed from one asylum to the other.
The diet regimen came under scrutiny only if the mortality rates were high or the cost of food was exorbitant. Ernst has discussed the case of the Benares asylum in which the average death rate was 36 per cent during the 1840s. An enquiry into the matter revealed that ‘the rate started rising to 8 percent in excess of that of the preceding years when daily allowance of atta, the main staple food, had been reduced to nearly half the former amount in 1844’.
50
Other times, the ex-officio visitors sometimes made criticisms and highlighted problems. Conditions in the Delhi asylum, for example, came under governmental scrutiny in the year 1871. The visitors, comprising the Inspector General of Hospitals and Inspector General of Jails, highlighted the inadequacies and, among other complaints, an objection was made to the diet scale. They noted that the food given to inmates was inadequate. Dr Taylor, the superintendent-in-charge of the Delhi asylum, stated in the annual report for the year 1872:
Both Dr. Tresidder and Dr. Dallas [visitors] have recommended an increase in the quantity of ghee and salt, and that the rice and dall comprising Friday’s diet from eight to ten chittack. In this I quite agree, and I have given the order for increase in anticipation of its sanction. I am of the opinion, after having most carefully watched the cases for last eight months, and the death rate would be reduced by a more liberal dietary, I think the female ones should have as much as the males…
51
The statistics showed that the next year, the mortality rate dropped to a considerable degree. Nevertheless, the diet was barely sufficient as, even after this limited increase, Dr Taylor remarked that he was ‘anxious to be allowed to increase the diet of the lunatics’.
52
He also pointed out that women were given less food in comparison to men. For the next two years, Dr Taylor reiterated the urgent need to increase the diet scale of the female inmates. In the annual report for the year 1874, Taylor had the following to say:
The diet scale is the same as it was last year. I think that the women should have more food. I recommended last year that they should have the same quantity as the male. I understand that in the North-West Provinces the allowance of flour is 12 chittacks per diem for both male and female; here it is 10 chittack for the former and 8 for latter. This is not enough I fear, and the high death rate of the females, contrasted with the very small mortality among the males, renders me very anxious to be allowed to increase the amount of the former food. The women and men both complain of not having enough food, but I think, though the men both could and would eat more if they could get it, the women are only in absolute want of an increase.
53
It was only after Dr Taylor’s incumbency that the diet scale of females was increased from 8 chittacks to 10 chittacks. 54 Taylor disregarded men’s complaints of ‘not having enough food’ and their diet remained unaltered.
Numerous attempts were made to economize expenditure in the lunatic asylums. The ramifications of this economizing drive had a serious effect on asylum food. The expenditure on food in asylums was considered to be excessively high, especially when compared to that on food in the jails. J.B. Scriven, the superintendent of the Lahore lunatic asylum, was of the opinion that ‘the food has been much more expensive than the jail food, as meat is supplied in small quantity every working day. We calculated some months ago that if the meat were cut out the food would cost nearly the same as the jail food.’
55
Such comparisons show how jails and asylums were invariably linked in the official discourse. This would have had an effect on determining the dietary scale of the asylums. The superintendent-in-charge of the Lahore asylum pointed out that
on comparing the dietary of this Asylum with that of other establishments of the same kind in other parts of the country as well as with the dietary of Punjab jails, I discovered that the allowance of ghi and fatty matter was much smaller than in these. On representing this through the surgeon-general, Punjab, the allowance of ghi was raised from 1/5 chittak to 1/2 chittak per head during the colder months of November, December, January and February.
56
The moral management movement preached kindness and humanity. An important principle of the system was that lunatics should be treated as patients and not as criminals. The practice of sending lunatics to jail was largely discarded in England. However, the ideals of the non-restraint movement were never practised in their totality in India. Lunatics were generally treated as ordinary criminals and insanity was virtually a criminal offence in colonial India. As W. Walker, the officiating surgeon of the Government of India, put it:
It hardly needs to be pointed out that the vast majority of the lunatic[s] confined in the asylums are paupers and criminal lunatics; and the first principle to lay down is that in all cases in which the pauper or criminal lunatic is in sound physical health, there is no need to treat him to any large extent differently in matters of diet, clothing & c. from one of the free population, or from prisoner in the same class of life in our jails. It is no doubt difficult to draw the line in case of mental disease between a condition of sound and unsound physical health; but this is not so difficult as to necessitate that every pauper insane and every criminal lunatic in an asylum should be treated as a patient in [a] hospital. If the lunatic or his friend can pay for his support, the case is different; but as long as he is a pauper in sound physical health there is no reason why he should live more luxuriously in a lunatic asylum than he would in his own house. This principle is acted upon in all European asylums for the insane.
57
The monotony of the institution gave food a special place in the lives of inmates. The officials were well aware of this fact, and therefore used food to control the behaviour of inmates. Food items such as fruits and sweets, and even stimulants like tobacco and cigarettes, were used to induce the lunatics to perform hard labour. 58 This approach of ‘reward and punishment’ was integral to the moral management system. Leonard Smith has pointed out that in the English asylums, ‘patients “actively employed” in the asylum or its grounds received extra diet’. 59 The superintendent-in-charge of the Delhi asylum remarked in this context that ‘on Sunday all are treated to either sweetmeats, or fruits in their season. This treat is looked forward by them, and in the cases of misbehaviour it is withheld as a means of punishment.’ 60 The superintendent was setting an example by withdrawing food as a form of punishment. This policy of reward and punishment was monetized by the beginning of the twentieth century when food items were replaced by monetary stipends.
The social distinctions around caste and religion were also practised around food habits. The James Clark Enquiry probing the conditions of the asylums was conducted in 1868. 61 Information regarding the different ranks and castes of the patients in the asylum was solicited. The superintendent-in-charge of the Nagpore asylum stated, ‘No distinction is made between the different ranks and castes in the asylum. Disregard of caste is one of the most common characteristics of insanity among natives.’ 62 The superintendent of the Patna asylum, on the other hand, stated that ‘the two divisions of Hindus and Muslims are recognised, different cooks and water carriers being provided for the two classes’. 63 Many of the asylums provided different cooks for Hindu and Muslim communities. Moreover, a high-caste Brahmin cook was often hired in order to avoid complications rising due to caste prejudices. According to the Hindu caste system, a high caste should not eat anything from the hands of the lower castes. Disregarding caste-based practices was common among the insane. However, there exist a number of instances when the insane belonging to the higher caste refused to eat food cooked by the lower caste or from people belonging to other religious backgrounds. This was often regarded as a symptom of their sanity. The superintendent-in-charge of Moydnapore asylum stated that ‘it is always an indication of returning sanity when in case Hindu patients begin to exhibit caste prejudice’. 64
The caste distinctions were supplemented with class privileges in the twentieth century. C.C. Manifold, the Inspector General of Civil Hospitals, United Provinces, noted:
During the year arrangements were attempted at Agra whereby the better class of Indian patients who can afford it could be admitted into the asylum paying Government charges and defraying all diet expenses and in some cases, providing private attendants, punkhas, &c. These cases have had their own special cooking arrangements and caste prejudices and customs could be fully complied with.
65
Food invariably differed when offered to patients belonging to European and Eurasian races. G.F.A. Harris, the Inspector General of Civil Hospitals of the United Provinces, mentioned that ‘[t]he cost of dieting a European lunatic has, under the orders of Government, been recently fixed at Rs. 30 a month’.
66
No special mention of such kind occurred in case of the ‘native’ lunatic. Saadat Hasan Manto’s famous story ‘Toba Tek Singh’ is set in the mental hospital of Lahore. He interestingly describes the moment when news of the Partition reached the lunatic asylum, leading to quite a commotion. Manto narrates:
In the European ward there were two Anglo-Indian lunatics. When they learnt that the English had left after granting independence to India, they were deeply shocked. They would now spend hours in secret confabulation about their changed status in the asylum. Would the European ward be there or done away with? Would they be served breakfast anymore? And, instead of Western style bread, would they be forced to swallow the ‘bloody Indian chapatti’?
67
Food remained at the heart of the system. The moral management system had only few tools, which included control of the environment surrounding the lunatics and the use of therapeutics. The patient, therefore, had to be disciplined through the few available viable means. Food helped in controlling the behaviour of the inmates and it also became a significant way of expressing care and kindness. At the same time, refusal of food by inmates was a common problem. A.W. Overbeck Wright, the superintendent of the Agra asylum, noted that ‘Delusions are common, and may lead to refusal of food, so that tube-feeding becomes necessary.’
68
Ernst, in her recent work, has pointed out that
Refusal of food was not uncommon at Ranchi and it was always responded to by forced feeding. Cruel as this may sound to modern observers, it was a practice that was considered not only fully appropriate at the time but also a strictly medical procedure, just as bleeding or blistering had been in earlier periods.
69
Diet was considered a vital part of the treatment regimen even in the twentieth century. Overbeck Wright, while describing the significance of diet, wrote that
[t]he diet should be at first light, but ample and nourishing, milk, farinaceous foods, fish, chicken, soups, etc., being given in as large quantities as the patient can be persuaded to take. When recovery is well begun, ordinary full diet should be freely given, and if possible some of the malt beverages, such as beer and stout.
70
However, as we have seen, food was given in limited quantities. Ernst aptly argued that
the art of economising on food provisions lay in the drawing up of high provision bills which matched an equally sophisticated—though not blatantly exaggerated—diet plan, on the one hand, and the distribution of low-quality food in low quantities to the patients, on the other.
71
Andrew Scull has pointed out that somatic treatments played a crucial role in the history of psychiatry. He remarked that ‘therapeutics, the translation of abstract knowledge into socially acceptable recipes for intervention and practical action, necessarily remains close to the heart of the medical enterprise’. 72 Food should be regarded as a significant therapeutic, more so in the absence of other concrete methods of treatment. Most of the patients came from the poorer sections of the society and suffered from impoverishment. A regimented diet helped these patients to recover from diseases related to malnourishment. Food also became a way through which care and treatment was extended. It occupied a significant place in the asylum’s inner life since mundane struggles around caste, religion, race, labour and treatment (refusal of food/forced feeding) revolved around the dietary regimen.
Recreation
Recreation, along with labour and diet, was considered to be therapeutic, as various forms of entertainment broke the monotony of the patients and enabled the inmates to relax. Dolly MacKinnon has argued that ‘providing entertainment combated the effects of institutionalisation. Entertainment and recreation gave selected inmates normal experiences of the outside world “inside” the asylum walls.’ 73 This section looks at the forms of recreation made available to inmates in north Indian asylums. Amusement was an essential part of the moral management system and therefore it was considered to be a part of the treatment regimen. Entertainment was provided to the inmates along the lines of race and class. In the nineteenth century, European patients were provided with amenities of superior quality, whereas Indian patients were provided inferior facilities. By the turn of the century, superior facilities were being provided to those Indian inmates who could pay for them.
The James Clark Enquiry had an interesting question regarding whether there was a dining room or recreational hall in the asylums. J.C. Whishaw, the Civil Surgeon of the Cuttack asylum, responded that ‘the patients dine—as almost all natives of Hindoostan dine—in the open air. When it rains they dine in a covered shed. There is no recreational hall.’ 74 Many of the other superintendents pointed out that they strategically used the work shed as the dining floor. The question of a recreational hall or space for recreation was raised again by Robert Harvey in 1899 and Jameson in 1922. 75 Throughout the colonial period, recreational spaces were improvised by appropriating spaces intended for other purposes (work sheds and so on), but were rarely built specifically for recreation.
Entertainment was considered to be a significant part of the official regimen. Dr Fairweather, the superintendent-in-charge of the Delhi asylum, noted that
every inducement is given to the lunatics to amuse themselves in any way they can, and for this purpose kites, toys, tom-toms, sittars are provided for those who care for them. The women have pet pigeons, rabbits and lambs; swings are erected for their amusement.
76
A wide array of recreation was offered to the Indian and European patients. G. Hutheson, the Inspector General of Civil Hospitals of the North-Western Provinces and Oudh, stated in the annual report of 1899:
different sorts of games, musical instruments, etc., were provided for natives; and books, papers, etc., procured for the European lunatics. In Bareilly, one of the European female lunatics was allowed out of the asylum for exercise. On festivals sweetmeats, fruit and extra diet were issued. The general effect of such indulgences was beneficial.
77
The insane were taken out for rides on special occasions. Dr Penny stated: ‘I borrowed the Municipal carts and sent them in a general procession, all dressed in their best. They went to Ram lela and Dewallee in my presence, and it was delightful to see the sympathy they met with from the passer[s]-by.’
78
Entertainers were hired to perform in the asylums. According to D. O’C. Raye, the Inspector General of Civil Hospitals, Punjab asylum:
The Superintendent of the Delhi Asylum mentions that, having had a small sum of money placed at his disposal by the Deputy Commissioner, and by some generous native gentlemen, he was able to give to such of the lunatics as were capable of enjoying it the amusement of a weekly nautch. He engaged a couple of bazár minstrels for this purpose. Dr. Dennys writes that he was much struck with the soothing influence which this native music seemed to have on some of the refractory and troublesome insanes; and he considers that the experiment was a success, not only by giving some enjoyment to a number of pitiable and unhappy lives, but also by having an actually beneficial effect on the mental state of some of the sufferers.
79
Nautches (Indian dance and musical performances) were at times considered beneficial, but at other times, they were regarded as injurious to the mental health of the inmates. Ernst has pointed out that some officials considered these nautches to be harmful. 80 The effects of nautches were debated but they were never banned. A report on the lunatic asylums of the United Province stated in this context that ‘amusements of various sorts (performances by jugglers, acrobats, minstrels) and native entertainments were provided for the lunatics’ on a regular basis. 81
A number of physical activities such as various games and different forms of physical exercises, including walks, were also introduced. In the words of G.F.W. Ewens:
Some of the sane men have built themselves little praying platforms, and all are allowed to keep religious books; means for gymnastics are provided though rarely used; a native paper is taken in, and in addition to various native games the asylum possesses a gramophone and magic lantern. Tobacco is amply provided, and at all the native festivals and at Christmas issues of ‘sweet rice’, fruit and sweetmeats are made, and native jugglers and rag-doll performers engaged. A sanctioned allowance of 10 rupees monthly is divided in rewards among the best workers and keenly appreciated, while there are facilities arranged with the contractor for spending this and any other private money their relatives may have provided them with. In short everything possible is done to make their existence as easy as possible and their surroundings pleasant, and it may reasonably be claimed that they are as comfortable as they can be made.
82
Religious activities were encouraged and the inmates were allowed to practice the rituals of their respective religions. Further, as discussed earlier, rewards were monetized by the beginning of the twentieth century. The opening of shops within the confines of asylum walls was a reflection of this increased amount of monetization. Such facilities allowed inmates to spend their money, but in order to buy items from the shop, they had to work hard or else they had to depend upon their relatives for monetary resources.
The forms of recreation underwent transformation between early to and mid-twentieth century. G. Tate, the Inspector General of Civil Hospitals, noted in the triennial report of the United Provinces for the years 1924–26:
recreation is also arranged for Pachisis, satranj, cards, and so on, were provided in every section. Sing songs with dhols and manjiras find great favour on Sundays while healthy and regular exercise is obtained by foot-ball, tennis and walking, etc. in the ‘better class’ section. The Fauji Akhbar, Vakil and Bharat-Mitra as well as books are purchased for the sections. Nautch-girls come round occasionally and visit all the sections singing and dancing in each.
83
In the 1930s, the patients began to be taken out for motor rides. Charles Lodge Patch, the superintendent of the Punjab hospital, was of the opinion that:
more than anything, the patients appreciate drives in the motor bus; but in spite of frequent renewals of spare parts, the bus is threatened with signs of a complete break-down, and the question of its renewal will have to be considered within the next year or two.
84
Modernization occurred not only in forms of emulating new techniques of treatment and entertainment but also in adapting to ‘class-based’ arrangements. From the beginning of the twentieth century, the number of patients admitted in these asylums had increased. The government tried to make these intuitions more amiable for the paying patients. In 1910, a regulation was passed which allowed the paying patient to keep an extra attendant at the cost of their family or friends. 85 These patients belonged to the middle classes and a new set of arrangements was introduced to cater to their specific needs. Ernst has observed that ‘the British class system had its equivalent in the highly stratified Indian caste system, and in divisions made along lines of religious, cultural, regional and class affiliation’. 86
The standards of the mental hospitals were improved by allowing a better arrangement for the class of paying patients. From the late 1920s onwards, electrification of the asylums had taken place. The triennial report for the mental hospitals in the United Provinces for 1936–38 lauded the efforts for ‘[the] establishment of fiction library for patients…[and the] provision of Radio sets’.
87
Moreover, ‘at the Mental Hospital Agra the patients and the staff had formed teams in the year 1941 by the name of the Menthosp Club. These teams played several hockey and football matches with the local team.’
88
D. Clyde, the Inspector General of Civil Hospitals, Punjab, noted in the annual report for the year 1945:
Certain games and articles for amusement are supplied to the patients. Patients are taken out [for] a walk daily in the morning and evening and are also taken to cinemas. Messrs. Mehra Brothers and Narain Dass of Lahore each continued to supply 7 gallons of petrol free of cost for the running of the bus of the hospital and the proprietors of the following cinemas showed their generosity by issuing free cinema passes to mental patients. 1. Nishat, 2. Palace, 3. Regent, 4. Prabhat, and 5. Ritz.
89
The nature of amusement underwent change not just because of changes in technology but also due to the transformation that was occurring within and outside the walls of the asylum. Since the beginning of twentieth century, numerous attempts were made to disseminate information about the asylums. The changing character of these mental hospitals attracted not only paying patients but also voluntary donations and voluntary help. According to C.C. Manifold, the Inspector General of the Civil Hospitals of the United Province:
A small concert is arranged fortnightly by the staff assisted by their friends which is much enjoyed by the inmates. A Christmas tree was provided and a special dinner and tea for the occasion. This year a donation of Rs. 40 was subscribed by members of the Telegraph department at Agra, and a tennis and badminton party with a string band helped considerably to make a bright and memorable occasion for the European inmates.
90
In England, as well as in some other British settler colonies such as Australia, asylum balls were a common feature. Dolly MacKinnon has suggested that ‘entertainments forged important political and social links between the invited guests and the institution’. 91 In the Indian context, lavish balls were never part of the recreational plan, but by the twentieth century, the asylum walls became permeable as local communities, groups and notable dignities of the city were expected to do voluntary work for these institutions. Recreation was a crucial part of everyday life in the asylums. It rejuvenated not only to inmates of the asylum but the staff as well.
Everyday Lives: Patients and Personnel
Erving Goffman, in his work Asylums (1961), has pointed out that ‘each grouping tends to conceive of other in terms of narrow hostile stereotypes, staff often seeing inmates as bitter, secretive and untrustworthy, while inmates often see staff as condescending, highhanded and mean’. 92 He argued that the people at the bottom of hierarchy were usually more dissatisfied with their jobs and the ways of life than the high-handed officials who cherished their privileges and work. Thus, they would utilize their circumstances, legitimately or illegitimately, in order to meet their ends. Goffman interpreted these everyday adaptations involving ‘unauthorised means’ to meet ‘unauthorised ends’ as secondary adjustment. 93 For Goffman, the primary adjustment is a process through which an individual transformed himself into a co-operator; 94 Goffman calls this the ‘underlife’ of the mental institution. This underlife could at times be marked by violence. In a volatile form, the inmates try to upset the structure, whereas in a ‘restrictive’ form of life, the inmates attempt to make small adjustments by subverting the regimes. It may be noted here that in the mental institutions, the subordinate staff and the patients were approximately at similar levels of hierarchy. They lived their underlives at the individualistic and social levels. The staff could do this secondary adjustment secretively or with selective members of the staff. They could also, at times, engage patients to meet their ends, or the patients could assimilate with some members of the staff in order to fulfil their aims. These situations were much more feasible in the mental hospitals than in other institutions because of their isolated nature and drab way of life. This section tries to reconstruct the ‘underlife’ in the colonial north Indian lunatic asylums. Goffman’s hypothesis gives us an insight into the multiple layers of entangled lives of the patients and the staff.
R. Charles Macwatt, the Inspector General of Civil Hospitals, Punjab, noted in the annual report for the year 1918:
There has been in 1917, one death from an overdose of opium in a criminal and there is strong reason to believe that the drug was self-administered owing to grief following the death of the man’s wife. In this connection, it may be mentioned the great difficulty, nay, the impossibility of preventing the surreptitious entry of toxic drugs through the agency of the attendants and sweepers. Regular searches are conducted of all such leaving and entering the asylum, but it is obvious that small parcels such as these drugs readily escape detection.
95
H.W.V. Cox, the superintendent of the Punjab lunatic asylum, also had the same problem:
in this connection it may be mentioned how futile our precautionary measures are for preventing the entry of toxic drugs through the agency of asylum servants, when it is pointed out how easy it is to introduce such drugs by simply throwing packets over the enclosure walls.
96
These examples point towards a high level of complicity existing between the inmates and the attendants. Hemp and other narcotic substances were considered to be the major causes of insanity. The smuggling in of these items was a combined attempt made by the subordinate groups to subvert the authorities and the discipline imposed on them in the asylums. These attempts formed part of the indirect confrontations that must have occurred at several levels. They went largely unnoticed as they were not considered worthy of mentioning in the annual reports or official memos.
There were other ways through which the patients and the staff subverted the everyday structures. Dr Fairweather of the Delhi asylum pointed out in the annual report for 1875:
I regret I cannot report favourably about the subordinate establishment. The assistant matron, the cook and a keeper have been discharged for stealing the lunatics’ food, and several of burkanzadas [armed guards] and keepers have been fined or dismissed for carelessness and harsh treatment of the lunatics under their charge.
97
G. Ross, the superintendent of Delhi asylum, mentioned in the annual report for the year 1880:
A new and very respectable man has been appointed in place of Salik Ram whom I dismissed, as he was arrested by the police on a charge of appropriating a piece of timber, the property of Government. He was altogether an ill-conducted man, and the asylum is well rid of him. I was obliged to prosecute the malli for being found in the female quarters at night, and also to make some changes among the warders. The visitors met once a month to inspect the asylum and to consider releases and admissions.
98
James C. Scott has pointed out that subordinate groups often used ‘everyday forms of resistance’.
99
For him, when these groups could not take political action, they resorted to everyday forms of resistance that included:
such acts as foot-dragging, dissimulations, false compliance, feigned ignorance, desertion, pilfering, smuggling, poaching, arson, slander, sabotage, surreptitious assault and murder, anonymous threats, and so on. These techniques, for the most part quite prosaic, are the ordinary means of class struggle. They are the techniques of ‘first resort’ in those common historical circumstances in which open defiance is impossible or entails mortal danger.
100
Acts such as stealing objects or having sexual relationships with inmates were integral to the daily acts of defiance that were resorted to by the subordinate staff in the absence of direct supervision.
The patients resisted attempts to force them to lead a dehumanized existence by refusing to eat food or wearing clothes. The superintendent-in-charge of the Delhi asylum, T.E.L. Bate, remarked in the annual report for the year 1887 that:
many of the lunatics throw off their clothing and bedding, and in this way expose themselves to chill, which is of course calculated to produce disease. Again many are very capricious and refuse their food from time to time. In such cases, although artificial feeding is resorted to, their health suffers.
101
C.C. Manifold, the Inspector General of the Civil Hospitals, wrote in the triennial report of the United Provinces:
It was a case of acute mania, the patient being constantly excited. He was very destructive, tearing up and throwing out of his cell the whole of his clothing and bedding. He contracted pneumonia from exposure, and being in a very run-down condition soon succumbed to the disease.
102
Escape and suicide were other common ways of defiance. H.J. Maynard, the Junior Secretary to the Government of the Punjab, pointed out:
It has been alleged that criminals purposely feign insanity in the hope of being committed to the Lahore Asylum, whence escapes are known to be facilitated by structural defects which make the buildings unsuitable for the confinement of even ordinary lunatics. Whether the statement that criminals feign lunacy for the purpose indicated be true or not it is a curious coincidence that quite recently the number of escapes from the Asylum have been unprecedented. It will be observed that there were no less than 10 escapes [in] 1897 and several have already occurred during the current year. The escape of criminal lunatics is serious, and in view of the fact that reports in respect to watch and ward were unsatisfactory.
103
Mills has pointed out that Indians often had hidden agendas and they made use of the asylum space according to their needs. The criminals used the asylum in order to escape harsh treatment and to run away from the asylums. The inmates, when they felt repressed, often resorted to suicide. The superintendent of the Lahore asylum stated:
Suicide was absolutely unknown from the opening of the asylum up to 1906, when a woman utterly without warning hanged herself by her clothing during the night and a man a few days later followed her example. Then in 1908 a man suddenly hanged himself with a strip of blanketing and two others followed suit at short intervals. It is difficult to see how such occurrences can be prevented especially in the winter; even with the most vigilant attendants and none of those here answer that description, every man cannot possibly be always under supervision and short of depriving them literally of all clothing they cannot fail to have facilities for effecting their purpose.
104
Strict vigilance was not adequate to prevent suicides. Suicide was sometimes a result of melancholy, but it was also the ‘last resort’ against a degraded existence. Suicidal patients formed an important category among the incarcerated patients. However, official reports only highlighted cases of patients who had committed suicide, and there is not much discussion about the patients with suicidal tendencies. 105
Illustrative cases of survival also come to the fore. According to Manifold, ‘in 1911 one death was due to heart failure following on old age. The patient had been 37 years in confinement and was 60 years old when he died.’ 106 These survivors had not only made these alien places adaptable but they also used these institutions for their benefit and survival. Inmates survived by forging new bonds and taking on new roles. Ross, the superintendent-in-charge, was of the view that ‘there were some very good performers on musical instruments. Hardeo Das, discharged cured, played the sitar very well indeed; and Pahulwan, Ruguath, Harphul, Ingo,—all musicians. A good deal of music and card-playing goes on when the lunatics get together in the evening.’ 107
The civil surgeon of the Jubbulpore asylum pointed out that
there are male attendants for male patients only. The female patients are too low to require a special attendant, one of them being a harmless monomaniac is proud and happy at this office devolving upon her, and she does it very well. I have authority to entertain female attendants should they be required at any time.
108
Dr Fairweather of the Delhi asylum wrote:
Ashraff Khan, the criminal lunatic…has been gradually restored to liberty and now he goes about free and unrestrained among the other lunatics. He has even within the last few weeks been made to consider himself a kind of assistant-keeper, and has helped order among the lunatics.
109
By acting as cook or a gardener, keeper or attendant, patients not only carved a niche for themselves in these alienating institutions but tapped some status and power for themselves. Thus, there were multiple layers of power dynamics within the asylum walls, including an assertion of agency and the lack thereof on the part of the inmates, whereby the logic of colonial dominance was often turned upside down.
Life in the asylum was based upon strategies of adaptation, survival and resistance. Resistance was sometimes subtle but incidents of ‘bloody’ violence were not uncommon. This violence may be ignored as the wild fury of the ‘madman’ or else invested with deeper meanings, reflecting the aspirations and frustrations of those deemed ‘insane’. J.B. Scriven, the superintendent-in-charge of the Lahore lunatic asylum, reported a violent event that occurred in the year 1868, which might be quoted at some length:
I regret also to have to record a disastrous out-break, attended with loss of life, and severe injuries to several of the attendants, that took place in the Asylum on the 24th of March. An inmate of the Asylum named Keetapai, a non-criminal lunatic who had been under treatment for the past five years. This man is perfectly sane in all points except one, viz., his own excessive rank and importance; he considers that he is an incarnation of the deity…as a rule he may be said to have a kind disposition, as evinced in his attention to the sick,—and his great boast was that he had cured some of the patients after they had been given up by the Native Doctor and myself—and also in his love for animals. I had permitted this man to keep a dog; unfortunately a litter of pups were born, and on their growing up they became such a nuisance that I was obliged to order their being disposed off; this was an offence not to be forgiven, and after evidently brooding over it, he persuaded a lunatic named Guggur Sing to join him in attacking the keepers. Keetapai was heard to say, ‘Oh we are lunatics, we can do what we like and kill them all, and nothing will be done to us.’ Unfortunately chance favored their design. A Bhistee of the Asylum, contrary to the strictest orders, having brought two large bamboos into his house, these were intended for the sides of a Charpoy; but they proved formidable weapons in the hand of a lunatic. Keetapai, though confined in the criminal ward, was allowed to walk and sit in the garden, and under this excuse obtained possession of the bamboos, which he managed to secrete away unobserved into the Criminal ward; he immediately gave one of them to Guggur Sing, and they simultaneously attacked the Warder at the Criminal gate, knocked him down, and rushed into the garden, attacking every keeper that attempted to oppose them; unfortunately there was a lunatic named Phummon working with a ‘phowrah’ in the garden, who suddenly became excited by the out-break and joined in the attack; but the other lunatics took no part except some by shouting and making a noise, while others attempted to save the keepers. The first keeper they met was killed near the entrance of the Criminal ward by a fearful blow on the head, they then rushed towards the outer gate, when they were met by another Burkundaz, who they also killed. On hearing the disturbance, Mr. Wilson, the Deputy Superintendent, who was in his house, rushed into the Asylum to see what was the matter; they met him at the gate, and he received some severe blows on the head, but was eventually rescued by the servants and one of the lunatics. Phummon and Guggur escaped from the Asylum, but were soon re-captured. On hearing of the catastrophy, I proceeded at once to the Asylum; the Police had assembled in force; the excited and violent lunatics were at once confined in the cells and order restored. By order of the Commissioner, the ringleaders, Keetapai, Guggur Sing, and Phummon were transferred to the Central Jail for greater security. A strict investigation took place, and Keetapai, Guggur Sing, and Phummon were tried for murder; but acquitted on the grounds of insanity, and ordered to be kept in confinement during Her Majesty’s pleasure. This is one of those unfortunate occurrences that all Lunatic Asylums are exposed to, notwithstanding the greatest precaution; the affair was so sudden and unprovoked that the keepers had no time to combine against their assailants. I can only state that it is the first and only out-break of a serious character that has ever taken place in the Asylum since it has been under my charge (a period of 15 years), and that the utmost vigilance and precautions are taken to prevent the possibility of a recurrence.
110
This was the day their world was turned upside down. Three lunatics came together and participated directly in the mayhem, while the others participated by shouting and making noises. Some helped to control the violence. Two attendants were killed and the deputy superintendent was injured. Keetapai had predicted that nothing would happen to them as they were lunatics and in accordance with his forecast, they were sent back to the asylum after being acquitted on grounds of insanity. Keetapai was sane enough to seek vengeance. The other two lunatics who participated must have felt the brunt of living behind the closed walls of the asylum.
Time and again, the insane attacked the warders, and sometimes also assaulted their fellow inmates. C.C. Manifold, the Inspector General of Civil Hospitals, United Provinces, noted in the triennial report for the years 1909–11:
In 1911 a lunatic named Gurdin, an inmate of the asylum for the past 5 years and who had never given indication of a tendency to develop violent symptoms, slipt [sic] into a godown in February and emerged with a chopper. Meeting another lunatic drawing water Gurdin attacked him, hacked at his neck and severed his head from his body. The murder was accomplished almost instantaneously and without any noise, and until a warder noticed Gurdin standing by the headless corpse no one realized what had happened. Seeing the warder coming towards him Gurdin threatened him with the chopper, but on the former advancing Gurdin ran into Major Cochrane’s garden where Major Cochrane and some guests had assembled. Major Cochrane went straight to Gurdin and while speaking soothingly to him pinned his arms to his sides and wrested the chopper from his grasp. Major Cochrane’s promptitude and skill averted the imminent danger of another murderous attack. The recognition by the Lieutenant-Governor of his prompt and courageous action was conveyed to Major Cochrane and his conduct was brought by Government to the notice of the Director-General of the Indian Medical Service. The warder, Baldeo, was rewarded with a gratuity of two months’ pay. Since this case the choppers formerly used for cutting up vegetables have been replaced by other more suitable appliances thus reducing the risk of such an occurrence to a minimum.
111
These extraordinary moments were part of their ordinary and everyday existence as murder and violence were not uncommon. Lunatics were aware of the immunity they had because of their ‘insanity’. These events may be regarded as the temporary fury of the insane or as the few sane moments of vengeance.
Conclusion
Erving Goffman’s work has explored the methodologies that unravel the complexities inherent in the interrelated lives of the patient and the staff. Their embedded and enmeshed existence formed the ‘underlife’ of the asylum. The quotidian tales of people and the institutions that they inhabited are quintessential when writing the social histories of madness. Alf Ludke has fervently argued that ‘historical analysis of everyday permits interrogation of struggles and occasional burst out of the anonymous/nameless masses’. 112 The complex temporal and spatial materialities of everyday lives of the asylum inmates have been explored here in order to discern how authority was constantly reordered and redefined. Their ‘everyday’ revolved around work, diet and amusement. It comprised of multiple adaptations and atonements, discernments and the detachments, and survival and subversion at the levels of both the staff and the patients.
Goffman’s concept of ‘underlife’ has been used here to undermine his larger argument about asylums as ‘total institutions’. 113 Total institutions are those whose ‘encompassing or total character is symbolized by the barrier to social intercourse with the outside and to departure that is often built right into the physical plant, such as locked doors, high walls, barbed wire, cliffs, water, forests or moors’. 114 The article has argued that the lunatic asylums in colonial India were not total institutions. Neither was the isolation imposed complete nor was the discipline exercised total. The authorities realized the limits of the mentally ill, and at no point of time were all the patients confined within the asylum forced to work. Only a limited number of patients who were regarded as ‘healthy’ were employed. There was a belief that employment would make the patients self-reliant and bridge the gap between the outside and inside worlds. Nevertheless, the workhouse-like nature of the asylums can be discerned as exigencies imposed by colonialism.
Psychiatry remained at the margins of colonial medicine. The state gave little attention to the development of psychiatry in India. Professor Edward Mapother of the Maudsley Hospital, London, visited Sri Lanka (then Ceylon) and India in 1937; he made a damning critique of the overall psychiatric infrastructure while conceding that the British were ‘bearing the white man’s burden’. 115 Mapother regarded the psychiatric infrastructure as ‘the white man’s burden’ because he believed that the British were doing the best that was possible under the circumstances. He wrote that ‘the wretched provision for the insane in India is apt to be excused in particular by reference to the cost of other medical purposes’. 116 He attributed these pathetic conditions to overcrowding and lack of infrastructure. In other words, it was argued that the empire was marred by many numbers of endemics and epidemics whereby the colonial state could not spare adequate financial resources to spend on psychiatric infrastructure. This resulted in a constrained growth of psychiatry in colonial India and, often, the vocational economy of asylums had to sustain the costs of running these institutions.
The asylum walls were more porous than they have been imagined to be. The patients were allowed to maintain contact with their families and the families were encouraged to be responsible for them. Local communities participated in asylum activities, while the patients were permitted to take rides outside the hospital. Diet and recreation can be regarded as fulcrums around which the social and the cultural lives of the patients revolved. The ‘external’ factors, such as state policies, the nature of government and cultural notions, played significant roles. In the course of this article, various psychiatric ideas and their prevalence and popularity at different times, individual cases, the politics of psychiatric practices and quotidian histories of the asylums have been discussed.