
Abstract
Little is known about correspondence between parents’ and children’s narratives after a child’s exposure to trauma. We examined 24 parent and child narratives of a child’s recovery using Linguistic Inquiry and Word Count, a software program that yields the percentage of words that fall into linguistic categories (e.g., personal pronouns) and psychological categories (e.g., emotion words). Analyses revealed significant parent–child associations for number of words, rate of cognitive processing words, and rate of anxiety words. No associations were found for anger or sadness words. With both similarities and differences in parents’ and children’s narratives, the current findings encourage further research in the domain of posttrauma narratives.
Almost everyone is exposed to a (potentially) traumatic event, such as a serious car crash, an assault, or a disaster in their lifetime (de Vries & Olff, 2009). Although immediate stress reactions are common, only a minority of the survivors need mental health care to support their recovery; most people recover naturally. Both in natural recovery and in treatment after trauma, narratives play a central role. In natural recovery, they are a vehicle for making meaning of an event, sharing experiences with others, and recruiting social support (e.g., Fivush, 2007; Harber & Cohen, 2005). In treatment, they are used for assessment purposes, as the starting point for exposure sessions, and for the modification of unhelpful thoughts. For example, in Prolonged Exposure Therapy (Foa, Hembree, & Rothbaum, 2007), clients recount their traumatic experience aloud for extended periods of time and listen to their recorded narratives as homework. Importantly, while children are frequently exposed to trauma, our knowledge about trauma narratives comes predominantly from adults.
Characteristics of narratives are related to physical and mental health outcomes. In experiments involving writing about stressful experiences, Pennebaker (1997) found that individuals who used a moderate number of negative emotion words in their writing (as opposed to small or large amounts) showed the largest drops in subsequent physician visits. A study on the narratives of survivors of assault showed that higher rates of cognitive processing words (e.g., “think,” “realize,” “know”) were related to lower posttreatment anxiety levels (Alvarez-Conrad, Zoellner, & Foa, 2001). In children, narrative characteristics also appear related to posttrauma outcomes. For example, the level of disorganization in a trauma narrative (e.g., use of confusing or nonconsecutive chunks, clear expressions of uncertainty) was found to predict acute stress symptoms in young survivors of assault or road traffic accidents (Salmond et al., 2011).
Parents have been shown to shape children’s narratives and autobiographical styles, with distal developmental outcomes as a result. Various theoretical frameworks, such as communication accommodation theory (Giles, Coupland, & Coupland, 1991), language style matching models (Ireland et al., 2011; Niederhoffer & Pennebaker, 2002), and social learning theory (Bandura, 1977) predict that children adapt to, or mimic, their parents’ language. Some studies have shown that the effects remain over time as well. For example, children of mothers who reminisce in a highly elaborative way (i.e., with long, detailed conversations) develop more coherent and emotionally expressive autobiographical narratives, have a better understanding of self, and regulate their emotions better than children of less elaborative mothers (Fivush, 2007). Several studies further suggest that mothers’ and children’s use of emotion and cognitive processing words—also referred to as mental state language—are associated (e.g., Kuebli, Butler, & Fivush, 1995).
Considering the findings above and the importance of parents’ role in children’s recovery in general (e.g., Morris, Gabert-Quillen, & Delahanty, 2012), it is likely that parents’ and children’s trauma recovery narratives show (at least partial) correspondence. Insight into parents’ and children’s trauma recovery narratives would allow a better understanding of their experiences and may provide new “levers” to enhance natural recovery and the effects of interventions. For example, it may lead to advice for parents on how to interpret children’s narratives or how to talk with their child after traumatic exposure, and for clinicians on how to tailor interventions to specific family members. However, virtually no empirical data have been collected on associations between parents’ and children’s narratives of children’s trauma. One notable exception is a study on narratives after a tornado (Bauer et al., 2005). Mothers’ use of mental state words in conarrations of the event with their children (4 months after the tornado) was related to children’s use of mental state words at a subsequent conversation 6 months later. Although this study provides important information, it included only one specific type of trauma exposure, and the narratives were not independently acquired (i.e., the narratives were acquired in conarrations, in which parents can directly influence their children’s narrative).
In the current study, we investigated the independently acquired narratives of trauma-exposed children and their parents. We aimed to explore two elements of the narratives: elaboration and mental state language. We operationalized elaboration as number of words in the narratives and mental state language as proportions of words referring to cognitive processes and emotions. With respect to emotions, we were interested in anxiety, anger, sadness, and optimism. Anxiety has traditionally been considered a core element of posttraumatic stress (Horowitz, 1997), leading to the initial categorization of posttraumatic stress disorder as an anxiety disorder in the Diagnostic and Statistical Manual of Mental Disorders–Fourth edition (American Psychiatric Association [APA], 2000). This categorization has now been changed into a trauma- and stress-related disorder (APA, 2013), acknowledging that a significant role can be played by other emotions such as anger and sadness (Dalgleish & Power, 2004; McHugh, Forbes, Bates, Hopwood, & Creamer, 2012). In addition, optimism has been suggested as an important predictor of recovery from trauma (Hobfoll et al., 2007).
In summary, based on the literature on emotion socialization and communication accommodation, we expected parent and child narrative characteristics to be significantly and positively associated. Specifically, we hypothesized that parents’ (a) total number of words; (b) rate of emotion words; and (c) rate of cognitive processing words would be positively related to their children’s total number of words, rate of emotion words, and cognitive processing words, respectively. We also expected to find differences between parents and children as groups, related to developmental differences in verbalization (Fivush, Sales, & Bohanek, 2008; Salmon & Bryant, 2002). In particular, we expected parents as a group to use (a) more words overall, (b) a higher rate of emotion words, and (c) a higher rate of cognitive processing words than children as a group.
Method
Participants
Families were recruited for a larger research project on child recovery from traumatic events. The details of the study procedures have been described previously (Alisic, Boeije, Jongmans, & Kleber, 2011, regarding the child interviews; Alisic, Boeije, Jongmans, & Kleber, 2012, regarding the parent interviews). The study protocol was approved by the Medical Ethics Committee of the University Medical Center Utrecht in the Netherlands. Eligible children were aged between 8 and 12 years, had been exposed to a single traumatic event at least 6 months previously, and were not currently receiving mental health care. The events met the A1 exposure criterion for posttraumatic stress disorder in the Diagnostic and Statistical Manual of Mental Disorders–Fourth edition (APA, 2000) as well as the exposure criterion of the Diagnostic and Statistical Manual of Mental Disorders–Fifth edition (APA, 2013). Written informed consent and verbal assent were obtained from the primary caregivers (further referred to as parents; all except two were biological parents) and the children, respectively. Within the timeframe of the study, 25 families out of the 34 approached consented. Of the 25 children, 15 were boys and 10 were girls (Mage = 10.7 years; SD = 1.04). The parents considered in the current analysis were 7 males and 18 females (Mage = 41.3 years; SD = 4.67). These children had been exposed to a traumatic event 10 months to 7 years prior to the study (median = 27 months). The traumatic events involved the sudden loss of a loved one (n = 6), violence (n = 8), and accidents that led to serious injury (n = 11).
Procedure
The parents and children were interviewed separately about the child’s traumatic event in a quiet room in the hospital or at home. The interviews were semistructured, with questions referring to the nature of the event itself, the child’s immediate reactions, changes in the child’s stress reactions over time, positive experiences, and factors that affected the child’s recovery. The wording of the questions was as open as possible, the interviews were conducted by an experienced, trained interviewer, and the participants could talk as long as they wanted. At the end of the interviews, every family received information about mental health care options. The core part of the interviews (excluding play with the children, introduction of the study, and ending) was audiotaped. One parent interview encountered a technical problem which resulted in an incomplete recording. Therefore, we excluded this interview and the related child interview from the subsequent analyses.
Coding and Analyses
The interviews were transcribed verbatim and participants’ narratives were submitted to the Dutch version of the Linguistic Inquiry and Word Count program (LIWC; Pennebaker, Francis, & Booth, 2001; Zijlstra, van Meerveld, van Middendorp, Pennebaker, & Geenen, 2004). LIWC provides quantitative information on elements of a given text across over 80 categories, including linguistic and psychological processes (see Tausczik & Pennebaker, 2010). The psychometric qualities of the program have been described extensively in Pennebaker, Chung, Ireland, Gonzales, and Booth (2007) and the psychometric equivalence of the Dutch to the original English LIWC dictionary has been established (Zijlstra et al., 2004).
Analyses involved the following LIWC categories: word count, cognitive mechanisms (e.g., “think,” “because,” “probably”), negative emotions (with its subcategories sadness, anger, anxiety), and positive emotions (with its subcategories positive feelings and optimism; Zijlstra et al., 2004). If two parents participated in an interview together (in seven cases), we randomly chose one of the parents to be included in the analyses. We identified three outliers (in the proportions of children’s anxiety words, parents’ sadness words, and parents’ positive feeling words; with a z score above 3.29) spread across participants. We transformed the outliers to the equivalent of a z score of 3 (cf. Field, 2005). Our main analyses involved descriptive statistics, Pearson product-moment correlations to examine associations between parent and child narratives in families, and paired sample t tests to identify differences between the group of parents and the group of children.
Results
General Characteristics of the Narratives
The 48 participants talked about a wide variety of topics. They shared memories of the event, their symptoms of distress (e.g., not being able to watch the news because items may show emergency services and remind of the trauma), and how these developed over time. They discussed coping strategies, such as seeking support from others, talking or avoiding talking about what happened, using rituals (e.g., designing a memorial stone together), and focusing on enjoyable moments. They also reflected on helping and restricting factors, such as excellent service at a hospital or a perpetrator who was unknown (see Alisic et al., 2011, 2012, for an in-depth qualitative analysis). The narratives were on average 2,887 words long (SD = 1,349). Almost 7% of the participants’ words reflected cognitive mechanisms, while 1.5% were negative emotion words (including anxiety, anger, and sadness) and 1.4% were positive emotion words (including optimism and positive feelings). Example quotes are provided in Table 1.
Examples of Word Use in Participant Narratives.
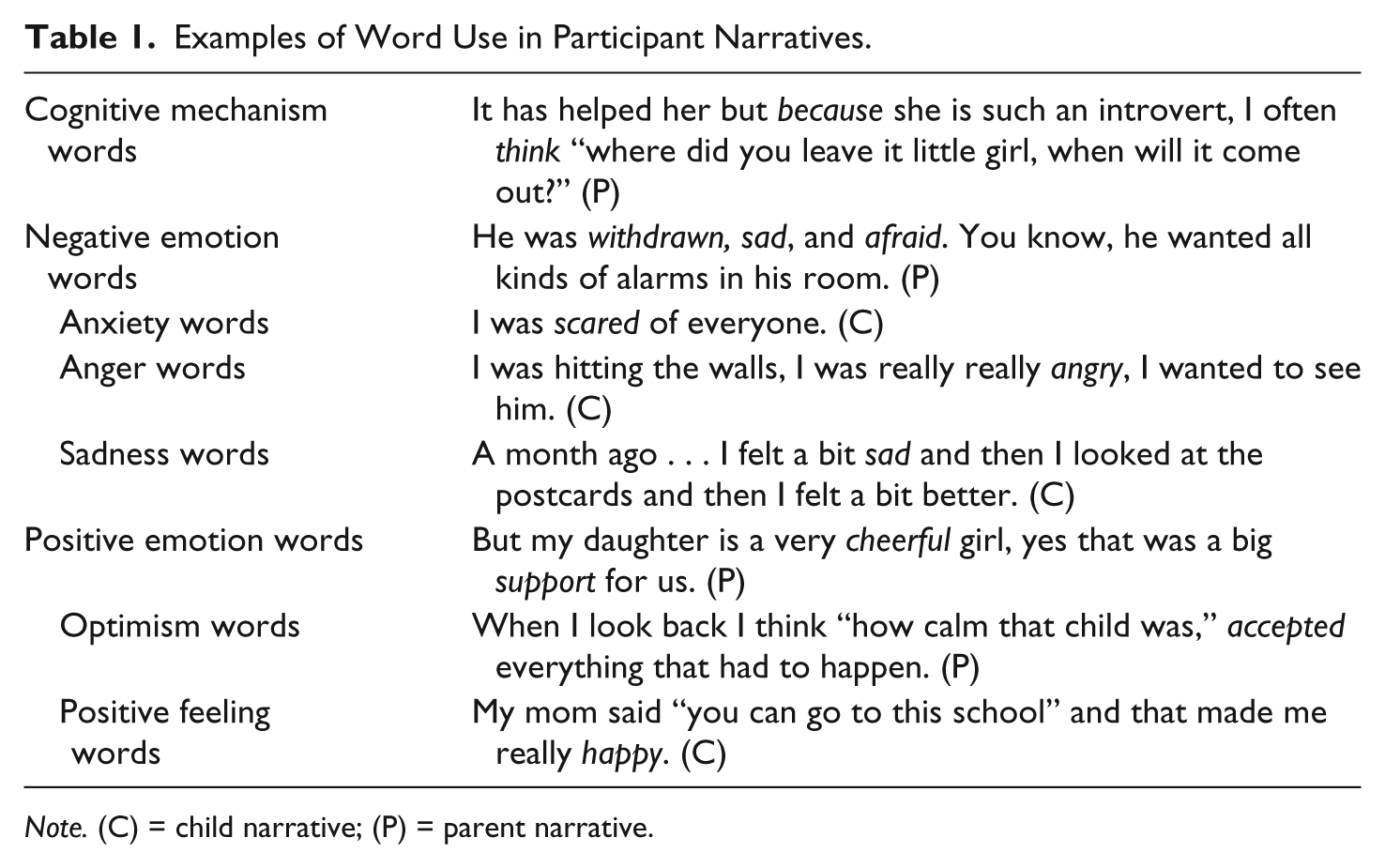
Note. (C) = child narrative; (P) = parent narrative.
Associations Between Parent and Child Narratives
Parents’ elaboration was significantly and positively related to their children’s elaboration; the correlation between parent and child word count was r = .43 (a medium effect based on the classification by Cohen, 1988). With regard to mental state language, greater cognitive mechanism word use in parents was related to greater cognitive mechanism word use in their children (r = .57, a large effect). There was no association between parents’ and children’s general rate of negative emotion words (r = .14). However, examining specific emotion categories, parents’ and children’s use of anxiety words were significantly related (r = .46, a medium effect), while no significant associations appeared for anger or sadness words (r = .23 and r = −.06, respectively). A similar pattern occurred for positive emotion words; while word rates in the overall category were not associated, the more specific categories showed varying associations, with the relation between parents’ and children’s optimism words being borderline significant (r = .34). Details on the interrelations are provided in Table 2.
Descriptive Statistics, Correspondence, and Differences Between Parent and Child Narratives.

Note. LIWC = Linguistic Inquiry and Word Count. LIWC categories except word count are percentages of the total amount of words in the narratives. The effect size of the paired sample t test (degrees of freedom = 23 for all comparisons) is expressed in Cohen’s d (mean of the difference scores divided by standard deviation of the difference scores; 0.2 is considered a small effect, 0.5 a medium effect, and 0.8 a large effect).
Differences Between Parents and Children as Groups
The parent narratives differed from the child narratives in various ways (see Table 2). Parent narratives were significantly longer (d = 1.08; a large effect), contained higher rates of cognitive mechanism words (d = 0.46; a small effect), lower rates of sadness words (d = 0.75; a medium effect), higher rates of optimism words (d = 1.02; a large effect), and to some extent, higher rates of positive feeling words (borderline significant with p = .07; d = 0.39; a small effect).
Discussion
Narratives are a central element of daily life, including after traumatic events (Adler, 2012; McAdams & McLean, 2013). Understanding similarities and differences among family members’ narratives can help tailoring assessment and treatment interventions, as well as increase a general understanding of these processes. The present study investigated similarities and differences in parents’ and children’s recovery narratives after a child had been exposed to trauma. The children in this study showed similarities with their parents in how they talked about their experiences; we found significant and substantial associations for length of the narrative (elaboration) and the rates of cognitive mechanism words, anxiety words, and, to some extent, optimism words. These results extend previous findings of similarities in conarrations where parent and child narratives are obtained together (Bauer et al., 2005). Our study extends this literature by revealing that similarities between parent and child narratives also exist when obtained separately, and therefore without parents directly steering the child’s narrative as she or he relays it.
These findings fuel the question whether parents shape children’s trauma recovery narratives in a structural way. In particular with regard to cognitive processes, where we saw the strongest correspondence, this may be an important field of further study. Cognitive processes, such as appraisal of the experiences and rumination about conflicts between new and previous beliefs about the self and the world, are deemed central in the development of traumatic stress symptoms (Ehlers & Clark, 2000). Specifically, trauma memory deficits, excessively negative appraisals of the event resulting in an ongoing sense of threat, and dysfunctional strategies to control the perceived threat are hypothesized to maintain posttraumatic stress (Ehlers, Mayou, & Bryant, 2003).
While rates of anxiety words were related, parents’ and children’s rates of anger and sadness words were not, in contrast to our expectations. It is possible that anxiety, which is traditionally seen as the core of posttraumatic stress, is more prone to socialization than other negative emotions. Overall, our findings suggest that not all emotion categories correspond equally in narratives; associations between parent and child use of emotion words appeared for some categories but not for all. In particular, the higher order “positive emotions” and “negative emotions” categories may obscure the associations for specific emotions. While unexpected in the context of our study, variation in the strength of associations across categories of emotion words has been reported for previous LIWC research among adults (e.g., Consedine, Krivoshekova, & Magai, 2012).
With regard to differences between the group of parents and the group of children, parents had longer narratives, higher rates of cognitive mechanism words, higher rates of optimism words, equal rates of anxiety and anger words, and lower rates of sadness words than children. While the first three differences were expected, based on the idea that children as a group would have fewer words and a shorter attention span for their narrative (cf. Salmon & Bryant, 2002), the latter two were not. In other words, parents did not consistently have higher rates of mental state language than children. In particular, the finding that children expressed proportionally more sadness and less optimism than parents is of interest. Perhaps parents and children had a difference in focus on the past (i.e., the losses and sadness related to the traumatic event) versus the future (i.e., possibilities), respectively. This would be in line with the suggestions of Tausczik and Pennebaker (2010) regarding verb tense in LIWC research. A post hoc analysis of our data showed indeed that parents used the past tense significantly less often, while they used the present and future tense significantly more often than the children.
The present study is exploratory in nature and its findings should stimulate further research rather than premature conclusions. Our main limitations are a small sample size, cross-sectional rather than longitudinal measurement, and an absence of concurrent in-depth mental health and attachment measures. Our findings do not allow for any conclusions on causation. Nevertheless, the study is unique by virtue of including independent parent and child recovery narratives about a range of single traumatic events and lays the foundation for future studies to elucidate the role of trauma recovery narratives in the family context. Moreover, our findings suggest that further study of parent and child trauma recovery narratives is important.
Future research will need to investigate whether the relations we found also arise over time and whether the effects flow from parent to child or (also) vice versa. Longitudinal studies, in which cross-lagged effects are taken into account, can answer these questions. For example, while we found correspondence in parent and child levels of elaboration in trauma recovery narratives and previous research found positive effects of mothers’ level of elaboration in general narratives on children’s outcomes (Fivush, 2007), a longitudinal design could help us start exploring whether teaching parents and children to be more elaborative in their recovery narratives facilitates well-being. In addition, rather than conducting “lab” tasks and experiments only, it will be necessary to study trauma narratives in daily life. Naturalistic observations, such as with the Electronically Activated Recorder (Mehl, Robbins, & Deters, 2012) may provide opportunities to examine natural language use in the family context in the aftermath of a traumatic event (Alisic et al., 2015). Furthermore, it would be useful to compare trauma narratives and their relations with those of other events. Finally, while previous emotion socialization and communication research has found gender differences and cultural differences in narratives and parent–child conarrations, this would also be of interest to test in the trauma context. For example, a naturalistic communication study with adolescents and their parents also showed that mothers demonstrated more similar styles with their daughters than with their sons (Beaumont, Vasconcelos, & Ruggeri, 2001). With regard to culture, a recent study suggests that school age children in India are less likely to express anger or sadness than children in the United States (Wilson, Raval, Salvina, Raval, & Panchal, 2012).
In conclusion, there are both similarities and differences in parents’ and children’s narratives of child trauma recovery. The current findings encourage more in-depth exploration of these narratives, within their natural context, and over time to ultimately promote an understanding of levers of trauma recovery in children.
Footnotes
Acknowledgements
We are grateful to the children and parents who participated in the study. We would also like to thank the anonymous reviewers and the editor for their helpful comments on drafts of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from two Dutch foundations, Stichting Achmea Slachtoffer en Samenleving and Fonds Slachtofferhulp, and a Monash University Larkins Fellowship.