
Abstract
Adults with congenital deafblindness and an intellectual disability are at high risk for exposure to chronic and severe stress. Sensory deprivation, separations from primary caregivers, and difficulties in communication, from birth on, make daily life stressful for them. Chronic and high stress can lead to deviancies in the cortisol curve. This, in turn, can have negative effects on mental and physical health. Nothing is known yet about the cortisol curve of adults with congenital deafblindness and an intellectual disability, but our hypothesis is that it will be deviant.
In this study, the cortisol curve of six participants with congenital deafblindness was compared to the curve of 40 typical controls. Remarkably, in spite of all past and present stress factors, the cortisol curve of the participants was rather normal. Possible explanations for this finding are discussed, amongst others individual differences in experiencing stress. Implications for further research are discussed.
Introduction
Individuals with congenital deafblindness (CDB) (dual sensory loss from birth) have a high prevalence of mental and behavioural disorders such as mental retardation, obsessive compulsive disorders, mood disorders, behavioural disorders, anxiety, psychosis and pervasive developmental disorders (Dammeyer, 2011; Hoevenaars-van den Boom, Antonissen, Knoors, & Vervloed, 2009; Luiselli, 1992; Van Dijk, 1982). In the group with acquired (post-lingual) deafblindness (ADB), individuals reported that the dual sensory loss negatively impacted their mental well-being which leads to increased anxiety, stress, depression and loss of self-esteem (Bodsworth, Clare, Simblett, & Deafblind UK, 2011; Capella-McDonnall, 2005; McDonnell, 2009).
Adults with CDB and an intellectual disability (ID), the target group of this study, face many challenges that may cause severe and chronic stress. Aside from their sensory deprivation, many of these adults have a history of social deprivation resulting from severe communication difficulties and stressful life experiences. Many of these people did not receive any deafblind-specific education or communication support adapted to their needs.
Although stress is a normal part of life, toxic stress can have very serious consequences. Toxic stress is defined as strong, frequent or prolonged activation of the body’s stress management system and it is provoked by stressful events that are chronic, uncontrollable and/or experienced without the person having access to support from caring persons (National Scientific Council on the Developing Child, 2009). Early in development, toxic stress can impair emotional well-being, exploration and curiosity, school achievement and other qualities (Nelson, Greenfield, Hyte, Shaffer, & Paul, 2011). Toxic stress is also known to lead to an increased risk of many conditions, like heart disease, diabetes, depression and anxiety disorders (National Scientific Council on the Developing Child, 2009).
Salivary cortisol can be used as a biological indicator of stress (Hellhammer, Wüst, & Kudielka, 2009). Cortisol is a glucocorticoid hormone that is produced by the adrenal glands as the end product of the hypothalamic-pituitary-adrenal axis (HPA axis). Cortisol is released in response to various biochemical agents and psychosocial stimuli, such as a challenging situation (Kirschbaum & Hellhammer, 1989). It plays a role in a person’s reaction to stressors and it is required for normal physiological regulation. In healthy individuals, cortisol levels show a circadian rhythm called the diurnal cortisol curve; levels peak in the early morning hours and are at their lowest around midnight (Lovallo, 2005).
The rhythmic pattern of cortisol secretion, resulting in the diurnal cortisol curve, is important for maintaining normal organ regulation and adaptive functioning. Impairment of this rhythm has been associated with poor long-term health (Kirschbaum & Hellhammer, 1989; Lovallo, 2005). In the short term, activations of the HPA axis tend to support adaptive functioning. However, there is substantial evidence to suggest that early and chronic exposure to high levels of stress leads to dysregulation of the HPA system (Fries, Hesse, Hellhammer, & Hellhammer, 2005; Gunnar & Vazquez, 2001) and increases the risk of physical and behavioural problems (Gunnar & Quevedo, 2007). Elevated cortisol levels have been found, for example, in emotionally maltreated children (Bruce, Fisher, Pears, & Levine, 2009) and in children who have a history of exposure to trauma and show symptoms of post-traumatic stress disorder (PTSD) (Carrion et al., 2002). Chronic stress and prolonged hyperactivity of the HPA system are believed to eventually result in down- regulation of the system or hypocortisolism, characterized by blunted cortisol responses to stressors and a flattened diurnal cortisol curve with low morning values (Fries et al., 2005; Heim, Ehlert, & Hellhammer, 2000; Loman & Gunnar, 2010). Low morning cortisol levels have been observed, for instance, in nonhuman primates exposed to repeated maternal separations (Sánchez et al., 2005), in children raised in neglectful institutions (Carlson & Earls, 1997) and in foster children, especially those with a history of neglect (Bruce et al., 2009).
Although adverse circumstances are likely to have a negative effect on cortisol levels, there are individual differences. Some of the variability in cortisol levels across individuals seems to be due to genetic differences (Clements, 2012; Nicolson, 2007) and coping styles (Nicolson, 2007). Nelson et al. (2011) also mention temperamental characteristics as a protective factor against toxic stress. Individuals perceive and evaluate situations differently and this perception, combined with the resources available to control the situation, determines how stressful an individual finds a situation (Lovallo, 2005).
The aim of the present study is to examine the diurnal cortisol curve in adults with CDB and an ID. No prior research results have been published about the cortisol curve in people with deafblindness, though other groups have been studied. For instance, the diurnal cortisol variation was smaller for blind individuals than for control subjects (Sack, Lewy, Blood, Keith, & Nakagawa, 1992). Sterkenburg, Janssen, Blankenstein, and Schuengel (2008) found a relatively flat cortisol curve in adolescents with an intellectual and visual disability who showed challenging behaviour; their cortisol levels were also lower in the morning and higher in the evening compared to a normative sample. In a group of children with severe and profound intellectual disabilities, Terstegen et al. (2003) found rather normal cortisol variation but one-third of the participants lacked a circadian rhythm. In sum, studies among persons with disabilities have shown some deviations of the diurnal cortisol curve as compared to control groups, but the findings do not show a distinct, constant pattern.
There is reason to believe that the diurnal cortisol curve of adults with CDB and an ID will differ from that of individuals without disabilities. First, individuals with deafblindness experience a lack of light and sound. Lack of light is known to affect circadian rhythms, for example, production of melatonin (Arendt, 2000). Second, because of the absence of well-functioning vision and hearing, daily life may be less predictable and controllable. This is known to lead to a rise in cortisol levels (Dickerson & Kemeny, 2004; Kirschbaum & Hellhammer, 1994). Third, many adults with CDB and an ID have a history of social deprivation as a result of, amongst other things, an atypical communication pattern and the experience of stressful events such as early separations from their primary caregivers because of hospital visits or entering an institution (Van Dijk, 1982; Van Dijk & Janssen, 1993). The exposure to such stressors may be expected to further contribute to deviancies in the diurnal cortisol curve in these individuals.
The present study was aimed at determining the diurnal cortisol curve of six adults with CDB and an ID, and comparing them to a control group consisting of 40 typical adults. First, we hypothesized that the cortisol curve of the participants with CDB and an ID would be lower and flatter than the curve of the control group. Second, we expected to gain more insights into individual variations between the curves of the participants and into the stress physiology of this unique population in general.
Materials and methods
Setting and participants
The assessments were conducted at Royal Visio, De Brink, a Dutch residential setting for individuals with intellectual and sensory disabilities. The study followed the tenets of the World Medical Association Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects, and was approved by the board of Royal Visio, De Brink. Written consent was obtained from the participants’ legal representatives.
Initially, seven adults with CDB and an ID (four males, three females) participated in this study. One of them, a woman, rejected the saliva sampling; as a result, too little saliva was collected to analyse her samples, and she was excluded from the study. During the saliva collection, the average age of the six remaining participants was 42 years (ranging from 37 to 48 years). They had been living at De Brink for 27 to 38 years. At the time of the study, they lived in group homes together with three to six others, with one or two staff.
The degree of sensory disabilities differed. Table 1 gives an overview of the relevant sample characteristics. The information was collected from the participants’ files at De Brink. As a child, all participants experienced life events related to maternal separations and housing changes. In the participants’ files, two to five maternal separations during the first five years of life are mentioned, mainly for hospital visits. All participants were living in an institution before the age of 11.
Participant characteristics
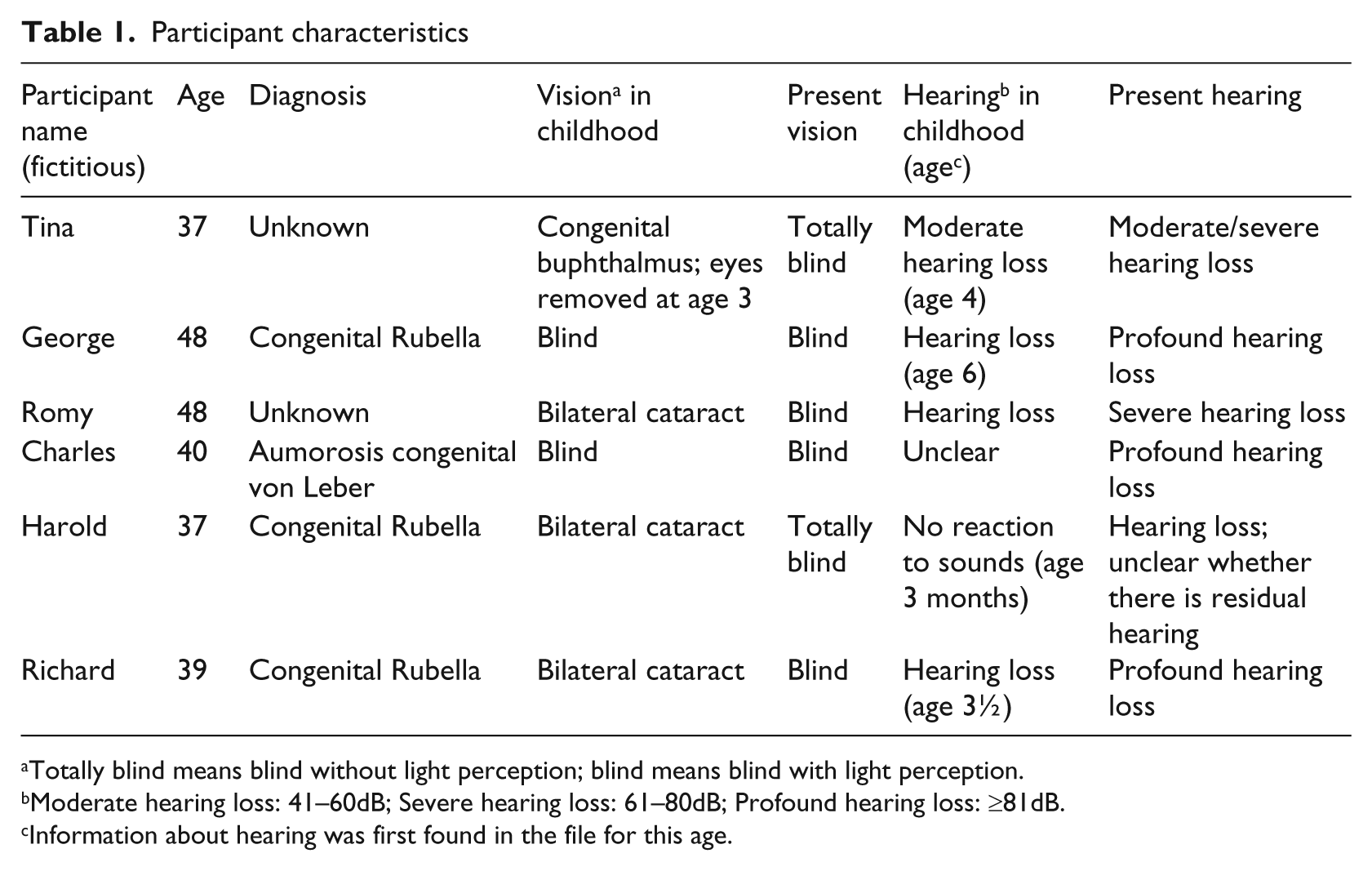
Totally blind means blind without light perception; blind means blind with light perception.
Moderate hearing loss: 41–60dB; Severe hearing loss: 61–80dB; Profound hearing loss: ≥81dB.
Information about hearing was first found in the file for this age.
Cortisol assessment in saliva
The use of saliva to determine cortisol levels has some important advantages: it is non-invasive, it is not painful and the samples can be collected at the participants’ home (Clements, 2012). Repeated measurement in the daily environment can provide a good estimate of the participants’ basal levels and diurnal variation (Nicolson, 2007).
Saliva was collected using a sterile cotton roll, which was swabbed along the person’s inner cheek and under the tongue to absorb saliva. It was stored in a Salivette in a refrigerator. Within one week, the samples were transported to a freezer, in which they were stored frozen at −20°C until analysis. Salivary cortisol was measured by radioimmunoassay (RIA) after extraction with dichloromethane and subsequent paper chromatography (Meulenberg, Ross, Swinkels, & Benraad, 1987). The samples were analysed at the Department of Laboratory Medicine, Radboud University Nijmegen Medical Centre, in the Netherlands.
Saliva samples from the participants with CDB and an ID were collected on seven days over a four-week period. On each day, five samples were collected at the following moments: just before getting up (mean (M) 7.56 h), before breakfast (M 8.48 h), before lunch (M 12.03 h), before dinner (M 16.52 h) and before going to bed (M 21.28 h). The saliva samples were collected by those caregivers who usually worked with the participants. The caregivers were asked to refrain from giving coffee, cola or orange juice to the participants within half an hour before the sample was collected. Caregivers also refrained from brushing the participants’ teeth within 30 minutes before sampling.
Control group
The control group was created by combining two control groups from a study of Eijsbouts et al. (2008), both consisting of 20 typical adults, into one new control group of 40 adults. Inclusion criteria were self-reported health, age between 18 and 47 years, normal physical examination and normal electrocardiogram. Exclusion criteria were pregnancy, an abnormal medical history or physical examination, medication use, endocrine diseases and psychiatric diseases. This control group was chosen because their samples were analysed with the same method and at the same laboratory as the study group’s samples. The saliva samples were collected from the control group at 4.00 h, 8.00 h, 12.00 h, 16.00 h, 20.00 h and 24.00 h. The 4.00 h samples are not included in the results.
Statistics
For each of the participants with CDB and an ID who had sampling moments with at least five values, outliers were calculated with the formulas Q1 – 1,5 × IQR and Q3 + 1,5 × IQR (Moore, McCabe & Craig, 2009). Outliers could be calculated for 16 out of the 30 sampling moments (53%) and four outliers were excluded from analysis. The mean diurnal cortisol curve was then calculated for the six participants as a group and for each of the six participants individually, and compared to the curve of the control group. Using the caregivers’ notes, the mean time of sampling was calculated for every sampling moment and rounded up to a whole hour.
The standard deviation was calculated for each sampling moment. For the participants with CDB and an ID the individuals’ mean cortisol levels were used in this calculation.
Results
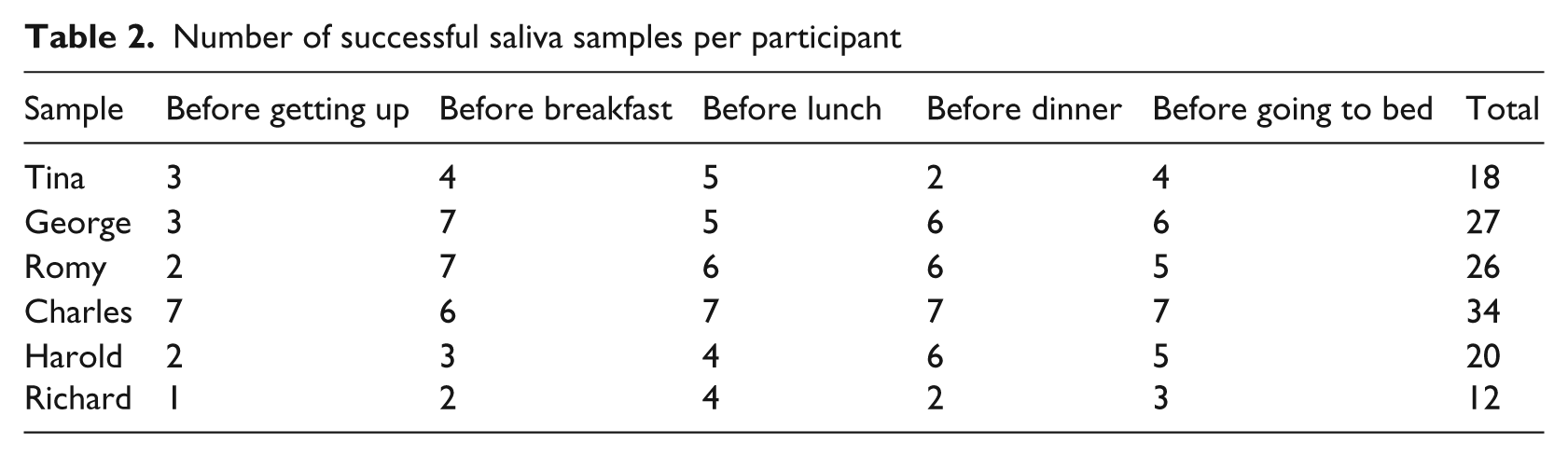
Thirty-five saliva samples were collected from each of the six participants with CDB and an ID. The number of useful saliva samples (> 0.05 ml) per participant varied from 12 to 34 (34% to 97%). Table 2 gives an overview of the number of useful samples for each participant at the five sampling moments (range one to seven). In total, 65 percent of all saliva samples could be analysed. The high percentage of missing samples can be explained in large part by the fact that the sampling process was not sufficiently adapted to the specific target group.
Number of successful saliva samples per participant
The participants’ mean diurnal cortisol curve largely resembles that of the control group, except for 9.00 h (as presented in Figure 1). At this point, a peak can be seen in the participants’ cortisol curve, but not in that of the control group because no sample was taken from them at that time. Inter-individual variation can be seen in the individual participants’ curves (as presented in Figure 2). The curves of George, Charles, Harold and Richard show a peak at the second collection moment; Romy’s cortisol curve lies above the control group’s cortisol curve and Richard’s cortisol curve lies below the control group’s curve. Both these curves appear somewhat flattened.
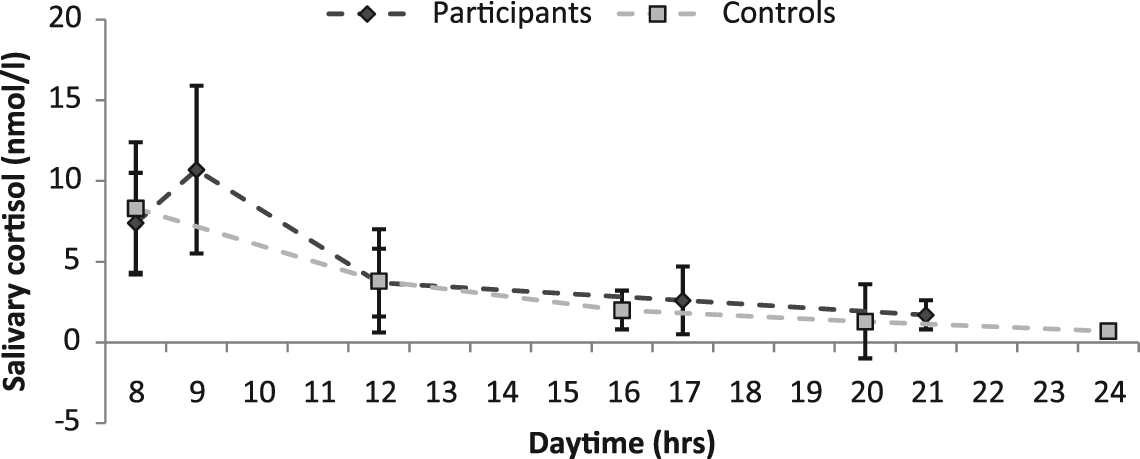
Cortisol curve of the participants compared to the cortisol curve of the controls.
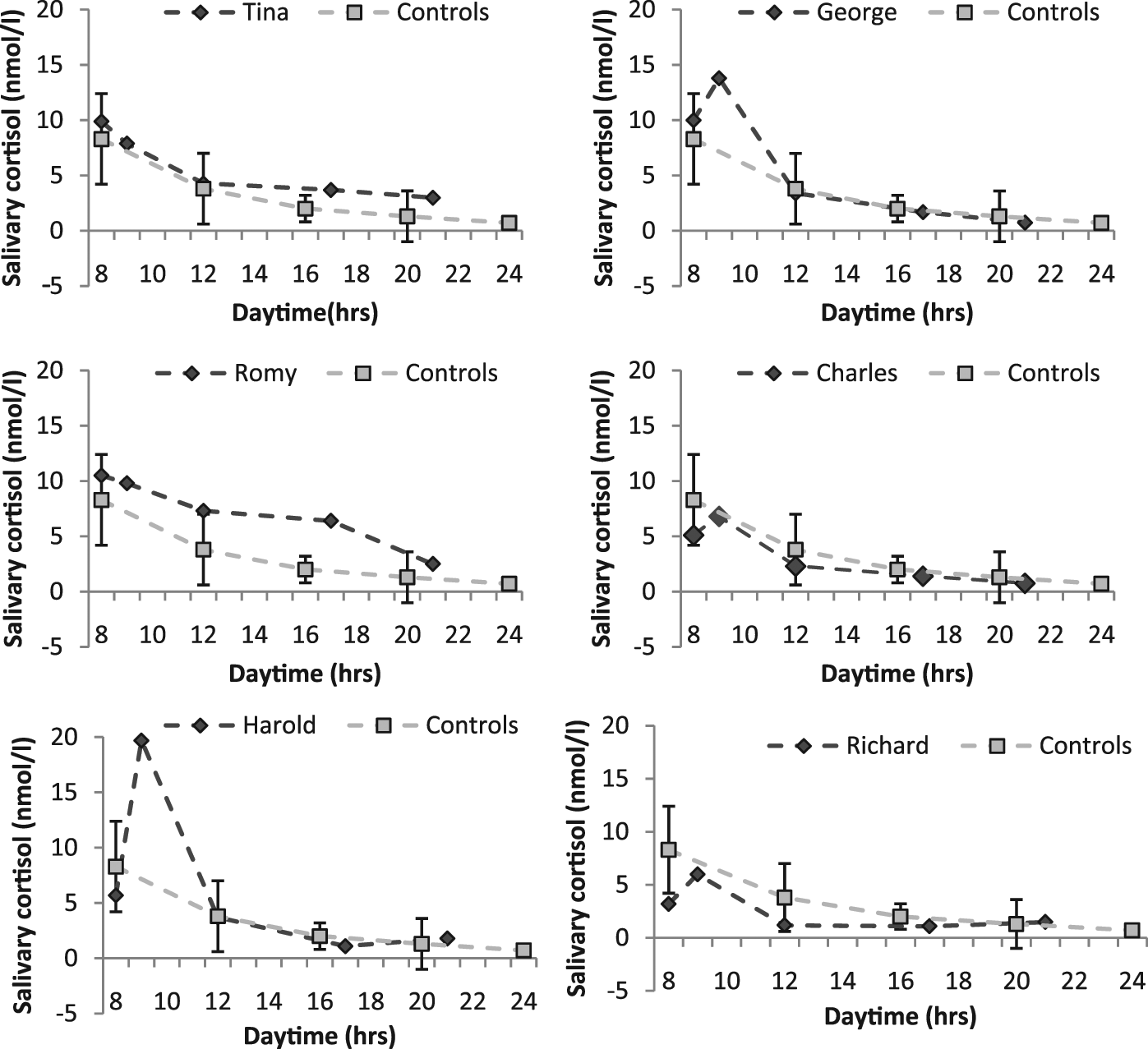
Individual cortisol curves of the six participants compared to the cortisol curve of the controls.
Discussion
This study compared the diurnal cortisol curves of six adults with CDB and an ID with the curve of a control group of 40 typical adults. The participants with CDB and an ID have been, and still are, at great risk for experiencing toxic stress. Our hypothesis was that the cortisol curve of these participants would be lower and flatter than the cortisol curve of the controls. Remarkably, the mean cortisol curve of the participants with CDB and an ID was rather normal, in contradiction with earlier findings showing that stress in early life often leads to changes in the diurnal cortisol curve (Heim et al., 2000; Heim, Newport, Mletzko, Miller, & Nemeroff, 2008). The fact that despite the presence of deprivation and disability, as a group the participants with CDB and an ID have a normal diurnal cortisol curve is nonetheless a very positive finding that speaks to their resilience.
The results show a substantial but normal individual variation among the six participants. Richard’s and Romy’s curves lie respectively below and above the curve of the control group – this is the case for part of their curves even when considering the SD’s of the control group – and appear slightly flattened, in line with the findings of Sack et al. (1992) and Sterkenburg et al. (2008) by persons with a visual disability. All participants have experienced potentially stressful maternal separations and went to live in an institution before the age of 11. However, we do not know the impact of these life events in terms of stressfulness for each participant. According to Lovallo (2005), the stressfulness of a specific event is determined by the individual’s appraisal of the event and by the resources available to control it. An individual can also have a genetic vulnerability to stress (Nicolson, 2007). Differences in the stress that participants experienced, in combination with differences in the developmental course of their disabilities, may very well cause the individual variation in cortisol curves. This may also be influenced by temperamental characteristics (Nelson et al., 2011). The participants also may have developed coping mechanisms to control stress, such as stereotypical behaviour like rocking. Moreover, the quality of past and present caregiving, the access to support from caring persons and individuals’ well-being are factors that probably also influence their diurnal cortisol curve. Unfortunately, the difficulties in communicating with the participants in the present study make it only possible to guess at the underlying reasons for the individual differences found.
The cortisol levels of our participants and the control group were assessed using the exact same method in the same laboratory, so differences in the results are not due to different methods or facilities. However, a limitation of the present study is that the participants’ saliva samples were not collected at exactly the same moments as the control group’s samples. This may well explain the presence of a distinct peak at 9.00 h in the cortisol curve of the group with CDB and an ID and the absence of a peak in the morning in the control group’s curve. Normally, there is a rapid increase in cortisol levels after awakening, the cortisol awakening response (CAR). This physiological response produces a peak in cortisol at around 30 minutes post-awakening (Wilhelm, Born, Kudielka, Schlotz, & Wüst, 2007). At least two samples in the morning are needed to see this peak in the diurnal cortisol curve. The peak is missing in the curve of the control group, because only one sample was taken in the morning. Two saliva samples were taken in the morning from the participants with CDB and an ID: just before getting up and before breakfast. The peak in their mean cortisol curve at 09.00 h may be due to this sample coinciding with their CAR. The peak is missing for Tina and Romy (see Figure 2), possibly because they already had been lying awake in their beds. In such a case, the sampling would be too late to capture the CAR. One participant, Harold, had a high peak at the second collection moment. An explanation, apart from the CAR, may be that he is rather obsessive about food. The second collection moment is prior to breakfast and was therefore possibly a stressful moment for him.
The number of participants in the study was relatively small, a problem inherent to the low incidence and complexity of the target group. Collecting enough saliva from the participants for scientific research was a challenge, as no more than 137 of the 210 intended samples could be collected. This is in line with an earlier observation made by Sterkenburg et al. (2008). The following recommendations can be made for collecting saliva from participants with an ID and additional disabilities, both in future studies and for medical reasons: a) give extensive instructions about the saliva sampling to caregivers (e.g. an instruction movie, a team meeting); b) take enough time for the collection; c) communicate with the participants in a way that is adapted to their ability to understand what is going to happen so that they will not be frightened (e.g. let them touch a cotton roll before collecting the saliva); and d) make adjustments to the sampling procedure (e.g. collect in two phases with a pause in between).
Despite the limitations, the present study offers a good base for future studies to elaborate on. The results give an interesting insight into the stress physiology of adults with CDB and an ID. It remains partly unclear how exposure to many risk factors for stress results in a normal cortisol curve. Factors like genetic vulnerability, coping mechanisms and temperament seem to play a role. It is also possible that what seems stressful for most people (e.g. a lack of sensory information) might not be experienced as stressful for someone born without vision and hearing. To a person who is born deafblind, a world without good information from vision and hearing is normal instead of deviant. This information is not perceived as lacking because it is not part of their reality at all. One might also adapt to living in unpredictable, uncontrollable and often novel situations from birth. The fact that the participants are all adults and have had time to adjust to their circumstances may also partially explain the positive results. In most of the studies that found deviant cortisol curves, the participants were children. The role of the ID on the results needs to be further clarified.
The results of this study are positive. They show that the presence of unfavourable circumstances do not have to lead to deviances in the cortisol curve. This speaks for the resilience of the participants in this study, but also raises questions about the underlying reasons for the individual differences. Although as a group the participants with CDB and an ID had a normal cortisol curve, two of them did have deviancies in the cortisol curve. Deviancies in the individual cortisol curves of the participants with CDB and an ID may be caused by a combination of factors. Some of these factors cannot be influenced but other factors, aimed at increasing their current well-being, can be influenced by, for example, decreasing the number of unpredictable and uncontrollable events in daily life, or training caregivers to be sensitive and responsive partners during daily interactions. This underscores the need of a specific approach for the target group.
The present study has shown that life events alone are not reliable predictors of cortisol levels. Future research is needed to discover whether factors such as adaptation to life events are better predictors.
Footnotes
Acknowledgements
We would like to acknowledge the contributions of Roel Menke and the staff and clients of Royal Visio, De Brink, Vries, The Netherlands.
Funding
This study was funded by Royal Visio, and by the University of Groningen, Department of Special Needs Education and Youth Care. The Radboud University Nijmegen Medical Centre, Department of Laboratory Medicine, supported this study by analysing the saliva samples.
Declaration of Conflicting Interests
The authors declare that they do not have any conflict of interest.