
Abstract
Low vision is a condition of visual impairment, generated by an underlying pathology that affects visual functioning and the development of daily activities. In the field of visual impairment, the developments in the analysis of access to rehabilitation services are scarce and incipient. The study approaches the understanding of the experiences of people with low vision in Medellín, Colombia, in their search for visual rehabilitation services. Ethnographic collective case study was conducted. Intersectionality was adopted to explore people’s experiences with low vision management health services. Five women and four men with low vision who attended the healthcare center participated in the study. Twenty-nine interviews and 16 participant observation exercises were carried out. Three categories emerged in the study: (1) I had never heard of low vision services; (2) Interaction with the health system: A path of struggles; and (3) Barriers that are exacerbated by the intersection of multiple identities and systems of oppression. The Colombian health system acts as an axis of structural oppression that interacts with the economic condition, educational level, and geographical location to generate greater difficulties for the identification of low vision management options, which also interact with the multiple and dynamic identities of each subject.
Keywords
Introduction
Low vision is a condition of visual impairment, generated by an underlying pathology that affects visual functioning and the development of daily activities (Burton et al., 2021; World Health Organization, 2019). By 2020, 295 million people with low vision were reported, representing 3.74% of the world population (Steinmetz et al., 2021). In Colombia, the 2018 national census reported a preliminary national disability prevalence of 7.1% and difficulties of the type of not seeing up close, far, or around constitute 18.7% (Instituto Nacional para Ciegos, 2020). For the specific case of Medellín, without more recent figures, by 2005, 3965 people with visual disabilities were reported (Departamento Administrativo Nacional de Estadística, 2006).
Low vision requires a health intervention process that addresses health needs regarding diagnosis, treatment, rehabilitation, and follow-up. The phases of health care for this group involve the ocular and visual evaluation by ophthalmologists and optometrists to define the patient’s condition and prescribe the necessary devices for the use of their vision remnant. Then, the functional rehabilitation process by health institutions provides people with different techniques, strategies, and resources that allow them to carry out daily activities and actively participate in any setting. It includes several services: orientation and mobility training, independent living skills training, counseling, psychological support, prescription, and assistive device training, all of which aim to enhance ongoing participation in well-being activities (van Nispen et al., 2020; World Health Organization, 2015).
Colombia‘s General System of Social Security in Health has public and private resources and is divided into two regimes: a contributory regime for those who can afford a monthly payment and a subsidized regime for the vulnerable population (Vargas et al., 2013). The system is administered by insurance companies that must guarantee access and quality of health care. Furthermore, people with paying capabilities can acquire additional private prepaid medical insurance services, to get a better healthcare experience. Due to its very structure, the health system has generated access barriers for different health conditions. It implies that users must use legal actions to demand healthcare interventions, even though sometimes de benefit plan includes those interventions. Therefore, in Colombia, litigation has become the structural element of democratic design, through which many people have had to fight to ensure access to medical care (Arrieta-gómez, 2018).
In 2015, the national Statutory Health Law established an important milestone: health was considered a fundamental right through the provision of services and technologies, based on a comprehensive concept of health (Ramírez Ramírez et al., 2016). This law sought to strengthen the service provision in a comprehensive manner and the expansion and unification of benefit plans regardless of the affiliation regime. For people with low vision, the benefit plan includes care for the diagnosis of eye disorders, general ophthalmological and optometric care, as well as specialized low vision evaluation which is carried out as a first step for the identification of the visual functioning profile; however, the subsequent stages are not clearly defined in the benefit plan: coverage of optical and non-optical devices and visual functional rehabilitation.
Despite the country’s progress in healthcare coverage and the “financial equity” promoted, the system has not solved equity problems, specifically in vulnerable groups such as people with disabilities (Hernández, 2002). We understand inequities because of social privileges and disadvantages. It influences people’s social position to shape their health and their power to use and demand quality health care (McCollum et al., 2019). Thus, we have considered the use of intersectionality as a lens to explore people’s experiences with low vision management health services, since it allows us to improve our understanding of inequality because it goes beyond the social hierarchies, either independently from each other or additively as it addresses social categories as mutually constituted and intersecting dynamically and interactively (Larson et al., 2016). Intersectionality is a theoretical-methodological perspective that seeks to identify how the intersection of social structures generates complex discrimination situations maintained and reproduced at structural, political, and discursive levels (La Barbera, 2017). This concept was proposed by Kimberlé Crenshaw (1991), who uses the metaphor of the crossroads and speaks of double, triple, and multiple discriminations (Crenshaw, 2015).
In the field of visual impairment, health research has assessed the prevalence of visual impairments, the management of eye disease. The developments in the analysis of access to rehabilitation services are scarce and incipient (Choi & Seo, 2021). Therefore, this study aims to contribute with elements for discussion in this area. Thus, the study approaches the understanding of the experiences of people with low vision in Medellín, Colombia, in their search for healthcare and rehabilitation services. For this manuscript, we are based on partial results of a broader ethnographic case study that focused on understanding the situated experience of people with low vision (Oviedo-Cáceres, 2021).
Methods
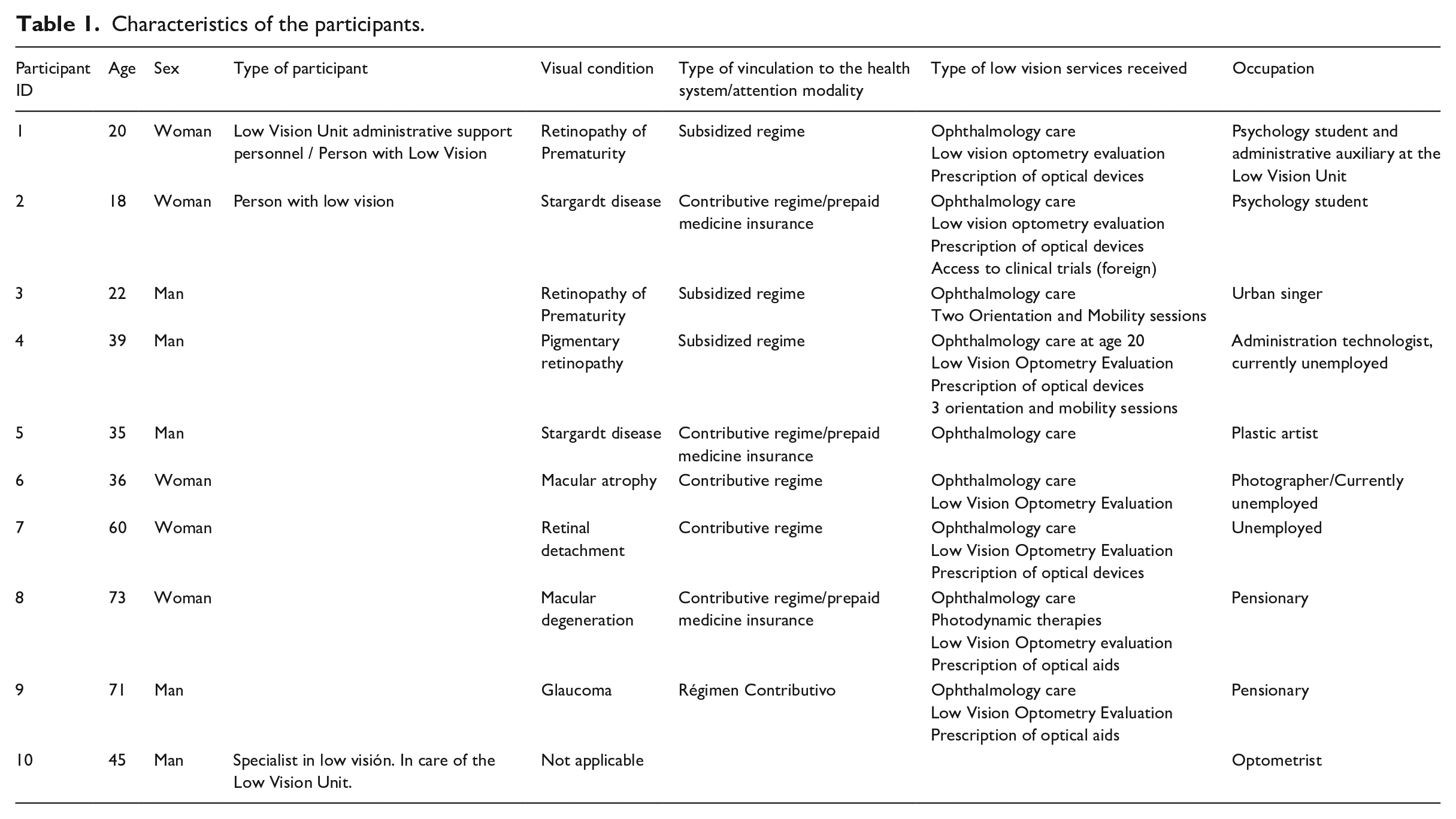
A collective case study (Simons, 2011; Stake, 1998) was carried out as an integrated system, composed of individual studies, meaning units of analysis, that share common characteristics. The interest is not focused on a specific case but a certain number of cases together (Stake, 1998). We took elements of the ethnographic method. Ethnographic case study differs per se from ethnographic research, which has traditionally involved prolonged immersion in the field. However, this does not detract from the depth and methodological rigor of ethnography (Simons, 2011). Intersectionality was adopted to explore people’s experiences with low vision management health services. For this, an intentional selection and sampling of extreme cases was carried out, given the interest to identify the different ways in which intersectionality shapes people’s experience (Martínez-Salgado, 2012). To select the cases, we considered that the experience of people with low vision is mediated, among other aspects, by gender and by the age at which the condition started. Thus, a man and a woman for each of the following groups were included: Youth (18–26 years old), adulthood (27–59 years old), and old age (over 60 years old), according to the assumed categorization life cycle. The research began with a group of six people, but the analysis and reflections that emerged from the work made it necessary to invite other participants to promote a greater understanding of the phenomenon, given the interest in the analysis of how the different axes of inequality intersect, generating diverse experiences. Thus, participants increased due to the snowball effect, using references from key informants and participants. So, participants from different contexts, social classes, educational levels, and types of health insurance were included (see Table 1).
Characteristics of the participants.
The research was carried out in Medellín, Colombia, specifically with people receiving visual rehabilitation processes in the Low Vision Unit of one of the two reference Ophthalmology Clinics that care for people with low vision in the city, which one of the most important high complexity ophthalmology clinic in Colombia. Following the COREQ checklist for reporting qualitative research, the research team has expertise in Public Health, Health Services, qualitative research, and Visual Impairment. The fieldwork and the interviews were carried out by the first author, an optometrist, academic, seeing woman, aspects that influenced the fieldwork and the approach to participants, specifically to men. During the fieldwork, the first author experience greater openness and closeness with the women, who were initially more willing to share aspects of their private life; the men showed a face of independence and control over their lives, to maintain the image of what a man is supposed to be in the context of a patriarchal society. However, with the course of the meetings, we managed to establish a relationship of trust.
Participants were contacted directly in the rehabilitation unit. Twenty-nine interviews were conducted with the 10 participants. Sixteen participant observation exercises were carried out, as well as an accompaniment to daily activities. All the interviews were recorded on a magnetic medium. Then, an identification code was assigned to each one.
The data analysis was carried out simultaneously with the information collection, so the emerging findings guided the following phases. The lead author analyzed each transcription, but the resulting codes and categories were refined through research team meetings for collective reflection, thus, expanding the possibilities for coding and analysis. The lead author maintained a reflective position throughout the analysis process to challenge assumptions and be open to multiple ways of “looking at” the data. Although the research team has no visual health problems, its members have worked with people with this condition. Each transcript and observation field note was individually coded, using low-level (open) and high-level (theoretical) coding to develop a rich understanding of the data, before comparing the codes between participants to form categories and topics. The team followed the moments proposed by Angrosino and Emerson (Angrosino, 2012; Emerson et al., 2011) for the information analysis process: descriptive analysis, identification of patterns, regularities, or emerging themes. Ethics approval for this study was provided by the CES University ethics committee (ID Project:824. Act number 160).
We used strategies to ensure the rigor and trustworthiness of the findings: peer debriefing discussions among the research team with the goal of airing biases and challenging assumptions throughout the data collection and analysis process; prolonged engagement and thick description using quotes that were reflective of the range of ideas expressed by the participants.
Findings
The following categories emerged in the study: (1) I had never heard of low vision services; (2) Interaction with the health system: A path of struggles; (3) Barriers that are exacerbated by the intersection of multiple identities and systems of oppression.
I had never heard of low vision services
An initial aspect is related to the difficulties experienced to get health care for their disability. It was not easy to find guidance on vision rehabilitation services, neither possibilities nor strategies for their management. Furthermore, many of them knew about this possibility long after their diagnosis, as if a veil of invisibility accompanies low vision. Low vision rehabilitation services were not mentioned; people were only informed of their ocular pathology but were not aware that it was generating a condition of visual impairment called low vision, nor that there was a specific care service for this condition. “I had never heard of low vision” was a frequently repeated phrase. The optometrists and ophthalmologists who attended them diagnosed their ocular condition, for example, glaucoma, macular degeneration, Stargardt’s disease, but did not mention low vision or visual impairment. “A retinologist saw me, he never spoke to me about low vision. I had no idea, there are many people who do not know low vision. If the specialists don’t give you the knowledge, how is one going to know?” [ID#7].
This scarce knowledge of low vision rehabilitation services is a repetitive aspect of their experiences, “If a person who has been in an ophthalmology process and a lot of other things, has not been referred to low vision is because something happens. I think that we have to train more ophthalmologists and optometrists” [ID#1]. “The low vision specialty does not have any advertising parameter. There is no institution, nor are there campaigns that tell people know what it is” [ID#2].
As the participants mentioned, very few institutions include this service. Medellín has only three health institutions that provide care for people with low vision. However, only one offers a comprehensive functional rehabilitation process. Another one makes diagnosis and prescription of optical devices, and finally, the institution of reference, where this research process was developed, makes the diagnosis process, prescription of devices, optical device tests, and designs a rehabilitation intervention plan, executed through referral to external institutions for the management of occupational therapy, psychology, and visual rehabilitation.
This lack of knowledge about the possibilities of low vision care and about the need to create an interdisciplinary team for its management is also recognized by the professional in charge of the service as a critical aspect that prevents timely care and has been a barrier in the institution. “I think that most people, even in large clinics, still don’t know. They don’t get the idea of what the low vision service means. One gets used to lack of awareness. This topic is not a blockbuster” [ID#10].
This veil of invisibility that generally accompanies low vision services emerges as a critical aspect, since all study participants, regardless of their form of care (through private payment, prepaid medicine, or through the health system), experienced difficulties in finding an orientation toward rehabilitation or management.
Interaction with the health system: a path of struggles
Once it is possible to have guidance for health care regarding their low vision, there is a difficulty related to the authorization for the service through the health system. People have difficulties with authorizations for low vision appointments, rehabilitation processes, and orders for assistive devices. These difficulties were exacerbated by the COVID-19 pandemic.
These barriers to service authorization are perceived by the optometry professional. “Low vision in Colombia is not known as a specialized service, so that is the problem. That service is unknown by insurance companies” [ID#10]. These difficulties lead to out-of-pocket payments by patients and their families to get medical care. “We have paid for every low vision appointment” [ID#9].
In addition, there is an issue related to the scarcity of low vision providers in the city, leading to a low opportunity for appointments delays for low vision attention and follow-up. In the ophthalmology clinic where this study was carried out, there is only one low vision professional. That is why the allocation times for appointments are so long and were made even longer by the pandemic. “With the pandemic, many things were delayed, not only for me but for everyone. I had those authorizations in March, and everything stopped” [ID#9]. However, those who have prepaid medicine services or who can afford a private service can manage to make appointments quickly. These difficulties for making a timely appointment are critical. Although low vision health care is not considered a vital emergency, it is “a social emergency,” as the participants tell us. That limitation for activities such as reading, working, or accessing visual information has a serious impact on their life quality, their perception of well-being, and their good living.
Once the intervention plan is established by the optometrist (which includes the prescription of necessary devices for the rehabilitation process such as magnifying glasses, telescopes, magnifiers, closed television circuits, filters, among others), a new barrier appears: these services are not included in the benefit plans. At this point there is another struggle that has been experienced by all the participants: It is very difficult to get the authorizations by the health system, I don’t know if visual health is a secondary issue because it is very difficult to get the authorization even for optical aids. I had to buy everything. They do not authorize. It can be done, but it is a long process that is better to avoid. We did it once by my mother spent more money on tickets, tutelage, and a lot of things. [ID#1]
In this sense, the professional in charge of the low vision service says: “I show them the process they must go through to get the authorization in case it is refused by the EPS: first, right to petition, then tutelage and then, if still refused, a petition to the health superintendence” [ID #10]. Because of this, people must buy the devices by themselves. “You cannot imagine how much I have spent on glasses, because there are glasses for the computer, binoculars and glasses. My insurance has never given me anything, and I have to change my devices frequently” [ID#4].
This path of barriers does not end with the purchase of the devices because then the next phase begins: the vision rehabilitation process. This point is even more complex because this service is not included in the health system: I try to get as much information as I can at the appointment and send the people for every service that is required. Then I give an order for a new appointment to be made once the patient has gotten some sort of training. Then it is time to pray to get the authorization and wait for the EPS to authorize and schedule the new appointment. 99% of the patients get to that appointment 8 months or a year later, and most of them arrive even without the first rehabilitation assessment, with all their instruments never used. A process that could be done in one month may take one or two years. [ID#10]
A new barrier emerges within this context and is related to the few centers that provide specialized visual rehabilitation in the city: There is only one place where they do rehabilitation therapy with the proper equipment and trained personnel. Unfortunately, some EPS send patients to places where there is only occupational therapy, and sometimes they get 15 or 20 therapies that had nothing to do with what they need. [ID#10]
None of the participants has had a complete vision rehabilitation process for the management of their low vision condition.
Barriers that are exacerbated by the intersection of multiple identities and systems of oppression
This panorama is made more complex by the intersection of different identities. Social dimensions, such as educational level, economic condition, and geographical location, were found to intersect with each other, generating greater difficulties for the identification of low vision management options, and for the access to optical devices and rehabilitation services, generating greater vulnerability.
The abilities of the participants to gather information about their ocular condition and their possibilities of attention were an important emergent key element. At this point, the educational level and the economic condition were combined to favor the identification of low vision management options. “My mother was studying psychology and she had a professor at the university who told her where to seek help, it helped us a lot. That’s how we got to find specialists; thanks to these contacts I was able to join to a group form of clinical trials in Mexico” [ID #5].
For many participants, the process of searching for and accessing services to manage their condition of low vision was difficult due to the complexities of the health system, the lack of services offered in the city, the lack of people with information to guide them, and their economic possibilities. However, the barriers were experienced differently by each participant according to age, educational level, economic possibilities, affiliation to the health system, and family support. The effects of the multiple barriers were exacerbated for those with specific identities. The case of a participant allows us to understand the way in which the intersection of their identities played a role in their initial care: I think that the fact that I did not live here was important, I was in Turbo, so it delayed my process because where I lived there was none of that, in fact, there still isn’t. On top of that, I belong to the subsidized regime and that makes everything more difficult. [ID #1]
On the contrary, another person who currently lives in a municipality far from the city of Medellín experiences these barriers in a different way, because his place of residence and his age are interrelated to make the possibilities of care more complex. “Where I live . . . it is far and it is not so easy for me to go to Medellín, because I am already very old, and I depend on my children to take me to appointments when they can” [ID #9].
Those people with a high educational level and with economic possibilities experience these barriers in a different way, because their identities, in a conjugated way, allow them to place themselves in a position of less vulnerability or to better face the oppressions given by the barriers described previously. “We really know that the insurance gives us nothing, so we always look for options here in Colombia or outside the country, to see what we can do or use to improve my vision” [ID #2].
Discussion
Our results show the complexities of the experiences faced by participants for the assessment and management of their low vision. An emerging critical aspect is the lack of recognition of this health condition, and, therefore, the exclusion experienced by people with low vision. The Colombian health system acts as an axis of structural oppression that restricts the possibilities of exercising the right to health for people with low vision, as it is not sensitive to the needs of the population to the extent that interventions are not contemplated in benefit plans or the organization of health services, causing people to take legal action to demand their rights.
This system does not comprehensively address the needs in diagnosis, treatment, and rehabilitation; only the low vision assessment is included, while other processes required for comprehensive health care are scattered and even blurred throughout the range of health procedures. This is explained by the structure of the system, and its managed care model, in which insurers use service authorizations as barriers that limit and delay care (Vargas et al., 2013), treatment, increasing to receive the attention, leading to higher costs and worsening access for the urban population in a socioeconomic level (Florez & Soto, 2007).
Although these technologies are not explicitly excluded from the health services financed by the system for people with low vision, there are barriers to their access, due to the administrative procedures or to the lack of knowledge by the insurance companies, among other reasons. The system is even weaker when it comes to visual functional rehabilitation (Toro-Hernández et al., 2019). As noted in our results, none of the participants has received a comprehensive rehabilitation, understood as a multidisciplinary and multicomponent process for the management of their visual impairment; they have only received specific, distant, and unarticulated interventions.
Therefore, they face a health system with high therapeutic dispersion, difficulty in accessing specialized care, administrative and procedural barriers to access services, and lack of trained medical professionals (Achury, 2016). In the context of disability, fragmentation leads to summative care, developed by different professionals, without any coordination, and it does not favor the needs of the population (Míguez Passada, 2012). The Pan American Health Organization highlights how the health systems of Latin America are highly fragmented, thus generating difficulties in service access, loss of care continuity, and lack of congruence of services with people’s needs (Montenegro et al., 2011).
The rehabilitation panorama in the world is also complex. Low vision rehabilitation services are only accessible to approximately 15 percent of the world’s population, with barriers similar: limited service availability, high costs, and health workers without enough skills and knowledge (World Health Organization, 2015). Eye care interventions remain not integrated into health insurance plans in many low- and middle-income countries and are often provided by charities and non-governmental organizations (World Health Organization, 2019).
The intersectional scope allowed us to see the oppression spectrum generated by the health system because it recognizes that people experience their lives through different intersecting identities. These factors can contribute to barriers in care and result in a worse health condition. This perspective has been used to address other problems, but to date, we have not found specific studies on visual health. Our results emphasize that access to low vision care is not determined by a single factor. The multiple identities of the subjects and the power relations between the structures interact simultaneously, affecting their possibilities (Collins, 2015). The economic condition, educational level, and geographical location intersected to generate greater difficulties for the identification of low vision management options, for access to optical devices and rehabilitation services, generating greater vulnerability. Although gender has been reported as an important barrier to access to health services, in this study the intersectional oppression and discrimination presented because of the invisibilization of low vision in the health system, as well as the structural shortcomings of the care centers, educational level, economic status and place of residence, meant that this gender identity has not been fully recognized as a critical marker for seeking and accessing rehabilitation services.
Our findings show another barrier related to the lack of care centers providing a complete comprehensive rehabilitation process. This panorama shows us the precariousness of care. This study was carried out in a high-level ophthalmological center in the second-largest city in the country, and even though it is a reference clinic for ophthalmological care, there is also a lack of interest concerning this issue. There is only one professional in charge of the service, which is not enough to provide timely attention. It has been reported that low vision services do not receive due importance in many developing countries like ours (Senjam, 2021).
The lack of awareness of visual health professionals emerges concerning the possibilities of care for people with low vision since they focus on the diagnosis of ocular pathology, sparing the functional and life implications this condition has. It is important because these two professions oversee detection, diagnosis, and referral to rehabilitation services. Similar situations are found in an international context since it is mentioned that vision rehabilitation has been neglected in ophthalmological and optometric practice (Sarika et al., 2019; World Health Organization, 2015).
Conclusion
The Colombian health system acts as an axis of structural oppression that interacts with the economic condition, educational level, and geographical location to generate greater difficulties for the identification of low vision management options, which also interact with the multiple and dynamic identities of each subject. Any effort to improve the inclusion of this population must have a simultaneous approach: improving the structure of the health system, the improvement of installed capacity, the qualification of healthcare providers, and the generation of targeted strategies for those whose identities generate greater oppression when interacting with health systems.
It is necessary to strengthen the Colombian health system to improve access to rehabilitation services for low vision, for this it is important to carry out a process of advocacy with the Ministry of Health to position low vision as a priority aspect of public health. In the same way, low vision and rehabilitation services should be included in the training of ophthalmologists and optometrists, so that this translates into better care and interventions to reduce the impact of visual loss.
Low vision, more than a visual impairment triggered by ocular pathologies, should be approached as a life condition that crosses the being in its multiple dimensions, which makes it necessary to understand the complexity of what its experience implies and the challenges it poses. If we continue to think of low vision only in terms of loss of visual acuity, visual field, contrast sensitivity, and other ocular functions, we will continue to perpetuate this view of disability as a matter of the body, making the subject invisible. The intersectional view of this work can provide elements to help professionals involved in care to think broadly, for example, raising the need to recognize how identities, oppressions, and contexts come together in people’s lives to create complex situations. When we only think of low vision as the sole marker of identity, we do not consider the fact that others, such as gender and age, can worsen the circumstances and implications of visual impairment. This would provide important elements for the implementation of person-centered care, in which the patient, family or caregivers, community, and providers work together to plan care at the intersection of the multiple identities of people with low vision. These elements open the door to a line of research and work to discuss vision rehabilitation from an intersectional perspective.
Limitations
The condition of isolation due to the COVID-19 outbreak implied conducting interviews through virtual media and face-to-face meetings and participant observations had to be limited.
Footnotes
Acknowledgements
The authors warmly thank the people who participated in this study and generously shared their experiences.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.