
Abstract
A retrospective study was carried out to evaluate the paediatric visual impaired population attending the Low Vision Clinic at Sheffield Teaching Hospitals NHS Foundation Trust, over a period of 14 years. Data were collected and analysed for children less than 17 years for prevalence, demographics, registration status, aetiologies, and types of low vision aids issued. The total number of children identified was 204. Of these, 19 percent of the children were registered blind, 45 percent were registered partially sighted, and 36 percent were not registered. The four diagnostic groups were genetic (29%), prenatal (36%), perinatal (23%), and childhood (12%). Describing local characteristics of paediatric visual impairment is a useful measure of current low vision service provision. This information can further inform educational, social, and health needs for the visually impaired children to ensure adequate service provision.
Introduction
Vision impairment (VI) in childhood can affect a child’s cognitive, physical, emotional, and neurological development and can adversely impact the child’s family and community (Batshaw & Perret, 1992; Day, 1997; Kaminer & McMahon, 1995; Sonksen, Petrie, & Drew, 1991). Knowledge of local demographic data of children with vision impairment is critical in planning and delivering services to meet their needs.
The prevalence and causes of paediatric VI vary depending on health-care provision, especially with regard to pregnancy, neonatal care, and socioeconomic factors. Childhood blindness is more prevalent in large parts of Asia, Africa, and South America compared to Western Europe (Foster and Johnson, 1990). There have been a number of estimates of VI in geographically defined populations in the United Kingdom (Alagaratnam, Sharma, Lim, & Fleck, 2002; Goggin & O’Keefe, 1991; Rogers, 1996). These studies have used a range of methods, sources, definitions, and outcome measures, limiting the scope to generate a summary estimate. However, the findings are broadly similar to the national surveys of VI, with clinical prevalence estimates around 10–20 per 10,000 children (Bodeau-Livinec et al., 2007; Rahi & Cable, 2003). More recently, Cumberland, Pathai, and Rahi (2010) reported a slightly higher prevalence of 2.4 per 1000 children, but this figure was obtained from parental reports rather than clinical records. Because of the variation in definitions, service provisions, and data collection, great caution is required in interpretation of any single estimate of the prevalence of VI or blindness among children in the United Kingdom.
In the United Kingdom, patients with VI may register as severely sight impaired (SSI) or blind if visual acuity is less than 3/60 with a full visual field, visual acuity is between 3/60 and 6/60 with a severe reduction of the visual field, or visual acuity is 6/60 or more with a very reduced visual field. To be registered as sight impaired (SI) or partially sighted, visual acuity is from 3/60 to 6/60 with a full visual field, visual acuity is up to 6/24 with a moderate reduction of visual field, or visual acuity is up to 6/18 with a large part of the visual field missing. Table 1 summarises the criteria for registration based on visual acuity and visual fields.
Registration of visual impairment based on visual acuity and visual fields

SSI: severely sight impaired; SI: sight impaired.
The UK Department of Health recommends that infants and young children who have congenital ocular abnormalities leading to visual defects should be certified as SI unless they are obviously SSI. Children aged 4 and over should be certified as SSI or SI according to their binocular corrected vision. No other UK specific guidelines exist for children.
There is limited data on the incidence of childhood VI in any region of the world, including the United Kingdom (Foster & Gilbert, 1992; Rahi & Dezateux, 1998; Thylefors, Negrel, Pararajasegaram, & Dadzie, 1995). The most serious ophthalmic disorders in children that result in VI are present or become manifest in early childhood. In England and Wales in 1990–1991, the combined incidence of registration of SI and SSI was 8 per 100,000 children aged 1 to 15 years (Evans, 1995).
Gilbert et al. (1993) recommend two ways of classifying causes for childhood VI: the anatomical classification (cornea, lens, retina, optic nerve, and other) and the aetiological classification (genetic, prenatal, perinatal, and childhood). This study employed the aetiological classification.
The Sheffield Low Vision Clinic was established in its current form in 1996. The clinic accepts patients with VI of any age from local and surrounding areas provided they are registered with a consultant in the hospital’s eye clinic. Referrals are accepted from ophthalmologists and orthoptists. All children registered as VI are referred to the Low Vision Clinic. Children who do not meet registration criteria are also referred; there is no minimum vision requirement to access the Low Vision Clinic. These children also require support, advice, and issue of low vision aids from the Low Vision Clinic. Patients are assessed by appropriately trained low vision therapists who are either orthoptists or ophthalmic-trained staff nurses. A functional visual assessment is performed, including distance and near visual acuity, contrast sensitivity function, visual field assessment to confrontation, and reading ability. Advice is also given to both parents and children on appropriate use of task lighting and glare avoidance. Strategies to improve reading fluency, such as eccentric viewing, use of typoscopes, and optimum positioning of visual targets, are also provided. Low vision aids are issued based on visual demands, educational requirements, preference, ease of use, and dexterity at the time of assessment rather than by prescription. It is generally not possible to predict exactly from levels of visual acuity what type and power of low vision aids will be required when issuing aids for children. Aids issued to all children follow appropriate training in their use.
The aim of this service evaluation study was to provide detailed local paediatric data regarding causes of VI and the provision of low vision aids.
Methods
A retrospective study was conducted of all children between 1 and 16 years of age (inclusive of 16-year-olds) seen in the Low Vision Clinic at the Royal Hallamshire Hospital in Sheffield between January 1996 and December 2009. The study was approved and registered as service evaluation with the local clinical effectiveness unit.
A dedicated low vision database was introduced in 2000 for all patients attending the clinic. Data were added to the database manually from the notes for patients seen since 1996. Data are entered onto the database at the first visit to include patient’s full name, date of birth, consultant, date of referral, date of low vision appointment, diagnosis, registration status, low vision aids issued, and appointment outcome. On subsequent visits, any change to registration status, diagnosis, and types of aids issued are updated.
Macros were employed to display the data from the low vision database in Excel format as an entry for each patient identified less than 17 years of age. Data on the age distribution, the registration status, the aetiologies of visual loss, and the types of low vision aids issued were gathered from the departmental low vision database. Gender was identified from the patient information system as it was not recorded on the low vision database.
Often more than one diagnosis was recorded and more than one aid had been issued. If more than one diagnosis was recorded, the principle diagnosis was used for classification purposes; for example, in a child with aniridia and nystagmus, both were recorded but aniridia was considered the primary diagnosis. The aetiological classification was used to categorise children into four main diagnostic groups: genetic, prenatal, perinatal, and childhood. All the different types of low vision aids issued for each patient during the 14-year period from 1996 to 2009 were included in the results and were classified into three broad groups. Telescopic aids include monoculars and binoculars. Stand magnifiers include flat-field magnifiers and illuminated stand magnifiers. The third category was hand magnifiers.
Results
A total of 204 children were identified. Table 2 summarises the paediatric demographic data to include age and gender distribution as well as the registration status of VI. The age distribution at the time of the first visit was 6 percent, under 4 years; 43 percent, 4–7 years; 31 percent, 8–11 years; and 20 percent, 12–16 years of age. More males (60%) than females (40%) were seen. In all, 45 percent were registered as SI, followed by those not registered (36%) with the remaining being those on the SSI register (19%).
Paediatric demographic data for age, gender, and registration status of VI

SSI: severely sight impaired; SI: sight impaired; NR: not registered.
Table 3 gives the primary causes of paediatric VI. Most children were diagnosed with a genetic (35%) or prenatal (34%) condition, with perinatal (21%) and childhood (5%) aetiologies being less common. Retinal disorders were further classified as rod/cone dystrophy, retinal dystrophy, and cone dystrophy following electrodiagnostic testing. The four major causes of VI, in order of frequency, were genetic retinal disorders such as retinal and cone dystrophy, albinism, optic atrophy, and congenital cataract. Nystagmus was a secondary diagnosis in 51 percent of all children but only 7 percent (14) as a primary diagnosis.
Classification of aetiologies of childhood VI
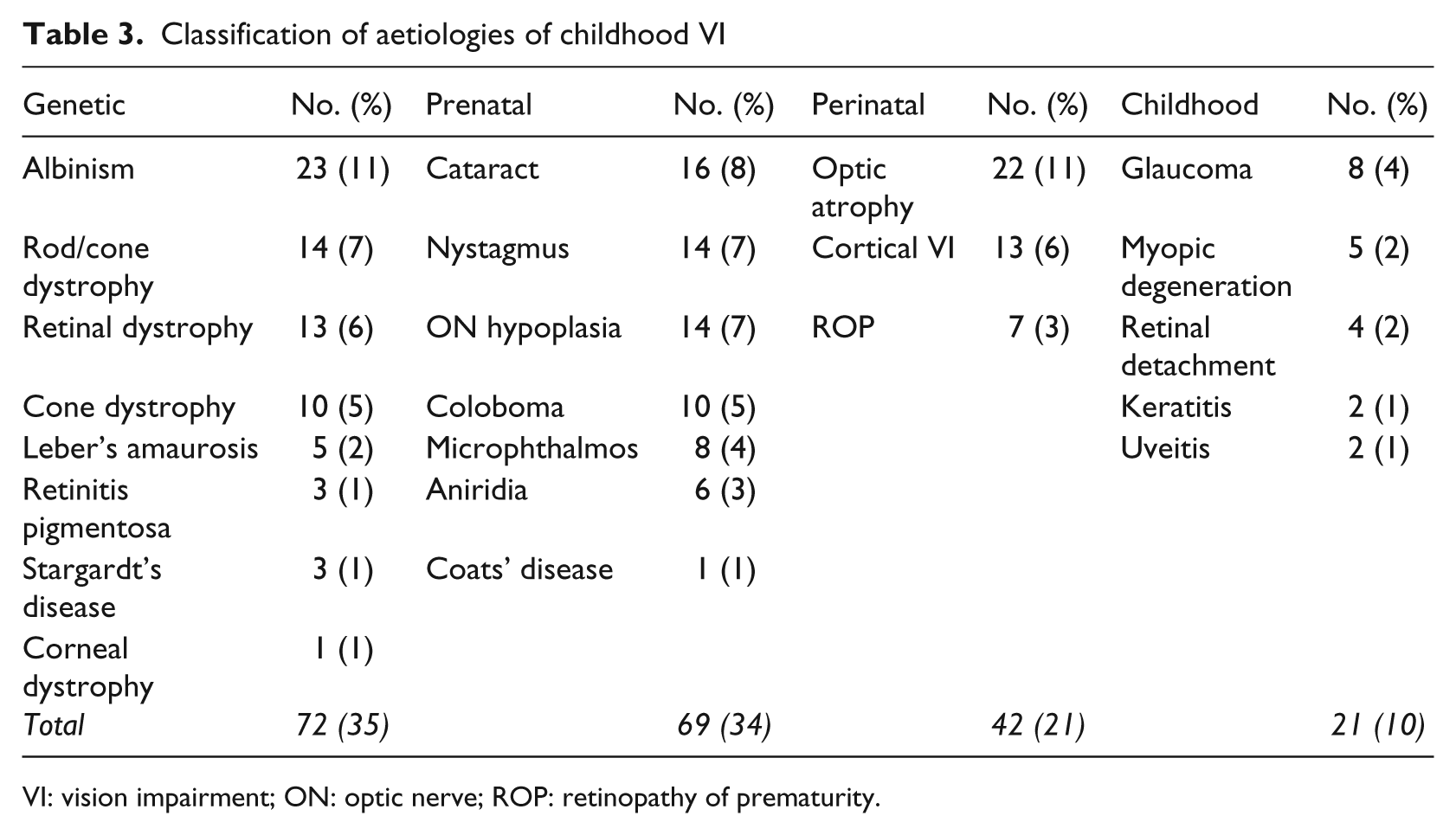
VI: vision impairment; ON: optic nerve; ROP: retinopathy of prematurity.
Following full assessment of visual function, visual needs, and personal circumstances, low vision aids are issued on a loan basis. Some children were issued with more than one aid, while no aids were issued for others. Most children were issued with both a stand magnifier (83%) and a telescopic aid (83%) followed by a hand magnifier (40%). Most of the non-registered children, 64 (86%), were issued with a low vision aid. Only 9 percent of children were not issued with a low vision aid.
Discussion
In this study, we included all children attending the Low Vision Clinic, irrespective of their registration status. A total of 204 children were identified. A large percentage of the children (36%) in this cohort were not registered as visually impaired. Other studies have mainly concentrated on demographic data of children with SSI.
In Sheffield, children attending the eye clinic are assessed by orthoptists and ophthalmologists, and are referred to the Sheffield VI service to access education and support services depending on the current visual status and individual difficulties rather than eligibility criteria for registration. This may be a factor in the number of children not registered but requiring VI input in this study. Findings from the British Childhood Vision Impairment Study (Cumberland, Pathai, & Rahi, 2010) also support evidence of under-registration where out of 439 children eligible for SSI registration, only 61.4 percent were certified a year later. Therefore, although registration data have traditionally been an important source of information, registration rates provide only general, minimum estimates of the incidence of severe VI and blindness. Additionally, registration is not compulsory in the United Kingdom.
Most of the children who were not registered as SI (86%) were issued with a low vision aid. Children with visual impairment who do not fulfil SI registration criteria still frequently require magnification to enhance print size for near tasks and enable the detail in pictures, graphs, and charts to be identified. Similarly, the use of telescopic devices facilitates distance object recognition important for both educational purposes and leisure.
It is not possible to identify why a low vision aid was not issued in some children (9%). However, children who do not require magnifying devices still need information and advice to manage their VI. Guidance on lighting, contrast, glare avoidance, optimum positioning of targets, and use of non-optical devices, such as raised desktops, typoscopes, and line guides, is also provided at the Low Vision Clinic to optimise visual performance to provide a functional assessment.
Children referred to the Sheffield Low Vision Clinic have a vast array of diagnoses, ranging from refractive pathology to rare genetic syndromes. Our results correlate well with previous European studies of similar socioeconomic status (Khan, O’Keefe, Kenny, & Nolan, 2007).
The genetic (35%) and prenatal (34%) diagnostic groups were the most common. In the genetic group, the most common aetiology resulting in VI was retinal disorders (18%) followed by albinism (11%). Cataract (8%) was the most frequent aetiology in the prenatal group followed by primary nystagmus (7%) and optic nerve hypoplasia (7%). Optic atrophy (11%) was the most common cause of impairment in the perinatal group. Our results show a small number of children (6%) with cortical visual impairment (CVI) compared to other studies (Alagaratnam et al., 2002). These results may be due to a significant number of our children not registered compared to only children on the SI/SSI register by Alagaratnam et al. (2002).
In the final childhood group, glaucoma (4%) was most common. A similar study conducted in Liverpool by Thylefors et al. (1995) reported the incidence of paediatric VI and showed a similar spread of causes. In 69 children with uncomplicated VI, genetically determined disease accounted for over half the cases, and albinism (22%), hereditary retinopathy (13%), and nystagmus (16%) were the most common aetiologies.
A previous comparative study by Kocur and Resnicoff (2002) reviewed demographic published data from several European studies, and their findings conclude that within Europe, causes of childhood visual loss vary depending on health-care provision. In highly industrialised countries of Europe such as the United Kingdom, the leading causes of childhood visual loss are lesions of the central nervous system (CVI), and congenital and retinal anomalies. In the middle income European countries, congenital cataract, glaucoma, and retinopathy of prematurity (ROP) are still high. Among Nordic children, cerebral amblyopia (23%), which is attributed to a lesion affecting the retrochiasmal part of the visual system, and secondary optic atrophy (19%) scored the highest (Rosenberg, Flage, & Hansen, 1996).
Improved medical care allows many critically ill children to survive often with damage to the visual system. These children are then registered as SI altering the demographics as described by other countries. If cerebral amblyopia was excluded from the incidence calculations, the Nordic figures would match UK demographic findings.
Our results note a male preponderance with a male to female ratio of 1.5:1. This compares favourably to previous UK-, European-, and North American–based studies (Evans, 1995; Rosenberg et al., 1996; Thylefors et al., 1995).
Twenty-six children were referred to the Sheffield Low Vision Clinic under the age of 5, the pre-school group. Three children were aged 2 and below, and they had an initial consultation with a low vision therapist for the service to be introduced to the parents. No aids were issued, but the therapist provided a detailed explanation of the diagnosis, implications on visual development, and long-term prognosis. Information and advice is also provided to all parents on suitable types of lighting, effect of glare, and impact of contrast on activities of daily living to facilitate optimal visual functioning. Annual appointments are offered to monitor visual status as well as the individual visual needs of the child in preparation for full-time education. Regular ophthalmic follow-up in the outpatient clinics is also arranged. Children in this pre-school group aged 2, 3, and 4 were generally issued with a low vision aid in order to introduce and familiarise the child with the concept of magnification. A flat-field dome was the most common aid issued. Issuing low vision aids at an early age through formal play encourages the child and parent to familiarise themselves with the concept of magnification. A developmental level of 2 years of age has been shown to be adequate for using a stand magnifier (Ritchie, Sonksen, & Gould, 1989). Over a period of time, they are able to develop these skills with the aim to gradually introduce more complex aids as the visual demand changes. It has previously been suggested that children who first receive low vision support at school, access this too late and that pre-school children of 3 years and older may benefit from simple magnification that could also impact on other areas of development, not just visual (Leat, 2002; Rudduck, Corcoran, & Davies, 2004). It has been argued by Gould and Sonksen (1991) that children should have access to support services before reaching school age, as the general development of the child can be greatly influenced in the pre-school years of life. Early access to low vision services for these children can have a large impact on their quality of life, education, and future employment prospects (Keil, Franklin, Crofts, Clery, & Cole-Hamilton, 2001; Pilling, Thompson, & Gottlob, 2005).
School-aged children formed the largest part of this cohort. Full-time education is compulsory for all children aged between 5 and 16 (inclusive) in the United Kingdom. Pupils progress from primary to secondary levels at age 11. There were two peaks in the age at referral to the Low Vision Clinic, the first between 5 and 7 years old and the second between 10 and 11 years old. This would seem to correlate with starting primary school education and progressing to secondary school education, respectively. This is the time in their education when their visual demands change significantly such as decreasing print size and quality as well as reduced contrast of printed materials. In secondary school particularly, the demands on the child in terms of examinations, speed and accuracy of reading, and written work, and also a change in environment result in an alteration in the requirement of magnification types resulting in additional training in the optimum use of their aids for both education and to promote independence.
The Sheffield Low Vision service has well-established links with the educational VI service. Both services work closely together to promote low vision aid competency, and this liaison continues to support the child throughout his or her educational years. Following parental consent to share information, annual reports are shared between the two services. Local children who attend special schools with severe visual and sensory impairment are not referred to the Low Vision Clinic but receive specialist VI input at school.
A flat-field dome was the most common magnifier issued followed by a telescopic aid, either monocular or binocular. Relatively fewer hand-held devices were issued possibly due to the increased difficulty in maintaining focus with hand-held devices for prolonged periods of time. It is essential to ensure that any training given is comprehensive and adaptable for individuals to promote proficiency and efficient use of time and resources.
Describing the local characteristics of paediatric VI in a large Low Vision Clinic is a useful evaluation of current service provision. The results provide prevalence data and information on the provision of low vision aids. The findings from this study provide evidence that a large number of children who are not registered as SI benefit from access to low vision services.
Footnotes
Declaration of conflicting interests
The authors declare that they do not have any conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.