
Abstract
This study describes the self-estimated functional ability of older adults with visual impairments (VI) living at home prior to and after 24 months of individual low vision rehabilitation (LVR) according to the International Classification of Functioning, Disability and Health (ICF) framework. The LVR was carried out according to regular standard of care in Finland. The study provides knowledge that is relevant for improving both LVR as well as other services for older adults living with VI. Thirty-nine older adults with VI initially participated in the study with 28 remaining for the follow-up at 24 months of LVR. Data were collected by an orally administered questionnaire including items from the Oldwellactive Wellness Profile instrument. Data were analyzed using the marginal homogeneity test, and the outcomes were divided into four categories according to the ICF framework. Comparisons between the baseline and 2-year follow-up revealed statistically significant decreases in daily functions, including going outdoors (p = .011), washing oneself (p = .016), taking care for personal hygiene (p = .046), dressing (p = .034), preparing meals (p = .041), and doing heavy housework (p = .046), following 2 years of received LVR. A statistically significant increase in the need for help was also observed during the study period (p = .025). The independence of older adults with VI decreased, and the need for external services or help increased during 24 months after the onset of receiving LVR. Visual problems were shown to widely affect functional ability. Activities and participation dimension together with loneliness are most affected and need attention in individual LVR.
Background
The global population is rapidly growing, and people all over the world are living longer than before (World Health Organization [WHO], 2018). Life expectancy is increasing in Finland also, with estimates suggesting that 26% of the population will be over 65 years in the year 2030 (Finnish Bureau of Statistics, 2015).
An aging population can be expected to increase the incidence of vision problems (Ray & Wolf, 2008). Visual impairments (VI) and blindness are among the 15 diseases that most severely burden the elderly (Prince et al., 2015). According to the WHO (2019), there are over 2.2 billion people with impaired vision in the world. It has been proposed that the scale of global burden of VI is comparable to that of Alzheimer’s disease and other memory disorders (WHO, 2011a). Poor visual performance results in considerable problems managing everyday tasks (Ray & Wolf, 2008). The WHO criteria define VI as visual acuity of <0.3 in the better eye (Ojamo, 2018; WHO, 2019). In this study, LVR was carried out according to the regular standard of care in Finland, which is offered to people who meet the WHO criteria. LVR aims at independence and active participation in society despite disability, as well as optimal use of residual visual functions (Markowitz, 2016). LVR services are provided to people living with VI by specialized healthcare as a multidisciplinary professional service. LVR is a highly individual service including various actions that range from assistive devices and modifications at home to disability-related support, counseling, and guidance.
Functional ability is a wide concept that encompasses all body functions and structures, activities, and participation (Pohjolainen & Saltychev, 2015). Furthermore, functional ability covers physical, psychological, and social aspects of how a person lives his or her daily life (Finnish Institute for Health and Welfare (THL), 2019). Descriptions of functional ability must take into account the existing life situation of a person because functional ability is not a static state (Pohjolainen & Saltychev, 2015). In this way, functional state is clearly an essential part of health and can accurately describe a person’s state of health (Üstün et al., 2003). For example, activities of daily living (ADL) deteriorate as the human body ages (Finnish Institute for Health and Welfare (THL), 2019; Silva et al., 2018). Two individuals with the same diagnosis may have completely different levels of activity. Functional ability includes both the effects of illness(es) and biological aging; therefore, it can provide a comprehensive picture of the health of older adults (WHO, 2011b).
The International Classification of Functioning, Disability and Health (ICF) provides a uniform framework for multiprofessional work and helps the various specialists in the team to understand functioning in the same way (Leissner et al., 2014). It considers health, body functions, and structures as well as activity and participation together with environmental and personal factors. Both are often important for older adults and visually impaired people. The ICF also provides a scientific basis for understanding and studying health and health-related states, outcomes, and determinants (Leissner et al., 2014; WHO, 2011b).
Aim
The present research aimed to describe the functional ability of older adults with VI prior to and after 24 months of regular standard of care low vision rehabilitation (LVR). The research question for this study was as follows:
Methods
Ethics
The Northern Ostrobothnia Hospital District granted the study permission, while a regional ethical committee provided a supporting statement. Participation in the study was voluntary and based on informed consent. The participants had the right to retract their participation from the study at anytime. Good scientific practice (Finnish National Board on Research Integrity [TENK], 2013) and the World Medical Association’s (WMA, 2013) Declaration of Helsinki were followed at every stage of the present research.
Data collection and study design
The data were collected between May 2016 and July 2019. This study is part of a longitudinal follow-up study (Siira et al., 2019a, 2019b, 2020) carried out at the Low Vision Center of the Oulu University Hospital (OLVC). The participants (n = 39) were older adults who were visually impaired according to the WHO criteria. The participants were living at home in Northern Ostrobothnia in northern Finland and were referred for LVR with no prior history of LVR. The participants had an average age of 83 years (SD: ±6.5, range: 70–93). In this study, data were collected prior to and after 24 months of LVR at the OLVC. Data were collected by wellness profiling approach (Oldwellactive) by Koistinen et al. (2013). The instrument was administered verbally. The participants also had a complete ophthalmic evaluation during their visit.
The Oldwellactive questionnaire was used in the interviews to obtain the self-reported functional abilities of the participating older adults. Oldwellactive was developed in Oulu, Finland, so that older adults can self-estimate their wellness and well-being (Koistinen et al., 2013). The complete Oldwellactive wellness profile contains both questionnaire-based assessments and physical measurements, such as the chair-stand test and handgrip measurement. The questionnaire has nine domains: independence; physical capability; mental capability; social network; loneliness; security; perceived health; lifestyle; and quality of life. The entire questionnaire contains 75 multiple-choice items scored on a 4-point Likert-type scale, ranking generally from 1 (poor) to 4 (excellent) (Koistinen et al., 2013). In this study, 35 items from eight domains were selected to describe functional ability matching the ICF framework.
Statistical analysis
The data were analyzed using SPSS software (version 25.0; IBM Corporation, Armonk, NY). Frequencies, percentages, and means were calculated to describe the characteristics of the research population. Self-estimated functional ability was analyzed by the nonparametric marginal homogeneity test. The ICF framework was taken into consideration when Oldwellactive items were being selected for the study, and selected items were combined for the analyses. A p value of .05 was set as the threshold for statistically significant difference.
Results
Background characteristics
The participants (n = 39) were 70–93 years old, most of them (59%, n = 23) between 80 and 89 years old. At the beginning of the research, the mean age was 83 years (SD: ±6.5), the median age also being 83 years. Almost one-third of the participants (31%, n = 12) were men. Most of the participants (64%, n = 25) lived alone and 18% (n = 7) had no children of their own (Table 1).
Participants’ background characteristics at the start (n = 39) and after 24 months (n = 28) of LVR.
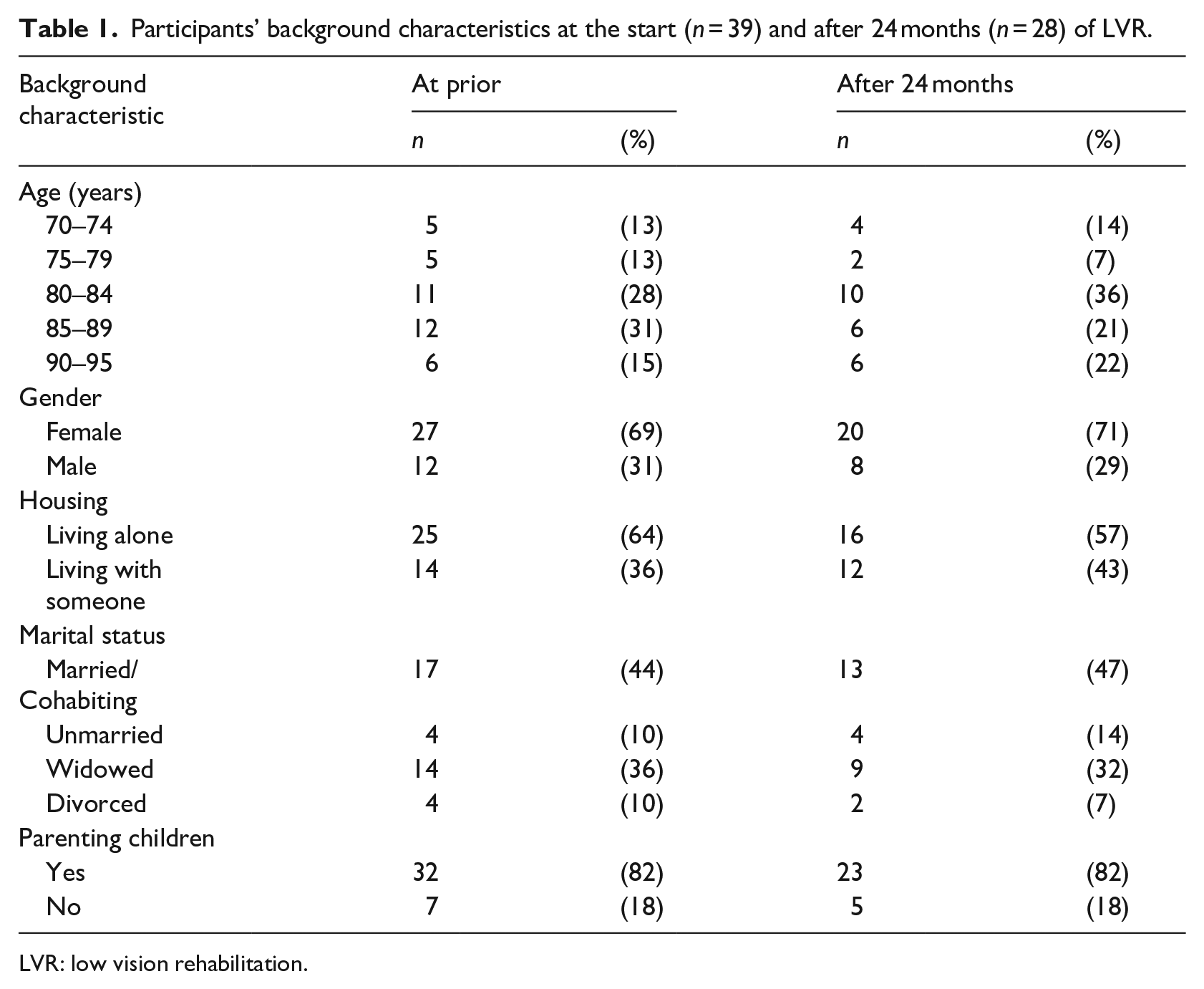
LVR: low vision rehabilitation.
Functional ability prior to and after 24 months of LVR
The number of responses to each item varies between 19 and 28 and is presented for each item in Tables 2–5. The percentages shown are calculated accordingly. The results are reported in accordance with the four ICF categories.
Results for ICF categories related to body functions and body structures.
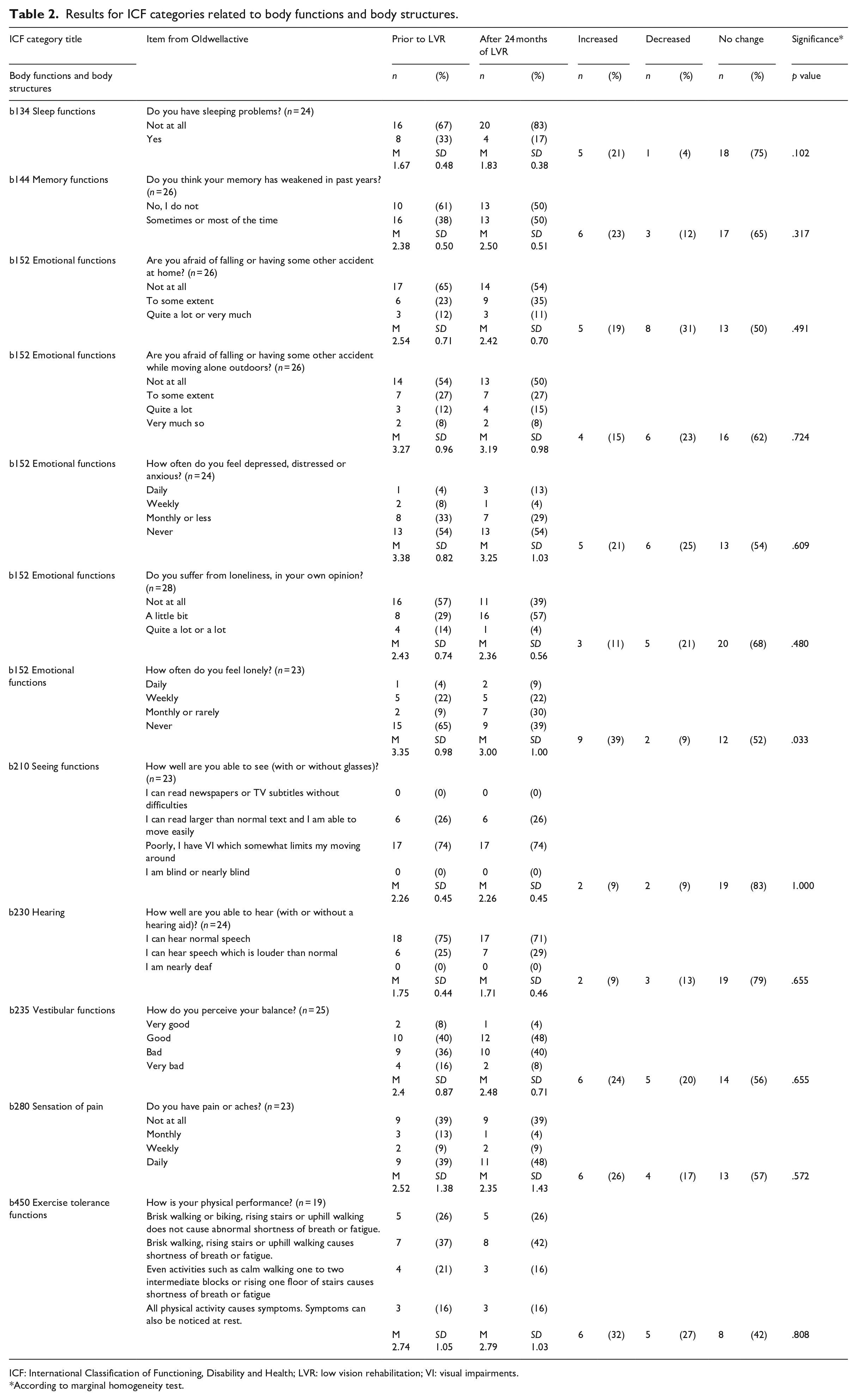
ICF: International Classification of Functioning, Disability and Health; LVR: low vision rehabilitation; VI: visual impairments.
According to marginal homogeneity test.
Results for ICF categories related to activities and participation.

ICF: International Classification of Functioning, Disability and Health; LVR: low vision rehabilitation.
According to marginal homogeneity test
Results for ICF categories related to environmental factors.
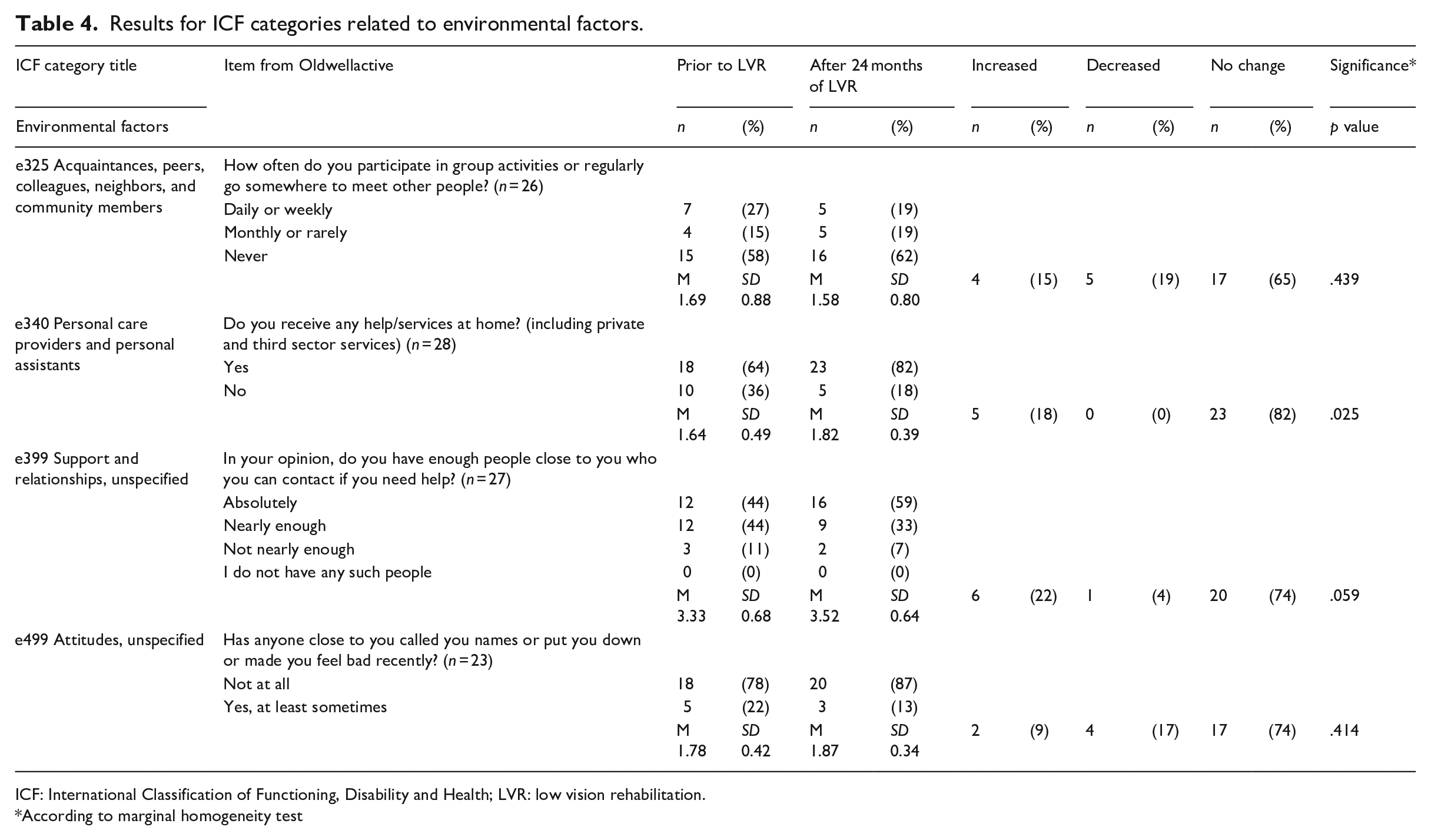
ICF: International Classification of Functioning, Disability and Health; LVR: low vision rehabilitation.
According to marginal homogeneity test
Results concerning personal factors in the ICF framework.
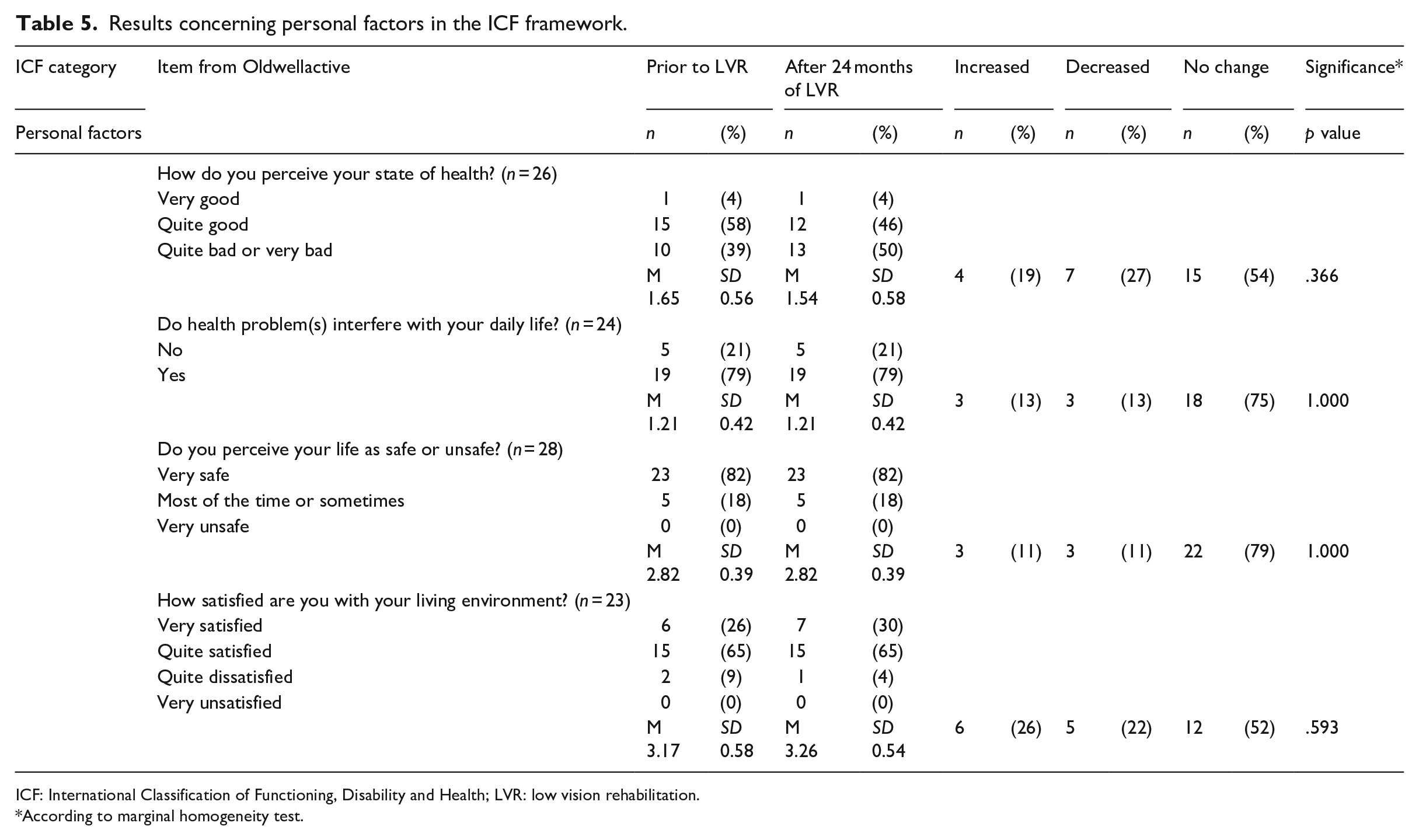
ICF: International Classification of Functioning, Disability and Health; LVR: low vision rehabilitation.
According to marginal homogeneity test.
Body functions and structures
Most of the participants did not have any sleeping problems either prior to (n = 16, 67%) or after 24 months of LVR (n = 20, 83%). After 24 months of LVR, half of the participants (50%, n = 13) felt their memory was weakened at least sometimes. The proportion of participants who were afraid of accidents (n = 12, 46%) rose slightly, as only 35% (n = 9) of the participants had been afraid of falling or having some other accident at home prior to the LVR. Furthermore, being afraid of falling, or experiencing some other accident while moving outdoors, also rose slightly, from 46% (n = 12) to 50% (n = 13), after 24 months of LVR. The same proportion of participants, 46% (n = 11), reported feeling depression, anxiety, or hopelessness prior to and after 24 months of LVR. Prior to LVR, more than half of the participants (57%, n = 16) reported not suffering from loneliness, while this proportion fell to 39% (n = 11) after 24 months of LVR, with 57% (n = 16) reporting that they suffered from loneliness a little bit. Thus, more of the participants suffered from loneliness after 24 months of LVR than prior to this LVR. More detailed results for this ICF category are presented in Table 2.
Activities and participation
In this study, the most pronounced effects of 24 months of LVR were found in the category of activities and participation, more specifically, going outdoors (p = .011), washing oneself (p = .016), taking care of personal hygiene (p = .046), dressing (p = .034), preparing meals (p = .041), and doing heavy housework (p = .046). All these tasks showed a negative change over the 24-month LVR period.
An identical number of participants reported being satisfied with their financial situation (n = 20, 87%) both prior to and after LVR. At both time points, one half (54%, n = 13) of the participants responded that they did not have any difficulties learning new things or skills. Furthermore, 18% (n = 5) of the participants were able to think clearly and felt that their memory functioned well after 24 months, which can be compared to only 7% (n = 2) at the start of LVR.
Prior to LVR, 65% (n = 17) of the participants reported that they can go outdoors. After 24 months of LVR, only 35% (n = 9) reported that they can go outdoors without the assistance of another person. Furthermore, 11 (42%) participants reported that going outdoors had become more difficult (p = .011). Prior to LVR, 20% (n = 5) of the participants reported needing help when washing themselves (bathing or showering), with this proportion rising to 48% (n = 12) effects after 24 months of LVR. Some of the participants also reported that taking care of personal hygiene had become more difficult over the course of LVR. For example, the proportion of participants who reported that they can independently take care of personal hygiene fell from 76% (n = 19) at the start of LVR to 48% (n = 12) after 24 months of LVR. Almost all the participants were able to independently use the toilet both before (92%, n = 23) and after LVR (96%, n = 24). A higher proportion of the participants reported problems dressing themselves after 24 months of LVR (36%, n = 9) than before the LVR (16%, n = 4), with 20% specifically reporting that they find it more difficult to dress themselves after 24 months of LVR. Detailed results for this category are presented in Table 3.
Environmental factors
Most of the participants (62%, n = 16) reported that they were not part of any regularly meeting group of people. After 24 months of LVR, only 18% (n = 5) of the participants reported not receiving any services or help, which was significantly less (36%, p = .025) than what was reported prior to LVR. Every participant reported that they had at least somebody who they can ask for help, but 41% (n = 11) reported either almost sufficient or insufficient social support after the LVR had lasted 24 months. Almost all the participants (96%, n = 22) were at least satisfied with their living environment. Detailed results for this category are presented in Table 4.
Personal factors
The participants reported varying evaluations of their wellness. Although the numbers between onset and 24-month follow-up were almost the same, 19% (n = 4) reported that they experienced their health better, and 27% (n = 7) reported decline. Half of the participants (54%, n = 15) reported their health unchanged during the 24-month LVR period. The participants reported their life to be safe (82%, n = 23) throughout the follow-up. Detailed results for this category are presented in Table 5.
Discussion
According to previous studies, VI is a disability that affects almost every aspect of everyday life (Leissner et al., 2014; Nollett et al., 2019). It is also undeniable that aging reduces functional ability (Storeng et al., 2018). At the end of the 2-year LVR period covered in this study, eight items had significantly decreased relative to baseline scores. Six of these items are connected to ADL functions and, as such, the presented results support what has been reported in earlier studies (Nollett et al., 2019). It is important to notice that a substantial share of these negative changes were in items within the activities and participation category, which had been defined according to the ICF framework. This provides valuable insight to LVR providers, that is, interventions should focus on maintaining the functional ability of older adults to maintain the quality of life among older adults with VI. In this age group, the best outcome may be maintenance of function – even in people without VI. Since VI presents an extra challenge for maintaining functional ability – in addition to the many other potentially emerging age-related health problems – the expected effect of LVR must be remembered to be limited and the overall ability to be dependent on several aspects also. In addition to functional ability, it should be paid attention to mental well-being.
Previous studies suggest that VI is associated with depression, anxiety, and social isolation (Evans et al., 2007; van der Aa et al., 2015). The results of this study concur with this earlier research, as participants reported suffering from loneliness more often at the end of LVR than they did before the LVR began, for example, timewise closer to the time before they became visually impaired. Almost half of the participants also reported depression, anxiety, or hopelessness both prior to and following LVR. It is important to note that loneliness is common among older adults (Savikko et al., 2019), and VI can aggravate the problem by making social situations more difficult to manage. Because VI carries an increased risk of loneliness, individual LVR should concentrate on preventing unwanted social isolation. This is also an important issue for social and healthcare professionals who work with older adults with VI.
Sleep problems are fairly common among older adults, as the biological process of aging affects the structure and quality of sleep (Talaslahti et al., 2012). In this study, however, only a few of the participants reported sleep problems after the 24-month LVR period. In addition to this, an interesting result was that, the majority of participants self-assessed their memory functions and ability to think clearly as very good or good after 24 months of LVR. Memory could be trained more than usual in the everyday of someone with VI because remembering things compensates for missing visual ability. Heyl and Wahl (2012) state that older adults with VI experience the importance of cognitive resources as better everyday functioning. Similar results were obtained in this study. The results in this study – which are solely based on self-estimation – are interesting as they disagree with Yu and Woo (2019) who identified subjective memory complaints among older adults with VI. Hence, LVR for older adults with VI should encourage them to actively use their memory, for example, by learning new skills and to train with leisure activities such as playing games perhaps and have new hobbies. Even practicing the use of visual aids and solving VI-related problems may challenge the cognitive capacity in a positive way and serve this purpose to some extent.
VI is a major factor in reducing social participation (Mick et al., 2018). There was dispersion in the answers relating to hobbies and participating in group activities on a regular basis. A clear majority (62%, n = 16) never participated in hobbies or groups outside their home, with only one-fifth (19%, n = 5) participating in these types of activities daily or weekly. Technology could help, for example, using a different kind of telerehabilitation solutions might provide a solution to introduce new activities into the lives of people with VI. There are also various assistive technologies that people with VI can use without major challenges (Kim, 2018). As such, there is a clear need for telerehabilitation interventions that can help older adults with VI participate in social group activities. However, this is an ambitious goal, and maybe more relevant for the generations born later than the participants of this study as they already are more familiar with computers and mobile devices.
In this study, the participants reported slightly worse experienced health and slight decreases in pains or aches after 24 months of LVR. These results may be related to some other medical condition which was not clarified in this study. The results also show that VI, although not paralyzing, is a disability that clearly restricts older adults from participating in group activities (Alma et al., 2012). In many fields, participants rated they self-reported results better in 24 months after the onset of the LVR. These findings did not reach statistical significance, however.
Previous research has already shown that ICF is a suitable frame of reference for studying the functional ability of a visually impaired person (Leissner et al., 2014). As such, the presented results indicate that modern LVR may focus too much on the practical issues of living with visual problems, for example, assistive devices and home modifications such as lightning improvements. This might be because it is provided by rehabilitation counselors specialized to address challenges faced by people living with VI. However, the results presented in this article agree with suggestions from previous studies (Rudman et al., 2016; Siira et al., 2019a), that is, LVR should focus on helping older adults with VI participate in society. These parts of the LVR process could come after older adults with VI have adapted to living with VI and learned how to correctly use the visual aids and compensatory measures. The presented results provide clear evidence of how relevant the ICF framework is for social and healthcare professionals, as this approach can give a broad perspective of functional ability which identifies weaknesses and strengths in diverse categories. Modern LVR therefore requires even more multiprofessional and interdisciplinary approach and collaboration of health and social care, third sector actors, peers, relatives, and volunteers.
This study provides novel insight as the functional ability of older adults with VI has not previously been examined over a 24-month LVR period using the ICF framework. This study also clarifies why older adults with VI need LVR, for example, so that they can learn to manage everyday life with VI and maintain their comprehensive functional ability. Future research should further address the functional ability of older adults with VI, and apply study designs which can clarify on which components of functional ability VI has the most impact. Research comparing the functional abilities of older adults with and without VI is needed.
Reliability
The mean age of the participants was fairly high, which is typical for the Finnish population of people affected by VI (Ojamo, 2018). Hence, although the sample was relatively small, it can be considered representative. After 24 months of LVR, 72% of the original participants remained in the study group. The other 28% had passed away (n = 5), canceled their consent (n = 2), could not be reached for further research (n = 1), or no longer fulfilled the inclusion criteria, for example, had moved into a care home or other medical reason (n = 3). It should be noted that the long follow-up period included in this study further increased the reliability of the reported results.
In addition to VI, all the participants had some other medical condition(s) which also affected their ability to manage home life, participation in social life, and needs for help. However, due to certain constraints, these additional ailments had to be ignored in the present research. It can be expected that as people age, their ability to function deteriorates, and that all change identified in this study does not result from VI.
The instrument used in the study, “Oldwellactive,” was specifically developed for older adults and it has been tested and validated. Oldwellactive has internal consistency from 0.71 to 0.92 (Koistinen et al., 2012). The age of participants was considered in interview situations, and the same researcher performed all the interviews. There is no simple explanation as to why some of the items had lower response rates, but it was noticed that some of the participants found the interview burdensome and did not have the strength to answer all the items. This may have weakened the reliability of the results, and, for this reason, the number of answers for every item is specified in the presented tables. The items chosen for the study were linked to ICF codes using a previously published approach (Cieza et al., 2005), and good scientific practice was followed throughout the study. It should be noted that the participants who were lost to follow-up may be those who fared even worse which would mean that the percentages presented after 24 months greatly underestimate the decline.
Conclusion
VI is a potentially isolating disease. The results of this study emphasize that this condition reduces social participation and increases the need for external help as well as feelings of loneliness and social isolation. Therefore, LVR designed for older adults should not only focus on traditional visual aids but also promote participation in social activities and staying active. This will ensure that older adults with VI can better maintain their functional ability, both in terms of life satisfaction and general health.