
Abstract
Objectives:
The loss of both hearing and vision (dual sensory loss) affects communication and potentially challenges the ability to maintain healthy social relations. The aim of this study was to examine the association between severity of sensory loss and relational strain among older adults with acquired dual sensory loss.
Method:
Data were collected through a national cross-sectional questionnaire survey and an administrative database. A total of 302 individuals with functional dual sensory loss ⩾50 years of age participated (66% response). Relational strain was measured as the perceived experience of excessive demands, worries, and conflicts with children, other relatives, or the personal support worker. Data were analyzed by multivariate logistic regression.
Results:
No associations between severity of dual sensory loss and excessive demands from or worries for children, other relatives, or personal support workers were found. Participants with total blindness and profound deafness had significantly higher odds for experiencing conflicts with children (odds ratio [OR] = 3.09, 95% confidence interval [CI] = [1.02, 9.38]) and the personal support worker (OR = 4.18, 95% CI = [1.23, 4.28]) compared to participants with residuals of both senses.
Discussion:
Individuals with total blindness and profound deafness might require special attention in rehabilitation to support them in maintaining healthy social relations.
Introduction
Relational strain
Social relations are important for both physical and mental well-being; however, research has shown that social relations are not unequivocally positive or negative (Antonucci, Ajrouch, & Birditt, 2014). Most studies on social relations focus on the beneficial aspects such as instrumental and emotional support provided by positive social relations. Less focus has been given to the constricting effects of positive aspects of social relations and the enhancing and constricting effects of negative aspects of social relations, also called relational strain. Conflicts, excessive demands, and worries have been highlighted as some of the main characteristics of relational strain (Antonucci et al., 2014; Lund, Nielsen, et al., 2014). In a Danish population-based study, it was found that approximately 20%–30% of 60-year-olds and approximately 15%–20% of 70-year-olds often or sometimes experienced conflicts with relatives (Due, Holstein, Lund, Modvig, & Avlund, 1999). Another population-based study in Denmark found that 6% of the sample always or often experienced conflicts with their children and 2% with other relatives and another 10% often or always experienced worries or demands from their children and 6% from other relatives (Lund, Christensen, Nilsson, Kriegbaum, & Rod, 2014). Several health-related factors are associated with relational strain, both as an exposure and outcome. For example, low self-rated health is a determinant of poor social relations (Lund, Avlund, Modvig, Due, & Holstein, 2004), and misconceptions, social exclusion, and stigma have been identified as some of the social consequences of living with a rare disorder (Lippe, von der Diesen, & Feragen, 2017).
However, other studies have found protective effects of negative relations on, for instance, survival (Antonucci et al., 2014). These protective effects could be due to demands posed to change inappropriate or unhealthy behavior (Antonucci et al., 2014).
Dual sensory loss
Dual sensory loss (DSL) is a condition where hearing and vision are concurrently impaired to a degree influencing access to information, communication, and mobility (Ask Larsen & Damen, 2014). The majority of people with DSL have age-related acquired DSL (Wittich, Watanabe, & Gagné, 2012), and it is estimated that approximately 20% of people aged 80 years or older meet the criteria for DSL (Dammeyer, 2013; Harada et al., 2008; Schneider et al., 2012). With aging populations in many western countries, the prevalence is expected to increase despite advances in treatment (Rein et al., 2009; Wallhagen, Strawbridge, Cohen, & Kaplan, 1997). People with DSL are dependent on social relations for functional independence and psychological and social well-being (Heine, Erber, Osborn, & Browning, 2002; Rudman et al., 2016; Saunders & Echt, 2007). Previous research on social relations among people with DSL has primarily focused on beneficial aspects such as emotional and instrumental support as well as social participation (Heine & Browning, 2014; Saunders & Echt, 2007; Schneider et al., 2011), all of which have been found to influence the effect of DSL on depression (Capella-McDonnall, 2005, 2009; Chou, 2008). However, previous studies have shown both benefits and drawbacks when it comes to social relations among people with DSL. In a qualitative study with 28 semi-structured interviews, it was found that individuals with DSL were highly dependent on close social relations in order to maintain independence, active social participation, and mobility (Hersh, 2013). However, at the onset of DSL, individuals developing DSL also reported feelings of frustration, confusion, and depression, and in both formal and informal relations they have often felt overprotected (Hersh, 2013). Perceived overprotection has also been found to increase over time among visually impaired individuals (Cimarolli, Boerner, Reinhardt, & Horowitz, 2013). Finally, it has been reported that individuals with DSL often experience communication breakdowns and are more aware of communication problems than their communication partners (Heine et al., 2002). In summary, persons with DSL risk experiencing feelings of frustration, confusion, and depression, as well as overprotection and communication breakdowns. In combination with dependency on social relations for independence and well-being, people with DSL might be at risk for experiencing a high level of relational strain in their close social relations.
Objectives
Social relations are of importance. However, little is known about how vision and hearing loss affect perceived relational strain among older adults with DSL. To prevent social withdrawal and promote healthy social relations and active participation for older adults with DSL, it is important to understand the magnitude of the perceived relational strain and to identify in which type of relations the strain appears. The objective of the following study was to investigate the frequency and types of strain and the association between severity of hearing and vision losses and the experience of excessive demands from, worries for, and conflicts with children, other relatives, and the personal support worker among older adults with acquired DSL.
The more severe sensory losses a person has, the less visual and auditory information is received to facilitate independence and communication with others. This might create a higher level of relational strain in the close social relations of those with severe sensory losses compared to those with milder sensory losses. Therefore, we hypothesize that concurrent total blindness and profound deafness will be associated with higher odds of experiencing excessive demands from, worries for, and conflicts with children, other relatives, and personal support workers compared to individuals with residual vision and hearing.
Methods
Study sample
The study was approved by the internal ethics committee at Department of Psychology, University of Copenhagen and the Danish Data Protection Agency (No. 2015/02). The objectives were investigated in a cross-sectional study in a closed study population that included all individuals aged ⩾50 years by March 2015 assessed with DSL by the national provider of rehabilitative services prior to May 2015 (N = 513). Around the age of 50 years is a life transition period, where menopause occur and children start leaving the house. People 50 years of age or older were included because their social network, social support, and relational strain are different compared to younger age groups (Due et al., 1999). Also, research has shown that there are few people with acquired DSL among younger age groups and that most of them have Usher syndrome (Dammeyer, 2013). For the above reasons and to include as many people with acquired DSL as possible, all individuals aged ⩾50 years were selected. The national provider is the only institution assessing for DSL in Denmark and uses the Nordic functional definition of DSL (Ask Larsen & Damen, 2014) as the criterion for including people in the service. Everyone, including professionals, relatives, or the individual experiencing sensory losses, can contact the national provider for an assessment for DSL. After positive assessment with DSL, a deafblind consultant will be assigned to have continuous contact with the individual with DSL and to provide special deafblind rehabilitative services depending on the need. The assessment and services are free of charge. In addition, each individual with DSL can have personal assistance from a personal support worker, referred to as a contact person, to compensate for the sensory losses. The contact person can be a friend or relative, but can also be a stranger. The contact person is employed by the local municipality and is hired for a certain amount of hours per week depending on the individual need of the individual with DSL.
Prior to data collection, 30 individuals were excluded due to severe health conditions that meant that they were unable to complete the survey even with assistance. Thus, 483 individuals with DSL were invited to participate. During data collection, 14 individuals died, another 13 individuals were excluded due to severe health conditions, 90 individuals denied to participate, and 64 individuals did not respond to the questionnaire. Data collection took place in 2015 and the aim was to include as large a sample as possible. The final sample included 302 individuals (66% excluding those who were excluded or died), of whom one participant had developed DSL below the age of 1. The remaining participants had all developed DSL after the age of 3. The representivity of the sample was investigated using χ2 and t-tests to analyze differences between respondents (n = 302) and non-respondents, deniers, dead, and excluded individuals (n = 211) by age, gender, residual vision and hearing, and allocation of a contact person. There were significantly fewer individuals with no residual vision or hearing in the sample compared to the non-respondents, deniers, dead, and excluded individuals (χ2 = 14.85, degrees of freedom [df] = 4, p = .005) (Figure 1). Furthermore, the sample was significantly younger and there were significantly more men and individuals who were allocated a contact person.

Distribution of residual vision and hearing in the sample (n = 302) and non-respondents, deniers, dead, and excluded individuals (n = 211).
Procedure and data sources
The objective was investigated using data from a cross-sectional questionnaire survey and an administrative database. An information letter was sent prior to the questionnaire survey. Non-responders were sent a second copy of the questionnaire before being contacted by a researcher via phone. The individuals with DSL could participate by completing the paper questionnaire, phone interview with a researcher, or an in-person interview in a location of their choice. They were furthermore encouraged to ask for assistance to complete the questionnaire if necessary. Deafblind consultants and contact persons were informed of the study in advance and received a guide for assisting with completing the questionnaires, should they be asked by the individuals with DSL for assistance.
In addition to the questionnaire survey, information was retrieved from an annually updated administrative database from the national provider. The information in the database was reported by the assigned deafblind consultants.
Definition of variables
Information on severity of vision and hearing loss was retrieved from the administrative database. This is based on the deafblind consultants’ evaluation of whether the individual with DSL had any residual vision and hearing, respectively. The information was recorded as yes, no, or do not know. For this study, residual vision and hearing was categorized as having both residual vision and hearing, having residual vision but no residual hearing, having residual hearing but no residual vision, and having no residual vision or hearing. Those registered with “do not know” were treated as missing (2%).
Previous research has shown that older adults with sensory loss have a high frequency of contact with close kin, but fewer or weaker contacts with more distant relations such as friends and other family members (Lind et al., 2003; Wahl et al., 2013). Furthermore, 80% of the sample reported to be living alone. Thus, for this study, we decided to focus on the relations with children, other relatives, and contact persons.
Frequency of worries, excessive demands, and conflicts were measured by the Copenhagen Social Relations Questionnaire (Lund, Nielsen, et al., 2014) in the questionnaire survey. The content and face validity of the Copenhagen Social Relations Questionnaire has been found satisfactory in a qualitative study including 31 participants. The test–retest reliability has been assessed by kappa values and found to be substantial to almost perfect for 41% of the items and showed moderate agreement for the remaining items except one (Lund, Nielsen, et al., 2014). Respondents were asked to answer every question for each type of relation (children, other relatives, and contact person). There were six response categories for each question (always, often, sometimes, seldom, never, and have none), for analyses the responses were dichotomized into “Always, Often, Sometimes, or Seldom” and “Never.” Participants who responded “have none” to a type of relation were excluded from the analyses of that relation. Furthermore, those who were not registered as having a contact person in the database were excluded from analyses of the relationship with contact persons. Thus, the overall sample sizes for analyses of excessive demands, worries, and conflicts were 241, 283, and 185 in relation to children, other relatives, and contact persons, respectively.
Information on age, gender, and assignment of contact person (yes/no) was obtained from the administrative database. Information on children (yes/no) and highest attained educational level (“Basic education to Primary and lower secondary school,” “Medium education to upper secondary school and vocational training,” and “higher education”) was reported in the survey.
Information on assistance received completing the survey was measured by the following questions included in the survey: Assistance from relatives (yes/no) and Assistance from contact person (yes/no).
Statistical analyses
Frequency of demands, worries, and conflicts were analyzed separately for relations with children, other relatives, and contact persons.
Multivariate logistic regression analyses were performed separately for relational strain with children, other relatives, and contact persons, respectively, to analyze the hypothesis that not having residual vision and hearing are associated with experiencing excessive demands, worries, and conflicts. All the regression models were adjusted for age, gender, highest attained educational level, and frequency of face-to-face contacts with the specific type of relation. A sensitivity analysis was performed to investigate whether social desirability bias was present due to the individuals with DSL having received assistance completing the questionnaire. Associations between demands from, worries for, and conflicts with children and relatives and assistance from a family member as well as demands from, worries for, and conflicts with contact persons and assistance from a contact person were tested using χ2 tests.
Associations between excessive demands, worries, and conflicts for the three types of relations (children, other relatives, and contact persons) were analyzed using Spearman correlations.
Missing information was handled with list-wise deletion as the missing information was not missing at random. All tests were two sided and the level of statistical significance was 5%. All analyses were performed in SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Sample characteristics
The mean and median ages of the sample (n = 302) were 81 and 85 years, respectively, and 70% were female. The mean and median ages of the onset of DSL were 64 (standard deviation [SD] = 21.56) and 70 years, respectively. Regarding highest attained educational level, 32% of the sample had basic general education and 39% had vocational training. Most participants had both residual vision and hearing (62%), 24% had only residual hearing, 5% had only residual vision, and 9% had neither residual vision nor hearing. Participants were encouraged to get assistance with completing the questionnaire if necessary, 39% received help from a contact person and 35% received help from a family member. The proportion of participants experiencing excessive demands, worries, or conflicts was lower for the age groups above 80 years of age across all types of relations (Figure 2). The highest demands were experienced in relation to children for most age groups. There was a lower proportion of participants experiencing worries for contact persons across all age groups (24%–32%) compared to children (37%–63%) and other relatives (31%–61%). There was a clear pattern indicating a tendency for fewer conflicts in the older age groups (7%–13% for ⩾80 years) compared to the younger age groups across all types of relations (18%–53% for <70 years). Conflicts with contact persons were lower than for children and other relatives in all age groups except for the ⩾90 years of age group (Figure 2).
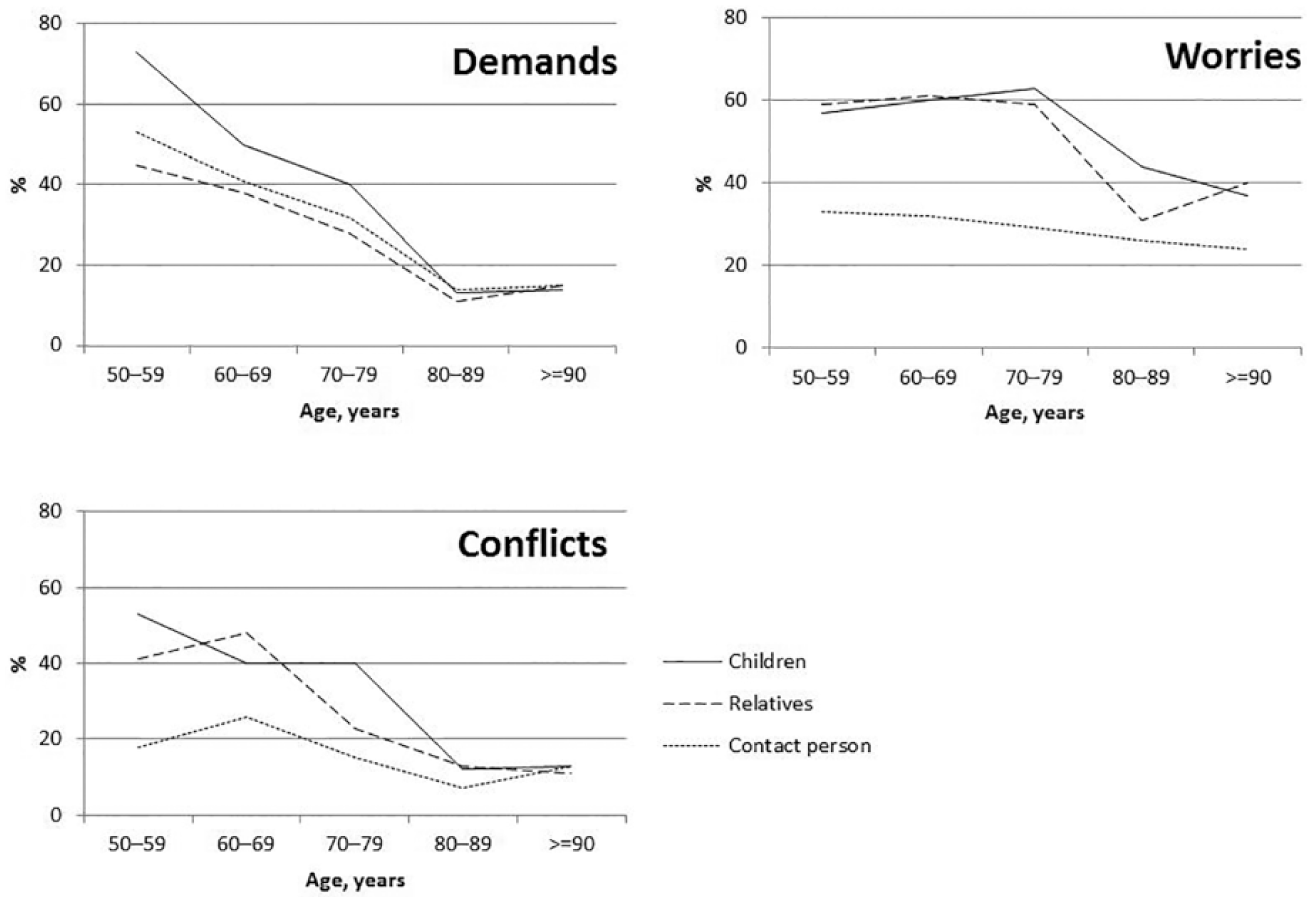
Proportions experiencing excessive demands, worries, and conflicts with children (N = 241), other relatives (N = 283), and contact person (N = 185) in age groups.
Excessive demands
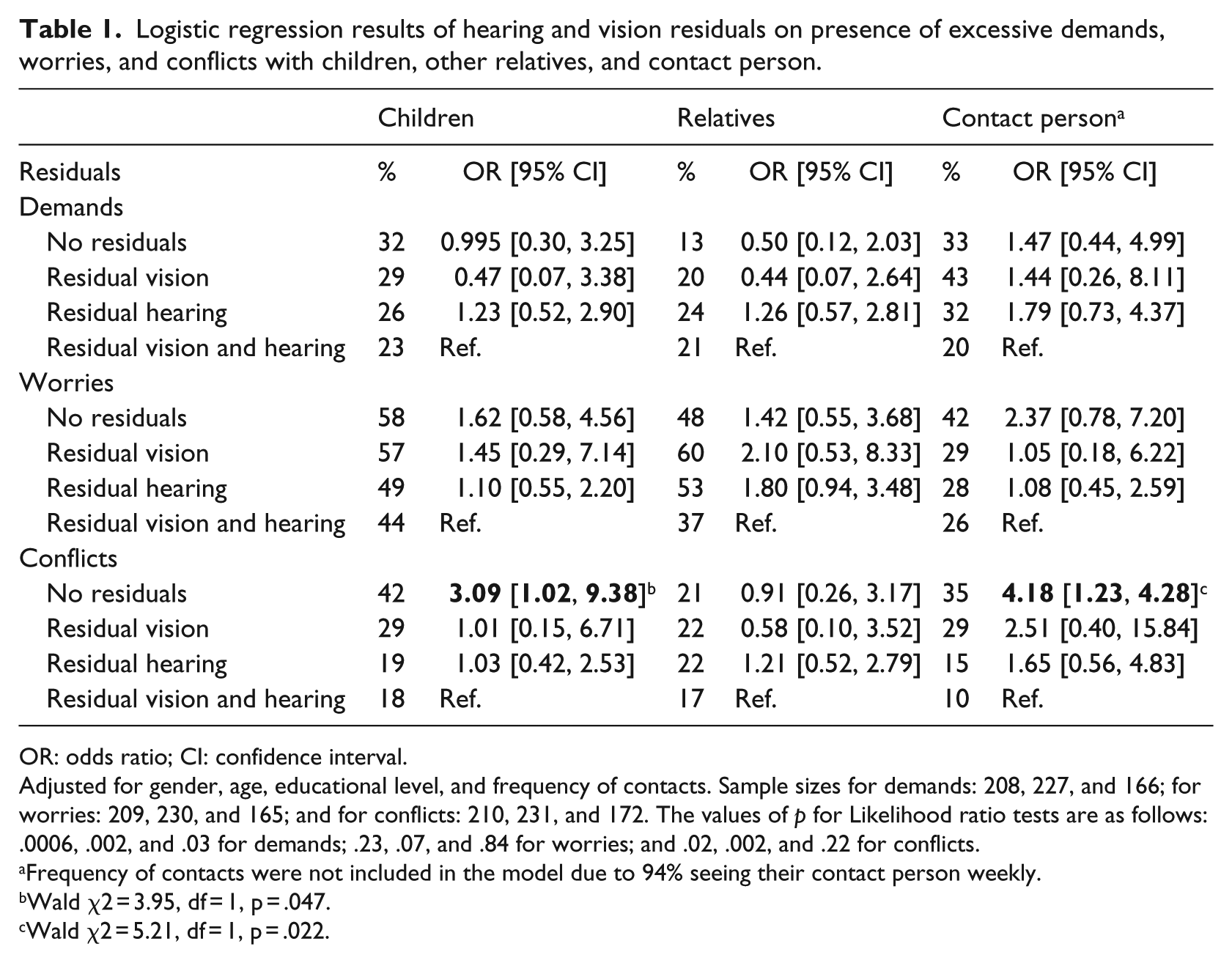
In relation to children, 32% of the participants with no residuals and 23% of the participants with residuals of both senses experienced excessive demands (Table 1). For relations with contact persons, the numbers were 33% and 20% (Table 1). The multivariate logistic regression models showed no significant associations between residual abilities and the experience of excessive demands from children (Wald χ2 = 0.87, df = 3, p = .83), other relatives (Wald χ2 = 2.31, df = 3, p = .51), or contact persons (Wald χ2 = 1.71, df = 3, p = .64) (Table 1). Thus, there was no support for the hypothesis that individuals with total blindness and profound deafness would have a higher odds for experiencing excessive demands from any of their relations compared to participants with both residual vision and hearing.
Logistic regression results of hearing and vision residuals on presence of excessive demands, worries, and conflicts with children, other relatives, and contact person.
OR: odds ratio; CI: confidence interval.
Adjusted for gender, age, educational level, and frequency of contacts. Sample sizes for demands: 208, 227, and 166; for worries: 209, 230, and 165; and for conflicts: 210, 231, and 172. The values of p for Likelihood ratio tests are as follows: .0006, .002, and .03 for demands; .23, .07, and .84 for worries; and .02, .002, and .22 for conflicts.
Frequency of contacts were not included in the model due to 94% seeing their contact person weekly.
Wald χ2 = 3.95, df = 1, p = .047.
Wald χ2 = 5.21, df = 1, p = .022.
Worries
The proportion of participants who had no residuals and worried for their children was 58%, whereas it was 44% for participants with residuals of both senses (Table 1). In relation to contact persons, it was 42% who worried for them among participants with no residuals and 26% among participants with residuals of both senses (Table 1). Again, the hypothesis was not supported and a multivariate logistic regression showed no significant association between residual hearing and vision and the proportion of participants experiencing worries for children (Wald χ2 = 0.99, df = 3, p = .80), other relatives (Wald χ2 = 3.79, df = 3, p = .28), or contact persons (Wald χ2 = 2.42, df = 3, p = .49) (Table 1).
Conflicts
In relation to children, 42% of participants with no residuals experienced conflicts, whereas it was 18% among those with residual vision and hearing (Table 1). The proportion of participants experiencing conflicts with contact persons was 35% for participants with no residuals and 10% for participants with residual abilities in both senses (Table 1). Again, there was no overall association between residual abilities and the experience of conflicts with children (Wald χ2 = 4.07, df = 3, p = .25), other relatives (Wald χ2 = 0.69, df = 3, p = .88), or contact persons (Wald χ2 = 5.36, df = 3, p = .15) (Table 1). However, post hoc analyses showed that participants with no residual hearing and vision had a three times higher odds of experiencing conflicts with children, odds ratio (OR) = 3.09, 95% confidence interval (CI) = [1.02, 9.38], and four times higher odds of experiencing conflicts with contact persons (OR = 4.18, 95% CI = [1.23, 4.28]) compared to the participants with residual abilities in both senses (Table 1).
Social desirability bias
Comparisons between those who had and had not received assistance completing the questionnaire with regard to the relational strain measures for that same relation showed no significant associations; thus, the variables of who assisted were not included in the multivariate logistic regression analyses (Results not shown).
Correlations
Almost all associations between outcome measures were significant (Table 2). The three strongest associations were experience of excessive demands from children and relatives, worries for children and relatives, and conflicts with children and relatives.
Spearman correlations between strain measures.
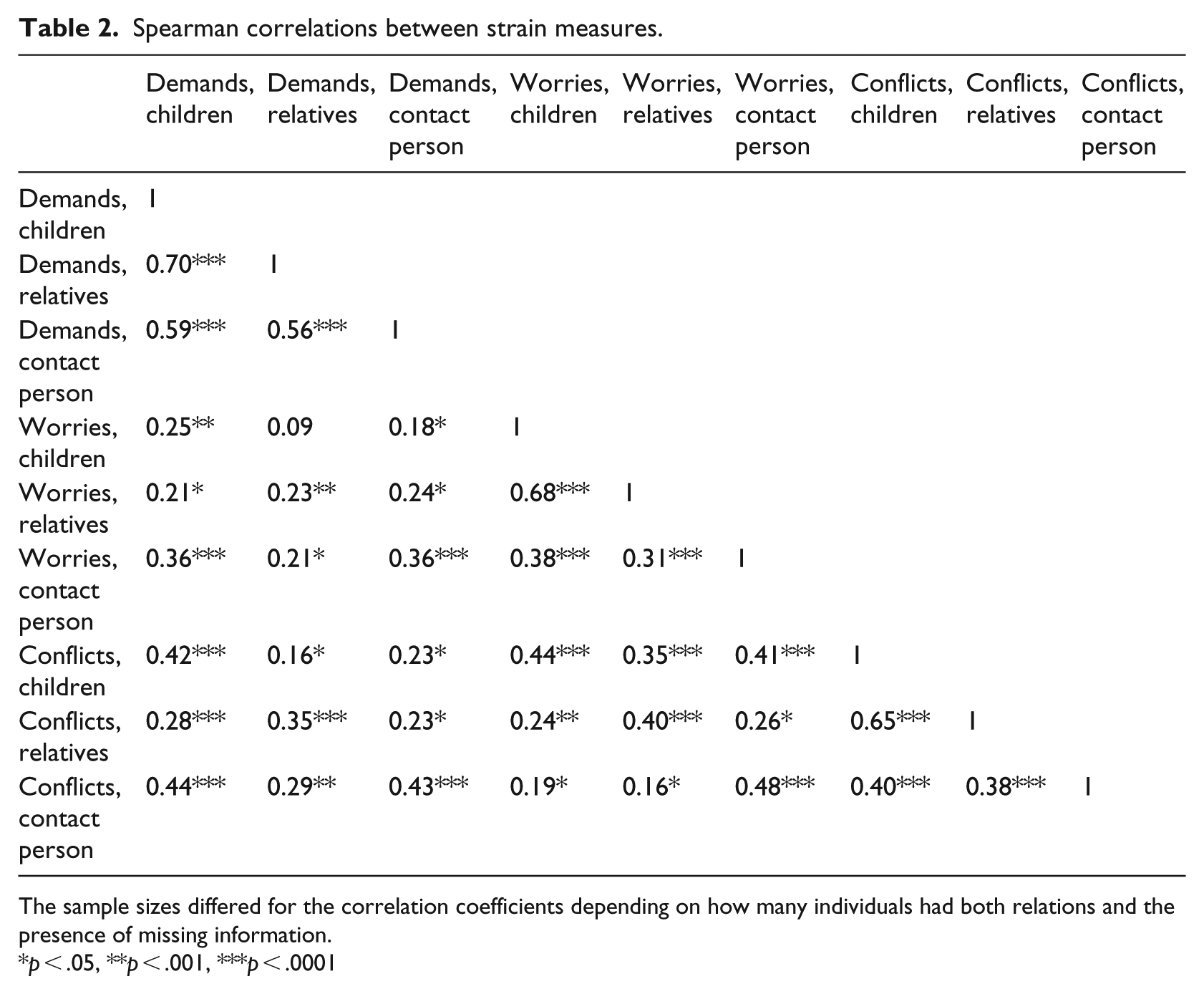
The sample sizes differed for the correlation coefficients depending on how many individuals had both relations and the presence of missing information.
p < .05, **p < .001, ***p < .0001
Discussion
The aim of this study was to investigate the frequency and types of strain and the association between severity of vision and hearing losses among people with DSL and relational strain, specifically excessive demands, worries, and conflicts with close social relations. Contrary to the hypothesis, the results revealed no overall associations between concurrent total blindness and profound deafness and relational strain with any type of relation. However, there were indications that participants with total blindness and profound deafness have higher odds for conflicts with children and contact persons compared to participants with residuals of both senses.
Overall relational strain
We evaluated three different types of relational strain: demands, worries, and conflicts, as several other studies have found different associations between the type of relation and the specific type of negative interaction (Antonucci et al., 2014; Birditt, Jackey, & Antonucci, 2009). A US study based on a general national representative sample of community-dwelling adults aged 65 years and older (n = 742) did not differentiate between the different types of negative interaction. They investigated the effect of communication difficulty on social exchanges and did not find an association between communication difficulty and negative social exchanges (Palmer, Newsom, & Rook, 2016). However, in this study, we differentiate between demands, worries, and conflicts and found different results for the three types of negative interaction. One reason for this could be that demands and worries are personal feelings, whereas conflicts are interpersonal.
Demands and worries
Individuals with DSL have previously reported feelings of overprotection and loss of independence (Hersh, 2013). Experiencing excessive demands can be due to other individuals demanding and expecting behavioral change of them, whereas a lack of demands might be a consequence of overprotection (Antonucci et al., 2014). One explanation for our results that no association between residuals and the experience of excessive demands was found could be that the individuals with no residuals are overprotected and are not challenged with demands by others to live independently. Furthermore, aging parents are perceived as placing a high demand on their children (Fingerman & Birditt, 2011); thus, it might be that the children experience excessive demands and not the parents with DSL. Another possible explanation for the lack of association between residual senses and excessive demands and worries could be that physical functioning, personality traits, and coping styles are stronger factors in predicting the experience of excessive demands and worries. This is supported by our finding of strong correlations between most of the strain measures (Table 2) and the findings of another US nation-wide longitudinal study, in a general sample of community-dwelling individuals aged 65 or older (n = 515), that negative exchanges and interpersonal conflicts tend to be stable over 6 years across different relations (Krause & Rook, 2003). However, it might be even more complex. Boerner, Reinhardt, Raykov, and Horowitz (2004) have studied stability and change in social negativity in a longitudinal study among adults aged 65 years and older with chronic visual impairment (n = 570). They found that initiated social negativity was stable but receiving social negativity reduced with age. Finally, because the participants of this study were of relatively old age, another reason might be that they have terminated negative social relations as suggested by the Socioemotional Selectivity Theory (Carstensen, Isaacowitz, & Charles, 1999). To test this explanation, a larger sample and longitudinal research is needed.
Conflicts
The proportion of participants experiencing conflicts in our study was somewhat higher than in another Danish study by Due et al. (1999), who described the structure and function of social relations in a general national random sample (n = 2011) of adults from the Danish Longitudinal Health Behaviour Study. The reason could be that Due et al. (1999) reported on those who responded that they experienced relational strain often and sometimes, whereas this study also included those who responded seldom and always. Another reason could be that the participants in our study are more dependent on their relations and cannot terminate relations with frequent conflicts as easily as people without sensory losses. As previously mentioned, individuals with DSL experience overprotection and communication breakdowns (Cimarolli et al., 2013; Heine et al., 2002; Hersh, 2013), which can contribute to interpersonal strain. A US study, performed in a general sample of individuals aged 13–99 years (n = 187), investigated intergenerational ambivalence. They reported that close social relations, where great amounts of social support and relational strain are present at the same time, can be ambivalent (Fingerman, Hay, & Birditt, 2004). Children and contact persons were the relations with whom our participants reported the most frequent contact; thus, these relations might also be subject to ambivalence. For instance, Hersh (2013) reported experiences of impatience from communication partners as communication with an individual with sensory loss can be difficult; communication partners may also feel anger or irritation if the individual with DSL, for example, does not hear and respond to a question. This is referred to as third-party disability (Scarinci, Worrall, and Hickson, 2012). It is plausible that individuals with some residual senses adapt using their residual abilities to maintain communication; thus, those without residual hearing and vision will experience greater problems in social interaction (Hersh, 2013). This could be the reason for our results only showing a potential difference between participants with no residuals and participants with residuals of both senses in relation to conflicts with children and contact persons.
Limitations
Our study has several limitations. The cross-sectional design means that we have not been able to study the development of relational strain and its connection to vision and hearing loss over time. This would be an important aim for future research. Another limitation is statistical power. Due to the somewhat low prevalence of acknowledged DSL and the challenges in accessibility to participate in questionnaire surveys, this study might be underpowered. Third, some of the participants in the study received help from their close social relations to complete the questionnaire. This might have affected the responses of those participants, leading to a risk of social desirability bias. We tried to examine this by investigating the associations between outcome measures and those who assisted in the completion of the questionnaires. However, as these examinations did not show significant differences in patterns of response depending on who assisted, the potential risk of bias is believed to be low.
Finally, medical assessments of hearing and vision would have improved the validity and reliability of the measures of severity of hearing and vision impairment. Medical data were not possible to obtain for this study, but it is recommended that future studies include such measures.
The proportion of individuals with no residual senses is lower in our sample compared to the full population receiving rehabilitative services in Denmark. This may have potentially biased the results of this study. The direction of bias will depend on the level of relational strain among those who have declined to participate. Furthermore, the results might not be fully representative for all individuals with DSL.
Conclusion and implications
No associations between having residual hearing and vision or not and the experience of excessive demands and worries were found, but individuals with total blindness and profound deafness had significantly higher odds for experiencing conflicts with children and contact persons compared to individuals with residuals of both senses. In supporting people with DSL, it is important to be aware of this risk factor to promote healthy relations for older adults with DSL. But overall, this study underlines that individuals with DSL form a heterogeneous group – also with regard to social relations. We recommend that future studies look further into the nature of the relational strain experienced by people with DSL and investigate how other factors such as personal characteristics, coping, and communication abilities and support might influence their social relations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Velux Foundation (VELUX33847).