
Abstract
For patients to enjoy the benefits of vision impairment registration, they need to be certified by an ophthalmologist. There have been concerns about barriers and a lack of awareness of benefits and certification criteria among ophthalmologists leading to under-registration. The purpose of this study was to gain insight into the certification process in terms of potential barriers, clinical decision-making, and understanding of current guidelines and registration benefits.
Ophthalmologists completed a survey on understanding registration benefits and barriers for certification (n = 22) and a survey on clinical decision-making in certification (n = 21). Furthermore, visual function and registration data were collected at a hospital Low Vision Clinic in Edinburgh from all new referrals (n = 89) over a 4-month period from August to November 2020. Our study showed that the main barriers for vision impairment certification were insufficient awareness of registration benefits, uncertainty of when to certify, and a lack of time in clinic. Ophthalmologists were more confident about certification of ocular versus neurological visual impairment. In terms of clinical decision-making, the ophthalmologists’ survey placed most importance on visual-field assessments, followed by visual acuity. Very little importance was placed on contrast sensitivity. Our findings suggest that ophthalmologists would benefit from more education into the benefits of registration and more guidance when registering patients with neurological conditions affecting functional vision in particular. It may be beneficial to highlight the role of contrast sensitivity during the certification process to ophthalmologists.
Keywords
Background
England and Scotland introduced new forms for certification of sight impairment (SI) and severe sight impairment (SSI) in 2017 and 2018, respectively (Public Health Scotland 2020; Royal National Institute for Blind people [RNIB], 2017; Scottish Government, 2017). The new CVI (Certificate of Vision Impairment) Scotland form replaces the BP1 form that was formerly used to formally certify someone as partially sighted (now SI) or blind (now SSI). In England, the new CVI form now combines registration for adults and children into one form (Department of Health and Social Care, 2018). This study took place in Scotland; therefore, the Scottish CVI form is now explained. In contrast to England, children are not considered for certification until they reach 16 years of age. Children are supported through the Visual Impairment Network for Children and Young People (VINCYP, n.d.). More information, including the registration criteria for VINCYP can be accessed on their website. The CVI Scotland form and ‘Explanatory notes for consultant ophthalmologists and hospital eye clinic staff’ concern the certification of SI and SSI of adults from the age of 16. The new form and explanatory notes were introduced to improve consistency and to address the issue of perceived under-registration after consultation with a number of stakeholders (Public Health Scotland, 2020; RNIB, 2013). Consistency in terms of when to certify varies between studies (Bartlett et al., 2021; Guerin et al., 2014). The explanatory notes provide guidance for certification in terms of visual acuity (VA) and visual field impairment (see Table 1). The notes also state that the definitions in the explanatory notes ‘. . . are used as a guide, and judgement may be required regarding a patient’s level of disability based on other visual parameters, e.g., for diagnoses such as functional visual blindness, blepharospasm, and oculo-motor apraxia’ (Scottish Government, n.d.). The CVI form defines SSI as ‘so blind that they cannot do any work for which eyesight is essential’. There is no legal definition for SI. The process of certification and registration is now explained.
Guidelines for certification for England and Scotland (Department of health 2017; RNIB, 2017; Scottish Government, n.d.).

The first step in the process of certification involves clinical decision-making whereby the consultant ophthalmologist decides whether a patient meets the criteria for certification. After completing and signing the CVI form, the patient is formally certified as SI/SSI. Patients now have a choice to be added to the register of sight impaired people, held by the local authority (or the agency acting on their behalf). The patient receives a certificate of registration once the local authority has processed the CVI form and updated the register. The certificate entitles patients to a number of benefits and concessions, including travel and TV licence. Registered patients are assessed by social care as per national standards (National Health Service [NHS], 2007) with a view to address support needs and to promote independent living, for example, through mobility training or emotional support. Registration also informs local councils about the need for improving accessibility of public spaces.
The purpose of this study was to gain insight into the certification process in terms of potential barriers, clinical decision-making and understanding of current guidelines and registration benefits by obtaining ophthalmologists’ views and by obtaining data about visual functions and registration status of patients attending the Low Vision Clinic at the Princess Alexandra Eye Pavilion (PAEP) in Edinburgh.
Methods
Data about age, gender, eye conditions, registration status, distance vision, contrast sensitivity, and visual fields were collected over a 4-month period from August to November 2020 from all new referrals (n = 89) to the Low Vision Clinic at the PAEP. The data were initially collected as part of a wider service evaluation for the Low Vision Clinic (Tooth, 2021). Distance vision was recorded in LogMAR scores. Registration status was recorded as the current registration or the registration immediately following the clinic visit. Contrast sensitivity was measured using the Mars contrast sensitivity test and recorded as a LogMAR score and a measure of severity. Any recent visual field data were considered for inclusion for this study but the dataset was too small to perform meaningful analysis. Data were analysed using a software package (SPSS Version 26).
Furthermore, two surveys were carried out among ophthalmologists in November 2021. The surveys were conducted using Survey Monkey. All ophthalmologists (n = 44) working at the PAEP were invited to take part. The grades of the ophthalmologists’ surveyed ranged from junior trainee to consultant level. Two-thirds of the staff surveyed were consultant level. A total of 22 ophthalmologists completed the survey about understanding registration benefits and barriers for certification. Respondents were asked what barriers for discussing certification applied to them and how well they understood the guidelines for certification, the process of registration and the benefits of registration. They were also asked how confident they felt about certifying patients with ocular versus neurological sight loss. Twenty-one ophthalmologists completed the survey about clinical decision-making in which they were asked which visual functions and other factors they assess and consider relevant for certification.
Ethical approval was obtained from the local health board (NHS Lothian) quality improvement and audit committee.
Results
Demographics
Of the 89 patients included in the audit, 62% were female. The age of patients attending the Low Vision Clinic ranged from 8 to 102 years (mean ± SD 72.47 ± 21.98). The majority of patients were elderly with 50.6% older than 80 and 29.2% between 65 and 80 years old. People of working age (16–65 years) represented 14.6%, and 5.6% were children. The commonest primary eye condition was age-related macular degeneration (AMD) (57.3%), followed by retinal/vascular disease (11.2%), glaucoma (9.0%), neurological vision impairment (10.1%), diabetic eye disease (6.7%), and ‘other’ (5.6%).
Registration status
In the hospital surveyed, information about registration status is held by the local authority rather than by the hospital. It is up to the clinician to record this information in the paper notes. It is assumed that figures for certification and registration are equal as all patients consented to be included in the register after certification. Registration status of patients attending the low vision service was documented in 76 case notes, and of these 76 patients 32% were registered as SI and 29% as SSI. About 6% were children and 33% were unregistered adults. The commonest cause for SI and SSI registration was AMD with 46% and 65%, respectively. Retinal and vascular conditions were recorded as the primary condition in 14% of SI and 17% of SSI registrations. Neurological conditions were recorded in 11% of SI and 9% of SSI registrations. Diabetic eye disease was recorded in 11% of SI registrations and glaucoma was recorded in 7% of SI and 4% of SSI registrations. About 70% of unregistered patients had AMD.
Perceived barriers for offering certification
In the survey, ophthalmologists were asked what barriers for offering or discussing certification for SI or SSI applied to them. While 41% indicated that they experienced no barriers at all, the majority of ophthalmologists did experience barriers. Figure 1 shows the responses from the survey.
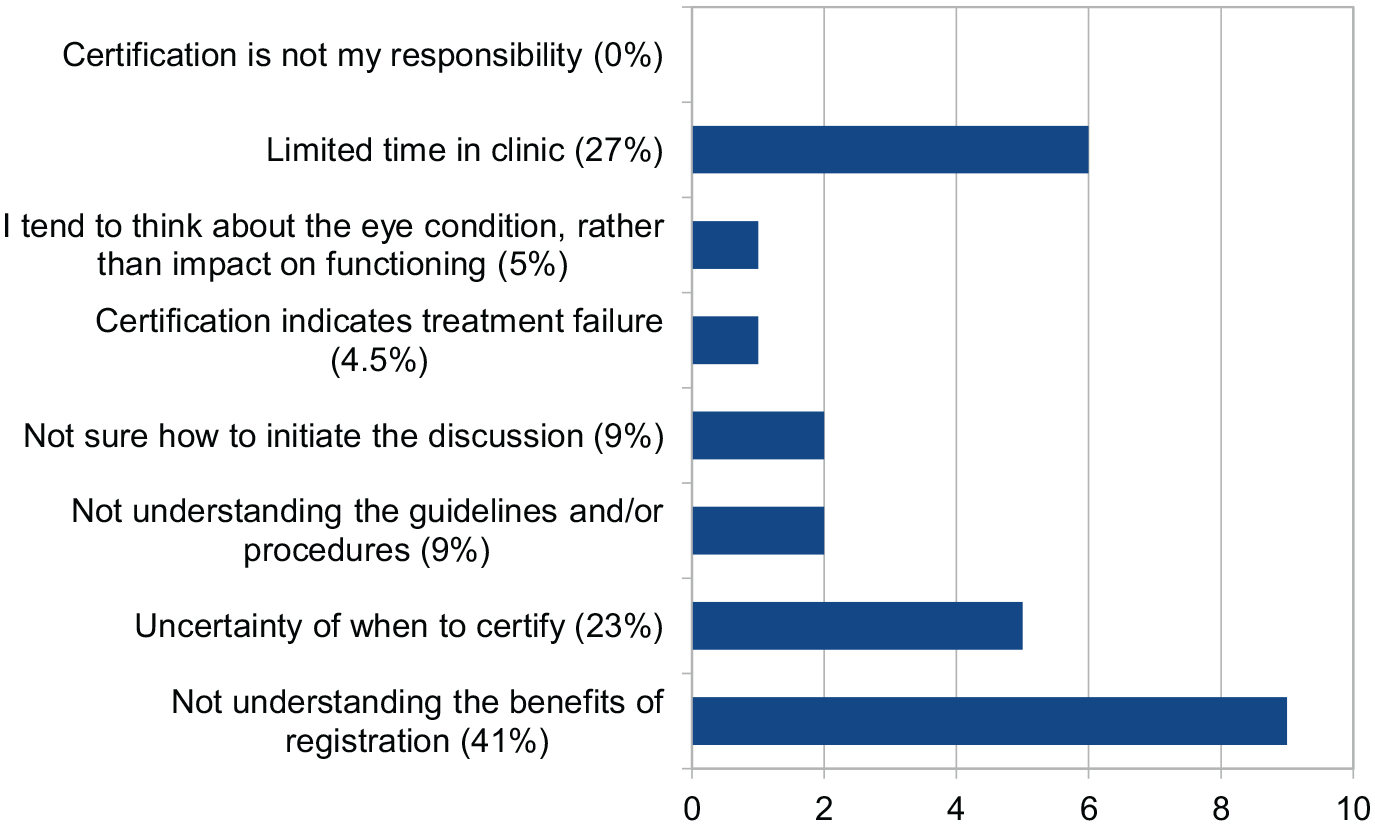
Barriers for discussing certification for SI/SSI as perceived by survey respondents. Additional barriers, from the ‘other’ category were lack of availability of CVI forms in clinic rooms and unwillingness of patients to accept help. It was also suggested by one respondent that ‘some patients would benefit from certification due to other physical problems when they are borderline for certification’.
Benefits of registration
Around 86% (n = 19) of ophthalmologists indicated that they explain the benefits of registration to their patients. Of those, 2 respondents indicated they had a good knowledge of the benefits, 10 had a fair knowledge, and 7 had minimal knowledge. Around 14% of ophthalmologists (n = 3) indicated that they do not discuss benefits with their patients.
Confidence in certification guidelines
Figure 2 shows how confident ophthalmologists (n = 22) felt about their understanding of the guidelines for certification and about certifying patients with ocular versus neurological visual impairment.
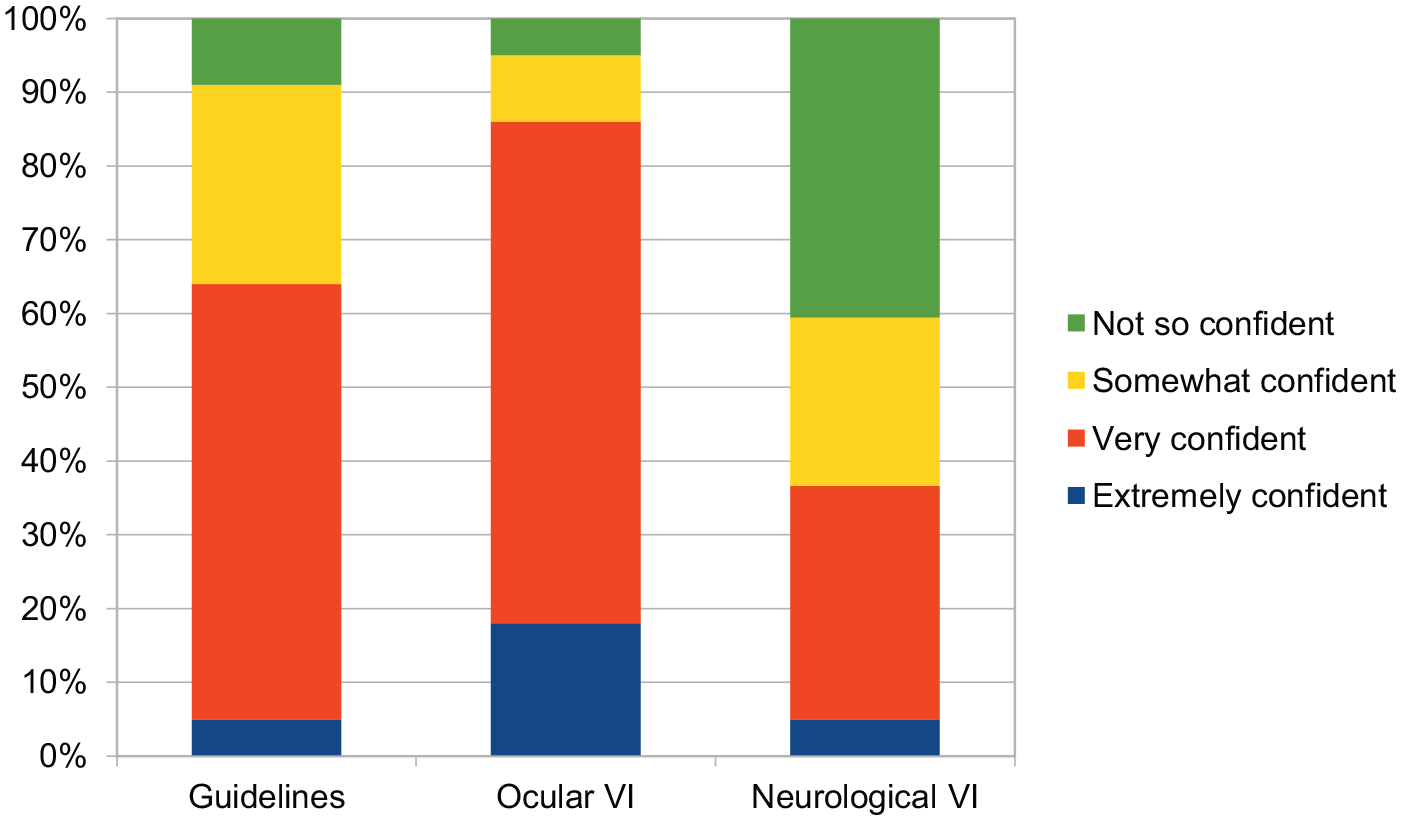
Responses to the questions: ‘How confident do you feel that you understand the guidelines for certifying patients for sight impairment?’, ‘Would you be confident to certify a patient with ocular vision impairment’, and ‘Would you be confident to certify a patient with neurological vision impairment (e.g., visual processing impairments)?’.
Timing of registration
Ophthalmologists were asked when is a good time to discuss or offer certification for vision impairment. Around 86% (n = 19) would consider certification when the patient is eligible and 64% (n = 14) would consider this when the patient asks for it. One respondent (5%) would wait until the end of treatment is reached, one respondent indicated that ‘it does not spring to mind’ to offer certification and one respondent would wait until the patient had ‘emotionally adjusted to visual loss’.
Registration status check
Two-thirds of respondents indicated that they usually or always check the registration status of patients attending the ophthalmology clinics.
Visual acuity
Ophthalmologists were asked when they would consider SI or SSI certification based on patients’ VA. For SI, 52% of respondents indicated that they would consider certification with any VA, depending on visual fields. The VA cut-off values (Snellen) from the other 48% ranged from 6/18 to 6/60 or worse. For SSI, 24% indicated that they would consider certification with any VA, depending on visual fields. The VA cut-off values from the other 76% ranged from 6/30 to 6/120 or worse.
Distance vision was measured in 86 patients attending the Low Vision Clinic during the audit period in 2020. LogMAR vision was measured in 95% (n = 82). LogMAR vision was not available in four cases. Two of these had a record of Snellen vision and two patients had ‘hand movement’. Snellen vision was converted into LogMAR scores and ‘hand movement’ was recorded as 3.00 LogMAR for the purpose of completing the dataset. Vision was measured with the habitual spectacle prescription. For patients without up-to-date spectacles, vision was measured after refraction. Around 15% (n = 13) had a vision of 6/12 or better (i.e., would meet vision driving standards based on VA alone), 63% (n = 54) had a vision between 6/12 and 6/60 (i.e., low vision, but not eligible for registration based on VA alone) and 22% (n = 19) had a vision of 6/60 or worse (i.e., visual impairment eligible for registration based on VA alone).
To relate VA measures to registration status, LogMAR distance acuity data were analysed for each group. The median (±IQR [interquartile range]) LogMAR acuity for the non-registered patients was 0.52 (±0.47). For the SI group, this was 0.70 (=/−0.44), for the SSI group 1.18 (±0.51) and for the VINCYP group 0.60 (±0.44); see Figure 3.

Box-plot showing LogMAR acuity in patients per group. The x-axis denotes the registration status in each group. The y-axis shows the LogMAR acuity scores.
Contrast sensitivity
Sixteen (76%) ophthalmologists indicated that they never assess contrast sensitivity. Four ophthalmologists (19%) rarely assess this and one (5%) sometimes assesses this function. Around 26% of patients (n = 23) attending the Low Vision Clinic had their contrast sensitivity measured (see Figure 4). For the SSI group, the average LogMAR score was 0.66. The average LogMAR scores for SI, VINCYP, unregistered, and unknown registration status groups were 0.94, 1.20, 1.23, and 1.00, respectively.
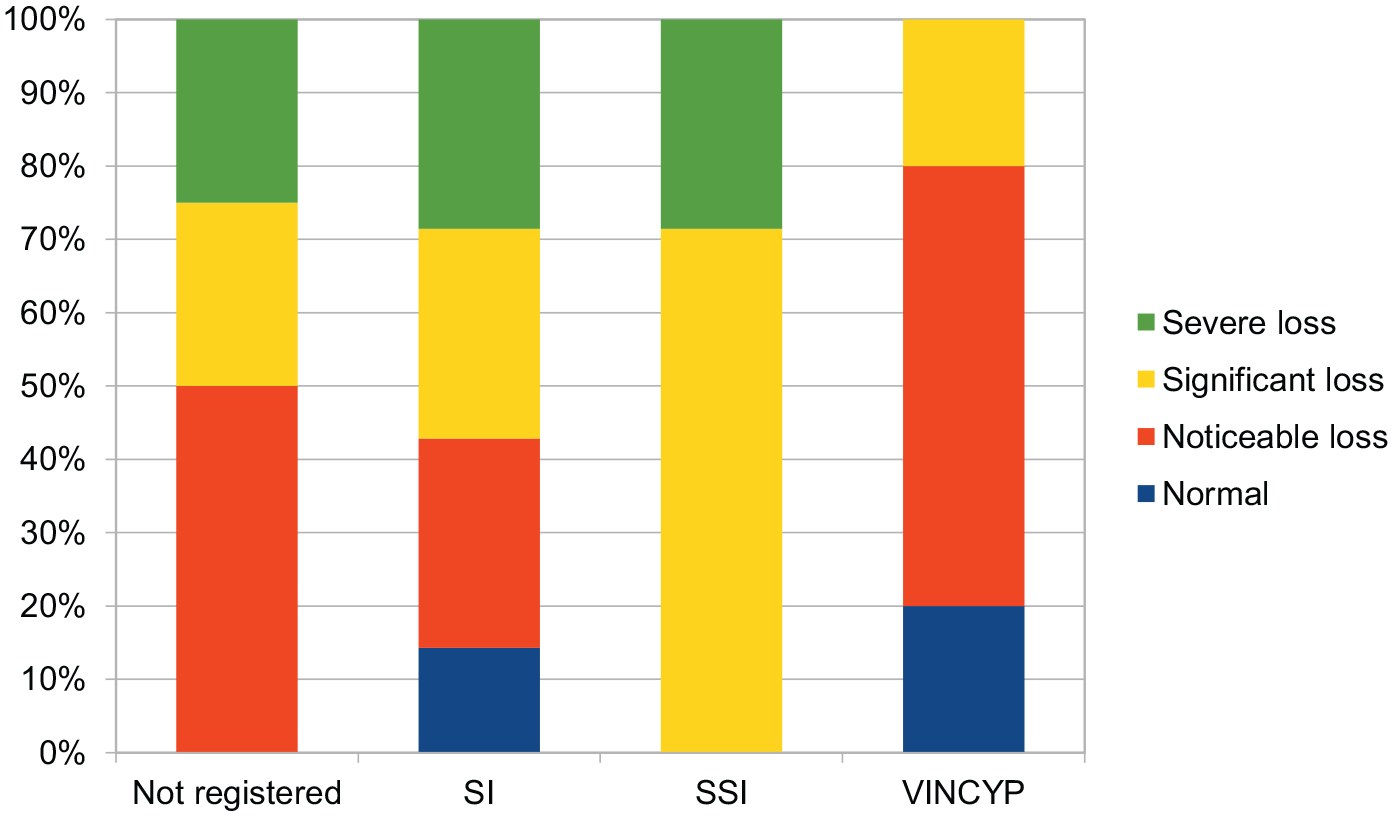
Bar graph showing Mars contrast sensitivity scores per group. The x-axis denotes the registration status in each group. Contrast sensitivity data were available for 23 patients. The y-axis shows the number of patients for each degree of contrast sensitivity. A score of 0–0.48 LogMAR is considered severe loss, 0.52–1.00 is considered significant loss, 1.04–1.48 is considered noticeable loss, and 1.52–1.76 is considered normal.
Visual fields
Seven ophthalmologists (33%) indicated that they always assess visual fields when they consider SI or SSI certification. Nine (43%) respondents indicated that they usually assess this function with four ophthalmologists (19%) sometimes, and one (5%) ophthalmologist rarely assessing this. Ophthalmologists were asked which visual field impairments they would consider significant in the context of certification. There was agreement among respondents that central scotoma (90%), tunnel vision (95%), hemianopia (90%), and lower field impairments (90%) were significant indicators when considering certification. Quadrantanopia (48%), patchy field loss (24%), and simultanagnosia (19%) were considered relevant by a minority of ophthalmologists.
Visual field data were available for nine patients (10%) attending the Low Vision Clinic. This included data from previous visits to the ophthalmology clinic. Of note is one glaucoma patient with tunnel vision and good VA (0.18 LogMAR) who was registered as SI. There was also one patient with central scotoma and significant contrast sensitivity loss who was not considered for certification.
Perceived relevance of visual functions
VA was considered to be a somewhat important factor when considering certification by the majority (57%). Around 5% rated this factor extremely important and 38% rated it very important. On the whole, visual fields were considered more important than VA with 52% considering it extremely important, 43% considering it very important and 5% rating it somewhat important. Contrast sensitivity was considered much less important with 33% rating it not so important, 43% rating it somewhat important, and 14% rating it very important.
Quality of life and co-morbidities
Most ophthalmologists (57%) indicated that they always ask patients about functioning and quality of life (QoL), with a further 19% usually assessing this and 24% sometimes assessing this. Respondents were asked if they would take other health issues into account when considering certification. Around 15% indicated that they always consider this, 24% usually, 48% sometimes, 10% rarely, and 5% never consider this.
Discussion
One-third of all registered patients (SI and SSI combined) had VA of 6/60 Snellen (or 1.00 LogMAR) or worse. The remaining two-thirds of registered patients had a vision better than 6/60. These figures show that in at least two-thirds of certifications, the decision to certify was based on a combination of factors, which is in keeping with the explanatory notes for consultant ophthalmologists and hospital eye clinic staff in Scotland (Scottish Government,n.d.). This study has shown that there is a wide range of VA measurements within each registration category. The survey also showed that there was no consensus regarding VA cut-off value and ophthalmologists stated that other factors play a role in decision-making. Compared to a consensus panel from a study by Bartlett et al. (2021), the consistency in terms of VA is lower in our sample and there was a trend for patients to be registered as SI and SSI with higher VA measurements. Due to the incomplete dataset for other factors, such as contrast sensitivity, colour vision, and visual fields and functional vision, one cannot draw firm conclusions as to what other factors were taken into account at the point of certification.
The survey showed that ophthalmologists particularly value visual fields as a guide for certification. Central scotoma, hemianopia, tunnel vision, and lower field impairments were considered most important. Patchy fields, quandrantanopia, and simultanagnosia were considered important by a minority of respondents. The guidance explicitly mentions all field defects except quadrantanopia and simultanagnosia. ‘Cloudy, blurry, superior or patchy’ central fields are considered relevant in the guidance (Department of Health, 2017; RNIB, 2017). One could argue that simultanagnosia can be similar to tunnel vision in terms of functional vision and is, therefore, relevant for certification. Quadrantanopia has an impact on functional vision as well, which renders it relevant for certification.
Although the majority of ophthalmologists stated that they would usually assess visual fields as part of the certification process, this was not consistently documented in the case notes. It is possible that a relative or absolute central scotoma was assumed in patients with moderate to severe macular degeneration based on the fundus appearance and optical coherence tomography (OCT) without a formal field test. Impaired visual fields are known to affect mobility (Miyasike-daSilva et al., 2019; Peli et al., 2016; Subhi et al., 2020), reading speed and text navigation (Kanonidou, 2011; Schuett et al., 2008), face recognition (Glen et al., 2013; Logan et al., 2020), and visual search (Bouwmeester et al., 2007; Kasneci et al., 2017).
Interestingly, the explanatory notes for England and Scotland do not mention contrast sensitivity despite the fact that this may even be a stronger indicator than VA and visual fields for reduced functioning and QoL (Alahmadi et al., 2018; Bennett et al., 2019; Johansson et al., 2020; Roh et al., 2018). One could argue that ‘blurry or cloudy’ vision describes impaired contrast sensitivity in the English notes. The Scottish notes only mention media opacities. Impaired contrast sensitivity affects mobility (Duggan et al., 2017; Leat and Lovie-Kitchin, 2008), reading speed and text navigation (Brussee et al., 2018; Leat & Woodhouse, 1993), face recognition (McCulloch et al., 2011), and driving (Owsley et al., 2001; Spreng et al., 2018). Ophthalmologists do not seem to value the importance of contrast sensitivity as much as the other visual functions and it is rarely assessed in ophthalmology clinics. One could argue whether contrast sensitivity should be included in the guidelines for certification and contrast sensitivity should be assessed as part of an assessment for certification. This assessment may be better carried out in a Low Vision Clinic, in which contrast sensitivity is measured and functional vision is assessed in greater detail. In our Low Vision Clinic, more training is required into the role of contrast sensitivity assessment as only a quarter of patients were assessed for this within the audit period.
Ophthalmologists generally discuss QoL and functioning with their patients, which is ultimately what certification should be based on. Other health issues are taken into account when considering patients for certification by a number of respondents. It appears from the survey that ophthalmologists promote timely certification. The majority also stated that they would check eligibility. It was not clear whether this was done at every clinic visit or only done when certification was discussed during the clinic visit. In the author’s experience, however, many patients attending the Low Vision Clinic stated having wished they had been offered support and certification at a much earlier stage. As this audit was a retrospective audit of the Low Vision Clinic rather than a general ophthalmology clinic, there are no data available about the percentage of patients attending ophthalmology clinics who would have benefitted from registration but were not offered certification or a referral to low vision services. Therefore, although ophthalmologists promote early certification, no conclusions can be drawn about their actual practice.
The survey indicated that ophthalmologists are more confident when considering certification in patients with ocular conditions compared to neurological conditions. In the United Kingdom, the leading cause of visual impairment in children is now cerebral visual impairment (Mitry et al., 2013; Rahi & Cable, 2003). They are considered for registration from the age of 16. This group of patients, as well as adults with acquired brain injury such as stroke, dementia, and brain tumours would benefit from specific certification guidelines for ophthalmologists to support their decision-making.
The survey showed that the level of knowledge about benefits of registration is variable among ophthalmologists. Knowledge about the benefits of registration appeared to be the main barrier for discussing certification along with limited time in clinic. Patients could be advised to discuss benefits in more detail with the Patient Support Officer to address these issues. Patient Support officers or Eye Clinic Liaison Officers are usually hospital based and provide a link between the hospital eye staff and rehabilitation and social services. Contrary to earlier findings (Barry & Murray, 2005; RNIB, 2013), this study showed that ophthalmologists did not intend to wait until the end of treatment was reached and did not perceive certification as a sign of treatment failure. No data were collected about the actual time patients had been eligible for registration before they were offered certification by an ophthalmologist.
Limitations
The audit data were collected in a Low Vision clinic in which vision impairment registration is addressed as part of the assessment. Certification takes place at all ophthalmology clinics, although less time is available in most clinics to address this. Therefore, these data may not be a true representation of the patient group as a whole. It is possible that a number of patients are not considered for certification or for referral to low vision services when they would have benefitted from this. This study looked at self-reported practice and opinions from ophthalmologists. While the ophthalmologists were in favour of early intervention, a further study is required to reveal whether this is a reflection of what actually happens in practice. Are patients offered certification at the right time? Are they referred to low vision services at an early stage? How satisfied are patients with the certification procedure and timing of interventions? This study did not address the role of colour vision impairment as this was rarely assessed in the Low Vision Clinic, despite the fact that colour vision is often impaired in conditions such as AMD, other retinal and neurological conditions and impacts on functional vision (Stoianov et al., 2018).
Conclusion
Overall, from our study, it appears that ophthalmologists are keen to provide optimal care and support for their patients by offering certification when they are eligible or when patients ask about registration, and they do not intend to wait until the end of treatment is reached before doing so. Waiting until the end of treatment and a perception that certification indicates treatment failure have previously been identified as barriers for certification (Barry & Murray, 2005; RNIB, 2013), and it is possible that ophthalmologists delay certification despite their good intention on some occasions. Although patient support services are well placed to provide information about registration benefits and can allow more time for patients to ask questions, we have shown that knowledge among ophthalmologists about these benefits is variable and could be improved. Furthermore, our study suggests that it may be beneficial for ophthalmologists to receive more training about certification in patients with neurological visual impairment and also guidance about the role of contrast sensitivity in this process. However, one needs to bear in mind that this was a small scale study, and a larger scale and more in depth study is needed to explore these findings further.