
Abstract
This article reports findings from research about trans* citizenship in 14 post-socialist countries. It evidences substantial deficits concerning trans policy making, and a lack of policy debate in this area. Most examined countries have a lack of protocols for official gender change in birth certificates, IDs, passports and other documents. Usually there are no guidelines, measures and procedures defining the standards of healthcare for trans persons. Practice concerning healthcare varies widely, and trans people and advocates exercise agency in negotiating access to care. The article suggests that trans citizenship studies need to foreground legal and social aspects of citizenship, as these are highlighted in the post-socialist context. Policy implications are discussed in relation to key citizenship debates including those concerning challenges to normative models of citizenship.
Introduction
[T]he number of transgender persons is so small, that there is no need to develop anything special. (S2, Head of Mental Healthcare Clinic, Latvia) (FRA, 2016: 79) There are not many [transgender] people in Bulgaria, this problem is not very popular and few specialists work on it … (S2, Surgeon, Bulgaria) (FRA, 2016: 79)
The provision of citizenship rights to support trans* people, as indicated in the opening quotes, may be low priority for policy makers and practitioners in the post-socialist region of former state-socialist countries, where political and economic transformation has taken place, but the newly established democracy might still be influenced by previous political and cultural norms. There is a lack of scholarship about trans* citizenship in the post-socialist context, and citizenship studies concerning sexual orientation and gender identities have historically been dominated by theories from the USA and Western Europe (see Richardson, 2017).
Trans* people in the 14 countries in this study are supported by international human rights and citizenship frameworks, including the Yogyakarta Principles on the Application of International Human Rights Law in Relation to Sexual Orientation and Gender Identity, which is a policy statement drafted in 2006 by a distinguished group of human rights experts in response to well-documented violence experienced by minority groups on the basis of their sexual orientation and/or gender identity (Kollman and Waites, 2009: 5). In addition, EU legislation is supposed to guarantee equal treatment for everyone in the EU member states, regardless of their sexual orientation and/or gender, via a range of directives and policy statements including the Treaty on the European Union and the Charter of Fundamental Rights of the EU (Takács, 2015). 1 In 2015, the Council of Europe passed a resolution supporting the rights of trans* people in European Countries (FRA, 2016); it challenges the way that some post-socialist countries oblige trans people to go through lengthy processes with medical gatekeepers (including sterilisation in a few cases) to gain access to legal recognition. Transposition of EU directives varies across post-socialist EU member states. For instance, in Poland the only anti-discrimination protection that trans* people have is in the labour code due to the EU directive. A more progressive situation is present in Hungary: the Hungarian Act on Equal Treatment and the Promotion of Equal Opportunities (ETA, 2003) was the first national equal treatment legislation in the world in 2003 that included gender identity, specifically providing anti-discrimination protection for trans* people. Recently some other post-socialist countries – notably former Yugoslav republics of Slovenia, Croatia, Serbia and Bosnia – also adopted explicit mentioning of gender identity and/or gender expression in their anti-discrimination legislation as the grounds on which discrimination is prohibited. Despite some positive changes in policies that address trans* issues, none of the examined countries provide full legal protection for their trans* citizens. According to Trans Rights Europe Index (Transgender Europe, 2016), which measures 22 legal items in areas of equality, non-discrimination, asylum, hate crime and family law, Croatia has the most trans-positive legislation (existing policies in 68% of 22 identified areas), followed by Hungary (50%), Slovakia, Serbia, Bulgaria, and Bosnia and Herzegovina (36%), Belarus (32%), Poland (27%), Slovenia (23%), Romania and Latvia (18%), and, finally, Russia and Lithuania with only 14% of trans-positive policies in place. 2
This article addresses the uneven patterning of trans trans* citizenship in nine EU (Bulgaria, Croatia, Hungary, Latvia, Lithuania, Poland, Romania, Slovakia, Slovenia) and five non-EU (Bosnia and Herzegovina, Belarus, Kyrgyzstan, Russia, Serbia) post-socialist countries. Whilst there are some positive developments concerning trans* citizenship, a lack of access to full citizenship rights is also common. We will show that the lack of and/or the trans* unfriendly legal regulations create numerous disadvantages for trans* people. The breaches of human rights that are evident in some countries are also present in terms of deficient access to healthcare. Healthcare is a key aspect of transsexual and many other trans* people’s citizenship in post-socialist countries and elsewhere, because access to legal gender recognition is, for transsexuals across post-socialist countries, a highly medicalised process. This article, in its analysis of data from five non-EU and nine EU post-socialist countries, provides an original contribution to the literature on trans citizenship and the policy literature concerning gender rights more broadly. Further research is needed about other aspects, such as political citizenship. For instance, there is an absence of trans* people in political office (Polish MP Anna Grodzka is an exception) and trans* people in countries such as Hungary have a higher than average rate of unemployment (Takács, 2016).
In delineating the key issues that trans* people in post-socialist countries face in relation to citizenship, the article provides insights regarding trans* citizenship studies more broadly. We take the work of T.H. Marshall (1950) as our starting point. For Marshall, citizenship rights were defined as those including civil rights (legal rights, free speech and movement), social citizenship rights (including healthcare and welfare) and political rights (including seeking public office). There are many critiques of Marshall’s work, including its masculinist assumptions regarding the public/private divide (Walby, 1994). Citizenship studies has been re-theorised, for example Roseneil (2013) outlines a multi-levelled, multi-dimensional citizenship which addresses economic resources, equality and recognition. Whilst acknowledging these important developments, we argue that there is still some purchase in a Marshallian-style focus on legal and social citizenship rights. In the post-socialist context, a lack of systematic legal protection and healthcare provision were outlined as crucial aspects of trans* citizenship. We also show that for trans* citizenship, legal and social (health) citizenships are enmeshed and need to be considered together.
The field of trans* citizenship has emerged since 2000, building on earlier conceptual work provided by sexual and intimate citizenship scholars (Evans, 1993; Weeks, 1998; Richardson, 2000, 2017; Plummer, 2001, 2003). Key aspects include autonomy and choice-based models of healthcare, self-determination regarding identity, equality (Monro, 2003, 2005; Monroe and Warren, 2004), community (Aizura, 2006), and recognition in political and legal terms (Hines, 2013). Authors such as (Monro, 2005, 2007) and Van der Ros (2013) use gender pluralist approaches, where sex and gender are seen as continua and in which trans* citizenship models include not just transsexual men and women but also others who identify as gender-fluid, non-binary or androgynous. West (2014) argues that trans* legal and political citizenships must be extended to include changes to cultural perception regarding issues such as bodily presentation, not just formal rights.
Trans* citizenship can be related to other areas of citizenship studies, for example lesbian citizenship (Richardson, 2000), in terms of the extent to which wider citizenship frameworks are problematized by addressing the rights of a particular group. For trans* citizenships, questions remain regarding whether it is just transsexual (men and women’s) citizenships that are sought, or citizenship rights for all gender variant people, which would entail fundamental changes to social sex and gender categorisation systems (see Monro, 2003). There are also various issues that cut across a number of interest groups: for instance, the public/private divide that is associated with liberal citizenship is problematic for trans* people, in relation to the crucial role that healthcare and birth certificate correction can play in their lives (see Monro, 2005).
One debate that is of particular importance in the post-socialist context concerns the universalist–particularist debate (Monro and Richardson, 2014). Universalism entails citizens being defined by what they have in common, and by universally binding rules and laws; such an approach underpins the development of universal human rights claims (Young, 1990), which are important for the human rights frameworks that increasingly support lesbian, gay, bisexual and trans* (LGBT) politics (Kollman and Waites, 2009; Richardson, 2017). Universalism has advantages for trans* citizenship in that it acts as a ‘level’, supporting the equality of everyone; also it is not strongly identity based, so is more inclusive of people with changing or ambivalent subject positions. Particularist approaches to trans* citizenship, in contrast, enable groups to be treated as distinct, and also address specifics such as the national contexts of trans* people in post-socialist countries. However, they can risk ‘freezing’ people in particular subject positions, which is problematic for some trans* people. Authors such as Hearn et al. (2011) support using a combination of universalist and particularist approaches. We follow this approach in referring to universalist trans* rights frameworks but also drilling down into the particularities of trans* people’s lived experiences, and policies regarding trans*, in post-socialist countries. As Lister (2011) notes, context matters in discussions about citizenship, including the influence of historical processes and current practices. Addressing the differences shaping trans* citizenships in each post-socialist country in a comprehensive way is beyond the scope of this article, but legislative details are available via Transgender Europe (2016). It should be noted that there are specific dynamics found in post-socialist countries, including changing gender and sexuality regimes in relation to the legacy of Soviet rule (Štulhofer and Sandfort, 2005; Kuhar and Takács, 2007; Kulpa and Mizieliñska, 2011), and the emergence of localised hybridized cultures, where nationalism becomes mixed with identities perceived to be Western (Marciniak, 2009).
We begin our discussion by describing the methodologies employed and providing a snapshot of the legal and social situation for trans* people in the 14 countries under discussion. We then review deficits concerning legal citizenship, and then address healthcare citizenship, including issues concerning resource constraints, healthcare monopolies and inconsistencies. The conclusion examines reasons for continuing policy and practice deficits concerning trans* citizenship in post-socialist countries, and comments on the implications for models of citizenship.
This article uses the term ‘trans*’ as an umbrella term, to represent a large variety of (non-normative) gender identities and expressions, including transsexual people, those who identify with both or neither of the usually available two gender categories, and gender nonconforming people. Where the discussion relates only to transsexual people, we use that term instead. The term ‘sex change’ is only included when this is the term used by interviewees.
Methodology
This article draws on two qualitative studies, both of which utilised purposive sampling and thematic analysis. The first study (S1), conducted by Kuhar and Takács in 2015, involved semi-structured interviews with altogether ten trans* activists (including six participants identifying themselves as trans*), allies and/or experts in trans* issues, from the following countries: Bosnia and Herzegovina, Belarus, Hungary, Kyrgyzstan, Lithuania, Poland, Russia, Serbia, Slovakia, and Slovenia. 3 In these interviews we examined the policy framework and policy deficits in relation to legal gender recognition and the availability of trans* healthcare, and the social perception of trans* issues as potentially reflected in anti-discrimination and equal treatment policies.
The second study (S2) was conducted by the Fundamental Rights Agency (FRA), with support from Monro and her team (FRA, 2016), and it included the following countries: Bulgaria, Croatia, Hungary, Latvia, Lithuania, Poland, Romania and Slovakia. Seventeen of the 310 professionals and policy makers with an LGBT remit who were interviewed in these countries had a specific role concerning trans* health care, and it is these interviews which are the main source here. Interviewees were sampled via contacts with public authorities and conducted by teams managed by the FRA. Interviews were recorded in the original language, transcribed (some in full, some in note form) and translated into English; more detail is provided in the report (FRA, 2016: 94).
Trans* citizenship in 14 post-socialist countries
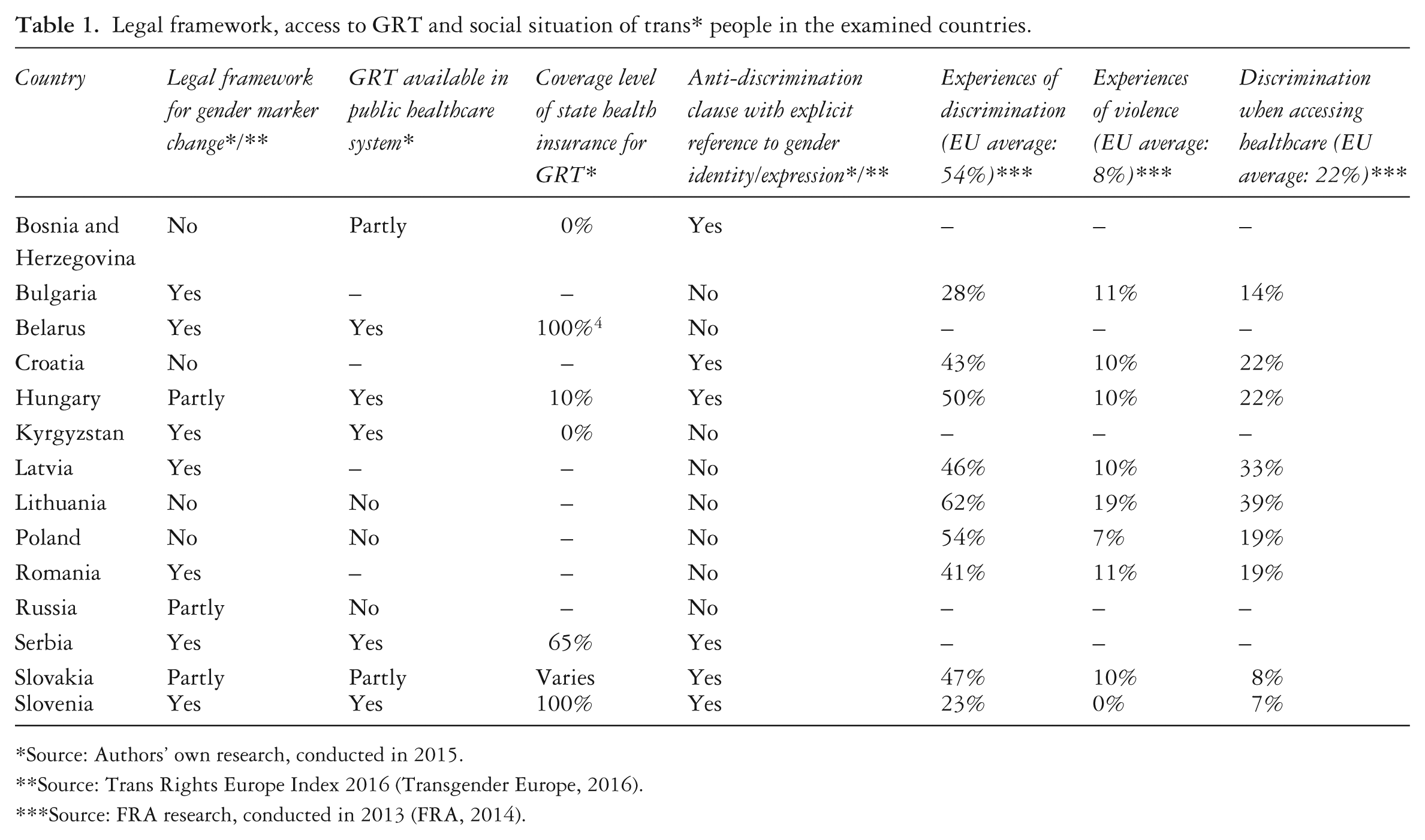
An overview of trans* policies and legal frameworks is provided in Table 1. This table combines research data and existing knowledge of the 14 examined countries in the following areas: legal frameworks for gender marker change, the availability of gender confirming/reassignment treatments (hereafter known as ‘GRT’), the coverage of this by state health insurance, the existence of anti-discrimination legislation with explicit reference to gender identity/expression, and indication of experiences of discrimination and violence.
Legal framework, access to GRT and social situation of trans* people in the examined countries.
Source: Authors’ own research, conducted in 2015.
Source: Trans Rights Europe Index 2016 (Transgender Europe, 2016).
Source: FRA research, conducted in 2013 (FRA, 2014).
It is clear from these results that, whilst there is some positive legal and medical provision, worrying deficits exist regarding trans* citizenship in a number of countries. The next section focuses on legislative deficits and inconsistencies. We also present findings concerning the strategic use of legislative anomalies by those concerned with trans* citizenship in some post-socialist countries. The research findings indicated that legal citizenship was a matter of key importance to trans* people in post-socialist countries.
Legal citizenship
Whilst some progress has been made, the trans* activists who contributed to the study highlighted the inadequacies concerning legal citizenship in post-socialist countries. At the most basic level, trans* people are unable to gain full legal recognition (change of identity documents) or gain it with considerable difficulty if they undergo gender transition in some of the countries in this study. For instance, a research respondent discussed a case where a trans* person’s documents do not reflect his appearance: He has to explain [his gender] every time. Very rarely it is an OK experience, like ‘oh, OK, fine, go ahead’… mostly they would get him off the bus, separate him, if he is on the airport, question him, you know, sometimes strip him down, they are just very aggressive … so he has to go and explain everything, but sometime it doesn’t help. It is a very stressful experience for him to cross the border. (S1, Trans* activist, Bosnia and Herzegovina)
Legal citizenship challenges vary across the countries. In Lithuania, for instance, the Civil Code states that ‘an unmarried natural person of full age enjoys the right to change the designation of sex in cases where it is feasible from the medical point of view’. The Code also states that the procedure should be prescribed by the law – but no such law has been introduced for more than 14 years. This is why ‘L’, a trans* person, took Lithuania to the European Court of Human Rights in 2007.
5
This case points to the gap in the relevant Lithuanian legislation: there is no law regulating full gender reassignment treatments – until such a law is enacted, no suitable medical facilities appear to be reasonably accessible or available in Lithuania. However, the issue of trans* citizenship is contested in Lithuania, as case law can be used to gain citizenship rights: The only thing that people can do is to have the gender reassignment, that is, they transition abroad and then they come back home having wrong identity documents. They can apply to the civil registry to change the documents. Then the civil registry refuses to do that because they have no legal basis to do that and then with this rejection trans* people can go to the courts and then the courts … order the civil registry to change the documents. (S1, LGBT activist, Lithuania)
Irregularities in the content of the law regarding gender confirmation are evident in several post-socialist countries. For example, in Hungary documents can be changed at any time – pre, mid- or post-surgery or other treatment – after obtaining two psychiatric/psychological assessments/referrals, and obtaining a new birth certificate and other related official documents due to official gender change is free of charge. However, this official procedure lacks any legal basis: it is grounded merely in a currently supportive official attitude. The overall lack of legal arrangements regarding accountability for trans* citizenship raises concerns about future legal consistency (Solymár and Takács, 2007).
Our data show other inconsistencies in the way legal citizenship is present or absent. In most of the examined countries there is some kind of legal framework, but, according to our respondents, an insufficient one as it does not correspond with the actual needs of trans* people. We have found several references to specific legal requirements in different countries which cannot be applied in practice. For example, in Russia – similarly to Kyrgyzstan and Belarus – one needs a certificate with an F64.0 (International Classification of Diseases – see: ICD10Data.com, 2017) diagnosis of ‘transsexualism’ which should be, according to the law, issued on a specific form (this refers to the International Classification of Diseases). But there is no form issued for this, so access to legal citizenship is dependent on the vagaries of the clerks working at the civil registry office. In Serbia there is varied practice: In the North [of Serbia] you can do it within 15 days and most clerks would know what they need to do even though there is no regulation … but in the South, clerks reject it as they are not covered by the law. They don’t know how to do it. Sometimes they ask the court and you can wait for 9 months or more for documents to be changed. (S1, Trans* activist, Serbia)
In Poland there is no specific law about gender recognition, only High Court rulings: ‘it was decided that in these cases your parents would be the ones who are responsible for giving you a legal gender and then they would be the ones to decide in that legal argument’ (S1, trans* activist and researcher, Poland). A bill to grant legal rights to Polish trans* people was blocked by the Polish president, Andrzej Duda, in October 2015 (Smith, 2016). The current provisions are very problematic, as the following quote demonstrates: especially to those people who are adults or who have families that do not accept them or respect them. If a family is against gender recognition, this usually doesn’t influence the decision of the court, but it influences the length of that process. (S1, Trans* activist and researcher, Poland)
Overall, trans* legal citizenship in post-socialist countries appears to be emerging in a fragmented and contested way. The lack of full gender recognition rights for trans* people is the main area of deficit, according to the trans* activist respondents. In addition there are other deficits, including rights for gender-diverse, gender fluid and non-binary people and reproductive rights (FRA, 2016).
What are the reasons for legal citizenship deficits in post-socialist countries? The interviews with public officials and professionals revealed major barriers to achieving full trans* citizenship. These include a lack of awareness about trans citizenship issues at both national and more local and frontline levels. Public officials often felt that the social climate is unsupportive of trans* citizenship-related work. For example: about the [LGBT] strategy … I don’t think our society is mature enough for this. (S2, Public authority representative, advisor, Lithuania) Simply, the social-intellectual context has not become mature enough for this. (S2, Public authority representative, director, Hungary) (FRA, 2016: 29)
The barriers to trans-positive citizenship interventions include prejudice founded on religious beliefs and/or traditionalism regarding gender and sexuality, and a lack of real levers to ensure that citizenship directives are implemented within EU countries. For instance, a Slovakian ministerial officer reported that allocation of resources to support LGBT equalities was ‘virtually impossible’ without a binding policy commitment (FRA, 2016: 32). These barriers concern LGBT citizenship in general, but there were indications that trans* citizenship was seen as particularly difficult by some respondents. Trans* challenges fixed notions of gender in specific ways, and have legal and medical implications which are different from those pertaining to lesbian, gay and bisexual people.
The FRA (2016) study shows overall that EU directives and recommendations provide a framework for trans* citizenship in the post-socialist EU succession countries. In some EU member states, trans* citizenship work is taking place as part of initiatives to support lesbian, gay, bisexual and trans* (LGBT) rights more broadly at frontline as well as national strategic levels: for example, in Poland, some training concerning LGBT issues is available to education professionals (FRA, 2016). However, the deficits regarding legal protection for trans* people are marked and affect key areas of trans* people’s lives, including identity recognition, and protection from discrimination and violence. We contend therefore that there is a need for a focus on the legal aspects of citizenship when considering the policy implications of gender diversity in post-socialist countries. Policy actors can appeal to universal notions of citizenship when implementing change in this area. However, the particularities of the countries, and their legal apparatus, mean that a particularist approach is also important in understanding trans* citizenship in post-socialist countries.
The legal aspects of trans* citizenship need to be considered alongside those relating to healthcare, as the medico-legal complex lies at the heart of trans* citizenship issues. Healthcare is, of course, one aspect of social citizenship, as outlined following Marshall (1950), but for trans* people, it is intertwined with legal citizenship. In most of the examined countries the precondition for the gender marker change in legal documents is the diagnosis of ‘transsexualism’ (F 64.0), and in others completed gender reassignment treatments are required. Healthcare is therefore the next area under discussion.
Trans healthcare
The FRA (2016) research outlined substantial support for trans* health-related citizenship across the EU, including in post-socialist EU countries. Developments are underpinned by standards such as the universalist Council of Europe Recommendation CM/Rec 2010 (5) which states that countries should ensure access to specialist services concerning gender reassignment; costs of this should be covered by health insurance. Respondents in a few countries, such as Croatia, Hungary and Slovakia, reported that their governments were showing some support for these measures.
hormonal therapy is covered by healthcare and sterilisation as well. But if you want something else, for example, some people really need or want genital surgery, which is not happening in Slovakia at all … So if you really want that, then you have to go to the Czech Republic and what happens is that the Slovakian public healthcare plan coverage allows you to use healthcare services in another state if those are not available in Slovakia. (S1, Trans* activist, Slovakia)
EU guidelines do appear to be having some impact on the ground: for example ‘we naturally try to form our policies in the healthcare field in line with those directions’ (S2, Secondary care officer, Hungary (FRA, 2016: 74)). There were also indications that a handful of proactive practitioners are taking very diversity-inclusive approaches, exceeding trans* citizenship situations in most other EU countries. For example, a Hungarian private in vitro clinic helped a trans* couple to have children, and a respondent reported that: I think that we are in a pioneering situation in that sense that the name change just on the basis of the diagnosis is permitted in very few countries. So that there is no need to operate or destroy anything. (S2, Deputy director, psychiatric clinic, Hungary) (FRA, 2016: 74)
The FRA (2016) research shows that trans* citizenship in post-socialist EU countries may be facilitated by a number of factors. These include the application of standard professional protocols, the use of internet resources by trans* people and professionals, and the existence of professional bodies and networks which can support professionals across national boundaries, again supporting arguments about the importance of universalist approaches to trans* citizenship (see above). For example, Slovakian professionals used information available in the Czech Republic to supplement the limited information available in Slovakia. Good partnerships with trans* activist and support organisations were seen as important in countries such as Bulgaria, Hungary and Romania. The importance of LGBT activism more broadly is discussed in the literature, for example, in a study based in Kyrgyzstan (Wilkinson and Kirey, 2010); here, notions of universal rights across the varied groups encompassed in the ‘LGBT’ acronym are evident.
Healthcare citizenship deficits
The research with both activists and policy makers and practitioners across the post-socialist countries reveal substantial deficits concerning trans* health-related citizenship. Crucially for transsexuals, full GRTs are unavailable in countries such as Croatia, Slovakia and Lithuania (FRA, 2016). There is an absence of formal protocols regarding GRTs in these and other countries, including Hungary, Slovenia and Romania. A lack of public policies concerning trans* healthcare has been reported in several countries including Bulgaria, Croatia and Poland.
Many of the trans* citizenship deficits involve problems with the law (see above) which can impact very negatively on transsexual healthcare. Where laws are absent concerning gender recognition, care can be severely affected: The law concerning gender reassignment has not been adopted. And these poor people have to [go to] Belarus, Russia and Thailand, pay lots of money and change their sex. As a doctor I am immensely ashamed that this law has been drafted … and up until now has not been adopted … [G]ender reassignment has even been crossed off of the surgery list. (S2, Doctor and clinic owner, Lithuania) (FRA, 2016: 78)
Other legal difficulties can also impede trans* health-related citizenship. For example, inconsistencies in Romanian law mean that most surgeons refuse to perform gender reassignment surgeries because they could be held criminally responsible for reproductive failure in their patients. In countries such as Hungary, where ‘[F]emale hormones cannot be prescribed to someone who is still officially a man’ (FRA, 2016: 78), trans* people are forced to use illegal sources, and face health risks.
In some of the countries where some transsexual healthcare is available, it is highly problematic. For example, an activist respondent reported that there is one doctor in Bosnia who claims that he can do ‘sex change surgery’, but in reality he does not have much experience in this field as he has only done one such surgery, and the results were not satisfying. For that reason most people from Bosnia go to Serbia for GRTs. However, when they come back, they face problems gaining legal gender recognition, as discussed above. Some extremely poor practice regarding trans* healthcare has taken place in post-socialist countries, including Slovakia, Latvia and Bulgaria. For instance: One transgender woman who wanted to have her testicles removed was rejected in all Bratislava hospitals. In Nitra they first admitted her and later discharged her on the grounds of the following argument: ‘We shall not support paedophiles’. (S2, Endocrinologist, Slovakia) (FRA, 2016: 81)
The provision of general healthcare to trans* people is also challenging in post-socialist countries; professionals reported that trans* people are likely to wait longer than other patients before accessing general healthcare services in countries including Bulgaria, Hungary, Poland and Romania, due to fear of stigmatisation (FRA, 2016). The FRA research indicated other barriers. Trans* healthcare was considered to be a low priority by many healthcare professionals and policy makers. Trans* people were often invisible to healthcare services, as they were reluctant to seek healthcare due to realistic fears of discrimination.
It is not just at the level of specialist care that there is a deficit of measures to support trans* healthcare; problems with a lack of awareness and ‘unfavourable reactions’ (FRA, 2016: 81) amongst general practitioners in countries including Bulgaria, Croatia, Hungary, Romania and Slovakia, and poor secondary and tertiary care in, for example, Bulgaria, Latvia and Slovakia. The difficulties are compounded by a lack of training about trans* healthcare in several post-socialist countries, including Bulgaria, Croatia, Lithuania and Latvia (FRA, 2016). Policy actors therefore need to consider a range of measures to address trans* healthcare deficits.
Resource constraints
Overall, ‘economic and social marginalisation places trans* persons in positions of vulnerability’ (FRA, 2016: 82). This can affect every area of life (for example, housing) but in particular it shapes trans* people’s abilities to access healthcare. For example, activists suggested that in Poland there are some hospitals where it is possible to claim surgical costs on the national healthcare plan, but that is not official and it is dealt with by those medical professionals who are able, and willing, to justify it under some different heading. A practitioner remarked that: Any surgery entails a cost of several thousand Polish zloty, which, to be honest, not every patient can afford. The treatment process is extended over time, which is not good for them because it’s not comfortable. Many patients do not complete the full surgical process mainly due to financial reasons. (S2, Transgender specialist, Poland) (FRA, 2016: 81)
The activist respondents reported that public healthcare funding for GRTs varied: the coverage ranged from 100% in Slovenia and Belarus, 65% in Serbia, to 10% in Hungary and zero in most of the other countries. For instance, in Russia ‘all treatment should be paid by the transgender [sic] people themselves including hormonal treatment, psychiatric examinations and, of course, these surgeries are not included in any public programmes’ (Russian activist and legal expert). This affects trans* people’s mental health, well-being, and ability to fully transition. Overall, therefore, resourcing of GRTs and related medical care is problematic, with deficits affecting trans* people’s access to citizenship rights including legal recognition. This situation shows that citizenship debates about the importance of recognition for trans* citizenship (Hines, 2013) need to take the centrality of economic inequalities into account.
Monopolies
Monopolies concerning GRT provision, and hence gatekeeping to legal recognition, exist in various countries. However, in a post-socialist context monopolising the diagnosis by a very few number of ‘specialists’ seems to be a more widespread practice than in Western countries, causing major problems for trans* citizenship. For instance, in Kyrgyzstan there is only one doctor known to be trans-friendly and most trans* people go there. In Belarus there is only one available psychiatrist, the head of the sexology department of the Minsk City Neuropsychiatric Clinic who publicly expresses very homophobic views and, according to our respondent (S1), believes that ‘it is possible to prevent transsexuality if the person grows up in an intact family with the right relations [sic]’. He sees ‘the transformation of gender roles’ in modern society as a problem.
The existence of monopolies concerning trans* medical care has important ramifications of trans* citizenship. If there are only a very limited number of healthcare centres that can be used by trans* people in the national healthcare systems, and there is no other choice or no possibility to ask for a second opinion, they may need to search for assistance abroad. As noted above, this can then lead to legal and social problems when they return. In addition, trans* citizenships are sometimes shaped by international events in very direct ways. For example, in Ukraine and Russia after the military intervention in Crimea, our Russian respondent reported that: we started to get requests by transgender people from Crimea, because before there was Ukrainian legislation there officially and in Ukraine they have only one board, an official board of psychiatrists in Kiev and they actually have a regulation, a protocol, that is not very good, not very progressive, because there is a surgery requirement, there is a requirement of dissolution of marriage and there is also a requirement that in order to change documentation a transgender person cannot have children under 18 years old. And of course the legislation is much more restrictive than in Russia. (S1, LGBT activist and legal expert, Russia)
The use of transnational travel to gain citizenship rights is a recurrent theme in the data from post-socialist countries. On the one hand, this demonstrates agency, as well as an increasing trend towards globalisation. On the other hand, the use of transnational means to support trans* citizenships is likely to be highly structured by economic disparities, as poorer trans* people, and less well-resourced healthcare practitioners, are less able to access them.
Inconsistencies and agency
As we have shown, the provision of healthcare to trans* people across post-socialist countries is very inconsistent, mirroring the legal inconsistencies and anomalies outlined above. This relates to broader issues with post-socialist welfare regimes being uneven, with diverse and often contradictory restructurings (Lendvai and Stubbs, 2015). Importantly, we have found that some actors use the anomalies in the healthcare system strategically, with both trans* people and those concerned with their care having to find ways to manipulate the system to gain some citizenship rights. This is interesting in terms of citizenship discussions. It points to the importance of agency when considering trans* citizenship; this can be termed ‘agentic citizenship’ and it may get overlooked if there is too much focus on universal rights.
Respondents reported that, in Hungary and Kyrgyzstan, the lack of legislation can provide state institutions with a significant degree of flexibility, so that the relevant institutions are able to establish procedures more responsive to human rights concerns. In some cases, professionals working with trans* people went out of their way to assist them: for example a Hungarian professional reported that ‘a lack of public health insurance for GRS means that surgeons have to find other ways to finance surgery, including using invented grounds’ (FRA, 2016: 82). Whilst such innovation is laudable, it can be imagined that some trans* people are excluded from such processes, raising concerns for policy makers committed to ensuring equal access to social rights.
Activism and organised engagement with medics and policy makers concerned with trans* citizenship is important in post-socialist countries. For example, in Kyrgyzstan trans* people started to demand services in 2006 and they were able to shape services as they worked closely with doctors. However, the inconsistent trans* health-related citizenship situations across these countries do provoke concern, as these processes lack clarity, transparency and accountability. Trans* people’s care becomes reliant on good luck, and some activists reported that bribery is used in some countries (for example, in Belarus) to access services.
In this section of the article we have shown that there are some advances in trans* healthcare citizenship, as driven by universalist EU directives in EU member states, by LGBT and trans* activism, or by the positive actions of policy makers and professionals working in the field. We have also uncovered breaches of citizenship rights, and some key themes of pertinence to the situation in post-socialist countries. We noted the ways in which the fragmented and legal and medical frameworks found in post-socialist countries also offer trans* people opportunities – either in building up coalitions with trans* supportive medical service providers, or in finding ‘ways around’ the insufficient state of affairs. In the final section of the article we will summarise the key issues concerning trans* citizenship in post-socialist countries, before addressing policy and citizenship implications.
Discussion
In terms of both healthcare and legal citizenships, there are instances of severe discrimination taking place in some of the examined countries (as also indicated in Table 1), in terms of basic identity documents, familial and relationship rights, and rights to freedom from discrimination in accessing state-funded healthcare provision. These should be of real concern to policy makers at domestic, EU and international levels, as breaches of human rights as defined in the Universal Declaration of Human Rights, the Charter of the Fundamental Rights of the EU and the Yogyakarta principles are taking place. Where some legal provision exists, there are substantial difficulties in most countries regarding inconsistent, arbitrary and/or discriminatory legislation. This makes the situation for policy makers working to support trans* rights in these countries difficult, and the legislative deficits are shown to have negative effects on trans* people’s lives.
Some post-socialist countries provide health-related citizenship rights to trans* people (see Table 1), but there are many deficits. These are related to non-existent or patchy provision of GRS, a lack of policies and protocols, insufficient prioritisation, a lack of awareness and active discrimination. Some patterns are particularly marked in this set of countries. These are: resource constraints, monopolies in healthcare provision, and inconsistencies in medico-legal provision. As is the case elsewhere, this places the onus on trans* people to build up their own networks of support (see Hines, 2007).
The research findings demonstrate a need to address both universal, and particularist, elements of trans* citizenship. At a universalist level, EU directives are important in supporting trans* citizenship and they are having a positive impact in the EU countries; however, they are far from being universally implemented and are often dependent on the goodwill of professionals and civic servants (FRA, 2016). Outside the EU, there is even greater reliance on proactive healthcare and legal professionals to meet trans* people’s citizenship rights, indicating a need for particularist analysis that addresses national and supranational contexts. There are also specificities concerning trans* citizenship in these countries, which may or may not be replicated elsewhere. Some of these are discussed above, including the level of inconsistencies in medico-legal situations, and the agentic citizenship efforts that both trans* people and trans-positive professionals make. The others concern the national contexts more broadly. The findings from the FRA report did show that there are positive moves taking place: during the communist regime these [trans*] issues were completely tabooed while today it is almost a normal subject of conversation … After the revolution the things really got going and, thank God, today there [is a full range of] surgeries these people may demand and we are able to offer. (S2, Plastic Surgeon, Slovakia) (FRA, 2016: 74)
Citizenship debates provide a further trajectory for policy analysis. Critiques of Marshall’s (1950) approach, including the erasure of the public/private divide (Walby, 1994) are relevant to trans* citizenship in post-socialist countries, as trans* peoples’ private lives are profoundly shaped by state policies. However, social and legal rights are crucial for trans* people, indicating the continued importance of Marshallian approaches. As noted above, there are questions about the types of citizenship sought and whether this may affect wider social gender structures. It seems that in the post-socialist context, gender-binaried transsexuals can be framed as questioning or threatening traditional ideas about gender roles by their mere existence, and thus they can encounter hostile interpersonal and social reactions. Trans* communities are increasingly faced with the organised resistance against gender equality and sexual citizenship in Europe in a form of so-called ‘anti-gender movements’, which are activist networks and lobbies that support traditional, sexist and homophobic norms and often have close connections to the Catholic Church. These movements, for example, initiated a referendum against marriage equality in Croatia, Slovenia and Slovakia. The basic idea that connects these movements is the concept of ‘gender ideology’, which functions as a multi-purpose enemy, which can be shaped in different ways in order to fit into the concrete goal of a political protest, predominantly concerned with protection of allegedly endangered traditional family (Hodžič and Bijelić, 2014; Kuhar and Paternotte, 2017). Although primarily aimed at opposing marriage equality and women’s reproductive rights, trans* rights are increasingly becoming targeted by anti-gender mobilisations, as trans* people are seen as those who are fundamentally questioning the neatly organised heteronormative binary gender system.
Another, related, issue is that the inclusion of trans* people together with lesbian, gay and bisexual people in activist organisations may also provoke transphobic reactions from policy makers, politicians or members of the public, regardless of the sexual identities of specific trans* people. Patterns of prejudice are not universal; for example, surveys of Slovenia and Poland found that there is greater resistance to international notions of LGBT rights in countries where (Catholic) religion is embedded in national identities (Ayoub, 2014). However, there are worrying developments, as this quote illustrates: The stigmatisation against them [trans* people], or literally anger, have strengthened in past years and have not subsided … that is a political [question] of how society treats minorities … (S2, Deputy Director, psychiatric clinic, Hungary) FRA, 2016: 79)
From a citizenship perspective, traditionalist masculinist and heterosexist models of citizenship are being deployed in some post-socialist countries in a highly restrictive way, excluding trans* people from models of a ‘good citizen’ (see Richardson and Monro, 2012). The situation regarding non-binary, androgynous or gender-fluid individuals is unclear from our data; it could be imagined that these trans* people are even more excluded from citizenship in post-socialist countries than others when they require access to trans-specific legal rights and healthcare, given the wider social context and political pressures.
Conclusion
Our article points to a need for legal and healthcare citizenship to be foregrounded, with respect to trans* people in post-socialist countries. Policy makers need to be aware that for many people this group, legal and social aspects of citizenship are intertwined and mutually constitutive in a way that is different to other social groups, because of the centrality of medical provision to an individual’s ability to gain legal recognition.
We have shown that a lack of comprehensive citizenship rights impact negatively on many aspects of trans* people’s lives in post-socialist countries, such as freedom from harassment and abuse, decision making about care pathways and reproductive rights. We argue that policy makers need to find ways to work with politically mobilised ideas, for example that gender diversity threatens the identities of more traditional men and women and heterosexual family forms. Notions of nationhood as bound to traditionalist identity and family forms are present elsewhere, for example in Northern Ireland, where a somewhat inclusive policy environment has evolved despite barriers (Richardson and Monro, 2012).
Overall, achieving trans* citizenship in post-socialist countries requires attention from policy makers and practitioners at domestic levels, internationally and at the EU level. In the EU member states, some leverage can be exerted via EU law, either through individual court cases or via the use of human rights directives, although resistance to the latter can be problematic (see FRA, 2016), and more research is required about this in the post-socialist context. Where there is no domestic political appetite for trans* citizenship, gains can still be made by supporting grassroots activist interventions and professional networks, as well as engaging in wider public awareness raising about trans* identities.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.