
Abstract
Research shows that HIV prevalence in transgender and non-binary persons is extremely high, with prevalence rates ranging up to 52.4% (Edwards et al., 2007). This high risk is associated with a number of (trans-specific) factors, such as stigma, discrimination, normative gender roles, involvement in sex work, a lack of knowledge about safe sex and an inaccurate perception of risk. This article critically reviews the last 10 years of research on transgender and non-binary persons and sexual risk from a feminist intersectional perspective that focuses on gender identity, class, ethnicity and other axes of difference that contribute to the high risk for HIV for (some) transgender and non-binary persons. There appears to be an interweaving of different factors in which the discrimination and stigmatisation of transgender and non-binary persons is central. The limitations and pitfalls of current research are pointed out, and suggestions for policy and further research are made.
Introduction
Over the past few decades, there has been extensive attention concerning the AIDS epidemic within a range of research areas. Though the impact of the HIV virus has been somewhat reduced, focusing on reducing sexual risk remains important, especially for some high risk groups. In their ‘Consolidated Guidelines on HIV Prevention, Diagnosis, Treatment and Care for Key Populations’, the World Health Organisation (WHO) states that transgender people are one of the five key target populations that are disproportionately affected by HIV, along with men who have sex with men (MSM), people in prisons or other closed settings, people who inject drugs and sex workers (WHO, 2014). The term ‘transgender and non-binary persons’ is used to describe the highly diverse group of individuals who cross or transcend culturally defined categories of gender, or whose gender identity and expression differs from what is normative for their assigned sex in a given culture and historical period (WPATH, 2012). Indeed, research shows that many transgender and non-binary persons engage in some form of sexual risk behaviour, and HIV prevalence among transgender women appears to be high (e.g. Baral et al., 2013; Herbst et al., 2008; Melendez and Pinto, 2007; Operario et al., 2008b, 2011). However, research focusing on transgender sexual risk behaviour is not extensive and current research on sexual risk among transgender and non-binary persons still has some sharp limitations. This review aims at critically revisiting research published between 2005 and 2015 in this area, using a feminist framework that focuses on intersectionality, thereby pointing out policy suggestions to improve the sexual health of transgender and non-binary persons.
Analysing the literature through a feminist intersectional lens
Traditional HIV risk behaviour research has been based mainly on individual cognitive-behavioural approaches stressing factors such as knowledge, self-efficacy and perceived risk (Amaro and Raj, 2000). A feminist perspective on health behaviour acknowledges that sexuality and behaviour are embedded in a specific social context shaped by gender roles and power structures, which is often overlooked in research on sexual risk taking (Amaro et al., 2001). Gender is a social construct that structures daily life through normative gender roles and power imbalances. However, experiences are never structured by gender alone, and this is where the concept ‘intersectionality’ comes in.
‘Intersectionality’ is a concept rooted in black feminist scholarship of activists and scholars such as bell hooks, Kimberlé Crenshaw and Patricia Hill Collins (Collins, 1990; Crenshaw, 1991; Lutz et al., 2011). Arguing that racism and sexism influenced their lives simultaneously, they stressed that classical theories about racism or sexism were inadequate to study black women’s experiences of combined oppression. The concept of ‘intersectionality’ is used to point out that every individual is positioned in society on a range of axes of difference such as gender, ethnicity, class and sexuality, and the combination of positions on these different axes is linked to different constellations of power. The intersection of these axes will determine a person’s opportunities in society and experience of discrimination. Sexism, racism, but also discrimination based on social class, sexual orientation or gender identity thus should not be viewed as self-contained forms of discrimination, but are always interwoven. They do not just add up with each other: it is the intersection of all of these that determines the experience of discrimination.
This feminist analysis serves as a critical review of current literature on transgender and non-binary persons and sexual risk taking. First the methodology used for this article will be outlined. Next, prevalence and risk behaviour data will be briefly summarised and the selective focus of current research will be questioned. A feminist and intersectional approach is then used to better understand the involvement of transgender and non-binary persons in sex work and their heightened risk for HIV and other sexually transmitted infections (STIs). The last part further investigates the binary gender perspective used in most literature on transgender sexual risk taking.
Methods
Data collection and selection
For this article multiple studies on transgender sexual risk behaviour and prevalence of HIV or other STIs published from 2005 to 2015 were screened. Since the 1990s there has been some research on transgender persons and risk of HIV. The reason why articles published within the last 10 years are used is that older research might be less relevant as knowledge and treatment options for HIV/AIDS, as well as knowledge and understanding of transgender and non-binary persons have been evolving rapidly.
Searches for peer-reviewed articles in English were repeatedly carried out between October 2015 and May 2016 on Web of Science and Google Scholar. Terms used were ‘transgender’, ‘gender non-conforming’, ‘Male-to-Female (MtF)’, ‘Female-to-Male (FtM)’, ‘crossdresser’, ‘(gender)queer’, ‘transsexual’, ‘transvestite’ and ‘HIV’, ‘Sexually Transmitted Disease/Infection (STD/STI)’ ‘sexual health’, ‘sexual risk taking’, ‘sex work’, ‘condom use’. To further extend the number of articles used for this review, the reference lists of all articles already obtained were consulted and all relevant cited articles published within the 10-year time frame were checked.
Studies included (n=47) were articles on prevalence and risk behaviours (self-report data (n=14) as well as test result data (n=11)), contextual factors associated with sexual risk behaviour (n=17), needs assessments aimed at developing interventions (n=1), (systematic) reviews (n=5) and meta-analyses (n=2). All articles initially obtained were screened by the authors and articles were excluded (n=6) if one of the following criteria applied: articles providing prevalence data that did not differ between transgender and non-binary persons and other populations (e.g. male sex workers or LGB populations), articles about persons having sex with transgender and non-binary persons that did not include data on transgender and non-binary persons themselves, articles using data obtained more than 15 years ago and articles with samples that contained fewer than five transgender and non-binary persons in their analysis. The final number of articles included in this review is 41. Of these 41 remaining articles, 20 contained empirical prevalence data, which is summarised in Table 1 below. 1
Studies providing HIV prevalence data (n=20).
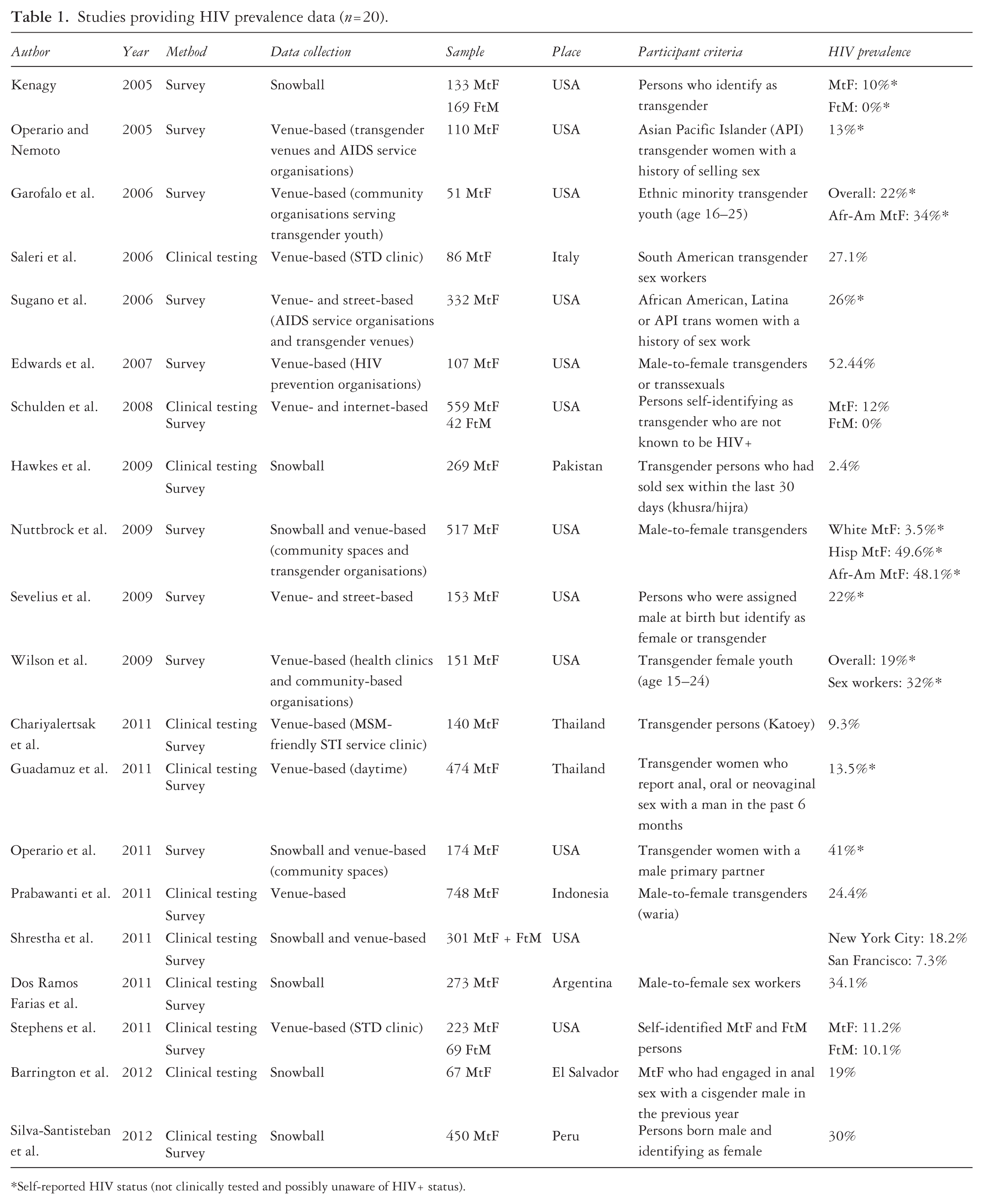
Self-reported HIV status (not clinically tested and possibly unaware of HIV+ status).
Following the five-stage framework (identifying the research question, identifying relevant studies, study selection, charting the data and collating, summarising and reporting the results) described by Arksey and colleagues (2005), this study is a scoping review of the existing literature aimed at identifying gaps in research and inviting critical reflection. A qualitative feminist discourse- and content analysis of the selected articles was carried out, with special attention to different intersectional positions and processes, in line with reviews such as Koehn, Neysmith, Kobayashi and Khamisa (2013) and Özbilgin, Beauregard, Tatli and Bell (2011), who also critically reviewed literature through an intersectional lens.
Results
Ten years of research: Who is studied (and who is not)?
As summarised in Table 1, HIV prevalence among transgender women is found to be high, while HIV prevalence rates appear to be low to non-existent among transgender men, although studies including transgender men are scarce. A meta-analysis of 29 studies focusing on HIV status among transgender women in the USA (of which five studies also included data on transgender men) indicated that 27.7% of transgender women tested HIV+, while 11.8% self-reported being HIV+ (Herbst et al., 2008). A systematic review of 39 studies resulted in a global HIV prevalence rate of 19.1% in transgender women (Baral et al., 2013). Furthermore, prevalence rates are higher for transgender women of colour (Garofalo et al., 2006; Herbst et al., 2008; Nuttbrock et al., 2009). Nuttbrock and colleagues (2009) for example, found an HIV prevalence rate of 3.5% for white transgender women in their sample, whereas the prevalence rates for Hispanic and African American transgender women were respectively 49.6% and 48.1%. Risk behaviours also appear to be high among transgender women. Inconsistent condom use with primary as well as non-primary or commercial partners, unprotected sex in serodiscordant relationships (in which one partner is HIV+), drug use and sex work are frequently reported (e.g. De Santis, 2009; Guadamuz et al., 2011; Kosenko, 2011; Nemoto et al., 2012; Operario et al., 2008b, 2011; Sausa et al., 2007; Wilson et al., 2010). An added risk factor for transgender and non-binary persons to contract HIV is sharing needles to inject hormones, frequently used to make their body look more feminine or masculine (Crosby and Pitts, 2007).
Inclusion criteria
As shown in Table 1, prevalence rates for transgender and non-binary persons vary widely. A lot of studies use limited sample and data collection methods, mostly using interviews, focus groups, self-assessment of HIV status and non-representative convenience or snowball sampling. Studies using HIV test results (n=9) show higher rates than studies using self-reported HIV status (n=11), which could indicate that a lot of transgender and non-binary persons do not know their HIV status. Large differences in sample sizes exist, with samples ranging from 67 to 559 participants. Participants are mostly recruited in community centres, health clinics or AIDS service organisations that seek to promote safer sex within transgender and non-binary, LGBT or sex worker communities, which may lead to over-representation of persons who are at high risk for HIV. Often, studies on HIV in transgender and non-binary populations focus on transgender female sex workers (n=18), and though there may be a link between transgender and non-binary persons and sex work, the results from these studies cannot be generalised to the broader transgender population. Furthermore, most of the studies on transgender and non-binary persons and sexual risk tend to focus only on transgender women (n=32). Research including (n=8) or focusing specifically on transgender men (n=1) is scarce, and research focusing on gender-nonconforming persons who do not fit within the male/female gender binary is even more scarce. A substantial part of the existing research is US based (n=28). There have been some studies stemming from the Asia Pacific area (n=7) and South America (n=4), mostly focusing on transgender female sex workers, but European peer-reviewed articles are almost non-existent (n=1). Also, a few systematic reviews and meta-analyses exist (Baral et al., 2013; Herbst et al., 2008; Operario et al., 2008b), but these tend to throw a wide range of respondents together, aggregating data that cannot be compared, mixing for example sex workers with non-sex workers or samples from different national contexts that can be very different with regard to transgender rights and policies and attitudes towards transgender and non-binary persons.
Definitions and categorisation in current research
Many of the studies that were surveyed use a rather broad, in some cases even non-binary definition of ‘transgender persons’. However, looking more closely at the samples, most of the studies tend to focus only on MtF or FtM transgender persons, often without defining these concepts or taking the uniqueness of their bodies and experiences into account, assuming ‘standard’ male or female anatomy. This does not reflect the diversity of bodies and identities found within the transgender population. Many transgender and non-binary persons do not identify with one of the two available categories (FtM or MtF) but instead identify as non-binary or genderqueer (Richards et al., 2016). However, these persons remain excluded from most current research. Binary categorisation of gender identity is thus very limiting, but this is also true for sexual orientation, especially for transgender and non-binary persons (for whom labelling their identity might already be complicated) and their partners (Operario et al., 2008a). Up to now, research on transgender sexual risk taking remains highly heteronormative: most studies only take into account transgender women who have sexual relationships with men and engage in receptive anal intercourse. As with gender identities, however, transgender and non-binary persons identify with a variety of sexual identities, and engage in a variety of sexual behaviours (Bauer and Hammond, 2015; Sevelius, 2009).
Limitations
The limiting sample and data collection methods used in current research have been acknowledged by some researchers (e.g. Baral et al., 2013; Herbst et al., 2008). The non-random recruitment methods and the selective focus frequently used could partially explain the very high and varied prevalence data. There has been no peer-reviewed research using a large sample that could provide generalisations for the transgender population as a whole (such as a national health survey that accounts for transgender and non-binary persons), although generalisations based on current data are frequently (and wrongly) made. The ‘Injustice at Every Turn’ report, one of the most extensive surveys on transgender discrimination ever undertaken (n=6456), shows an overall HIV prevalence rate of 2.64% for transgender and non-binary persons, which is still four times the national average prevalence rate in the US (Grant et al., 2011), but much lower than most of the existing research indicates. Because of the large and diverse sample, this rate could be more reliable when estimating HIV risk for transgender and non-binary persons.
An intersectional experience of discrimination
Transgender and non-binary persons are legally recognised in some countries today, but laws restricting gender expression or recognition are still widespread and the human rights of transgender and non-binary persons are frequently violated (Stocks, 2015). Transgender and non-binary identities are still seen as deviant and are marginalised and stigmatised globally. Stigma affecting transgender and non-binary people is still high, and many transgender and non-binary persons feel discriminated against because of their gender identity and/or expression (European Union Agency for Fundamental Rights, 2014; Grant et al., 2011). Almost all of the studies included in this review acknowledge the role of discrimination and transphobia in the sexual risk behaviour of transgender and non-binary persons (e.g. Islam Khan et al., 2008; Kosenko, 2011; Operario et al., 2011; Sugano et al., 2006). Discrimination and stigma may lead to lower self-esteem, mental health issues, suicidal thoughts, a fatalistic attitude and the need for acceptance and approval from others, which appear to be high among transgender persons (Marshall et al., 2016). This in turn may lead to lower self-efficacy to use condoms and negotiate safe sex (Williamson, 2010). Transgender persons also face discrimination and social exclusion in health care settings, which leads to exclusion from HIV prevention and treatment services (Baral et al., 2013). Furthermore, because of stigma and discrimination, some transgender women have a heightened need to feel safe and loved and to be affirmed in their female gender identity, which they consider more important than their sexual health (Crosby and Pitts, 2007; Melendez and Pinto, 2007). A protective factor for the negative influence of discrimination on the sexual risk behaviour of transgender and non-binary persons is social support (Golub et al., 2010; Wilson et al., 2012). Unfortunately, a majority of transgender and non-binary persons report experiences with family rejection (Grant et al., 2011; Motmans et al., 2010). Transgender and non-binary persons tend to turn more towards their friends in situations of need in comparison with cisgender persons (Motmans et al., 2011). Social networks among transgender and non-binary persons play an important role in their lives (Reisner et al., 2009; Wilson et al., 2012), especially those online (Motmans et al., 2011), and transgender communities appear to be more densely connected than for instance the LGB community (Barrington et al., 2012).
Transgender and non-binary persons’ experiences of discrimination are complex and varied, and simultaneously influenced by other intersecting social positions (de Vries, 2015; Hines, 2010). The intersection of transgender identity with ethnicity, social class and citizenship status becomes clear when we look at the link between transgender persons and sex work, the topic that has been most documented in research on transgender sexual risk taking.
Intersections with class, ethnicity, citizenship status and passability
Research on transgender and non-binary persons and sexual risk taking frequently focuses on (MtF) transgender sex workers. This is no coincidence: transgender and non-binary persons face discrimination in housing, employment and access to social services, which may lead to economic marginalisation. This in turn facilitates the engagement of transgender persons in sex work (Collumbien et al., 2009; Crosby and Pitts, 2007; Herbst et al., 2008; Kosenko, 2011; Nadal et al., 2014; Sausa et al., 2007) and forces people into risky sexual situations, because this creates an imbalance in power to effectively negotiate safe sex (Kosenko, 2011). Prevalence rates for sex work among transgender women range from 15% (Bauer and Hammond, 2015) up to 67% (Wilson et al., 2009). This data might not reflect involvement in sex work within the broader transgender community, as has been discussed above, but reports using a more representative sample than the peer-reviewed studies included in this review, such as a Dutch LGBT study on sexual health (n=393) and the ‘Injustice at Every Turn’ sample (n=6456), show rates of 11% of transgender women being involved in sex work, while rates for cisgender women are much lower (estimated around 1–2%) (Grant et al., 2011; Rutgers WPF, 2013). The involvement of transgender men in the sex industry seems to be low, but is also largely undocumented.
Engagement in sex work significantly heightens risk of HIV (WHO, 2014). A systematic review of HIV prevalence rates among transgender sex workers indicates that 27.3% of the transgender sex workers over all samples included in the review were HIV+, whereas 14.7% of the transgender women not involved in sex work, 4.5% of the cisgender female sex workers and 15.1% of the cisgender male sex workers over all samples appeared to be HIV+ (Operario et al., 2008b). However, other studies claim that sexual risk behaviour is higher with primary than commercial partners, for instance because of fear of losing intimacy or negative attitudes towards condoms from the primary partner (Operario et al., 2011; Wilson et al., 2010). Many transgender sex workers endorsed a 100% condom rule for customers, but financial hardship may lead them to engage in unsafe sex with commercial partners too (Nemoto et al., 2012).
Economic hardship caused by discrimination is frequently cited as the main reason why transgender women engage in sex work, although there could also be other reasons, such as social support from the transgender sex worker community (Sausa et al., 2007; Wilson et al., 2009). Sex work could also allow transgender women to express their gender identity in a way that is highly symbolic in terms of gendered acts and social roles (Nuttbrock et al., 2009). Furthermore, the eroticisation of transgender bodies creates a large market for transgender women within the sex industry, and this sexual stereotyping of transgender persons may lead to stereotype-confirming behaviour (Kosenko, 2011). This is even more so for African American, Asian and Latina transgender women (Sausa et al., 2007), who experience a double exotification and eroticisation of their bodies, and face even more discrimination in the labour market. Ethnicity also plays an important role in engagement in sex work for transgender women. A study from Hwahng and Nuttbrock (2007) shows how within their sample of black, Asian and white sex workers, sex work is mainly seen as a way of survival by transgender women of colour, who usually have lower socio-economic status. This gives them less negotiating power for safe sex than white transgender women, for whom sex work appeared to be more recreational and part of the experience of dressing female, which placed them at significantly lower risk for HIV (Hwahng and Nuttbrock, 2007). Even within the group of ‘transgender sex workers’ large differences exist, which are shaped by the intersection of different positions in society and lead to different outcomes with regard to sexual risk.
Another factor at play in engagement in sex work is citizenship status, which is particularly relevant in the current context of European austerity policies that have increased poverty and inequality. As Sausa and colleagues (2007) found, some transgender and non-binary persons migrate to the USA looking for a more liberal society, leaving behind their conservative culture that did not accept their gender identity. However, transgender and non-binary persons frequently experience difficulties during their migration process in trying to acquire citizenship status (Seuffert, 2009). Once arrived in the country of destination, they are confronted with multiple barriers to social inclusion, such as lack of access to the mainstream job market, health care and insurance. These circumstances often facilitate engagement in sex work for transgender and non-binary migrants (Sausa et al., 2007). Undocumented transgender and non-binary migrants are even more pushed towards the sex industry for survival as they do not have any legal status, and as such are especially vulnerable to HIV. Furthermore, in some countries, sex work is illegal, which places transgender sex workers in an even more vulnerable position.
Passability as a cisgender woman seems to have influence on engagement in sex work for transgender women as well: transgender and non-binary persons who can be regarded as cisgender by others experience less discrimination on the labour market, which makes them less likely to experience social exclusion, which protects them from having to rely on sex work for survival (Sausa et al., 2007). Hormone therapy and surgeries that make the body appear more feminine are costly and many transgender women cannot afford these, especially transgender and non-binary persons who already experience discrimination because of their position on other intersecting axes. Even transgender women with a regular job sometimes use sex work as a way to save up for gender reassignment therapy (Sausa et al., 2007). Next to physical appearance, legal gender recognition also plays an important role in the passability of transgender and non-binary persons. But, legal gender recognition in most countries is, when available, still based on medical procedures. Not all transgender and non-binary persons have access to these trans care procedures or facilities, nor do all transgender and non-binary persons wish to undergo these. Large-scale studies in both the United States and the European Union have indicated that around 40% of the global self-identified transgender population have not sought psychological and/or medical help regarding their gender identity (Grant et al., 2011; European Union Agency for Fundamental Rights, 2014).
It is the intersection of transgender identity with gender, ethnicity, class, passability and citizenship status that will lead to this particular experience of discrimination which puts transgender persons at high risk for HIV. These axes of difference do not each on their own add up to the experience of discrimination, but instead are dynamically influenced by each other. As de Vries (2015: 21) notes: “labor markets are not solely divided by gender or race or sexuality. Rather, these blend together creating economic barriers for some and opportunities for others”. The combination of these different axes of difference leads to differences in power, which provide persons with more or less capability to enforce safe sex, and differences in the experience of discrimination, which might ultimately push people into sex work in order to survive. The notion of power is thus crucial in linking discrimination to sexual risk.
Binary perspectives
Regardless of the feminist, queer and trans studies canon, Western societies today still largely see gender as a given binary structure that shapes human interactions, institutions and policy making. As such, transgender and non-binary persons are marginalised and defined as deviant or pathological, which leads to further imbalances in power and ‘cisgender privilege’. ‘Cisgender privilege’ can serve as an extension of the concepts ‘white privilege’ and ‘male privilege’, as introduced by Peggy McIntosh (1990) to refer to unconscious and unrecognised advantages that make whites or men feel confident, comfortable and oblivious about race or gender and protect them from hostility and distress, but in turn leave non-white groups or women feeling uncomfortable, alienated and discriminated against.
Of course, the experience of privilege should also be seen as intersectional, as different types of privilege, such as class privilege, heterosexual privilege, age privilege, physical ability privilege or educational privilege, are always intertwined. Depending on their position on other axes of difference, transgender and non-binary persons can experience certain (dis)advantages in daily life. For instance, a passing white trans male has different life experiences and privileges in comparison with a non-binary person of colour, but both are confronted with disadvantages, hostility and distress that cisgender persons are not aware of.
Normative gender roles
The binary sex/gender structure is accompanied by normative gender roles that shape behaviour and expression. Some of the reviewed research has taken these normative gender roles into account. Sex acts, sexual scripts and even protection methods are gendered, and this could also have an influence on the sexual risk behaviour of transgender persons (Kosenko, 2011). The social construction of ‘the feminine’ has a strong impact on how transgender and non-binary persons perceive and construct their bodies and sexual behaviour (Bauer and Hammond, 2015; Rodriguez-Madera and Toro-Alfonso, 2005). As such, using a condom (an act usually performed by a male person) could be seen as a contradiction to their feminine identity, and receptive anal intercourse could serve as an affirmation of a female gender identity for transgender women (Herbst et al., 2008; Rodriguez-Madera and Toro-Alfonso, 2005). As noted above, sex work gives transgender women the chance to express a social role that symbolises their gender identity and as such also serves as an affirmation of their female gender role (Nuttbrock et al., 2009).
Knowledge and education
As pointed out above, most research on transgender and non-binary persons and sexual risk is still highly cis- and heteronormative, and so serves to maintain the limited binary gender perspective of Western societies. Mainstream knowledge about and education in sexual health also remain highly cisnormative today. Engaging in unsafe sex could be related to a lack of knowledge about HIV and safe sex or a wrong perception of risk for transgender and non-binary persons (Barrington et al., 2012). Some transgender persons seem to hold misconceptions about HIV and feel that safe sex information does not apply to them (Kosenko, 2011; Rodriguez-Madera and Toro-Alfonso, 2005). Furthermore, the HIV prevention needs of transgender and non-binary persons differ from those of MSM, but transgender women especially are still sometimes seen as part of the MSM community (Crosby and Pitts, 2007), which erases the specificity of their bodies and experiences. There is still a lack of knowledge about trans-specific safe sex behaviour and trans-inclusive as well as trans-specific sex education remain largely non-existent. Society’s binary perspective also influences the sexual risk behaviour of transgender and non-binary persons, who are still invisible or defined as deviant in knowledge, education and health care.
Conclusion
Within the European context, research on transgender and non-binary persons and sexual risk is almost non-existent. The same is true for Africa or other parts of the world except the USA, South East Asia or South America. Within the existing literature, there has been a disproportionate focus on the HIV prevalence and sexual risk taking of North American transgender women and transgender female sex workers. Research including transgender men or non-binary persons persons has been scarce. Yet, conclusions of this existing research are frequently generalised for the global transgender population as a whole and transferred to other contexts and localities. This is problematic, since countries differ greatly with regard to transgender rights, policies and attitudes towards transgender and non-binary persons and as such cannot be compared.
The influence of discrimination on sexual risk behaviour has been acknowledged in almost every article included in this review. Stigmatisation and discrimination of transgender and non-binary persons remains highly prevalent worldwide, and this seriously influences their vulnerability to HIV risk. However, transgender and non-binary persons’ experiences of discrimination are structured by a number of intersecting social positions, such as ethnicity, social class, citizenship status and passability. The intersection of these axes of difference determines economic barriers and opportunities and leads to differences in power, which provide persons with more or less capability to enforce safe sex. These power differences also lead to differences in the experience of discrimination, which might ultimately push people into sex work in order to survive. The intersectionality perspective used in this article could explain why some transgender and non-binary persons might have an elevated risk of getting HIV. However, a focus on specific risk populations within the transgender population is not enough. Taking the broader transgender population into account, some other problems emerge: society’s binary perspective also influences sexual risk behaviour, and trans-inclusive as well as trans-specific sexual health knowledge and education remain scarce. This cisnormativity contributes to the discrimination of transgender and non-binary persons, as they are still defined as deviant to the cisgender norm and their bodies and experiences are erased. In order to improve sexual health in transgender and non-binary persons, it is thus crucial to address discrimination, stigmatisation and cisnormativity in society, develop trans-inclusive policies and provide for trans-inclusive sexual education and health services.
Implications for research
Overall, more research on transgender and non-binary persons and sexual risk is needed. Future research should use large, more generalisable samples, for example by taking transgender and non-binary persons into account in national health surveys instead of only proposing male/female options. This research should be focusing on the broader transgender community as well as on high risk groups, and taking into account specific national and cultural contexts as well as the highly diverse nature of the transgender population. When studying sexuality and sexual health, gender identity and sexual orientation should be viewed as more fluid and complex and the diversity of transgender and non-binary bodies, behaviour and experiences should be considered.
As this article showed, it is important to assess the intersectional nature of the experience of discrimination with regard to sexual risk behaviour in transgender and non-binary persons. As Davy (2011) already pointed out, an intersectional approach in health care research is important to address questions of access to health care and health disparities. Some research cited in this article considers the role of ethnicity, social class, passability or citizenship status in estimating the sexual risk of transgender and non-binary persons, but other intersecting axes of difference should also be explored, such as for example disability or sexual orientation. These could also potentially contribute to a specific experience of discrimination that influences one’s vulnerability for HIV.
Implications for policy and health care
The policy implications of this article are many: in order to improve sexual health for transgender and non-binary persons, it is crucial for social policy to acknowledge the role of discrimination and stigma, for example by taking up gender identity and -expression in antidiscrimination legislation, or supporting transgender health care and services that serve the needs of transgender and non-binary persons. In doing so, the intersectional nature of the experience of discrimination should be accounted for. Policies should be designed to tackle discrimination in the housing and jobs markets, and transgender as well as non-binary persons should be able to get legal recognition without medical requirements. Access to health care and insurance should be ensured and gender reassignment therapy for transgender and non-binary persons, if desired, should be covered. Also, transgender and non-binary persons should be accounted for in migration policies, recognising their gender identity during registration and as a ground for asylum seeking, ensuring them security and safety and addressing possible problems they may face in reception centres for asylum seekers.
It is important that transgender and non-binary persons be recognised in policy programmes as well as in research, even if not focused on transgender and non-binary persons. Policy measures should aim at creating linguistic and bureaucratic categories that are non-binary, such as for example a third alternative for legal gender recognition. Governments should fund research focusing on transgender and non-binary persons and sexual risk in their specific national context and develop trans-specific safe sex interventions targeted to (parts of) the transgender population, as well as targeted prevention for risk populations to increase knowledge and safer sex behaviour. In addition, non-binary sexual education is needed that disconnects sexual acts from gender roles and bodily characteristics from gender identities, as well as safe sex interventions targeting the general population that include transgender and non-binary experiences and bodies. These could not only reduce HIV risk for transgender and non-binary persons, but also reduce stigmatisation and discrimination and ultimately make society less cisnormative. Making transgender and non-binary bodies and experiences a visible part of public discourse and no longer defining them as deviant is crucial to normalising their existence.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Notes
Author biographies
![]() ) at the Centre of Sexology and Gender at the University Hospital of Ghent. His expertise includes LGBTIQ new social movements, equality policy, human rights, discrimination, violence, well-being, health and quality of life. He is one of the founding members and current board member of the European Association for Transgender Health (www.epath.eu). Joz holds an MA in Clinical Psychology, postgraduate experience in Women’s Studies and a PhD in Social Sciences. He has a long record of policy driven research, both qualitative and quantitative, on LGBTI and gender equality issues.
) at the Centre of Sexology and Gender at the University Hospital of Ghent. His expertise includes LGBTIQ new social movements, equality policy, human rights, discrimination, violence, well-being, health and quality of life. He is one of the founding members and current board member of the European Association for Transgender Health (www.epath.eu). Joz holds an MA in Clinical Psychology, postgraduate experience in Women’s Studies and a PhD in Social Sciences. He has a long record of policy driven research, both qualitative and quantitative, on LGBTI and gender equality issues.