
Abstract
The hospital-based care of pregnant women who are obese is complex. Current guidelines recommend early epidural analgesia, but there is disagreement about the guidelines and their implementation by anesthesiologists. In this study, we conducted semistructured interviews with 42 specialist anesthesiologists about their experiences implementing the “early epidural” recommendation. We examined the impact of intergroup identity and system factors on the language used by anesthesiologists to express their experiences, framing the work by social identity and communication accommodation theory. Leximancer text mining was used to elicit the dominant theme “epidural” in the interviews, and discourse analysis aided in exploring selected extracts. Findings indicated that anesthesiologists expressed their role primarily as technical experts, along with the core value of accommodating patients’ wishes. Furthermore, the extent to which they were prepared to accommodate the perspective of other health professionals was a key indicator of the intergroup climate.
Keywords
The maternity care of women who are pregnant and obese (WPO) may involve midwives, general practitioners, anesthesiologists, and obstetricians. One issue in their care that has received much attention in recent years is the best way to provide pain relief for WPO in labor, and in particular, how and when epidural analgesia should be applied. An epidural catheter is a thin plastic tube, placed using a needle inserted between the bones of the spine and used to administer local anesthetic to the nerves around the spine, providing relief from the pains of labor. In spite of the lack of a high-quality evidence base, professional guidelines recommend that anesthesiologists should routinely provide obese women with epidural analgesia early in labor. There is significant controversy about this guideline and uptake is far from universal. Furthermore, as maternity care in hospital involves many different health professions along with patients and their families, pain relief can become a site of intergroup tension and conflict. Patients and their families have personal and cultural views on pain relief in labor, which may not be consistent with those of health care professionals. Attitudes to pain relief among health-care professionals also vary. At one extreme, some midwives encourage intervention-free deliveries; at the other, anesthesiologists offer and recommend epidural analgesia, the most effective but also the most invasive form of pain relief in labor. On this basis, there is reason to believe that the application of the early epidural guideline provides a context for intergroup conflict, and that it finds expression in (non)accommodative language.
In this article, the ways in which hospital anesthesiologists express their experience and reflect the hospital culture and climate in implementing (or not) early epidural analgesia (EEA) guidelines were examined using social identity theory (SIT; e.g., Tajfel & Turner, 1979) and communication accommodation theory (CAT; e.g., Giles & Soliz, 2014). We believe anesthesiologists have a strong role-based identity, demonstrating dominant core values around their technical expertise. Enacting these values leads them to adopt an intergroup stance in their communication with other health professionals, which is influenced strongly by the intergroup relations in the hospital. The EEA recommendation is likely to be a trigger point about which there is significant intragroup disagreement, and which may lead to nonaccommodative communication (see Gasiorek, 2016) between health professionals caring for WPO.
Maternal Obesity and EEA Guidelines
Maternal obesity is increasing in prevalence, consistent with increasing obesity in the general population (World Health Organization, 2016). Body mass index (BMI) is used to classify obesity according to a person’s weight and height. In Queensland between 2009 and 2013, 19.4% of pregnant women were classified as obese (BMI > 30) and 4% had a BMI > 40 (known as Class III obesity), which is associated with the most severe health consequences (Queensland State Government, 2015a). Women who are pregnant and have a BMI > 40 are considered to have high-risk pregnancies, and they are more likely than other women to suffer gestational diabetes, preeclampsia, stillbirth, and blood clots (Cedergren, 2004; Robinson, O’Connell, Joseph, & McLeod, 2005). WPO are more likely to require caesarean section, sometimes urgently (Chu et al., 2007; Knight, Kurinczuk, Spark, & Brocklehurst, 2010; Sullivan et al., 2015), and for this reason are more likely to require anesthetic services, often in a time-critical manner.
From 2006, several interpretive reviews by expert anesthesiologists have strongly suggested that WPO should routinely have epidural analgesia inserted early in labor (EEA: Mace, Paech, & McDonnell, 2011; Saravanakumar, Rao, & Cooper, 2006; Soens, Birnbach, Ranasinghe, & van Zundert, 2008). Their rationale is logical; if an epidural is placed early in labor, it is easier to insert and, should caesarean delivery become necessary, medication can be administered via the epidural, providing anesthesia and thereby avoiding general anesthesia. The risks of general anesthesia, especially in urgent conditions, are greater in for WPO than for other women (Douglas & Preston, 2011; Quinn, Milne, Columb, Gorton, & Knight, 2013). 1 The underlying aim of the EEA guideline is to reduce risk: avoiding rare but disastrous complications of general anesthesia in WPO is an overriding priority for anesthesiologists (Quinn et al., 2013). As we noted above, there is a greater chance that WPO will need surgical intervention (e.g., caesarian section), and the risks of general anesthesia for these women are greater than for women who are not obese. Thus, an early epidural that avoids this outcome is likely to bring benefit. However, there are also risks with an epidural, including problems with insertion, drug administration, and effectiveness, and these risks are also greater for WPO than for women who are not obese. 2 Furthermore, the woman may not want an epidural and may resent the coercion to have one (Eley et al., 2014). The whole process of EEA may also turn out not to be necessary; the woman may deliver naturally without further intervention and the catheter may not be used.
From 2007, guidelines from international professional bodies in the United States (American Society of Anesthesiologists Task Force on Obstetric Anesthesia, 2007), Canada (Davies et al., 2010), and the United Kingdom (Centre for Maternal and Child Enquiries, 2010) have used cautious language to recommend EEA for WPO. The U.S. guideline cautions that there is a lack of evidence, and the U.K. guideline states: “An early epidural may be advisable depending on the clinical scenario.” In Queensland (and more generally in Australia), state government guidelines follow the recommendations of the larger international bodies, and the guideline current at the time of this study did not strongly recommend EEA (Queensland State Government, 2010). In Australia, specialist anesthesiology doctors provide obstetric care for maternity patients in public and private hospitals. They provide anesthesia for planned and emergency caesarean sections and provide epidural pain relief for women in labor. Despite the cautious language used in formal guidelines and in a profession striving for evidence-based practice, opinion leaders in anesthesia have encouraged the practice of EEA in WPO.For instance, in one anesthetic clinic, we found that WPO are counselled to and do change their minds from using other forms of pain relief to planning for epidural analgesia in labor (Eley, Donovan, Walters, Brijball, & Eley, 2014). We also found that some WPO experience emotional distress after receiving this recommendation, signaling a potential lack of accommodation to the woman by anesthesiologists, in favor of following the local protocol. While WPO may be advised to have an epidural, healthy women who are not obese are encouraged by midwives and obstetricians to make their own choices when deciding on pain relief preferences in labor and do not participate in an antenatal anaesthetic appointment.
In sum, the issue of EEA is ambiguous and complex, which is the kind of hospital context that others have found to be likely to involve intergroup communication (Hewett, Watson, Gallois, Ward, & Leggett, 2009; Lingard et al., 2004). Therefore, we frame this research with CAT and SIT.
Professional Identity and Interprofessional Communication
The interprofessional dynamics of hospital-based maternity care reflect the complex nature of staff relationships in health care organizations. Despite an overarching goal of providing maternity care, staff members are divided into groups based on their work-based roles, training, and skill sets (Hewett et al., 2009). For example, there are perceived and real power differences between midwives and doctors (Watson, Heatley, Kruske, & Gallois, 2012), with each profession promoting the model of care that best serves its own power base. In order to provide EEA, anesthesiologists need to navigate these complex intergroup relationships. There are real and virtual territory boundaries, and anesthesiologists must communicate across them.
Relationships between health care professionals have previously been examined using SIT (see Hewett et al., 2009, for examples in the hospital context). SIT describes how individuals’ self-concept and self-esteem are influenced by their membership of groups (in-groups); in certain contexts, group memberships are the strongest influence on these variables (Leach, Watson, Hewett, Schwarz, & Gallois, 2016). (. Individuals are members of more than one group, and their behavior will change depending on which group membership is salient at the time of an interaction. According to this approach, in the hospital environment, anesthesiologists are likely to view themselves as members of an in-group of anesthesiologists, as well as doctors, health professionals, and so forth. The in-group enhances self-esteem by promoting positively distinctive descriptions of the self and the group (Palomares, Giles, Soliz, & Gallois, 2016). (). Interactions by anesthetists with obstetricians, midwives, and WPO usually occur away from the operating room, which is their most usual and comfortable environment. SIT theorizes that the context of interactions will influence which identity is salient at any given time (Giles and Maass, 2016; Harwood & Giles, 2005), and we expected context to influence the communication strategies of anesthesiologists.
The importance of anesthesiologists’ nontechnical skills, including communication with patients, families, and colleagues, has been increasingly recognized since the 1980s (Flin & Maran, 2015). Nontechnical skills such as communication and collaboration feature prominently in the CanMEDS Framework (Frank & Danoff, 2007), with technical ability being a comparatively smaller component of the overall “medical expert.” However, anesthesiologists’ nontechnical skills have typically been studied in reference to episodes of patient care that occur within the context of the operating room environment (Crossingham, Sice, Roberts, Lam, & Gale, 2012; Flin & Maran, 2015). Teamwork and communication by anesthesiologists have also been analyzed within this context (Bleakley, Allard, & Hobbs, 2012; Bleakley, Boyden, Hobbs, Walsh, & Allard, 2006; Lingard et al., 2004; Lingard, Reznick, Espin, Regehr, & DeVito, 2002). These researchers have found that the group memberships of health professionals (which they call tribes) are strong influences on their communication (and particularly on underaccommodation; see below), and that an important consequence of nonaccommodative communication is lower quality patient care.
Communication by anesthesiologists to and about their patients and colleagues as they perform their role outside of the operating room, however, has not been extensively examined before. Increasingly, anesthesiologists provide services outside the operating room. The labor ward is one such location; others include bronchoscopy suites, cardiology suites, radiology suites, and mental health facilities. Evaluating anesthesiologists’ communication outside the context of the operating room is important, because consistent with SIT, the context in which interactions occur is likely to influence how they experience communication with patients and staff in those environments (Giles and Maass, 2016).).
Different communication strategies may enhance or minimize the differences between interdisciplinary groups in health care. CAT (e.g., Gallois, Ogay, & Giles, 2005; Giles & Soliz, 2014) elucidates the sociolinguistic strategies used by speakers to achieve this (along with perceptions and reactions), based on their motivation and intergroup orientation in any encounter. Speakers may accommodate (make adjustments to their verbal and nonverbal behavior, language style, language) in order to reduce differences across intergroup boundaries, which is likely to facilitate successful communication, or they may not accommodate in various ways, which is likely to raise the intergroup temperature (Harwood & Giles, 2005; Watson, Jones, & Hewett, 2016). Hewett and colleagues (eg Hewett, Watson, & Gallois, 2015) observed that in times of conflict, doctors were more likely to underaccommodate in their interactions with other doctors (not change toward the behavior of others; see Gasiorek, 2016; Gasiorek & Giles, 2012). Individuals may also engage in stereotyped communication, as a way of promoting a positive in-group identity (Palomares et al., 2016). For example, Hewett et al. (2015) found that specialist doctors used in-group jargon in medical record entries which members of other specialties did not understand; anesthesiologists, similarly, may rely on in-group jargon and technical concepts that other health professionals or (particularly) patients do not know.
The Present Study
Anesthesiologists, therefore, are likely to feel discomfort and tension about the EEA guideline and its implementation, as this process involves communication with patients and colleagues from other professions. Their language and communication, and especially the extent to which these are (non)accommodative, should be good indicators of their perceived quality of intergroup relations and their attitudes toward members of other salient groups. Beyond their communication with others, their communication about other salient groups is also likely to signal their intergroup perceptions. In this study, we asked anesthesiologists about their experiences with the EEA guideline, and we explored their narratives, focusing on the ways in which they described their own behavior and that of colleagues and patients.
The study team included a specialist anesthesiologist who conducted the interviews (VE), an academic obstetric physician providing care to WPO (LC), an intensive care physician (JL), a senior academic anesthesiologist who coauthored one of the interpretive reviews on EEA (AZ: Soens et al., 2008) and an expert in health communication (CG). Each author has his or her own bias. For example, the senior anesthesiologist maintains that EEA is the correct approach in WPO, whereas the first author has observed significant practical problems instituting the recommendation and is acutely aware of the lack of supporting scientific evidence. The study took place in public hospitals, where anesthetic care is provided only by specialist doctors (not nurse anesthesiologists), and health care is primarily government-funded.
Using CAT, the language of anesthesiologists was explored to determine the impact of the EEA guideline on perceptions of anesthesiologists’ interactions with midwives, obstetricians, and patients, and how their professional identities were expressed. In this context, anesthesiologists mainly described interactions which took place outside the operating room. We chose a qualitative approach because of the dearth of literature on this topic and the necessity to capture the communication of participants in rich detail. We posed two research questions:
For Research Question 1, we examined anesthesiologists’ expressed attitudes toward EEA and the extent to which the guideline affected the core skills and values in their identity as anesthesiologists. We also explored how they expressed their relationship to WPO, and how accommodative they seemed to be, as they implemented the guideline (or did not do so). For Research Question 2, we looked at anesthesiologists’ descriptions of their interactions with other health professionals, and explored their accommodation with these out-group members in the context of doing an early epidural.
Method
Participants
A total of 259 specialist anesthesiologists working at nine selected public hospitals in South East Queensland were e-mailed a recruitment invitation via their professional college, The Australian and New Zealand College of Anaesthetists. Purposive sampling was used, and only anesthesiologists undertaking current obstetric anesthetic practice were chosen for the final sample. The minimum level of experience was Year 1 of specialist practice; no maximum level of experience was set. The Australian and New Zealand College of Anaesthetists training program consists of 5 years, commencing after a minimum of 1 year of postgraduate medical training. In Year 1 of specialist practice, anesthesiologists are fully qualified and wholly responsible for the care of their patients and for trainee anesthesiologists working under their supervision. Maximal demographic variation was sought, so that a range of anesthesiologists different in sex, age, practice patterns, and locations were recruited. Participants worked at hospitals that were different in size, location, and level of anesthetic and maternity services. In 2013, delivery rates ranged from 1,923 to 5,470 per year at these hospitals, accounting for 44% of the state’s deliveries (Queensland State Government, 2015b). Theoretical saturation (Sandelowski, 1995) was used to identify the completed sample of 42 anesthesiologists who met the selection criteria. When new ideas ceased emerging from the interview transcripts, no further interviews were conducted. Data were collected between February and April 2015.
Materials and Procedure
After accepting the invitation, participants were contacted at their place of work. Prior to the interview, participants completed a written questionnaire to provide demographic data, which included their age, sex, years of practice, and proportion of practice dedicated to obstetric anesthesia. Semistructured interviews (see the appendix for interview protocol) were conducted with participants by the first author, in a private location at the participant’s place of work. This location proved to be more suitable for participants and also encouraged snowball recruiting to augment the sample. Interviews were scheduled at the convenience of the participant, lasted between 30 and 60 minutes, and were audio-recorded with participant permission. Verbatim transcription was performed by a professional transcription service, and all transcriptions were checked by the first author for accuracy.
Data Analysis
Leximancer™ text-mining software (Smith & Humphreys, 2006) was used to organize the thematic analysis. Leximancer has been previously been used as a thematic analysis tool in health communication research (e.g., Baker, Gallois, Driedger, & Santesso, 2011; Cretchley, Gallois, Chenery, & Smith, 2010; Hewett et al., 2009). Based on the frequency of words and their co-occurrence, Leximancer creates concepts, which are words that co-occur frequently; it then groups co-occurring concepts into themes. Leximancer recognizes the boundaries between sentences, paragraphs, and documents and measures co-occurrence within two-sentence blocks. Words such as “and” and “of” are excluded from the analysis via a customized “stop-list,” that removes words of weak semantic value. The program displays concepts and themes visually as a two-dimensional map, as well as calculating indices of the prominence and co-occurrence of concepts. Examples of the context and co-occurrence of concepts can then be directly analyzed from the relevant text extracts. Leximancer has advantages compared with traditional methods of qualitative analysis, as the themes and concepts are identified automatically, reducing coding bias. This software differs from other programs such as NVivo™ in which researcher interpretation occurs after themes and concepts are identified, rather than during the process of developing concepts (nodes in NVivo) and their relations. Thereafter, analysis still depends on interpretation by the researcher, who must read and analyze all relevant extracts. In this study, after conducting the initial mapping process, we analyzed the text by reading and rereading text extracts related to the concepts contained in the most prominent theme epidural, and relevant to the research questions.
As an anesthesiologist and investigator, VE had “insider” status. Fluency in the jargon and terminology of the targeted group facilitated the establishment of rapport, allowing participants to divulge more information than they may have otherwise shared. The risk of insider status is the potential for the researcher to make assumptions about the meaning of interview transcripts. Constant reflection during interviews and analysis was necessary to recognize and avoid this and reduce the impact it may have had on the data. CG reviewed the analysis and text extracts. In-depth reading of the transcripts occurred throughout data collection, to allow theoretical saturation to be identified. Ethical approval was granted by the University of Queensland (2014-SOMILRE-0101); all participants provided written informed consent.
Results
The demographic profile of participants is shown in Table 1. While the weight and BMI of the anesthesiologists was not measured, observation and estimation revealed no obese anesthesiologists in the sample. The Leximancer map is shown in Figure 1. Reclustering the map demonstrated stability. Sequential maps were created in which the same concepts (within each theme bubble) were represented in the same relationships (the spatial relationships of concepts within themes and of themes with each other), supporting the reliability of the analysis (Smith & Humphreys, 2006). If words are semantically confused or used ambiguously by speakers, an unstable map is produced (i.e., each time the map was created, there would be different concepts within the themes and the themes would have a changing spatial relationship). Figure 1 also shows the concepts within themes, identified by Leximancer according to their frequency of use and co-occurrence with other concepts. The theme “epidural” is the largest, and its red color coding indicates that it is the most important in terms of both frequency and connectivity with the other themes and concepts (Leximancer Manual, 2011). After reading the extracts, we found that the three themes were related to overlapping concepts:
Demographic and Practice Information on 42 Specialist Anesthesiologists in South East Queensland.
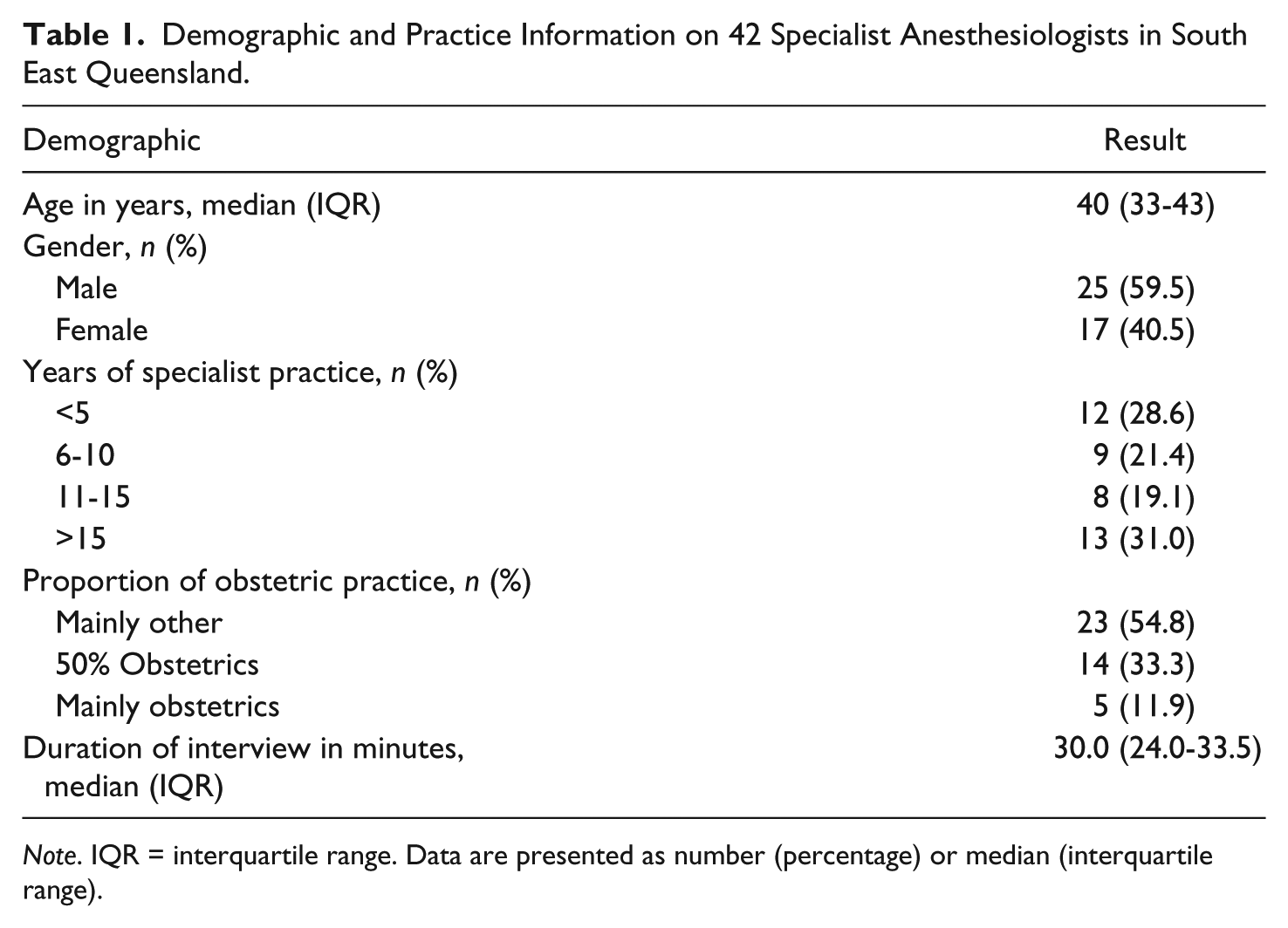
Note. IQR = interquartile range. Data are presented as number (percentage) or median (interquartile range).
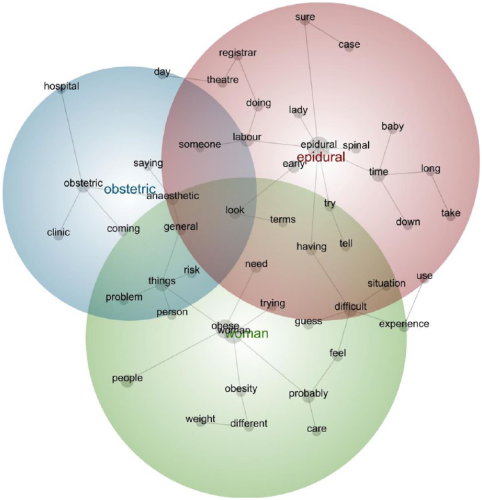
Leximancer map showing three major themes and their concepts.
Epidural—Included concepts regarding the concern of anesthesiologists regarding anesthetic technique in caring for WPO.
Obstetric—Included concepts concerning communication between anesthesiologists and obstetric staff.
Woman—Included concepts related to the demands placed on anesthesiologists when providing anesthetic care to WPO.
In order to answer the research questions, the text extracts pertaining to the concepts within the most prominent theme, epidural, were discourse-analyzed in detail through iterative and interpretative reading. Illustrative extracts are presented below; participants are identified by “P,” their identifying number, gender, and type of hospital.
Research Question 1: Influence of Identity on Communication About the Implementation of EEA
Complying With Patients’ Wishes
Despite the known recommendations for EEA, many anesthesiologists stated that WPO should make their own decisions about analgesia in labor, rather than be overly influenced by an anesthesiologist. P27 appeared keen to accommodate to the women’s need to lead the birth process and to set the priorities: I do wonder whether we are forcing all these people that don’t really want epidurals to have epidurals. I don’t force them to have an epidural in the birth suite if they don’t want one though, that’s for sure. (P27, male, tertiary hospital)
P27 was reluctant to override the preexisting birth plan of the pregnant woman, despite being aware that other anesthesiologists did make the recommendation. Force is a strong word, and signals this participant’s reluctance to use his power to make the patient comply. In the second sentence, he shows his lack of support for this practice and positions himself as on the side of the woman. This is consistent with a core value of anesthesiologists: keeping their patients happy by agreeing with their wishes.
In the face of a woman resisting the recommendation of EEA, other anesthesiologists also described how they would not persist in the recommendation, but would comply with the patient’s wishes. In particular, the birth plan (a plan for labor and delivery developed earlier in pregnancy by the woman and her team, which in general does not include an anesthesiologist) was blamed as a barrier to successfully making the recommendation of EEA: Yeah it’s the birth plan that gets in the way. If they’re expecting a nice normal natural delivery with no medical intervention at all, and the next thing is that you’re walking in to put in an epidural, because they’re not coping it’s, that’s, the first difficult part. (P9, male, regional hospital)
Women make a written birth plan in the antenatal period. The plans contain personalized lists of preferred treatment options during labor and are meant to be communicated to everyone involved in the birth. Anesthesiologists are more likely to see women for the first time in the final weeks of gestation (or only when they are already in labor), meaning that birth plans have already been finalized. Traditionally, anesthetic input late in the gestation is preferred; at this time, most complications with the pregnancy have been identified (e.g., preeclampsia, gestational diabetes, breech position of the baby, or diagnosis of a large baby). The plan for delivery (which may change throughout the pregnancy) will have been decided and this will determine the nature and content of any anesthetic recommendations. However, P9 highlighted the downside of late anesthetic input—that anesthesiologist’s involvement and opinion are not always welcomed, as they were not part of the original plan. In the previous extract, P9 described the plan as for a “nice normal natural delivery with no medical intervention at all.” In this way, he mildly derogates the woman as being naïve, perhaps aided in this by unspecified health professionals (e.g., midwives, nurses, obstetricians). His job is to fix the problem of the woman “not coping” because of this overoptimistic plan. His negative talk may be a defensive reaction: Birth plans are seen by some anesthesiologists as undermining their role. The plans are perceived to highlight their out-group status and make their opinions irrelevant. The path of least resistance for the anesthesiologist is then to comply (resentfully in some cases) with the woman’s birth plan.
Technical Expertise and Identity
Anesthesiologists described technical success in the insertion of the labor epidural as their main role in providing care for obese pregnant women, and they found significant satisfaction in achieving success: It’s probably the one that sticks in my mind because it’s the most recent, but I always feel some great joy when I get an epidural in a BMI of 50! Um, uh, when it’s working well. (P6, female, regional hospital)
P6 celebrated her joy at fixing the “problem” of obesity. Her reference to the patient as “a BMI of 50” rather than as a woman, patient, or person is a common strategy in doctors’ talk, and positions the patient clearly as a problem that needs to be solved with the anesthesiologist’s technical skills (she gets the epidural in). This characterization also suggests a degree of obesity stigma. Although they did not talk about being dictatorial in their recommendations, some anesthesiologists would prefer that WPO elected for EEA, to maximize their own chance of technical success and fulfilling their role.
While technical success was central to the identity of anesthesiologists, they did not want to be seen as technicians alone. Nevertheless, their reluctance to make strong recommendations, especially against the patient’s birth plan, tended to relegate their role to that of technician. In the extract below, the anesthesiologist indicates her resentment of colleagues: But a lot of the feeling is that epidurals are a bad thing . . . that there may not be a desire for some people in labor ward to have an epidural put in. I feel like we’re almost at the beck and call of them; when they request it, we do it. (P40, female, regional hospital)
P40 described a feeling of disempowerment and resentment of the out-group status she feels is cast on her by the “people in labor ward” (i.e., other health professionals). She also objectifies them (“some people”; “we’re at the beck and call of them”). P37, however, had a somewhat different view, and described her in-group’s role in the whole process: So if we’re just people who turn up in the . . . in the middle of the night and whip an epidural in and then disappear again and we’re never seen again, then we only have ourselves to blame if people don’t look on us a part of the team. (P37, female, tertiary hospital)
P37 reflected on how the behavior of anesthesiologists can detract from their effectiveness as team members. She states that altering their own behavior in a more accommodative way (not just whipping in an epidural and disappearing) may modify the intergroup stance of midwifery staff and obstetricians toward them. P37 also suggested that anesthesiologists may prefer to be somewhere else, rather than in the labor ward. Anesthesiologists may feel better equipped with the skills required for technical success, compared with the nontechnical skills required to negotiate an analgesic plan with a patient earlier in pregnancy, as part of her birth plan, or to navigate the “off-turf” context of teamwork on the labor ward. When they are out of their usual environment of the operating room, the professional identity of anesthesiologists is likely to be more salient and lead to the nonaccommodative behavior of “whipping in an epidural” (the skills of which they are confident) and returning to their familiar environment (the operating room or anesthetic department). They will have then satisfied key elements of their identity; they have “fixed” the problem of obesity with their technical prowess; they have a satisfied patient, and they may be able to avoid general anesthesia if surgery is required. While professional bodies may prioritize the importance of nontechnical skills like good communication in the desired characteristics of a specialist anesthesiologist, these participants expressed strongly that technical ability contributes significantly to their professional identity.
Research Question 2: Interprofessional Communication Accommodation and Implementation of EEA
Disagreement About the Guideline
There was intragroup disagreement on enacting the EEA recommendation. There were two strong positions expressed by anesthesiologists regarding making the recommendation of EEA, with all anesthesiologists aligning themselves with one of the two stances. Some anesthesiologists recognized the theory behind the recommendation but did not follow it in practice, largely deferring to the patient’s preference. Others strongly supported the recommendation and followed it whenever possible, even when this was against the patient’s wishes. The views of P28 were common; his recommendation is strongly affected by the initial preference of the woman in planning or not planning to have an epidural. In addition, he expresses a lack of confidence in the evidence supporting the guideline: Um, I don’t steer them towards having an epidural if they’re not planning one. Um, I know the concept is around that you, therefore, prevent general anesthesia. I’m not sure that’s completely proven, um, I’m not sure that necessarily, you know, very few women coming for an otherwise normal pregnancy and delivery end up having a general anaesthetic, so, I’m not sure about the numbers and whether it really pays to tell everybody with a BMI over some number that they should have an early epidural. The logic doesn’t seem to be there to me. (P28, male, tertiary hospital)
P28’s preference to follow the patient’s initial plan is apparent, as he doubts the efficacy of the recommendation and the supporting evidence. He referred to the patients as women, indicating a more accommodative stance toward them, and indicated that accommodating to them has higher priority for him than following a guideline with relatively little evidence behind it.
For some anesthesiologists, the potential legal implications of suggesting and implementing EEA for women who did not want it formed a second reason for not following the recommendation. Some individuals went further, emphasizing that they would recommend EEA without insisting as an attempt to change the woman’s mind, but would document carefully that the patient declined the recommendation: If the patient was very anti-epidural, I wouldn’t ever try too hard to talk someone into an epidural, in case they were the one that got the complication. So if they don’t want an epidural that’s fine, uh, I would recommend an early epidural and then document that I’d discussed it with them and that they didn’t want it. (P1, male, tertiary hospital)
P1 described “defensive documentation.” Citing fear of a complication, P1 implied that he had met his obligation by making the recommendation and had no responsibility to push the issue. While P1 was prepared to accommodate the patient’s wishes, he could be described as engaging in reluctant or even avoidant accommodation (Giles & Soliz, 2014). 3 Both of these forms of accommodation may be associated with resentment toward the other person or group. In this example, the attitude of P1 toward the patient was not positive, and this accommodation appeared to be mainly a way to avoid future problems and even future interaction with her.
On the other hand, the clinical practice described by P6 was typical of those anesthesiologists who strongly advocated EEA, without questioning the validity of the guideline: I strongly would suggest that you have an epidural to save you having a general anaesthetic. That would be my preference. (P6, female, regional hospital)
P6 reiterated the sentiment of all anesthesiologists interviewed, in wishing to avoid general anesthesia in WPO. In contrast to the other anesthesiologists, P6 was willing to communicate her strong recommendation, regardless of the woman’s plans. In doing this, she relied on her own expertise to show that she had the patient’s best interests at heart.
Anesthesiologists and Obese Maternity Patients
Descriptions by anesthesiologists of their care of WPO reveal a significant bias against the women themselves. P22 stereotyped obese pregnant women from a poor socioeconomic background as having low intelligence and an inability to understand the concepts behind their care. He specifically doubted their ability to understand the rationale behind why a WPO may have to be transferred to a larger institution which has better facilities and personnel: Because some ladies in this socio economic group in this institution have, some don’t have very good prenatal care and have very low education and probably wouldn’t understand, you know, the whole concept of that anyway. (P22, male, regional hospital)
When technical success was limited or prevented by the obesity of the patient, anesthesiologists expressed resentment toward the woman and a belief that her obesity was a preventable disease, described here by P3: It is something people could do something about and so I suppose that I think with the anesthesiologist there’s a bit of a resentment . . . There’s a resentment about the fact that because people have chosen not to look after themselves. You know, and that makes our life more difficult. But also, we’re expected to do as good a job. (P3, female, regional hospital)
P3 did not use the first person to describe her feelings toward obese patients, but instead referred to “the anesthesiologist,” “our” and “we.” In this way, she distanced herself from the reported emotions of her in-group, but also highlighted the intergroup context between anesthesiologists and patients. She also mentioned the potential for technical failure here, and she blamed this on the patients’ decision “not to look after themselves” which she perceived had caused their obesity. As technical success is central to the salient professional identity of the anesthesiologist, technical failure that is blamed on the patient will enhance the preexisting tension between WPO and anesthesiologists.
Reported speech (cf. Buttny, 2004) is a technique of softening an opinion by attributing it to others. This strategy is demonstrated by P7 in describing an interaction with a registrar who had been unable to insert an epidural in an obese pregnant woman: The way it was presented to me was that, that the reason I couldn’t get the epidural was the patient’s fault. (P7, male, regional hospital)
This phrasing means that P7 need not take personal responsibility for blaming the patient. However, P7 later showed that he does, in fact, share the opinion that the patient is to blame: Because this is a, a preventable condition and um, we now have got a, a crisis or a difficult situation, which otherwise wouldn’t be that way if this preventable condition hadn’t happened. (P7, male, regional hospital)
In blaming the patient, P7 still avoided saying that he is doing the blaming himself, by using the passive voice and not naming the woman (or patient). Nonetheless, he attributed the current situation (“we now have got a crisis”) on a longstanding factor (obesity—the “preventable condition”). Like P3, he positioned himself as the victim (put into a difficult situation) and resented the patient’s lack of attention to her preventable condition, obesity. In doing this, he indicated a nonaccommodative stance toward women who are obese and pregnant.
Anesthesiologists and Other Health Care Professionals
In addition to their interactions with patients, intergroup conflict with colleagues in other professions was evident when anesthesiologists described the practical application of the EEA recommendation. With anesthesiologists identified as the in-group, out-groups included obstetric doctors and midwifery staff, as the following extract shows: we say needs early epidural. I would put it to you that most obstetricians and midwives would think that just means we need more time because it might be difficult. I don’t know, maybe we should ask them . . . I don’t think they have this . . . any other idea on why we might want to get that epidural in early and, you know, and get it in in hours when there’s other help available. (P37, female, tertiary hospital)
P37 indicated that she believed that the midwifery staff and obstetricians did not recognize the needs of anesthesiologists. With different priorities to anesthesiologists, they were described as a homogenous out-group, although P37 did concede that she was not entirely sure of the other group’s perspective. She showed some vulnerability regarding technical success, predicting that she may need help. P29 went further, communicating negative intergroup relations with midwives in particular: I think all over the world, there is a bit of feeling against epidurals in, among midwives . . . Because um, . . . they [have to] work harder for the delivery in terms of monitoring. They sent this big paper saying that it works. I just had a quick read of the main thing and I think it’s a sham medicine. This is my personal feeling. Put, we’re sticking normal saline into the back and calling it, saying it works. And so that reinforces my perception that they, they don’t want anesthesiologists to have anything to do with pregnant women if they can help it. (P29, male, regional hospital)
In this extract, P29 indicated stereotyping of midwifery staff, blaming laziness on their preference against epidural analgesia. When any laboring woman has an epidural for pain relief, midwives are required to perform more frequent observations such as blood pressure and pulse rate monitoring. He openly criticized midwifery-led analgesia. The reference he made to “sham medicine” is to the practice of injecting saline under the skin in the sacral area, administered by midwifery staff for analgesia in the first stage of labor (Hutton, Kasperink, Rutten, Reitsma, & Wainman, 2009; Måtensson & Wallin, 1999). While several papers have reported significant benefits of this technique, it is not a service provided by anesthesiologists, some of whom are skeptical about its efficacy. This is evidence of boundary work (cf. Petronio, Ellemers, Giles, & Gallois, 1998), with the anesthesiologist unwilling to share the role of “analgesia provider” to laboring women with the out-group (midwives). P29 also perceived that anesthesiologists were not welcomed by midwives when attending the labor ward. The context of the midwife–anesthesiologist interaction occurring in the labor ward may enhance that perception by anesthesiologists, as they are out of their territory.
Anesthesiologists expressed frustration at being asked to administer epidural analgesia late in the labor of obese women, as it threatened their technical success. Late in labor, the pain of uterine contractions can be so severe that women are unable to sit still to allow safe epidural insertion. In the extract below, P21 expressed her significant frustration about an epidural that could have been administered much earlier to a less distressed woman. Conflict is evident as P21 goes from home territory (the anesthetic department) into the birth suite. The word “marches” evokes images of a military conflict: the message from the midwife was we’d like an epidural, this lady’s been stuck at eight centimetres since 10 o’clock this morning. So, I said, what’s the plan? Oh, well, she wants an epidural. Yes, but what’s the plan if she’s stayed stuck at eight centimetres since 10 o’clock this morning. Well, I’ve just been asked to phone you. Ah, okay, so you already get a, okay, on the phone, so, I went marching next door to the birth suite. (P21, female, regional hospital)
Her fury led to underaccommodation in the telephone interaction with the midwife (she maintained her own stance and did not move to address the needs of the other person in the encounter). The midwife in this extract also appeared to underaccommodate. Repetition of the phrase “what’s the plan” by P21 did not result in the desired answer. P21 suspected that a caesarean delivery was required, but she had not been involved in the planning; her out-group status has been emphasized, resulting in this high-tension interaction. P21 referred to midwives and obstetricians, who were physically located on labor ward (away from the operating room), and who she perceived to have excluded her professionally from the planning surrounding this woman’s care. In this case, midwives and obstetricians were described as a combined out-group. P21 also recognized the similarities between her experiences in the context of the operating room with experiences and interactions in the context of the labor ward: As an anesthesiologist, if you’re doing a complex operation and you don’t like your surgeon on the other side and you don’t think he’s doing a good job, your anxiety levels are sky high, and so I think in some ways the obstetric department here, we’re uncertain about some of the midwives, and certainly uncertain about some of the consultants [senior obstetricians] in terms of decision-making. (P21, female, regional hospital)
Anesthesiologists mainly described conflicting priorities dominating their interactions with midwives. They felt their own aims of providing early epidurals for WPO were at odds with the perceived preference of midwives to encourage a natural delivery without an epidural. However, some expressed respect for the midwife–patient relationship and recognized the potential for midwives to make early epidural insertion easier: We should not neglect the midwives because the patients trust the midwife more than any other part of the team. And given the pre-eminent relationship, I think the education in this aspect would be very valuable. And I, if they can provide extra mental reassurance and support and saying that yes, this could be difficult, it would carry a lot of psychological relief for the patient. (P23, male, regional hospital)
P23 used accommodative language to describe the superior relationship between the laboring woman and her midwife. He viewed the role of the anesthesiologist as less important, and he raised the prospect of collaboration between the two groups.
Conditions for Successful Intergroup Relations
Descriptions of the difficulties implementing the EEA recommendation were uniform across hospitals, with the exception of one. This small hospital provided only low-risk maternity services in a low socioeconomic area with a high rate of obesity. A large number of obese women wished to deliver at the institution (in order to be close to their social support system), which had a limited clinical service capability compared with the other hospitals. Key clinicians from the anesthetic department and obstetric department, therefore, had been required to define their service limitations and to have a unified approach for managing obese pregnant women, which is described by P18: she got them from a combination of British guidelines, the American guidelines, the Australian guidelines and, um, spending some time with our obstetric lead . . . She runs the obstetric department, you know, working out what the guidelines would be for . . . larger ladies. And it certainly seems to work. We do get the larger ones coming to the clinic. (P18, female, Hospital 5)
P18 showed a somewhat overaccommodative stance toward WPO, referring to them as “larger ladies.” Overaccommodation may be observed when an individual, often in an effort to accommodate, uses language based on negative stereotypes of a certain group (e.g., Gallois et al., 2005). This stance has also been termed inappropriate accommodation (see Gasiorek, 2016), as the stereotype may not pertain to the person concerned. In this case, P18 assumed that the WPO would not want to be called “obese” or “overweight” and used her own term “larger ladies.” The local guidelines at this institution were made specifically to match the limited resources of this hospital, rather than to accommodate the women’s wishes to deliver close to their home and social support system. Nevertheless, these cross-disciplinary activities by key members of the clinical specialties are likely to have improved the intergroup relationship among them to the point where the nearest tertiary center had become a shared out-group. This is confirmed by P14: It’s been difficult to get some of the tertiary centres to accept them when they’re still within our agreed BMI limit, early days, and they’d rather they stayed here and we moved them late, [and] the patients [would] rather that they were under the care of the same midwives and obstetricians throughout the majority of their care. (P14, female, Hospital 5)
These extracts indicate that a large in-group has emerged for anesthesiologists at this hospital, consisting of all staff caring for obese pregnant women at this institution. In fact, this group may include the pregnant women themselves. Membership of this group may be more salient than their professional identity as anesthesiologists, due to the service limitations of the hospital and the effectiveness of their collaborative activities. As the smallest hospital included in this study, the limited human and physical resources of this institution meant that uniform application of their jointly made guideline was essential. P14 described how patients’ preferences (to deliver in their local hospital, close to family and friends) had become secondary to the cross-boundary disagreement between the small regional hospital and the tertiary center to which they referred their high-risk patients. This was the only hospital in which all anesthesiologists described positive relations with other clinical groups, described here by P14: We are getting informed when the larger ladies are coming through so that we can catch them early and they are picked up at the handover and, yeah, and the obstetricians make a point of saying, “oh by the way her BMI is, you know, 40 whatever” so we know they’re there. (P14, female, Hospital 5)
This reportedly accommodative communication was very different to descriptions by anesthesiologists from the other hospitals, who consistently complained about late or no referrals for epidural analgesia in laboring obese patients.
Discussion
The aim of this study was to examine communication by anesthesiologists around the application of the EEA guideline, and the impact of intergroup relations—with WPO and with colleagues in other professions—on language and communication. Achieving technical success is central to the professional identity of anesthesiologists, along with a desire to please the patient and to avoid general anesthesia. Components of the epidural recommendation conflict with these core values—changing a woman’s mind toward having an epidural may not please her, but it allows technical prowess to be displayed and may prevent general anesthesia. The extent to which individual anesthesiologists adhere to these core values is strongly signaled by their communication about both patients and colleagues. In all but one hospital, conflicting intergroup priorities and late involvement of anesthesiologists in the birthing plan, obstructed the administration of EEA. In that hospital, prevailing practice conditions created one overarching group of maternity care providers with a unified approach to WPO.
Implications for Theory
Our results show the advantages of applying SIT and CAT in health care contexts. Anesthesiologists’ identities are strongly implicated in their relations with patients and other staff groups. The priority they place in the central value of technical expertise over nontechnical skills such as communication may hinder implementation of the recommendation and be a barrier to interdisciplinary teamwork. Anesthesiologists’ negative stereotypes about patients and midwives, as reflected in the language they used to describe these groups, contributed to a strongly intergroup context for their interactions.
Anesthesiologists described accommodative language in their interactions with patients; they tended to respect the wishes of patients even against their own desires. This attitude is likely to enhance smooth patient–doctor interactions and enact the core value of “keeping the patient happy.” There was evidence though, that this reluctant accommodation left anesthesiologists resentful and may have led to more negative stereotypes that would affect future interactions (Gallois et al., 2005).
Finally, this study identifies conditions where intergroup relations and communication are improved. The health context is complex, and intergroup relations can vary greatly as a function of system factors like access to resources and local aspects of the status hierarchies, rather than through longstanding conflicts based on group memberships (cf. Hewett et al., 2009). For example, in this study, at one institution, there was no intragroup disagreement between anesthesiologists regarding EEA. The development of a tailored set of agreed guidelines in this hospital produced a shared identity and a new salient out-group (the nearest tertiary center). This identity was reflected in the accommodative communication among staff.
Implications for Practice
There was skepticism among anesthesiologists in this study about the validity of using EEA with WPO, leading to significant variation in their interpretation and application of EEA in the women they cared for. This variation was exacerbated by the tendency for anesthesiologists to acquiesce to the wishes of their patients. It was evident that the recommendation of EEA is far from universally applied by this group. If anesthetic departments wish to successfully implement EEA in WPO, addressing this intragroup disagreement is necessary, as exemplified by the single hospital where the anesthesiologists had a uniform approach to the care of WPO. Anesthesiologists armed with evidence to support the practice of EEA (from large prospective studies, or audit of local outcomes) may be less skeptical about efficacy and more confident in making stronger recommendations against the wishes of their patients.
In addition, the contexts in which anesthesiologists work, and in which they express feelings of discomfort, could be significantly improved by more accommodative communication between health professionals, and between anesthesiologists and patients. For example, the disadvantages of late involvement by anesthesiologists in the antenatal period for WPO should be acknowledged. Early interdisciplinary birth planning would go a long way toward preparing women for the possibility of medical intervention during birth, and could result in better contingency planning in their birth plans. Furthermore, this kind of interprofessional teamwork would help anesthesiologists to be better integrated into the birth team, and enhance their comfort in working out of their preferred environment (their own department and the operating room). Overall, this kind of extra communication should aid decision making by the woman and allow effective multidisciplinary care.
Limitations and Suggestions for Future Research
The limitations of this study are recognized. Despite best efforts at recruitment, two hospitals were represented by only two participating anesthesiologists. The insider status of the first author may have facilitated participants’ responses in the interviews, but it also may have introduced bias in the final interpretation and synthesis. We acknowledge that the participants are likely to be a subgroup of anesthesiologists for whom this is an area of particular interest or disagreement. In addition, we have analyzed anesthesiologists’ interpretations of events and have not directly observed the communication and interactions that have taken place. We believe that the extent to which anesthesiologists showed a (non)accommodative stance toward patients and colleagues is likely to be reflected in the language they use when talking to these people (Gallois et al., 2005). This is a hypothesis, however, and needs to be tested in future research.
This is a study of anesthesiologists’ perceptions and the ways in which their perceptions are expressed in the language. Their perceptions are important in relation to this subject and are likely to influence their own communication and that of others with whom they interact (cf. Giles, 2016). Behavior is not the same as perceptions; furthermore, examining these interactions from the perspective of other health professionals would reveal how others perceive the behavior of anesthesiologists. Finally, consideration must be given to the role of the hospital system and the guidelines themselves, and their influence on the enactment of identity and intergroup communication. SIT and CAT will be important contributors to such research.
Conclusion
The early epidural administration recommendation is variably applied, with anesthesiologists deferring to patient preference, and this situation illustrates the complexity of communication in health care, particularly given the fragmentation among professions that exists today. Our results indicate that attempts by anesthesiologists to implement these guidelines are inconsistent and provoke preexisting intergroup tensions between anesthesiologists and patients and between anesthesiologists and other staff. The impact of intragroup disagreement, leading to intergroup hostility among the providers of maternity care, requires recognition and exploration in research focusing on patient outcomes, as well as changes in practice. Health care organizations must identify and manage the consequences of intergroup hostility and its communication in language in order to enhance the provision of quality care to this group of pregnant women.
Footnotes
Appendix
Acknowledgements
We would like to acknowledge the help of our participants and the hospitals in which they work. We are also grateful to the editor and two anonymous reviewers for helpful comments on earlier drafts of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a PhD Support Grant from the Australian Society of Anesthesiologists and a PhD Scholarship from the Royal Brisbane and Women’s Hospital.