
Abstract
We decided to conduct a study to determine the prevalence of visual impairment, blindness, refractive errors, and other visual functions in nursing homes of Iran. In this cross-sectional study, 133 elderly persons were selected from seven nursing homes using proportional-to-size random sampling. A Snellen chart was used to measure visual acuity (VA). Refraction was measured in all participants using autorefractometry and retinoscopy. A cover test was applied to assess ocular deviation. Stereopsis, color vision, and contrast sensitivity were evaluated with distance glasses. The prevalence (95% confidence interval [CI]) of visual impairment (VI) (<20/60), low vision (<20/60 to <20/400), and blindness (⩽20/400) was 41.88% (32.81–50.95), 32.48% (23.87–41.09), and 9.40% (4.03–14.77), respectively, based on best-corrected visual acuity (BCVA). The prevalence of myopia (spherical equivalent (SE) < −0.5 D), hyperopia (SE < 0.5 D), and astigmatism (cylindrical power < 0.5 D) was 53.50% (44.19–62.58), 36.84% (28.38–46.19), and 86.84% (79.17–91.97), respectively. VI and refractive errors had no association with age and sex (p-value > .05 for all). The prevalence of other ocular diseases was as follows: cataract 66.06% (57.02–75.09), glaucoma 1.52% (1.85–5.40), one eyed caused by injury 6.10% (2.67–11.67), and corneal opacity 3.81% (1.25–8.68). The prevalence of VI was 4–20 times and the prevalence of cataract was 3–4 times higher in NHRs compared with community-dwelling older people, indicating the grave situation of vision in these people. It is necessary to conduct further studies to find the reasons behind this disparity and perform interventions, including periodic and screening examinations upon entry to nursing homes to decrease the burden of ocular diseases in NHRs.
Introduction
Improved living conditions and longevity have increased the aging population in many countries (Whitmore, 1989), leading to increased prevalence of age-related ocular diseases and visual disorders like glaucoma and cataract (Friedman et al., 2004). A review of the literature shows that ocular diseases and visual impairment (VI) in older people threaten their function independence, including their daily living, quality of life, and mobility (Horowitz, 1994; West et al., 2003).
Increased aging population raises the demand for nursing and care services, which in turn increases the population of nursing home residents (NHRs) (Danial, Motamedi, Mirhashemi, Kazemi, & Mirhashemi, 2014). Although studies have shown that the prevalence of ocular diseases and visual disorders, like VI, cataract, and refractive errors, is high in community-dwelling elderly people (Hashemi, Khabazkhoob, Emamian, Shariati, & Fotouhi, 2012; Tielsch, Javitt, Coleman, Katz, & Sommer, 1995; VanNewkirk et al., 2000; Yekta et al., 2009), the situation is even worse for NHRs (de Winter, Hoyng, Froeling, Meulendijks, & van der Wilt, 2004; Horowitz, 1994; Jack, Smith, Neoh, Lye, & McGalliard, 1995; Klein, Klein, Linton, & De Mets, 1991; Mitchell, Hayes, & Wang, 1997; Owsley et al., 2007a; Owsley et al., 2007b; Taiel-Sartral et al., 1999; Tielsch et al., 1995; Van der Pols et al., 2000; VanNewkirk et al., 2000; West et al., 2003; Whitmore, 1989).
The higher prevalence of VI, cataract, and refractive errors in NHRs underline the importance of studies in this population (Mitchell et al., 1997; Owsley et al., 2007a). Depending on the study type and definition, the prevalence of VI in NHRs is 3–15 times higher than its prevalence in community-dwelling older persons (de Winter et al., 2004; Horowitz, 1994; Mitchell et al., 1997; Owsley et al., 2007a; Taiel-Sartral et al., 1999; Tielsch et al., 1995; Van der Pols et al., 2000; VanNewkirk et al., 2000; Whitmore, 1989; West et al., 2003). Moreover, the prevalence of cataract is up to 80% (de Winter et al., 2004; Jack et al., 1995; Owsley et al., 2007a; Whitmore, 1989; Tielsch et al., 1995) and the prevalence of refractive errors is upto 50% (Owsley et al., 2007b) in this population. The reason for this disparity is not clear, but studies have suggested several factors like lower access to eye care services and mobility limitations (Friedman et al., 2004; Owsley et al., 2007a). More importantly, most causes of ocular problems in NHRs are treatable and therefore vision loss can be prevented through identification and treatment of the cause (de Winter et al., 2004; Tielsch et al., 1995).
Since Iran’s population is aging, the number of NHRs is on the rise as a result of lifestyle changes and increased number of abandoned elderly people (Danial et al., 2014). Several studies have investigated visual health in NHRs in the world (de Winter et al., 2004; Friedman et al., 2005; Mitchell et al., 1997; Owsley et al., 2007a; Taiel-Sartral et al., 1999; Tielsch et al., 1995; Whitmore, 1989), which have provided health policymakers and stakeholders with comprehensive information on the visual status of these people and the eye care services they have received to make policies and plans for visual health improvement. However, to the best of our knowledge, no study has evaluated the visual status of NHRs in Iran. Therefore, we decided to conduct a study to determine the prevalence of VI, blindness, refractive errors, and other visual functions in nursing homes of Iran.
Materials and methods
This descriptive, analytical, and cross-sectional study was conducted in elderly people above 55 years who lived in nursing homes of Mashhad in 2009. The sample size was calculated 121, considering a prevalence of 57% for VI in a similar study (Owsley et al., 2007a), precision of .09, and Type I error of 5%. The calculated sample size was increased by 10% to provide a better estimate of the study outcomes, so the final sample size was 133 participants. There are seven nursing homes in Mashhad. A list of all elderly people in each nursing home was prepared, and 133 elderly persons were selected using random proportional-to-size sampling. The objectives of the study were explained to the subjects and informed consent was obtained from all of them. Then, all participants received the Mini-Mental State examination (MMSE). This tool contains 13 questions with a total score ranging from 1 to 30 and is used to assess the mental state and detect cognitive impairments. Studies have shown that people suffering from mild to moderate cognitive impairment (scores above 15) give reliable answers to oral questions during an interview (Danial et al., 2014; Friedman et al., 2005; Friedman et al., 2004; Owsley et al., 2007a; West et al., 2003).
Examinations
The general health condition and the presence of systemic diseases, including hypertension, diabetes, hyperlipidemia, and Alzheimer’s disease, as well as ocular diseases like cataract, glaucoma, corneal opacity, and history of ocular surgery were extracted from the participants’ medical records. Then, all subjects underwent optometric and ophthalmological examinations, starting with distance uncorrected visual acuity (VA) measured with a Snellen chart. Then, objective refraction was measured using an auto refractometer (Topcon RM8800 autorefractor, Topcon Corporation, Japan), and the results were refined with a retinoscope (BETA 200 retinoscope, HEINE Optotechnic, Germany). If the retinoscopic reflex was not clear for reasons like a small pupil diameter or media opacity, radical retinoscopy was done at a closer than standard distance. Subjective refraction was done in the next stage, and the best-corrected distance and near VA was recorded. Then, distance and near cover tests were applied to assess the status of binocular alignment at 6 m and 40 cm, using distance and near optical correction. The target used for the cover test was one line above the corrected VA threshold on the near and distance Snellen chart.
Contrast sensitivity was measured with distance glasses using the Pelli-Robson contrast sensitivity chart (60 cm x 90 cm) at 1 m, which corresponds to a spatial frequency of 1 cycle/degree. This chart has eight lines, and each line contains six letters organized as two triplets per line. In each line, the triplet on the left has a higher contrast than the triplet on the right. The contrast also decreases line by line from top to bottom, and the test result is presented in a logarithmic scale as 1/contrast. Finally, subjects with an uncorrected VA worse than 20/20 underwent slit lamp biomicroscopy (BM 900, Haag Streit, Mason, Ohio, United States).
Definitions
A best-corrected visual acuity (BCVA) worse than 20/60, but better than 20/400 in the better eye, was considered low vision, and a VA worse than 20/400 was considered blindness (Dandona & Dandona, 2006). Myopia was defined as a spherical equivalent (SE) equal to or worse than −.5 D, and hyperopia was defined as a SE worse than .5 D. A person with a refractive error in at least on eye was considered a case of refractive error. If one eye was myopic and the fellow eye was hyperopic, the person was considered a case of myopia. Astigmatism was defined as a cylindrical power worse than .5 D in at least one eye.
If the dementia test was positive, VA was measured three times. The result of VA testing was not recorded if at least two of three measurements were not consistent.
Statistical analysis
Mean and 95% confidence interval (CI) was used for quantitative data analysis and percentage and 95% CI were used for data description. T test, X (Friedman et al., 2004) test, and analysis of variance (ANOVA) were used for comparison of variables according to age and sex. p-values less than .05 were considered significant.
Ethical issues
The Ethics Committee of Mashhad University of Medical Sciences approved the study protocol, which was conducted in accord with the tenets of the Helsinki Declaration. All participants signed a written informed consent.
Results
Of 133 invited persons, 131 participated in the study (response rate = 98.5%). The mean age of the participants was 77.67 ± 8.43 years and 68.7% of them were women. According to documents and subjects’ records in the nursing homes, the prevalence (95% CI) of hypertension, diabetes, hyperlipidemia, and Alzheimer’s disease was 28.24% (21.11–36.65), 19.84% (13.81–27.67), 12.21% (.7–19.11), and 54.19% (45.51–62.63), respectively. The mean ± SD score of MMSE was 16.16 ± .29 and 44% of the subjects had MMSE scores > 15.
According to the subjects’ medical records, a history of ocular surgery, unilateral cataract surgery, and bilateral cataract surgery was seen in 15.26% (10.01–22.59), 7.63% (4.12–13.7), and 9.92% (5.80–16.44) of the participants, respectively. Cataract was detected in 66.06% (57.02–75.09) of the participants, which was unilateral in 18.35% (10.97–25.73) and bilateral in 47.71% (38.18–57.23). The prevalence of glaucoma, having one eye due to trauma, and corneal opacity was 1.52% (1.85%–5.40), 6.10% (2.67–11.67), and 3.81% (1.25–8.68), respectively.
According to the BCVA, the overall prevalence of VI, low vision, and blindness was 41.88% (32.81–50.95), 32.48% (41.09–23.87), and 9.40% (4.03–14.77), respectively. Table 1 shows the prevalence of VI, low vision, and blindness according to age groups. According to Table 1, the highest prevalence of VI and low vision was in the age group above 85 years and the highest prevalence of blindness was seen in the age group 61–65 years. However, we found no difference in the prevalence of VI, low vision, and blindness according to age (p-value: .224, .522, and .858, respectively). According to sex, the prevalence of VI and low vision was higher in women while the prevalence of blindness was higher in men, but the difference was not significant (p-value: .227, .147, and .624, respectively). The most important cause of VI was refractive errors, followed by cataract and glaucoma (Table 3).
Prevalence of refractive error and visual impairment based on age and sex in nursing home resident in Iran.

CI: confidence interval; BCVA: best-corrected visual acuity; #: no observation.
Based on BCVA.
The mean SE was −0.18 D (−1.01–0.62) in the right eye and −.3 D (−1.06–0.45) in the left eye. According to Table 1, the prevalence of myopia, hyperopia, and astigmatism was 53.50% (44.19–62.58), 36.84% (28.38–46.19), and 86.84% (79.17–91.97), respectively. The highest prevalence of myopia and hyperopia was seen in the age group above 85 year and 61–65 years, and the highest prevalence of astigmatism was seen in the age groups 55–60 and 66–70 years. However, there was no significant difference in refractive errors according to age (p-value: .305, .264, and .427, respectively). According to age, the prevalence of myopia and astigmatism was higher in men and the prevalence of hyperopia was higher in women, although the difference was not significant (p-value: .335, .611, and .101, respectively).
Exophoria was the most common condition in near (37.37%, 95% CI: 27.85–47.67) and distance cover test (13%, 95% CI: 7.10–21.20). As for contrast sensitivity in the left and right eye, the highest frequency was related to contrast sensitivity between 1.5 and 1.8 (43.3% for both eyes). The highest frequency of binocular contrast sensitivity was related to contrast sensitivity above 1.8 (38.5%). An abnormal binocular contrast sensitivity was seen in 30.8% of the subjects who underwent the contrast sensitivity test (a score of below 1.5 on the Pelli-Robson test) (Table 2).
Results of cover test and contrast sensitivity in nursing home residents.
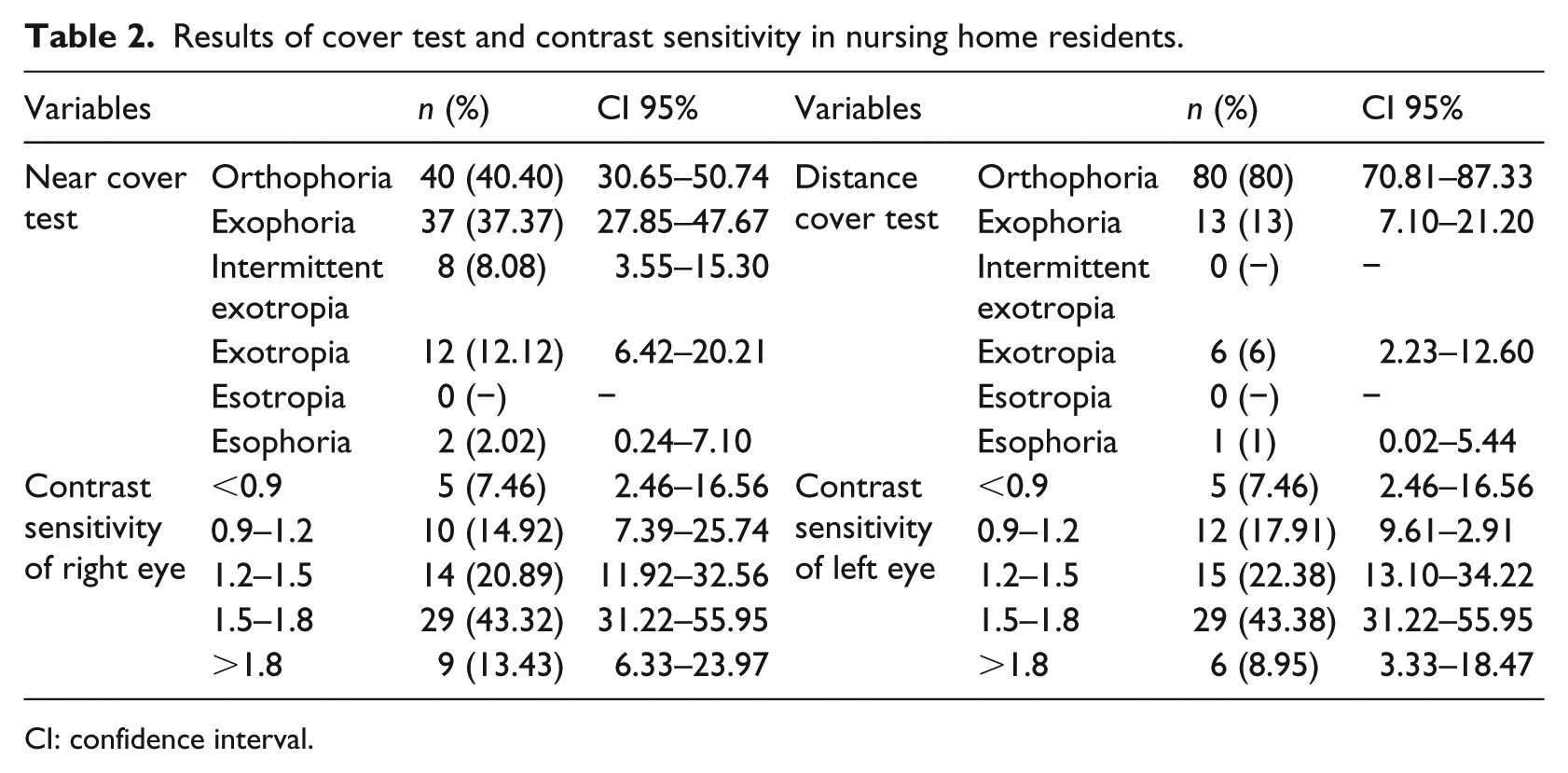
CI: confidence interval.
Of 55 participants who had prescription glasses, 28 did not wear them regularly, mostly because wearing them did not improve their vision (50%). About 40% of the participants had their eyes examined more than 2 years ago, and about 20% of them never received eye examinations. On the other hand, the most important reason for moving to a nursing home was loneliness followed by systemic diseases (Table 3).
Other visual characteristics of nursing home residents.
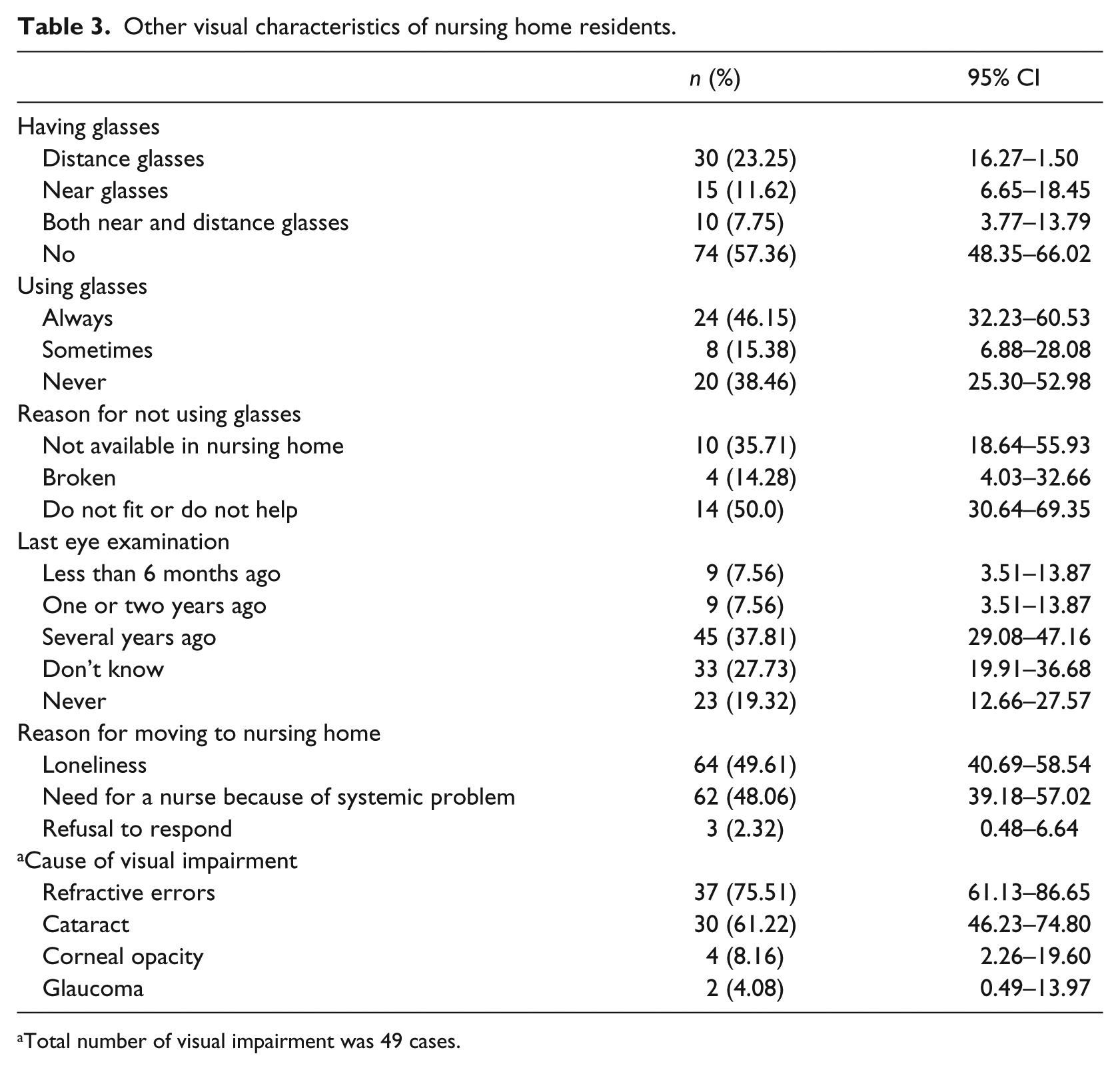
Total number of visual impairment was 49 cases.
Discussion
According to BCVA < 20/60, of every 10 NHRs, 4 had VI (3 had low vision, and 1 was blind). The high prevalence of refractive errors and cataract indicates the grave condition of ocular problems and suggests urgency in delivery of eye care services. Before comparing the results of different studies, it should be noted that the characteristics of NHRs are associated with both within-country and between-country variations; therefore, caution should be practiced when comparing the results. According to Table 4, which presents the prevalence of VI in similar studies, the prevalence of VI in our study was higher than some (de Winter et al., 2004; Friedman et al., 2004; Horowitz, 1994; Mitchell et al., 1997; Owsley et al., 2007a; Tielsch et al., 1995; West et al., 2003; Whitmore, 1989) and lower than some other studies (VanNewkirk et al., 2000; Waked, Saad, Mehanna, Sleilaty, & Kortbaoui, 2007), which could be due to differences in the definition or ethnicity and race of the participants. On the other hand, the prevalence of VI in our participants was 4–20 times higher when compared to its prevalence in similar age groups of community-dwelling people, as domestic studies have reported a prevalence of 2–11% (Hashemi, Khabazkhoob, Emamian et al., 2012; Hashemi, Khabazkhoob, Saatchi, Ostadimoghaddam, Yekta, 2017; Hashemi, Yekta, et al., 2017; Yekta et al., 2011; Yekta, Hashemi, Ostadimoghaddam, Shafaee, Norouzirad, Radaye-moghaddam, et al., 2013), which is far lower than our results. In line with our study, some other studies have also reported a higher prevalence of VI in NHRs as compared to community-dwelling older persons (de Winter et al., 2004; Horowitz, 1994; Klein et al., 1991; Mitchell et al., 1997; Owsley et al., 2007a; Taiel-Sartral et al., 1999; Tielsch et al., 1995; Van der Pols et al., 2000; VanNewkirk et al., 2000; West et al., 2003; Whitmore, 1989). The reason for this disparity is not clear. It seems that more visually impaired people are taken care of in nursing homes due to the negative effect of vision loss on independent functions (Friedman et al., 2004). On the other hand, people suffering from VI lack the independence for daily activities and have a higher chance of being transferred to the nursing home (Hashemi et al., 2013). Moreover, NHRs have a lower access to specialists as a result of lack of transportation and escort availability, and the physicians who visit nursing home periodically consider a short time for examinations (Hashemi et al., 2013). Furthermore, many NHRs who have glasses may not wear them because they do not improve their vision (Owsley et al., 2007a). All the above reasons lead to increased prevalence of untreated eye disease in these people. Contrary to the above study, we found no significant association between age and VI in our subjects.
Prevalence of visual impairment in nursing home residents based of similar studies.
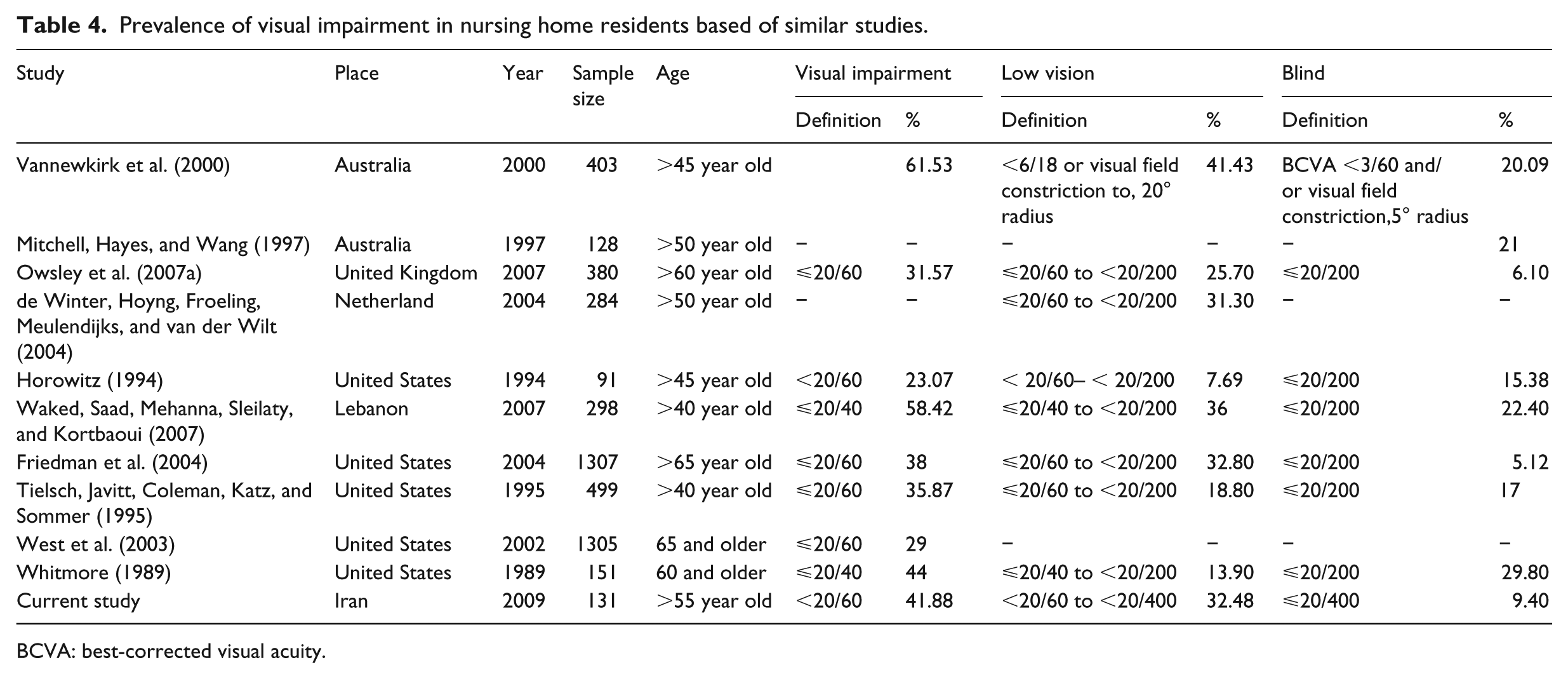
BCVA: best-corrected visual acuity.
Studies have shown that in addition to VI, the prevalence of refractive errors is also high in NHRs. Owsley et al. (2007b) reported a prevalence of 42.25% and 26.76% for myopia and hyperopia in nursing homes of Birmingham, respectively, which are lower than our findings, indicating the more serious condition of NHRs in Iran. Comparison of the prevalence of refractive errors between our study and studies investigating community-dwelling older people (Hashemi, Khabazkhoob, Yekta, et al., 2012; Javadi et al., 2004; Yekta et al., 2009; Yekta, Hashemi, Ostadimoghaddam, Shafaee, Norouzirad, & Khabazkhoob, 2013; Ziaei et al., 2013) also shows a lower prevalence of myopia, hyperopia, and astigmatism in these studies. This is while refractive errors were the most important cause of VI in our study, which could be simply treated with prescription glasses (Jack et al., 1995).
Studies have shown an increase in the prevalence of hyperopia and astigmatism with age which could be due to presbyopia (Hashemi, Khabazkhoob, Yekta, et al., 2012; Javadi et al., 2004; Yekta et al., 2009; Yekta, Hashemi, Ostadimoghaddam, Shafaee, Norouzirad, & Khabazkhoob, 2013; Ziaei et al., 2013). However, we found no significant association between age and different types of refractive errors.
Our results showed a high prevalence of cataract in NHRs (18.35% in one eye and 47.71% in both eyes), which is consistent with the results of a study by Whitmore et al. (Whitmore, 1989) but higher than other studies (de Winter et al., 2004; Friedman et al., 2005; Jack et al., 1995;
Owsley et al., 2007a; Tielsch et al., 1995). The prevalence of cataract in Iranian community-dwelling older people is reported to be 12%–16% (Hashemi, KhabazKhoob, Miraftab, Mohammad, & Fotouhi, 2011; Owsley et al., 2007c), which is much lower than its prevalence in NHRs. The high prevalence of cataract in NHRs may be due to lower rate of eye examination in these people, lack of knowledge about cataract surgery, or lack of family support for surgery (Friedman et al., 2005). The finding is very important because cataract was the leading cause of VI in a study by de Winter et al. (2004) and the second cause of VI in our study as well as the study conducted by Owsley et al. (2007b). Cataract surgery boosts vision and increases independence, leading to improved quality of life in older people.
A marked percentage of the NHRs in this study had glasses, but about half of them wore glasses regularly because their glasses did not fit or improve their vision. This finding indicates a high prevalence of unmet need in this population, which can be easily addressed with prescription of proper glasses. On the other hand, it seems that routine eye care does not occur in many nursing homes since 40% of the subjects had their eyes examined more than 2 years ago, which is a very long time, and 20% never had their eyes examined during their residence in the nursing home. Considering the above and the high prevalence of VI and refractive errors, it is highly recommended to set up periodic eye examinations in these centers to improve the NHRs’ quality of life through addressing their visual needs.
Although it is clear that VI has negative impacts on the health-related quality of life and activity in the elderly, most subjects in our study mentioned that they were moved to the nursing home for other reasons like loneliness or systemic diseases, which is consistent with the results reported by Owsley et al. (2007a). Contrary to the results of a study by Wang, Mitchell, Cumming, Smith, and Blue Mountains Eye Study (2003), it seems that VI is not an independent factor for sending people to the nursing home and has a secondary or intermediary role in this regard.
We also measured contrast sensitivity in our study. Abnormal binocular contrast sensitivity defined as a score of below 1.5 on the Pelli-Robson test is used as an indicator for detection of disorders in near activities like mobility and reading (Owsley et al., 2007c).
In our study, the score of the Pelli-Robson test was below 1.5 in 30.8% of the subjects, which was lower than the results reported by Owsley et al. (2007a) but higher than a study in community-dwelling older people, indicating a far worse visual state of NHRs in comparison with age-matched community dwellers.
One of the strong points of this study was using several information sources like interview with NHRs, different measurement tools, and their records for determining their visual status. Unlike similar studies, in addition to distance VA, we also evaluated the participants’ visual field and contrast sensitivity. To the best of our knowledge, this was the first study of the NHRs’ visual status in Iran. However, this study also had some limitations. For example, we could not evaluate possible reasons for low eye care utilization in nursing homes (staff shortage, low knowledge of eye care services, lack of infrastructure, etc.), which need to be addressed in future studies.
Conclusion
According to BCVA worse than 20/60, 40% of the study population suffered from VI, which is 4–20 times higher than the results of studies in community-dwelling older people. The prevalence of other ocular problems, like refractive errors and cataract, was also high. Unmet refraction needs also had a very high prevalence, as about half of the people who had glasses did not use them because they did not fit their vision. This is while refractive errors, which can be simply treated with glasses, were the leading cause of VI in our patients. Considering the high prevalence of visual problems, it is suggested that studies should be designed to find the reasons for this disparity in order to decrease the burden of VI and other visual problems through effective interventions like periodic examinations and screening tests upon entry to nursing homes.
Footnotes
Funding
This project was supported by Mashhad University of Medical Sciences.