
Abstract
The NHS is facing a combination of lower spending and increasing demand. In response, NHS England is requiring local areas to substantially rethink and reshape services through Sustainability and Transformation Plans. These have been devised largely without the involvement of patients and citizens, giving rise to widespread concerns about service loss. Other structural changes are also taking place that have no obvious place for citizen engagement. All of this is highlighting the problem of a lack of local accountability and legitimacy for decision-making in healthcare. This commentary describes the changes, identifies the accountability gap and suggests a framework for future development.
Introduction
The issue of citizen accountability in the National Health Service (NHS) has been troublesome from the outset. In the 1940s, Nye Bevan famously quipped that “if a hospital bedpan is dropped in a hospital corridor in Tredegar, the reverberations should echo around Whitehall”. His victory over Herbert Morrison’s preference for local government control of health services ushered in fifty years of centralised control of the NHS, with citizen accountability channelled through Parliament and the Health Secretary (Timmins, 1995). A shift towards some form of localism slowly gained ground towards the end of the last century with a range of ad hoc initiatives like GP fundholding, practice-based commissioning and locality commissioning (Smith et al., 2009), but it was not until the Health and Social Care Act 2012 that a significant attempt was seemingly made to reduce the day-to-day involvement of central government politicians by empowering local clinicians and others working in the newly created clinical commissioning groups (CCGs) (King’s Fund, 2011).
Along with this localisation, modest attempts were made to give citizens a stake in the new machinery of governance. On the provider side, the emerging NHS foundation trusts (FTs) had a trust board and a part-elected body of governors, while GP practices were incentivised to have patient forums; on the commissioning side, CCGs were required to appoint a ‘lay member’ to their board to support engagement with patients and citizens. None of these could be said to have been significant or successful (Hudson, 2015), but arguably as long as patients and the public were satisfied with the way their health services were functioning there may have been little interest in greater citizen involvement.
The combination of the global recession and the austerity programmes pursued by UK governments since 2010 has changed the situation. Under intense financial pressure, the agency responsible for the day-to-day functioning of the NHS – NHS England – has required local areas to plan for radical reconfiguration of their services through the mechanism of Sustainability and Transformation Plans (STPs) in the hope of securing more cost-effective provision. These STPs have now become the catalyst for citizen action and opposition, and are casting a long overdue light on the issue of healthcare services and citizen accountability.
This commentary examines the nature and impact of STPs in the context of citizen accountability within the NHS, explores other changes that are contributing to a loss of local accountability in health and care services, and outlines some ways in which citizen accountability could be strengthened.
The emergence of Sustainability and Transformation Plans
The genesis of STPs lies in the seminal ‘Five Year Forward View’ (FYFV) published by NHS England (2014) which set out a vision of how healthcare services needed to change to meet the needs of the population. Greater emphasis was to be placed on prevention, integration of services, and putting patients and communities in control of their health, and a number of care models were proposed that were to be tested across the country at fifty ‘vanguard’ sites.
Since the vision underpinning these models was around ‘systems’ rather than separate organisations spanning secondary, primary and community care, there was also a need to develop some planning mechanism. STPs are intended to serve such a purpose. They were not mentioned in the FYFV, appearing much later in planning guidance issued in December 2015 (NHS England, 2015). Further guidance in 2016 (NHS England, 2016a) indicated that STPs were destined to be the main vehicle for planning services across areas in England – 44 areas were identified as the geographical ‘footprints’ on which the plans would be based and these had to be submitted to NHS England in October 2016. This tight timescale took hold without any consideration of how these new entities were to be led, structured and held accountable.
These changes are significant and have some apparent attractions. They could provide the vehicle for planning that was lost to the system when strategic health authorities (the bodies linking central government to local health areas) were abolished under the 2012 Act, and might serve as the catalyst for the holy grail of integrated health and social care services. Indeed, the new care models could presage a landmark shift in the NHS machinery that will challenge the purchaser–provider split that has dominated the policy landscape for a quarter of a century. However, the place of patients and the public in all of this appears not to have been considered.
The NHS, STPs and citizen accountability
The proposed changes foreshadowed by STPs have been less well-received by patients and the public who have been more concerned about the prospect of loss of access to valued services, especially accident and emergency facilities and maternity units. These concerns have only been heightened by their exclusion from the STP decision-forming process.
The rapid turnaround time demanded by NHS England between production of an STP and consultation on the contents left little time for meaningful engagement (House of Commons Public Accounts Committee, 2017). The patient ‘watchdog’, Healthwatch England, complained of the public being brought in at “the very end” of the process and being expected to “rubber stamp over-simplified plans” (Health Service Journal, 2016a). And in terms of accessibility, STPs have been found to consist of a mixture of jargon and technical language with few concessions to lay readers and those unfamiliar with the ways of the NHS (King’s Fund, 2017).
Even where those working in STP footprints might have wanted to engage more effectively with their populations, the attitude of NHS England hampered their efforts. Local areas were left uncertain as to when they were allowed to publish their plans, whether this should be the full plan or a summary version, and how they could control ‘unauthorised’ disclosure by their less constrained local government partners (Health Service Journal, 2016b). By mid-October 2016 hastily installed ‘footprint leaders’ were being told to publish only summary plans and even then only after they had been discussed with NHS England (Health Service Journal, 2016c). Some local authorities broke ranks and published full plans, though even here the crucial financial summaries were not made available (CIPFA, 2016).
This exclusion of patients and the public led to growing suspicion and resentment on their part (Boyle et al., 2017), especially when NHS England instructed STP leaders to actively reject Freedom of Information requests to see draft plans. Regardless of the content of the plans, the view took hold that they were simply a secret vehicle for cuts to treasured services. Even amongst STP leaders themselves, a sense grew that broader priorities were being lost in the centrally inspired drive to achieve financial balance (King’s Fund, 2016). By the time of the 2017 General Election, STPs had become a major political issue with the Labour Party complaining of “decisions [made] behind closed doors with no genuine involvement of local people” (BBC, 2017).
Cognisant of the problem, NHS England (2016b) published advice for local health and care leaders on how to ‘put the communities they serve at the heart of their work’. By March 2017 the ‘Next Steps’ document (NHS England, 2017) was acknowledging that “making progress […] cannot be done without genuine involvement of patients and communities” (p. 34) and STPs were instructed to “involve local people in what the plans are and how they will be implemented” (p. 35). However, with STPs having no formal status and with no mechanism of local accountability, the citizen voice remains thwarted.
All of this is serving to highlight an important public policy dilemma for NHS services. Whereas other local services such as social care, schooling and housing have at least some historical and current channel of local democratic accountability, the NHS has no such legacy. In addressing this dilemma it is important to understand the administrative status of STPs in terms of their accountability.
Accountability failure and STPs
In addition to weak engagement channels with patients and the public in strategic development, STPs face two further barriers to effective accountability – an ambiguous legal status; and an uncertain relationship with democratically elected local government.
Ambiguous legal status
STPs are non-statutory bodies with no formal powers yet needing to reach agreement with a raft of statutory agencies, each of which is pursuing separate agendas. In addition the STP footprint is often bigger than existing health and local government structures, leading to complex multi-agency relationships (A. Hudson, 2016). Although each of the footprints has a ‘leader’, the process of appointment has been murky. Each area was asked by national NHS bodies to select a named individual to lead the development of the plan, but the process seems to have lacked fairness and clarity as well as been heavily influenced at national level (King’s Fund, 2016). In the absence of any formal powers, or of local consent to the appointment, these leaders could not expect to command authority across the agencies in their area.
All of this has left STPs in an ambiguous position in relation to the statutory powers held by other agencies. Where a ‘significant transaction’ for a foundation trust is proposed, for example, the approval of more than half of the governors is required; staff must be consulted and engaged where any hospital transfer is involved; and local authorities have the power to call in proposals with which they disagree. It was not until the ‘Next Steps’ update on the FYFV was published in March 2017 (NHS England, 2017) that any belated indication was given as to how STPs were expected to evolve.
The Next Steps document is potentially far-reaching. It says STPs are to be “more than just the ‘wiring’ behind the scenes” (p. 32); rather they are to have their own “basic governance and implementation ‘support chassis’” (p. 33). This, it is said, will consist of: an STP board drawn from the constituent organisations and including “appropriate non-executive participation”; an appointed STP chair or leader subject to ratification by NHS England; and programme management support created by pooling expertise across local commissioners, providers and other partners (p. 33). This would amount to a fundamental rewiring of the previous major restructuring brought in as recently as the 2012 Health and Social Care Act, but there is still no indication that patients or the public would have any formal role in these new arrangements.
Marginalisation of local government
In the absence of a direct role for citizens in the STP process, an alternative route of influence is through the role of democratically elected local councils – in principle, key partners to the NHS in reshaping local services. Here again the evidence is disappointing. Only three of the 44 footprints had a leader from a local authority background (Public Sector Executive, 2016) and little or no consideration appeared to have been given to the fit between STPs and local government boundaries. Indications of a strained relationship soon appeared including local government publishing STP plans against NHS England advice or simply refusing to sign up to STP proposals (Health Service Journal, 2016a, 2016d).
Public and patient involvement (PPI) in the ‘New NHS’
STPs are only part of a complex wave of structural changes taking place across the NHS and local government that is raising questions about accountability to local populations.
Current mechanisms within the NHS for engaging patients and the public are weak and fragmented. Responsibilities are spread across Local Healthwatch, foundation trust (FT) governors, lay members of clinical commissioning group boards and patient reference groups based in GP practices. All are characterised by weak powers and limited engagement: FT governors are relatively powerless in relation to FT boards and are invisible to their small electorates; most CCGs are stuck on a failed engagement model centred on public meetings; patient reference groups are optional and focus on micro issues like patient appointment arrangements and opening hours; and Local Healthwatch has yet to prove itself as a ‘consumer champion’ (Carter and Martin, 2016; Hudson, 2015).
This situation is now further complicated by the rapidly shifting nature of commissioning and provision in the NHS and local government – changes that challenge the role and purpose of existing PPI mechanisms. On the commissioning side, the trend is towards a bigger scale of activity. National planning guidance (NHS England, 2016a) urges CCGs to come together and share senior leadership, decision-making, contracting and other management, or even formally merge. This is already happening across England in an ad hoc way, dependent upon local relationships. In London, for example, five CCGs are moving towards a single chief officer to match their STP footprint; and in West Yorkshire eleven CCGs covering a population of 2.5 million have formed a joint commissioning committee to make decisions on behalf of all of them.
Local government is also undergoing major change with separate local councils changing in nature by coming together to form ‘combined authorities’. More recently there have been major devolution settlements in some conurbations – Greater Manchester, for example, is bringing together 37 local authority and NHS organisations under a joint commissioning board (Walshe et al., 2016). Channels of accountability to local people are becoming increasingly incomprehensible in these larger, more remote configurations.
Similar issues arise on the provision side. Foundation trusts are coming together in a number of ways ranging from ‘buddying’ relationships, hospital ‘chains’, other forms of ‘group’ status and merger. Indeed, some areas are being encouraged to develop an ‘accountable care organisation’ model that seeks to combine both the commissioning and providing functions (NHS England, 2017). General practice – traditionally small scale – is not immune from this trend with practice mergers, the creation of GP hubs and locality-wide GP ‘federations’. In Suffolk, for example, 14 practices serving a population of 113,000 have combined into a single partnership. Again the existing models of PPI such as FT governors and patient reference groups are at risk of being swept further into irrelevance.
Meanwhile the scale of private sector delivery of publicly funded contracts is growing. Half of the spending on community health services now goes to private companies (Financial Times, 2017) while adult social care provision is now effectively entirely privatised (B. Hudson, 2016). This raises important and unresolved issues of accountability to service users and local citizens, especially where services are provided by companies owned by many thousands of shareholders owning shares that are traded through stock exchanges (Mulgan, 2000). The distinction between public and private law is still well entrenched and protects private companies from effective scrutiny and accountability.
Conclusion: Where next? Rethinking accountability
The combination of reduced budgets and increased demand has led health and social care organisations (via STPs) into significant restructuring formats and service plans. These have taken place with little public debate or citizen consent. In this process the already tenuous mechanisms for engaging and involving local people in decision-making have been further weakened and sidelined. Denied a legitimate and robust role, citizens have, literally, taken to the streets. This is a major weakness and suggests that a fundamental rethink is needed on the nature of local accountability for healthcare decision-making.
Accountability matters because in its absence those in power with the capacity to act might do so without regard for those whose lives are affected by the actions (Papadopoulos, 2010). The ways in which STPs and other changes are affecting local services and support are exposing the weaknesses in how public officials are acting to fulfil public trust. Policy networks, invisible to outsiders, are constituted in such a way that it is hard to identify those who are responsible for decisions – the paradox of ‘shared responsibility’ that can obscure clarity of accountability (Bovens, 2010). Within these networks both elected representatives and the wider citizenry can too easily come to be regarded as intrusive and potentially troublesome.
Current mechanisms of public and patient involvement in healthcare decision-making are weak and unsustainable – further tweaking of existing approaches would not be adequate. Martin (2008) notes the tendency towards selectivity and elitism in public-involvement practice, with a reliance on self-selection or the selection of acquiescent or financially better-off individuals. This results in only a few voices being heard, usually at the expense of socially marginal groups.
The bigger task is to rethink the whole notion of accountability and put in place a raft of options and opportunities that, in aggregate, bring people’s views and preferences squarely into the equation. The model in Table 1 – adapted from the framework developed by Conklin et al. (2010) – offers a menu for development.
Model for development of accountability.
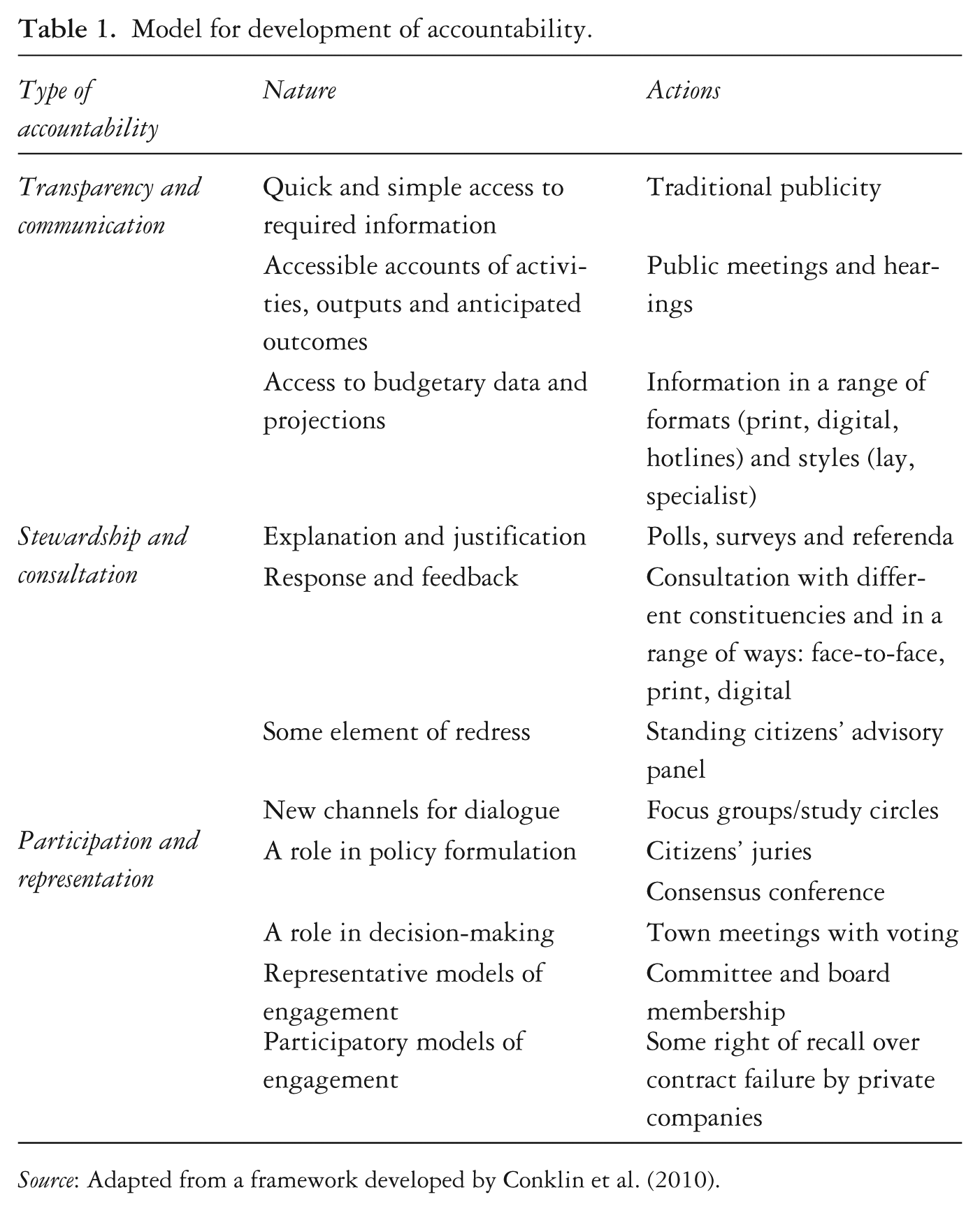
Source: Adapted from a framework developed by Conklin et al. (2010).
Conklin et al. (2010) note that public involvement has been advocated as a means to enhance the responsiveness of healthcare systems and it has been sought in various fields of health policy, including health service planning and delivery, health research and priority-setting. Yet despite its obvious appeal, the concept of public involvement has remained poorly defined and its rationale and objectives are rarely specified when applied to the healthcare sector. The threat to service availability from austerity policies, the structural turbulence on which no consultation has taken place, and the retreat of decision-making into obscure and opaque policy networks is rendering this deficiency unsustainable. Opening up this ‘black box’ and engaging with citizens will need to move from rhetoric to reality if the healthcare debate is to have legitimacy.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.